Influence of Personality, Resilience and Life Conditions on Depression and Anxiety in 104 Patients Having Survived Acute Autoimmune Thrombotic Thrombocytopenic Purpura


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Controls
2.2. Psychometric Assessment
2.2.1. Patient Health Questionnaire 9 Items (PHQ-9)
2.2.2. Generalized Anxiety Disorder 7 (GAD-7)
2.2.3. FLei
2.2.4. Resilience Scale 11 (RS-11)
2.2.5. Life Orientation Test–Revised (LOT-R)
2.2.6. Quality of Life Questionnaire C 30 (QLQ-C30)
2.3. Covariates
2.4. Statistical Analyses
3. Results
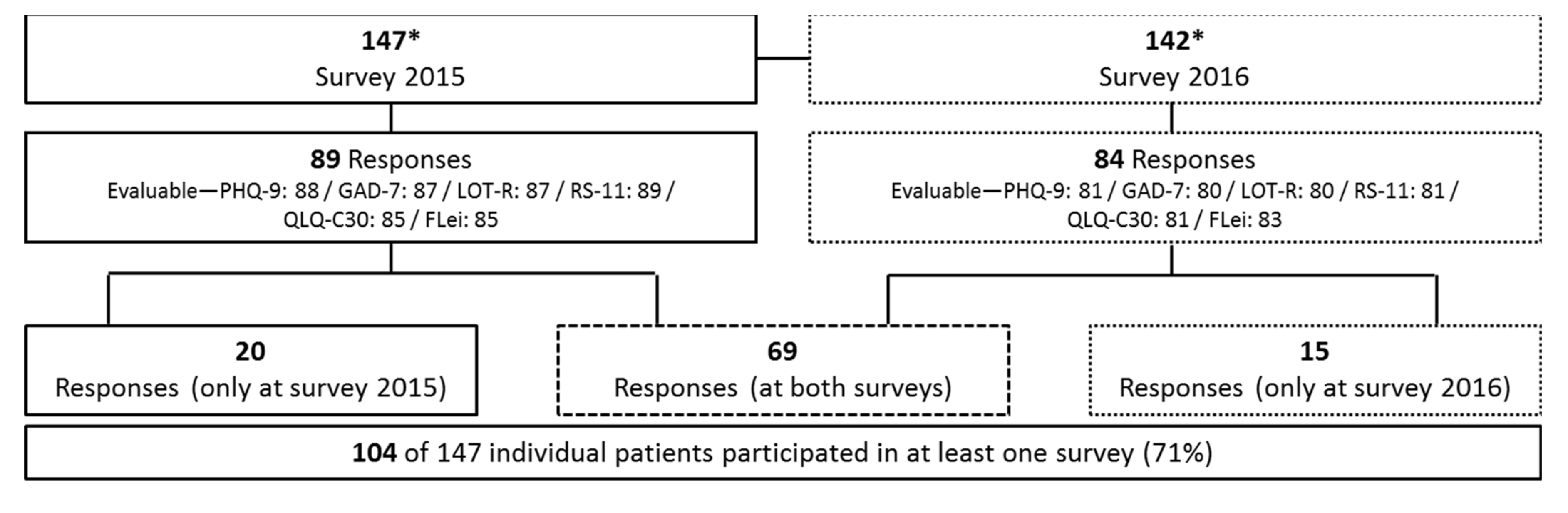
3.1. Study Population
3.2. Patient Characteristics
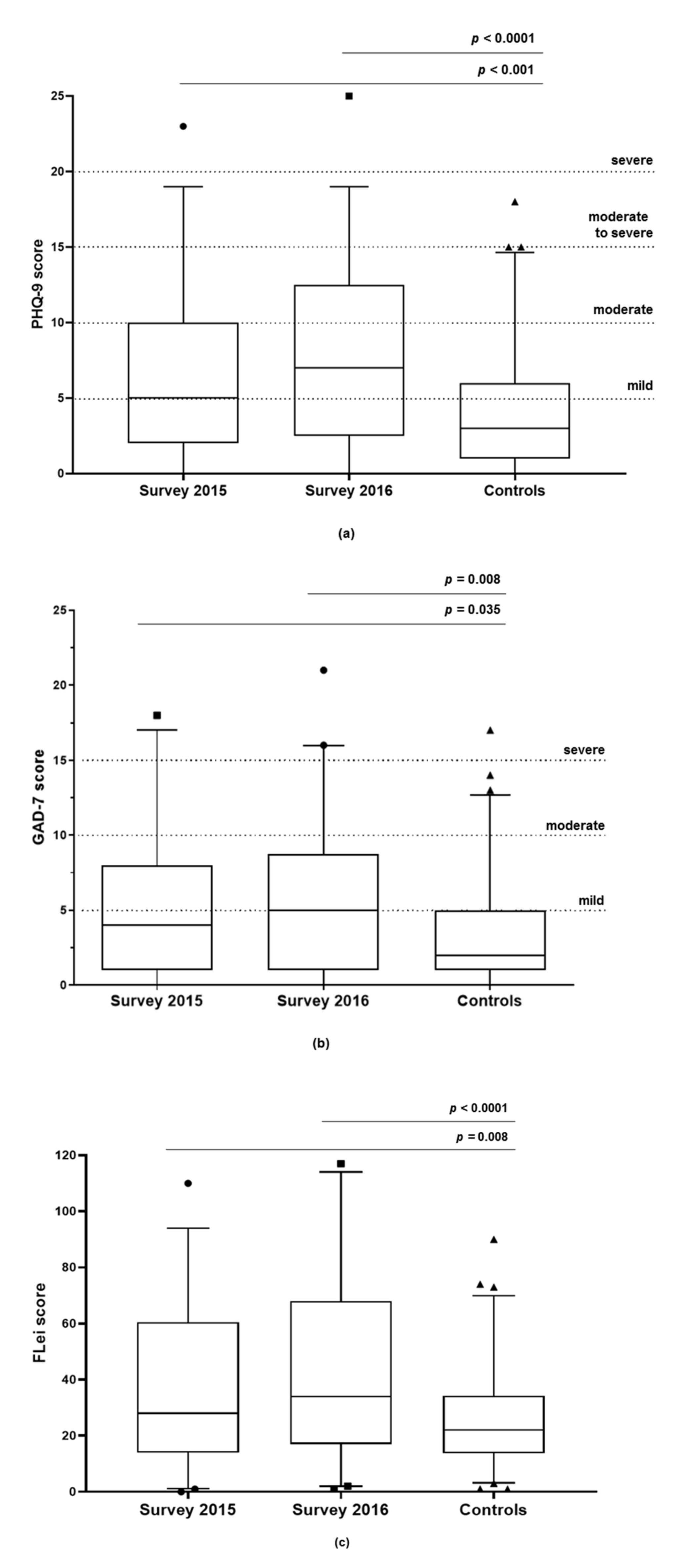
3.3. Depression (PHQ-9)
3.4. Anxiety Disorder (GAD-7)
3.5. Cognitive Performance (FLei Score)
3.6. Resilience (RS-11)
3.7. Attitude to Life (LOT-R)
3.8. Quality of Life (QLQ-C30)
3.9. Correlation of Life Circumstances and Personality with Depression
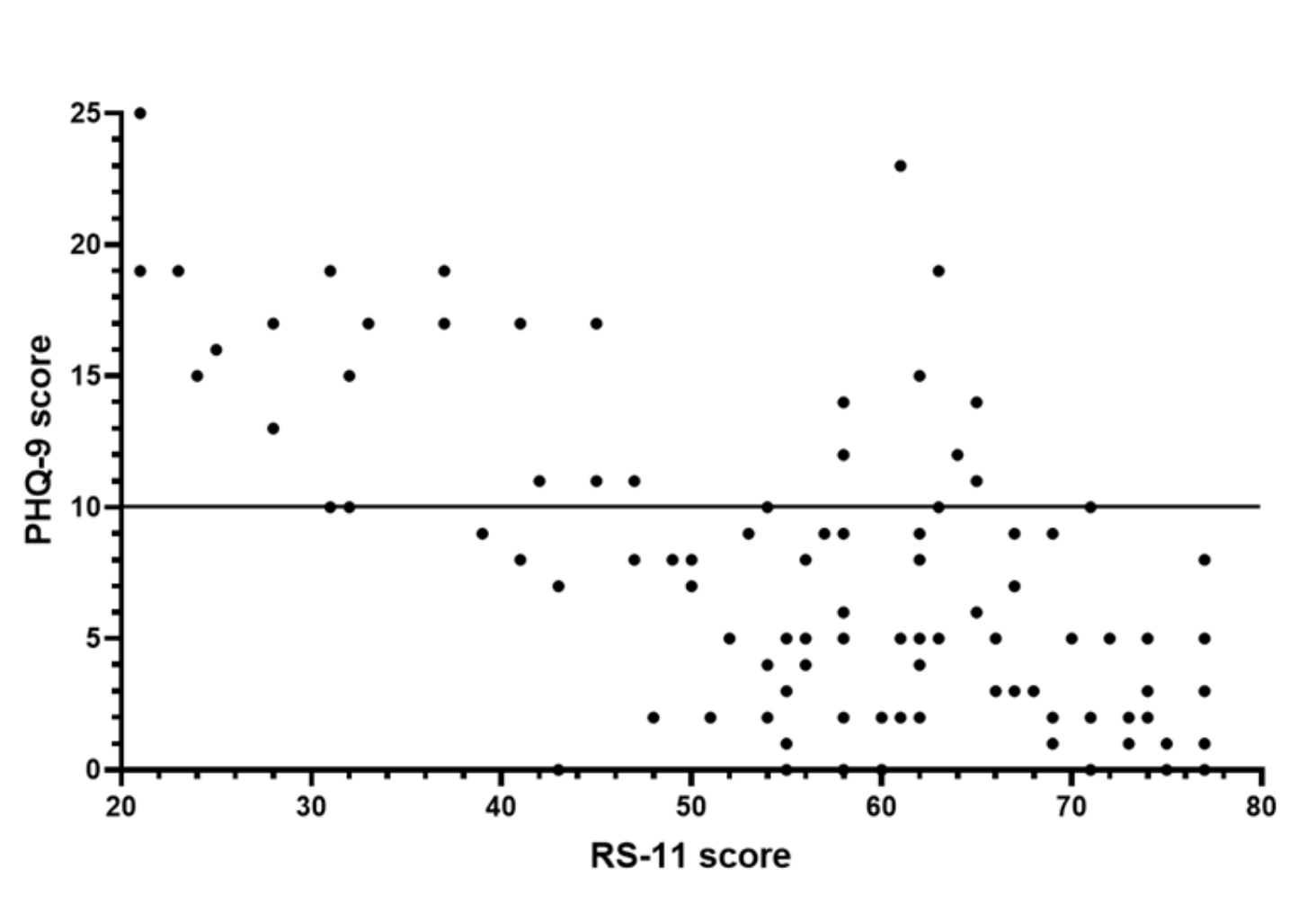
3.10. Correlation of Resilience with Depression
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsai, H.M. Pathophysiology of thrombotic thrombocytopenic purpura. Int. J. Hematol. 2010, 91, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawley, J.T.; Scully, M.A. Thrombotic thrombocytopenic purpura: Basic pathophysiology and therapeutic strategies. Hematol. Am. Soc. Hematol. Educ. Program. 2013, 2013, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Hovinga, J.A.K.; Vesely, S.K.; Terrell, D.R.; Lammle, B.; George, J.N. Survival and relapse in patients with thrombotic thrombocytopenic purpura. Blood 2010, 115, 1500–1511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, A.S.; Lewis, Q.F.; Scott, J.G.; Hovinga, J.A.K.; Lammle, B.; Terrell, D.R.; Vesely, S.K.; George, J.N. Cognitive deficits after recovery from thrombotic thrombocytopenic purpura. Transfusion 2009, 49, 1092–1101. [Google Scholar] [CrossRef]
- Cataland, S.R.; Scully, M.A.; Paskavitz, J.; Maruff, P.; Witkoff, L.; Jin, M.; Uva, N.; Gilbert, J.C.; Wu, H.M. Evidence of persistent neurologic injury following thrombotic thrombocytopenic purpura. Am. J. Hematol. 2011, 86, 87–89. [Google Scholar] [CrossRef]
- Han, B.; Page, E.E.; Stewart, L.M.; Deford, C.C.; Scott, J.G.; Schwartz, L.H.; Perdue, J.J.; Terrell, D.R.; Vesely, S.K.; George, J.N. Depression and cognitive impairment following recovery from thrombotic thrombocytopenic purpura. Am. J. Hematol. 2015, 90, 709–714. [Google Scholar] [CrossRef] [Green Version]
- Riva, S.; Mancini, I.; Maino, A.; Ferrari, B.; Artoni, A.; Agosti, P.; Peyvandi, F. Long-term neuropsychological sequelae, emotional wellbeing and quality of life in patients with acquired thrombotic thrombocytopenic purpura. Haematologica 2020, 105, 1957–1962. [Google Scholar] [CrossRef] [Green Version]
- Deford, C.C.; Reese, J.A.; Schwartz, L.H.; Perdue, J.J.; Hovinga, J.A.K.; Lammle, B.; Terrell, D.R.; Vesely, S.K.; George, J.N. Multiple major morbidities and increased mortality during long-term follow-up after recovery from thrombotic thrombocytopenic purpura. Blood 2013, 122, 2023–2029. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, S.; Oluwole, O.; Cataland, S.; McCrae, K.R. Post-traumatic stress disorder and depression in survivors of thrombotic thrombocytopenic purpura. Thromb Res. 2017, 151, 51–56. [Google Scholar] [CrossRef]
- Falter, T.; Schmitt, V.; Herold, S.; Weyer, V.; von Auer, C.; Wagner, S.; Hefner, G.; Beutel, M.; Lackner, K.; Lammle, B.; et al. Depression and cognitive deficits as long-term consequences of thrombotic thrombocytopenic purpura. Transfusion 2017, 57, 1152–1162. [Google Scholar] [CrossRef] [Green Version]
- Kauhanen, M.; Korpelainen, J.T.; Hiltunen, P.; Brusin, E.; Mononen, H.; Maatta, R.; Nieminen, P.; Sotaniemi, K.A.; Myllyla, V.V. Poststroke depression correlates with cognitive impairment and neurological deficits. Stroke 1999, 30, 1875–1880. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.G.; Spalletta, G. Poststroke depression: A review. Can. J. Psychiatry 2010, 55, 341–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegert, R.J.; Abernethy, D.A. Depression in multiple sclerosis: A review. J. Neurol. Neurosurg. Psychiatry 2005, 76, 469–475. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.H.; Ford, D.V.; Jones, P.A.; John, A.; Middleton, R.M.; Lockhart-Jones, H.; Osborne, L.A.; Noble, J.G. A large-scale study of anxiety and depression in people with Multiple Sclerosis: A survey via the web portal of the UK MS Register. PLoS ONE 2012, 7, e41910. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.M.; Currie, K.C. Depression, anxiety and their relationship with chronic diseases: A review of the epidemiology, risk and treatment evidence. Med. J. Aust. 2009, 190, S54–S60. [Google Scholar] [CrossRef] [PubMed]
- Van der Kooy, K.; van Hout, H.; Marwijk, H.; Marten, H.; Stehouwer, C.; Beekman, A. Depression and the risk for cardiovascular diseases: Systematic review and meta analysis. Int. J. Geriatr. Psychiatry 2007, 22, 613–626. [Google Scholar] [CrossRef]
- Cuijpers, P.; Smit, F. Excess mortality in depression: A meta-analysis of community studies. J. Affect Disord. 2002, 72, 227–236. [Google Scholar] [CrossRef]
- Schiele, M.A.; Domschke, K. Epigenetics at the crossroads between genes, environment and resilience in anxiety disorders. Genes Brain Behav. 2018, 17, e12423. [Google Scholar] [CrossRef] [Green Version]
- De Berardis, D.; Fornaro, M.; Valchera, A.; Rapini, G.; Di Natale, S.; De Lauretis, I.; Serroni, N.; Orsolini, L.; Tomasetti, C.; Bustini, M.; et al. Alexithymia, resilience, somatic sensations and their relationships with suicide ideation in drug naive patients with first-episode major depression: An exploratory study in the “real world” everyday clinical practice. Early Interv. Psychiatry 2020, 14, 336–342. [Google Scholar] [CrossRef]
- George, J.N.; Vesely, S.K.; Terrell, D.R.; Deford, C.C.; Reese, J.A.; Al-Nouri, Z.L.; Stewart, L.M.; Lu, K.H.; Muthurajah, D.S. The Oklahoma Thrombotic Thrombocytopenic Purpura-haemolytic Uraemic Syndrome Registry. A model for clinical research, education and patient care. Hamostaseologie 2013, 33, 105–112. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beblo, T.; Kunz, M.; Brokate, B.; Scheurich, A.; Weber, B.; Albert, A.; Richter, P.; Lautenbacher, S. Construction of a Questionnaire for Complaints of Cognitive Disturbances in Patients with Mental Disorders. Z. Neuropsychol. 2010, 21, 143–151. [Google Scholar] [CrossRef]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas 1993, 1, 165–178. [Google Scholar] [PubMed]
- Scheier, M.F.; Carver, C.S.; Bridges, M.W. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the Life Orientation Test. J. Personal. Soc. Psychol. 1994, 67, 1063–1078. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Schwarz, R.; Hinz, A. Reference data for the quality of life questionnaire EORTC QLQ-C30 in the general German population. Eur. J. Cancer 2001, 37, 1345–1351. [Google Scholar] [CrossRef]
- Jacobi, F.; Hofler, M.; Strehle, J.; Mack, S.; Gerschler, A.; Scholl, L.; Busch, M.A.; Maske, U.; Hapke, U.; Gaebel, W.; et al. Mental disorders in the general population: Study on the health of adults in Germany and the additional module mental health (DEGS1-MH). Nervenarzt 2014, 85, 77–87. [Google Scholar] [CrossRef]
- Terrell, D.R.; Tolma, E.L.; Stewart, L.M.; Shirley, E.A. Thrombotic thrombocytopenic purpura patients’ attitudes toward depression management: A qualitative study. Health Sci. Rep. 2019, 2, e136. [Google Scholar] [CrossRef]
- George, J.N. TTP: Long-term outcomes following recovery. Hematol. Am. Soc. Hematol. Educ. Program. 2018, 2018, 548–552. [Google Scholar] [CrossRef] [Green Version]
- Harter, M.; Baumeister, H.; Reuter, K.; Jacobi, F.; Hofler, M.; Bengel, J.; Wittchen, H.U. Increased 12-month prevalence rates of mental disorders in patients with chronic somatic diseases. Psychother. Psychosom. 2007, 76, 354–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alwan, F.; Mahdi, D.; Tayabali, S.; Cipolotti, L.; Lakey, G.; Hyare, H.; Scully, M. Cerebral MRI findings predict the risk of cognitive impairment in thrombotic thrombocytopenic purpura. Br. J. Haematol. 2020, 191, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, F.; Hofler, M.; Siegert, J.; Mack, S.; Gerschler, A.; Scholl, L.; Busch, M.A.; Hapke, U.; Maske, U.; Seiffert, I.; et al. Twelve-month prevalence, comorbidity and correlates of mental disorders in Germany: The Mental Health Module of the German Health Interview and Examination Survey for Adults (DEGS1-MH). Int. J. Methods Psychiatr. Res. 2014, 23, 304–319. [Google Scholar] [CrossRef] [PubMed]
- Martin-Subero, M.; Kroenke, K.; Diez-Quevedo, C.; Rangil, T.; de Antonio, M.; Morillas, R.M.; Loran, M.E.; Mateu, C.; Lupon, J.; Planas, R.; et al. Depression as Measured by PHQ-9 Versus Clinical Diagnosis as an Independent Predictor of Long-Term Mortality in a Prospective Cohort of Medical Inpatients. Psychosom. Med. 2017, 79, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Lewis, Q.F.; Lanneau, M.S.; Mathias, S.D.; Terrell, D.R.; Vesely, S.K.; George, J.N. Long-term deficits in health-related quality of life after recovery from thrombotic thrombocytopenic purpura. Transfusion 2009, 49, 118–124. [Google Scholar] [CrossRef]
- Kaiser, T.; Janssen, B.; Schrader, S.; Geerling, G. Depressive symptoms, resilience, and personality traits in dry eye disease. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 591–599. [Google Scholar] [CrossRef]
- Toukhsati, S.R.; Jovanovic, A.; Dehghani, S.; Tran, T.; Tran, A.; Hare, D.L. Low psychological resilience is associated with depression in patients with cardiovascular disease. Eur. J. Cardiovasc. Nurs. 2017, 16, 64–69. [Google Scholar] [CrossRef]
- Avila, M.P.W.; Lucchetti, A.L.; Lucchetti, G. Association between depression and resilience in older adults: A systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 2017, 32, 237–246. [Google Scholar] [CrossRef]
- Hu, T.; Xiao, J.; Peng, J.; Kuang, X.; He, B. Relationship between resilience, social support as well as anxiety/depression of lung cancer patients: A cross-sectional observation study. J. Cancer Res. Ther. 2018, 14, 72–77. [Google Scholar] [CrossRef]
- Choi, Y.; Choi, S.H.; Yun, J.Y.; Lim, J.A.; Kwon, Y.; Lee, H.Y.; Jang, J.H. The relationship between levels of self-esteem and the development of depression in young adults with mild depressive symptoms. Medicine (Baltim.) 2019, 98, e17518. [Google Scholar] [CrossRef]
- Southwick, S.M.; Charney, D.S. The science of resilience: Implications for the prevention and treatment of depression. Science 2012, 338, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Knoebl, P.; Cataland, S.; Peyvandi, F.; Coppo, P.; Scully, M.; Hovinga, J.A.K.; Metjian, A.; de la Rubia, J.; Pavenski, K.; Edou, J.M.M.; et al. Efficacy and safety of open-label caplacizumab in patients with exacerbations of acquired thrombotic thrombocytopenic purpura in the HERCULES study. J. Thromb. Haemost. 2020, 18, 479–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Heading | iTTP Patients | Healthy Controls | |
|---|---|---|---|
| Time of survey | 2015 | 2016 | 2016 |
| Number (n) | 89 | 84 | 134 |
| Gender and age | |||
| Female | 69 (76%) | 69 (82%) | 108 (81%) |
| Male | 20 (24%) | 15 (18%) | 26 (19%) |
| Age (years) median (min, IQR, max) | 48 (18, 37–59, 86) | 51 (21, 38–59, 87) | 48 (19, 30–60, 79) |
| Data for age missing | 6 | 7 | 0 |
| Current partnership | |||
| Yes | 62 (73%) | 60 (75%) | 96 (74%) |
| No | 23 (27%) | 20 (25%) | 34 (26%) |
| Data missing | 4 | 4 | 4 |
| Occupation, BMI, smoking status | |||
| Employed | 45 (51%) | 41 (50%) | 72 (55%) |
| Studying | 3 (3%) | 1 (1%) | 14 (11%) |
| Retired | 26 (30%) | 22 (27%) | 27 (21%) |
| Unemployed | 2 (2%) | 4 (5%) | 2 (1%) |
| Working at home | 4 (5%) | 7 (8.5%) | 5 (4%) |
| Other | 8 (9%) | 7 (8.5%) | 10 (8%) |
| Data missing | 1 | 2 | 4 |
| BMI median (min, IQR, max) | 26 (18, 23–31, 48) | 28 (18, 24–32, 47) | 24 (18, 21–26, 42) |
| Obesity (BMI ≥ 30) | 24 (27%) | 29 (35%) | 12 (9%) |
| Data missing | 0 | 2 | 4 |
| Smoking | 22 (25%) | 21 (25%) | 18 (14%) |
| Data missing | 0 | 1 | 2 |
| Physical activity | |||
| Hardly active (1–2×/month) | 25 (29%) | 32 (39%) | 22 (17%) |
| Quite active (3–4×/month) | 10 (12%) | 13 (16%) | 24 (18%) |
| Active (1–2×/week) | 33 (39%) | 24 (30%) | 45 (34%) |
| Very active (3–4×/week) | 14 (16%) | 8 (10%) | 32 (24%) |
| Extremely active (>5×/week) | 3 (4%) | 4 (5%) | 9 (7%) |
| Data missing | 4 | 3 | 2 |
| Number of comorbidities 1 | |||
| 0 | 20 (22%) | 10 (12%) | 48 (36%) |
| 1 | 25 (28%) | 20 (24%) | 43 (33%) |
| 2 | 14 (16%) | 23 (28%) | 18 (14%) |
| ≥3 | 30 (34%) | 30 (36%) | 23 (17%) |
| Data missing | 0 | 1 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falter, T.; Böschen, S.; Schepers, M.; Beutel, M.; Lackner, K.; Scharrer, I.; Lämmle, B. Influence of Personality, Resilience and Life Conditions on Depression and Anxiety in 104 Patients Having Survived Acute Autoimmune Thrombotic Thrombocytopenic Purpura. J. Clin. Med. 2021, 10, 365. https://doi.org/10.3390/jcm10020365
Falter T, Böschen S, Schepers M, Beutel M, Lackner K, Scharrer I, Lämmle B. Influence of Personality, Resilience and Life Conditions on Depression and Anxiety in 104 Patients Having Survived Acute Autoimmune Thrombotic Thrombocytopenic Purpura. Journal of Clinical Medicine. 2021; 10(2):365. https://doi.org/10.3390/jcm10020365
Chicago/Turabian StyleFalter, Tanja, Sibylle Böschen, Markus Schepers, Manfred Beutel, Karl Lackner, Inge Scharrer, and Bernhard Lämmle. 2021. "Influence of Personality, Resilience and Life Conditions on Depression and Anxiety in 104 Patients Having Survived Acute Autoimmune Thrombotic Thrombocytopenic Purpura" Journal of Clinical Medicine 10, no. 2: 365. https://doi.org/10.3390/jcm10020365