The Italian COVID-19 Psychological Research Consortium (IT C19PRC): General Overview and Replication of the UK Study

 , , , , and
, , , , and 
Abstract
:1. Introduction
Aims
2. Methodological Section
2.1. Study Plan
2.2. Participants
2.3. Measures
2.4. Analytic Methods
3. Results
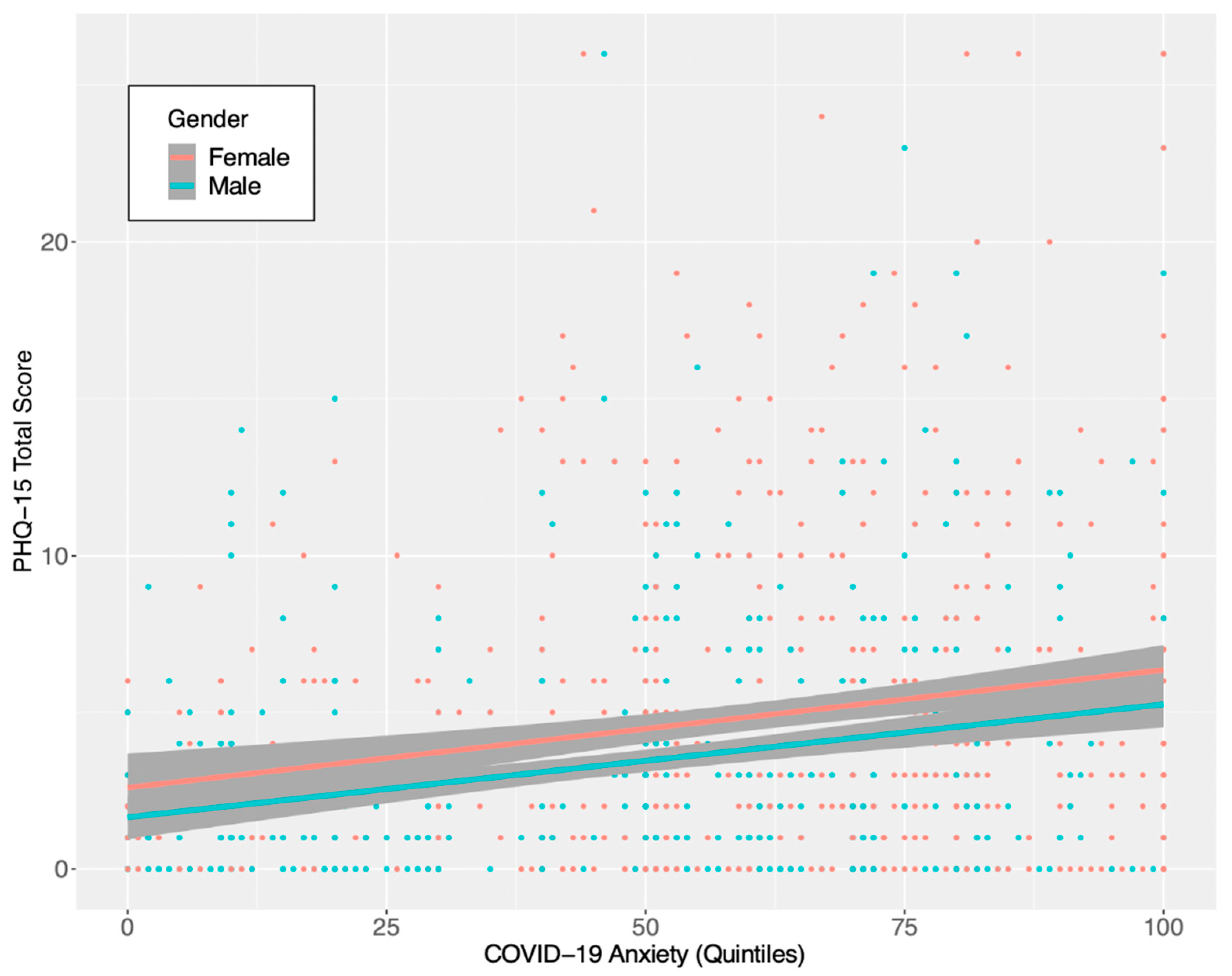
3.1. Somatic Symptoms
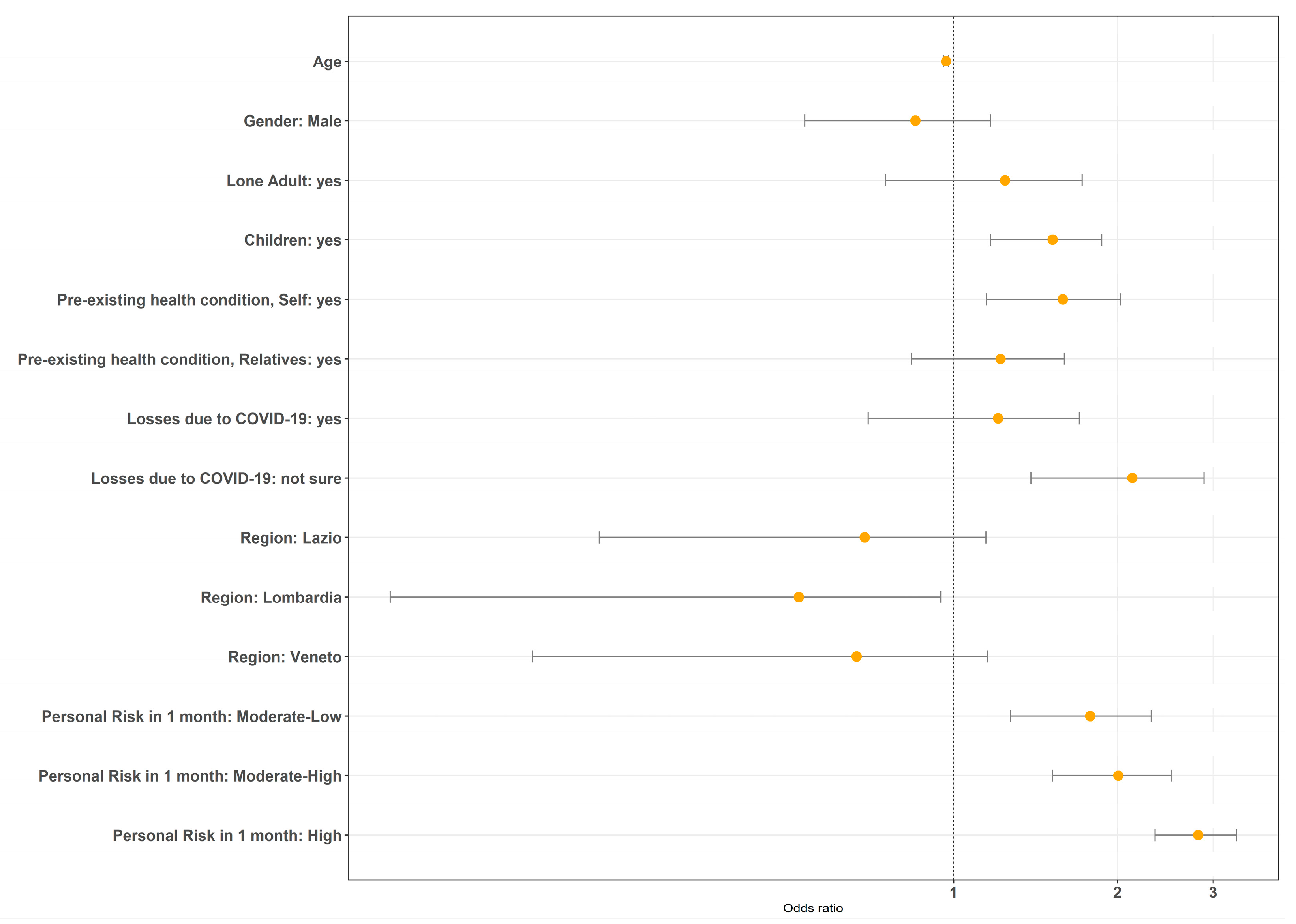
3.2. Anxiety, Depression, and Traumatic Stress
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baud, D.; Qi, X.; Nielsen-Saines, K.; Musso, D.; Pomar, L.; Favre, G. Real estimates of mortality following COVID-19 infection. Lancet Infect. Dis. 2020, 20, 773. [Google Scholar] [CrossRef] [Green Version]
- Zaim, S.; Chong, J.H.; Sankaranarayanan, V.; Harky, A. COVID-19 and Multiorgan Response. Curr. Probl. Cardiol. 2020, 45, 100618. [Google Scholar] [CrossRef] [PubMed]
- Funk, S.; Salathé, M.; Jansen, V.A.A. Modelling the influence of human behaviour on the spread of infectious diseases: A review. J. R. Soc. Interface 2010, 7, 1247–1256. [Google Scholar] [CrossRef] [PubMed]
- Wind, T.R.; Rijkeboer, M.; Andersson, G.; Riper, H. The COVID-19 pandemic: The ‘black swan’ for mental health care and a turning point for e-health. Internet Interv. 2020, 20, 100317. [Google Scholar] [CrossRef]
- Forte, G.; Favieri, F.; Tambelli, R.; Casagrande, M. The Enemy Which Sealed the World: Effects of COVID-19 Diffusion on the Psychological State of the Italian Population. J. Clin. Med. 2020, 9, 1802. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Cellini, N.; Canale, N.; Mioni, G.; Costa, S. Changes in sleep pattern, sense of time and digital media use during COVID-19 lockdown in Italy. J. Sleep Res. 2020, 29, e13074. [Google Scholar] [CrossRef]
- Cerami, C.; Santi, G.C.; Galandra, C.; Dodich, A.; Cappa, S.F.; Vecchi, T.; Crespi, C. COVID-19 Outbreak in Italy: Are We Ready for the Psychosocial and Economic Crisis? Baseline Findings from the Longitudinal PsyCovid Study. SSRN Electron. J. 2020. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Panzeri, A.; Pietrabissa, G.; Manzoni, G.M.; Castelnuovo, G.; Mannarini, S. The Anxiety-Buffer Hypothesis in the Time of COVID-19: When Self-Esteem Protects from the Impact of Lone-liness and Fear on Anxiety and Depression. Front. Psychol. 2020, 11, 2177. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef]
- Yang, Y.; Li, W.; Zhang, Q.; Zhang, L.; Cheung, T.; Xiang, Y.-T. Mental health services for older adults in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e19. [Google Scholar] [CrossRef]
- Yao, H.; Chen, J.-H.; Xu, Y.-F. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry 2020, 7, e21. [Google Scholar] [CrossRef]
- Kang, L.; Wang, G.; Liu, Z. Targeted long-term mental health services in Wuhan dealing with COVID-19. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 1–3. [Google Scholar] [CrossRef]
- Gardner, P.J.; Moallef, P. Psychological impact on SARS survivors: Critical review of the English language literature. Can. Psychol. Can. 2015, 56, 123–135. [Google Scholar] [CrossRef]
- Gatto, M.; Bertuzzo, E.; Mari, L.; Miccoli, S.; Carraro, L.; Casagrandi, R.; Rinaldo, A. Spread and dynamics of the COVID-19 epidemic in Italy: Effects of emergency containment measures. Proc. Natl. Acad. Sci. USA 2020, 117, 10484–10491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McBride, O.; Murphy, J.; Shevlin, M.; Gibson-Miller, J.; Hartman, T.K.; Hyland, P.; Levita, L.; Mason, L.; Martinez, A.P.; McKay, R.; et al. Monitoring the psychological, social, and economic impact of the COVID-19 pandemic in the population: Context, design and conduct of the longitudinal COVID-19 psychological research consortium (C19PRC) study. Int. J. Methods Psychiatr. Res. 2020, e1861. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute, Istituto Superiore della Sanità. Report Monitoraggio Settimanale Covid-19: “Lieve Aumento dei Casi. Rispettare Misure di Precauzione”. Available online: http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioNotizieNuovoCoronavirus.jsp?menu=notizie&p=dalministero&id=4971 (accessed on 15 November 2020).
- Berardi, C.; Antonini, M.; Genie, M.G.; Cotugno, G.; Lanteri, A.; Melia, A.; Paolucci, F. The COVID-19 pandemic in Italy: Policy and technology impact on health and non-health outcomes. Health Policy Technol. 2020, 9, 454–487. [Google Scholar] [CrossRef]
- Shevlin, M.; McBride, O.; Murphy, J.; Miller, J.G.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; McKay, R.; Stocks, T.V.A.; et al. Anxiety, depression, traumatic stress and COVID-19-related anxiety in the UK general population during the COVID-19 pandemic. BJPsych Open 2020, 6. [Google Scholar] [CrossRef]
- Shevlin, M.; Nolan, E.; Owczarek, M.; McBride, O.; Murphy, J.; Gibson Miller, J.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; et al. COVID-19-related anxiety predicts somatic symptoms in the UK population. Br. J. Health Psychol. 2020, 25, 875–882. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-15: Validity of a New Measure for Evaluating the Severity of Somatic Symptoms. Psychosom. Med. 2002, 64, 258–266. [Google Scholar] [CrossRef] [Green Version]
- Cano-García, F.J.; Muñoz-Navarro, R.; Abad, A.S.; Moretti, L.S.; Medrano, L.A.; Ruiz-Rodríguez, P.; González-Blanch, C.; Moriana, J.A.; Cano-Vindel, A. Latent structure and factor invariance of somatic symptoms in the patient health questionnaire (PHQ-15). J. Affect. Disord. 2020, 261, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The Patient Health Questionnaire (PHQ-9)—Overview. J. Gen. Intern. Med. 2001, 16, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Manea, L.; Gilbody, S.; McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. Can. Med Assoc. J. 2011, 184, E191–E196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092. [Google Scholar] [CrossRef] [Green Version]
- Hinz, A.; Klein, A.M.; Brähler, E.; Glaesmer, H.; Luck, T.; Riedel-Heller, S.G.; Wirkner, K.; Hilbert, A. Psychometric evaluation of the Generalized Anxiety Disorder Screener GAD-7, based on a large German general population sample. J. Affect. Disord. 2017, 210, 338–344. [Google Scholar] [CrossRef]
- Cloitre, M.; Shevlin, M.; Brewin, C.R.; Bisson, J.I.; Roberts, N.P.; Maercker, A.; Karatzias, T.; Hyland, P. The International Trauma Questionnaire: Development of a self-report measure of ICD-11 PTSD and com-plex PTSD. Acta Psychiatr. Scand. 2018, 138, 536–546. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision, 2018). Available online: https://icd.who.int/browse11/l-m/en (accessed on 15 November 2020).
- Ben-Ezra, M.; Karatzias, T.; Hyland, P.; Brewin, C.R.; Cloitre, M.; Bisson, J.I.; Roberts, N.P.; Lueger-Schuster, B.; Shevlin, M. Posttraumatic stress disorder (PTSD) and complex PTSD (CPTSD) as per ICD-11 proposals: A population study in Israel. Depress. Anxiety 2018, 35, 264–274. [Google Scholar] [CrossRef]
- Cloitre, M.; Hyland, P.; Bisson, J.I.; Brewin, C.R.; Roberts, N.P.; Karatzias, T.; Shevlin, M. ICD-11 Posttraumatic Stress Disorder and Complex Posttraumatic Stress Disorder in the United States: A Population-Based Study. J. Trauma. Stress 2019, 32, 833–842. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B Stat. Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Ho, S.M.Y.; Chan, J.C.K.; Kwong, R.S.Y.; Cheung, C.K.Y.; Wong, C.P.Y.; Wong, V.C.W. Psychological resilience and dysfunction among hospitalized survivors of the SARS epidemic in Hong Kong: A latent class approach. Health Psychol. 2008, 27, 659–667. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Wu, J.; Hao, S.; Yang, M.; Lu, X.; Chen, X.; Li, L. Long term outcomes in survivors of epidemic Influenza A (H7N9) virus infection. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.M.; Wong, J.G.W.S.; McAlonan, G.M.; Cheung, V.; Cheung, C.; Sham, P.C.; Chu, C.-M.; Wong, P.-C.; Tsang, K.W.T.; Chua, S.E. Stress and Psychological Distress among SARS Survivors 1 Year after the Outbreak. Can. J. Psychiatry 2007, 52, 233–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esterwood, E.; Saeed, S.A. Past Epidemics, Natural Disasters, COVID19, and Mental Health: Learning from History as we Deal with the Present and Prepare for the Future. Psychiatr. Q. 2020, 91, 1121–1133. [Google Scholar] [CrossRef] [PubMed]
- Seery, M.D.; Holman, E.A.; Silver, R.C. Whatever does not kill us: Cumulative lifetime adversity, vulnerability, and resilience. J. Pers. Soc. Psychol. 2010, 99, 1025–1041. [Google Scholar] [CrossRef]
- Casagrande, M.; Favieri, F.; Tambelli, R.; Forte, G. The enemy who sealed the world: Effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020, 75, 12–20. [Google Scholar] [CrossRef]
- Parola, A.; Rossi, A.; Tessitore, F.; Troisi, G.; Mannarini, S. Mental Health through the COVID-19 Quarantine: A Growth Curve Analysis on Italian Young Adults. Front. Psychol. 2020, 11, 567484. [Google Scholar] [CrossRef]
- Spinelli, M.; Lionetti, F.; Pastore, M.; Fasolo, M. Parents and Children Facing the COVID-19 Outbreak in Italy. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age | Gender | Income | C-19 Human Losses | P.H.I. | C-19 Anxiety | PHQ-15 (Pain) | PHQ-15 (Gastro) | PHQ-15 (Cardio) | PHQ-15 (Fatigue) | PHQ-15 (Total) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | 0.19 *** | ||||||||||
| Income | 0.00 | 0.12 *** | |||||||||
| C-19 Human Losses | −0.12 *** | −0.09 ** | −0.04 | ||||||||
| P.H.I. | 0.21 *** | 0.09 ** | −0.07 * | −0.05 | |||||||
| GAD-7 (Total) | −0.23 **** | −0.13 **** | −0.02 | −0.28 *** | 0.06 | ||||||
| C-19 Anxiety | −0.06 | −0.14 **** | −0.05 | 0.31 **** | 0.01 | 0.23 **** | |||||
| PHQ-15 (Pain) | 0.07 * | −0.09 ** | −0.08 * | 0.15 **** | 0.19 **** | 0.25 **** | 0.10 ** | ||||
| PHQ-15 (Gastro) | −0.23 **** | −0.15 **** | 0.00 | 0.25 **** | 0.10 ** | 0.35 **** | 0.10 ** | 0.46 **** | |||
| PHQ-15 (Cardio) | −0.09 ** | −0.13 **** | 0.00 | 0.29 **** | 0.19 **** | 0.40 **** | 0.12 *** | 0.43 **** | 0.59 **** | ||
| PHQ-15 (Fatigue) | −0.07 * | −0.13 **** | −0.04 | 0.18 **** | 0.18 **** | 0.31 **** | 0.13 *** | 0.5*** | 0.56 **** | 0.51 **** | |
| PHQ-15 (Total) | −0.08 * | −0.15 **** | −0.04 | 0.24 **** | 0.20 **** | 0.36 **** | 0.12 *** | 0.75 **** | 0.82 **** | 0.71 **** | 0.81 **** |
| Pain | Gastro | Cardio | Fatigue | Total Score | |
|---|---|---|---|---|---|
| Model 1 | |||||
| COVID-19 anxiety | |||||
| Quintile 1 | - | - | - | - | - |
| Quintile 2 | 0.18 | 0.61 ** | 0.33 * | 0.23 * | 1.36 ** |
| Quintile 3 | 0.26 * | 0.91 *** | 0.55 *** | 0.30 ** | 2.03 *** |
| Quintile 4 | 0.26 * | 0.89 *** | 0.53 *** | 0.47 *** | 2.15 *** |
| Quintile 5 | 0.56 *** | 1.20 *** | 0.90 *** | 0.72 *** | 3.40 *** |
| R2 | 0.02 *** | 0.04 *** | 0.03 *** | 0.04 *** | 0.05 *** |
| Model 2 | |||||
| COVID-19 anxiety | |||||
| Quintile 1 | - | - | - | - | - |
| Quintile 2 | 0.13 | 0.42 * | 0.22 | 0.14 | 0.92 * |
| Quintile 3 | 0.12 | 0.46 * | 0.26 | 0.10 | 0.95 * |
| Quintile 4 | 0.08 | 0.37 | 0.19 | 0.23 | 0.87 |
| Quintile 5 | 0.25 * | 0.38 | 0.32 | 0.32 * | 1.27 * |
| Control variables | |||||
| Age | 0.006 ** | −0.01 *** | 0.00 | 0.00 | −0.02 |
| Gender (Male) | −0.18 * | −0.30 * | −0.24 * | −0.20 * | −0.93 ** |
| Income (Max) | −0.12 | 0.08 | 0.10 | 0.00 | 0.04 |
| Health Problem (Yes) | 0.52 *** | 0.63 *** | 0.60 *** | 0.50 *** | 2.27 *** |
| GAD-7 ≥ 10 | 0.75 *** | 1.82 *** | 1.48 *** | 0.87 *** | 4.93 *** |
| Region | |||||
| Lazio | −0.19 | −0.17 | −0.12 | −0.14 | −0.63 |
| Lombardia | −0.21 * | −0.15 | −0.09 | −0.19 | −0.64 |
| Veneto | −0.26 * | −0.38 | −0.19 | −0.18 | −1.03 * |
| Human Losses due to COVID-19 | |||||
| Yes | 0.30 * | 0.71 *** | 0.37 * | 0.41 *** | 1.80 *** |
| Not sure | 0.43 * | 0.34 | 0.09 | 0.34* | 1.21 |
| R2 | 0.14 *** | 0.24 *** | 0.22 *** | 0.18 *** | 0.27 *** |
| n | Anxiety/Depression (n%) | Adjusted OR (95% CI) | |
|---|---|---|---|
| Age | |||
| 1038 | 271 (26.10%) | 0.962 (0.951–0.973) *** | |
| Gender | |||
| Female | 531 | 165 (31.07%) | - |
| Male | 507 | 106 (20.90%) | 0.728 (0.406–1.048) |
| Living Location | |||
| Rural | 49 | 11 (22.45%) | - |
| Town | 297 | 57 (19.19%) | 0.960 (0.162–1.815) |
| Suburb | 123 | 41 (33.33%) | 1.648 (0.796–2.551) |
| City | 569 | 162 (28.47%) | 1.365 (0.592–2.200) |
| Lone Adult | |||
| No | 899 | 238 (26.47%) | - |
| Yes | 139 | 33 (23.74%) | 1.258 (0.759–1.744) |
| Children | |||
| No | 680 | 131 (19.26%) | - |
| Yes | 358 | 140 (39.10%) | 1.552 (1.203–1.902) ** |
| Income | |||
| −15.000 €/yr | 218 | 66 (30.27%) | - |
| −28.000 €/yr | 214 | 50 (23.36%) | 0.709 (0.224–1.189) |
| −55.000 €/yr | 212 | 50 (23.59%) | 0.880 (0.380–1.377) |
| −75.000 €/yr | 211 | 67 (31.75%) | 1.039 (0.543–1.534) |
| +75.000 €/yr | 183 | 38 (20.54%) | 0.559 (0.009–1.100) |
| Pre-Existing Health Condition, Self | |||
| No | 869 | 222 (25.54%) | - |
| Yes | 169 | 49 (29.00%) | 1.356 (0.911–1.813) |
| Pre-Existing Health Condition, Relatives | |||
| No | 811 | 192 (23.67%) | - |
| Yes | 227 | 79 (34.80%) | 1.526 (1.145–1.906) ** |
| Human Losses due to COVID-19 | |||
| No | 888 | 217 (24.43%) | - |
| Yes | 109 | 38 (34.86%) | 1.519 (1.017–2.012) * |
| Not Sure | 41 | 16 (39.02%) | 2.027 (1.267–2.771) ** |
| Region | |||
| Campania | 227 | 65 (28.63%) | - |
| Lazio | 234 | 61 (26.06%) | 0.972 (0.504–1.440) |
| Lombardia | 391 | 94 (24.04%) | 0.728 (0.292–1.165) |
| Veneto | 186 | 51 (27.42%) | 0.912 (0.407–1.414) |
| Personal Risk at 1 Month | |||
| Low | 269 | 33 (12.26%) | - |
| Moderate—Low | 252 | 46 (18.25%) | 1.435 (0.924–1.955) |
| Moderate—High | 261 | 75 (28.73%) | 1.930 (1.453–2.423) *** |
| High | 256 | 117 (45.70%) | 2.565 (2.104–3.047) *** |
| n | C-19 Related Anxiety (n%) | Adjusted OR (95% CI) | |
|---|---|---|---|
| Age | |||
| 1038 | 190 (26.10%) | 1.001 (0.989–1.014) | |
| Gender | |||
| Female | 531 | 126 (23.73%) | - |
| Male | 507 | 64 (12.62%) | 0.336 (−0.028–693) *** |
| Living Location | |||
| Rural | 49 | 5 (10.20%) | - |
| Town | 297 | 62 (20.87%) | 2.111 (1.147–3.265) * |
| Suburb | 123 | 26 (21.14%) | 1.648 (0.796–2.551) |
| City | 569 | 97 (17.04%) | 2.035 (0.994–3.238) |
| Lone Adult | |||
| No | 899 | 170 (18.90%) | - |
| Yes | 139 | 20 (14.38%) | 0.629 (0.051–1.168) |
| Children | |||
| No | 680 | 112 (16.47%) | - |
| Yes | 358 | 78 (21.79%) | 1.001 (1.595–1.402) |
| Income | |||
| −15.000 €/yr | 218 | 51 (23.39%) | - |
| −28.000 €/yr | 214 | 42 (19.62%) | 0.721 (0.214–1.223) |
| −55.000 €/yr | 212 | 28 (13.20%) | 0.219 (−0.353–0.775) |
| −75.000 €/yr | 211 | 33 (15.64%) | 0.389 (−0.171–0.937) |
| +75.000 €/yr | 183 | 36 (19.67%) | 0.949 (0.386–1.507) |
| Pre-Existing Health Condition, Self | |||
| No | 869 | 157 (18.06%) | - |
| Yes | 169 | 33 (19.52%) | 1.015 (0.510–1.501) |
| Pre-Existing Health Condition, Relatives | |||
| No | 811 | 136 (16.77%) | - |
| Yes | 227 | 54 (23.7%) | 1.325 (0.904–1.738) |
| Human Losses due to COVID-19 | |||
| No | 888 | 159 (17.90%) | - |
| Yes | 109 | 23 (21.1%) | 1.099 (0.541–1.628) |
| Not Sure | 41 | 8 (19.51%) | 1.283 (0.355–2.108) |
| Region | |||
| Campania | 227 | 49 (21.58%) | - |
| Lazio | 234 | 42 (17.95%) | 0.913 (0.402–1.421) |
| Lombardia | 391 | 64 (16.37%) | 0.719 (0.250–1.190) |
| Veneto | 186 | 35 (18.81%) | 0.935 (0.390–1.473) |
| Personal Risk at 1 Month | |||
| Low | 269 | 17 (6.32%) | - |
| Moderate–Low | 252 | 33 (13.09%) | 1.747 (1.134–2.392) * |
| Moderate–High | 261 | 43 (16.47%) | 1.956 (1.366–2.585) ** |
| High | 256 | 97 (37.89%) | 3.196 (2.647–3.798) *** |
| n | Traumatic Stress (n%) | Adjusted OR (95% CI) | |
|---|---|---|---|
| Age | |||
| 1038 | 269 (25.91%) | 0.968 (0.957–0.979) *** | |
| Gender | |||
| Female | 531 | 157 (29.56%) | - |
| Male | 507 | 112 (22.09%) | 0.850 (0.532–1.168) |
| Living Location | |||
| Rural | 49 | 13 (26.53%) | - |
| Town | 297 | 59 (19.86%) | 0.670 (−0.092–1.475) |
| Suburb | 123 | 33 (26.83%) | 0.940 (0.109–1.803) |
| City | 569 | 164 (28.82%) | 1.049 (0.312–1.832) |
| Lone Adult | |||
| No | 899 | 236 (26.25%) | - |
| Yes | 139 | 33 (23.74%) | 1.243 (0.749–1.722) |
| Children | |||
| No | 680 | 134 (19.70%) | - |
| Yes | 358 | 135 (37.70%) | 1.520 (1.169–1.87) ** |
| Income | |||
| −15.000 €/yr | 218 | 60 (27.52%) | - |
| −28.000 €/yr | 214 | 52 (24.30%) | 0.906 (0.425–1.386) |
| −55.000 €/yr | 212 | 58 (27.36%) | 1.259 (0.771–1.749) |
| −75.000 €/yr | 211 | 63 (29.85%) | 1.099 (0.600–1.597) |
| +75.000 €/yr | 183 | 36 (19.67%) | 0.657 (0.102–1.203) |
| Pre-Existing Health Condition, Self | |||
| No | 869 | 216 (24.85%) | - |
| Yes | 169 | 53 (31.36%) | 1.587 (1.148–2.023) ** |
| Pre-Existing Health Condition, Relatives | |||
| No | 811 | 197 (24.29%) | - |
| Yes | 227 | 72 (31.71%) | 1.219 (0.836–1.597) |
| Human Losses due to COVID-19 | |||
| No | 888 | 219 (24.66%) | - |
| Yes | 109 | 33 (30.27%) | 1.207 (0.696–1.702) |
| Not Sure | 41 | 17 (41.46%) | 2.130 (1.386–2.886) ** |
| Region | |||
| Campania | 227 | 70 (30.83%) | - |
| Lazio | 234 | 57 (24.36%) | 0.686 (0.223–1.146) |
| Lombardia | 391 | 92 (23.53%) | 0.519 (0.092–946) * |
| Veneto | 186 | 50 (26.88%) | 0.663 (0.168–1.154) |
| Personal Risk at 1 Month | |||
| Low | 269 | 29 (10.78%) | - |
| Moderate–Low | 252 | 51 (20.24%) | 1.782 (1.272–2.307) ** |
| Moderate–High | 261 | 69 (26.43%) | 2.008 (1.519–2.518) *** |
| High | 256 | 120 (46.87%) | 2.815 (2.345–3.310) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bruno, G.; Panzeri, A.; Granziol, U.; Alivernini, F.; Chirico, A.; Galli, F.; Lucidi, F.; Spoto, A.; Vidotto, G.; Bertamini, M. The Italian COVID-19 Psychological Research Consortium (IT C19PRC): General Overview and Replication of the UK Study. J. Clin. Med. 2021, 10, 52. https://doi.org/10.3390/jcm10010052
Bruno G, Panzeri A, Granziol U, Alivernini F, Chirico A, Galli F, Lucidi F, Spoto A, Vidotto G, Bertamini M. The Italian COVID-19 Psychological Research Consortium (IT C19PRC): General Overview and Replication of the UK Study. Journal of Clinical Medicine. 2021; 10(1):52. https://doi.org/10.3390/jcm10010052
Chicago/Turabian StyleBruno, Giovanni, Anna Panzeri, Umberto Granziol, Fabio Alivernini, Andrea Chirico, Federica Galli, Fabio Lucidi, Andrea Spoto, Giulio Vidotto, and Marco Bertamini. 2021. "The Italian COVID-19 Psychological Research Consortium (IT C19PRC): General Overview and Replication of the UK Study" Journal of Clinical Medicine 10, no. 1: 52. https://doi.org/10.3390/jcm10010052