
Antiphospholipid Syndrome-Induced Leriche Syndrome in a Man with Lower Limbs Sensory and Motor Defect

 , , and
, , and
Abstract
:1. Introduction
2. Case Presentation
2.1. Interview
2.2. Physical Examination
2.3. Laboratory Analysis
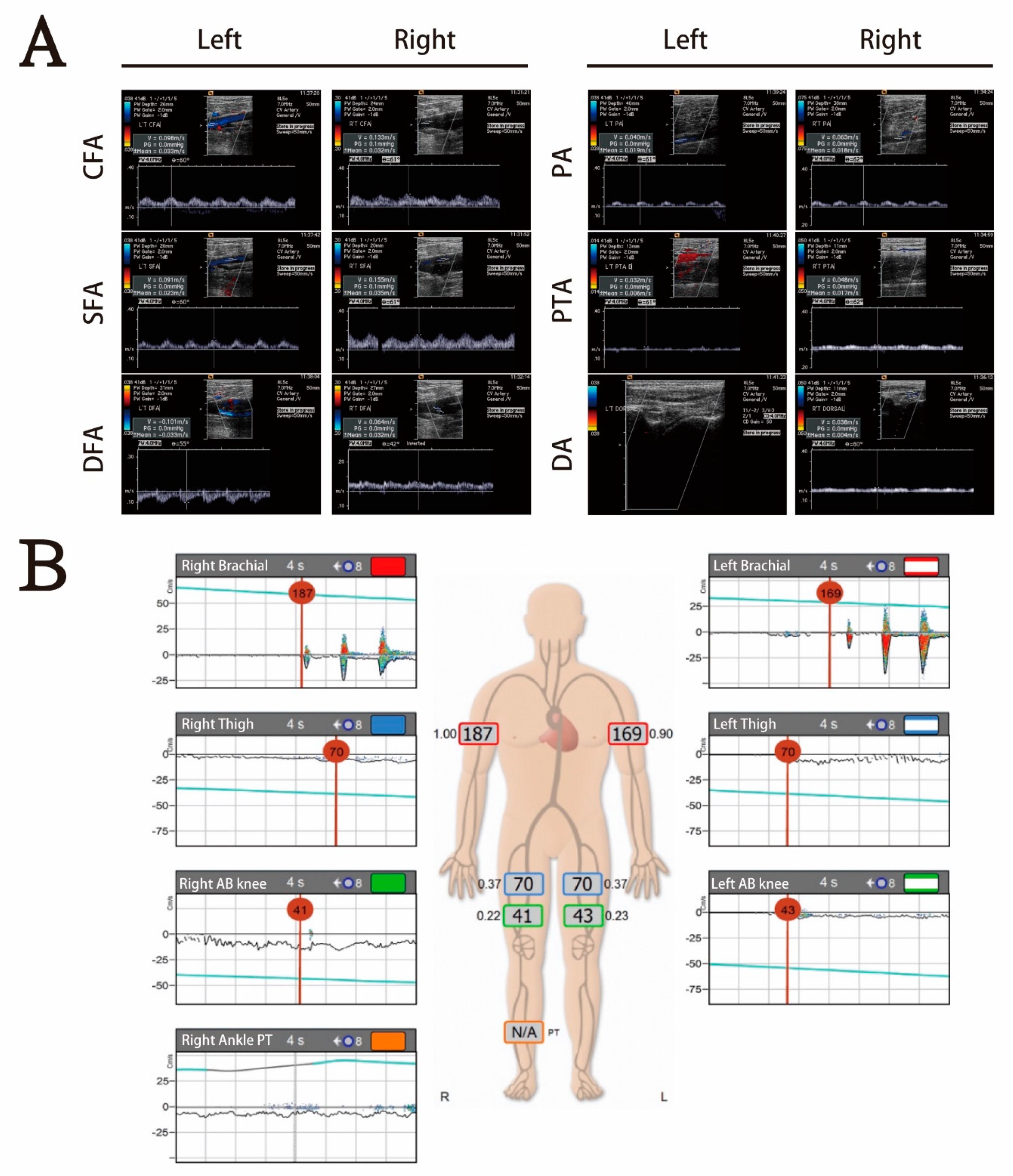
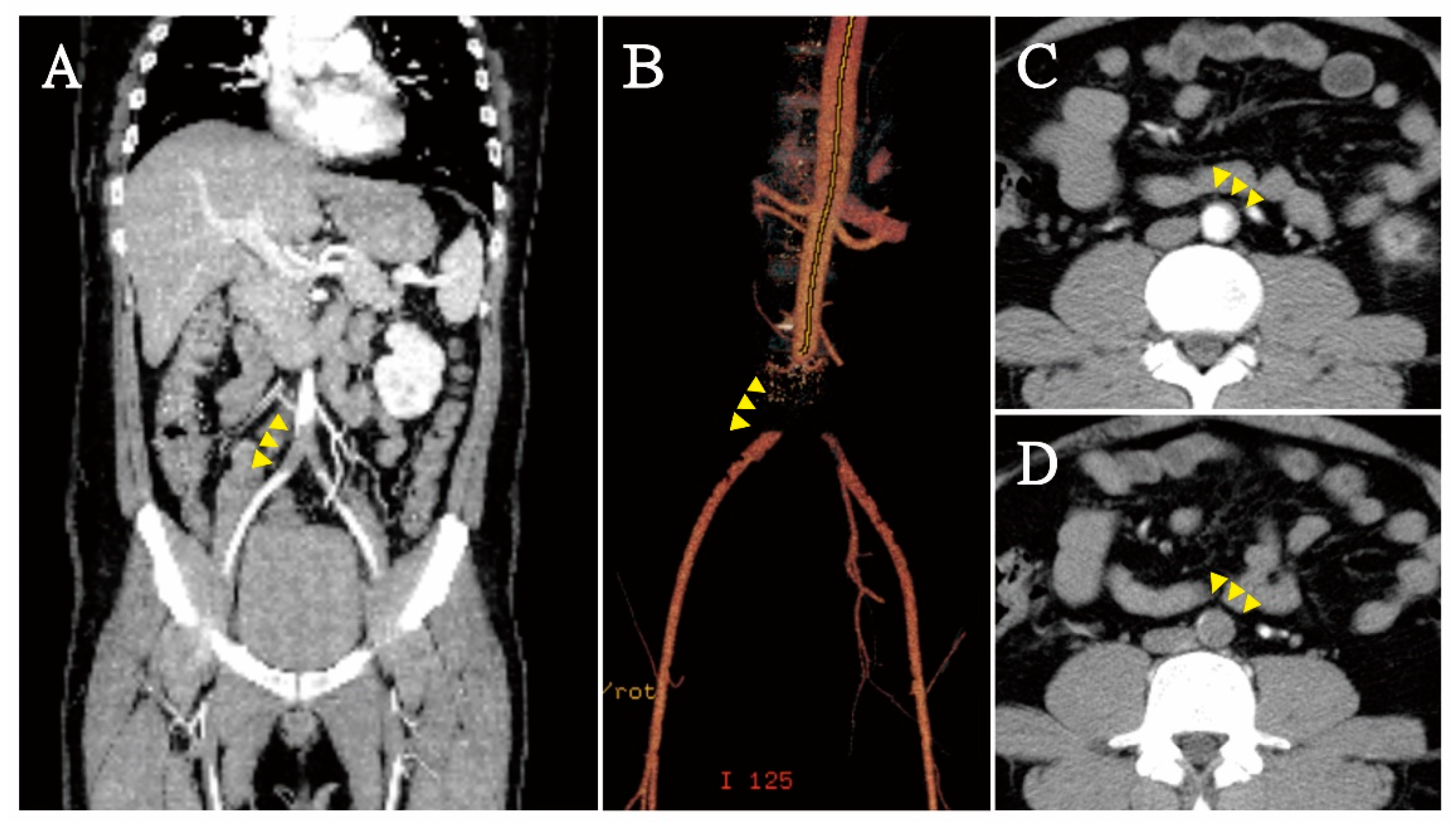
2.4. Imaging Tests
2.5. Diagnosis and Treatment
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mahendrakar, S.M.; Sandhu, H.S.; Khan, A.H.; Loya, Y.S. Leriche Syndrome: Acute Onset Painful Paraplegia of Vascular Origin with Catastrophic Consequences. J. Clin. Diagn. Res. 2017, 11, OD22–OD23. [Google Scholar] [CrossRef]
- Rutherford, R.B.; Baker, J.D.; Ernst, C.; Johnston, K.W.; Porter, J.M.; Ahn, S.; Jones, D.N. Recommended Standards for Reports Dealing with Lower Extremity Ischemia: Revised Version. J. Vasc. Surg. 1997, 26, 517–538. [Google Scholar] [CrossRef] [Green Version]
- Schreiber, K.; Sciascia, S.; De Groot, P.G.; Devreese, K.; Jacobsen, S.; Ruiz-Irastorza, G.; Salmon, J.E.; Shoenfeld, Y.; Shovman, O.; Hunt, B.J. Antiphospholipid Syndrome. Nat. Rev. Dis. Primers 2018, 4, 17103. [Google Scholar] [CrossRef] [PubMed]
- Pengo, V.; Ruffatti, A.; Legnani, C.; Testa, S.; Fierro, T.; Marongiu, F.; de Micheli, V.; Gresele, P.; Tonello, M.; Ghirarduzzi, A.; et al. Incidence of a First Thromboembolic Event in Asymptomatic Carriers of High-Risk Antiphospholipid Antibody Profile: A Multicenter Prospective Study. Blood 2011, 118, 4714–4718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervera, R.; Serrano, R.; Pons-Estel, G.J.; Ceberio-Hualde, L.; Shoenfeld, Y.; de Ramón, E.; Buonaiuto, V.; Jacobsen, S.; Zeher, M.M.; Tarr, T.; et al. Morbidity and Mortality in the Antiphospholipid Syndrome During a 10-Year Period: A Multicentre Prospective Study of 1000 Patients. Ann. Rheum. Dis. 2015, 74, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Sole, K. Mechanisms of Thrombosis in Antiphospholipid Syndrome. Nat. Clin. Pract. Rheumatol. 2006, 2, 176. [Google Scholar] [CrossRef]
- Levy, Y.; Shenkman, B.; Tamarin, I.; Pauzner, R.; Shoenfeld, Y.; Langevitz, P.; Savion, N.; Varon, D. Increased Platelet Deposition on Extracellular Matrix under Flow Conditions in Patients with Antiphospholipid Syndrome Who Experience Thrombotic Events. Arthritis Rheum. 2005, 52, 4011–4017. [Google Scholar] [CrossRef]
- Gezer, S. Antiphospholipid Syndrome. Dis. Mon. 2003, 49, 696–741. [Google Scholar] [CrossRef] [PubMed]
- Cervera, R.; Espinosa, G.; Bucciarelli, S.; Gómez-Puerta, J.A.; Font, J. Lessons from the Catastrophic Antiphospholipid Syndrome (Caps) Registry. Autoimmun. Rev. 2006, 6, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.C.; Oh, D.S.; Lee, H.S.; Kim, S.H.; Park, J.H.; Lee, K.H.; Kim, H.J.; Yang, J.H.; Lee, S.E. Leriche Syndrome Misdiagnosed as Complex Regional Pain Syndrome in a Patient with Neuropathic Pain Caused by a Chip Fracture: A Case Report. Medicina 2021, 57, 486. [Google Scholar] [CrossRef] [PubMed]
- Ulukan, M.O.; Karakaya, A.; Oztas, D.M.; Beyaz, M.O.; Rodoplu, O.; Erdinc, I.; Unal, O.; Dayangac, M.; Turkoglu, H.; Ugurlucan, M. Thoracoabdominal Aortic Aneursym Accompanied by Leriche Syndrome in a Patient with Coronary Artery Disease: Management Strategy in a Single Case Experience. Ann. Vasc. Surg. 2021, 73, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.; Mattsson, G.; Magnusson, P. A Case Report of Acute Leriche Syndrome: Aortoiliac Occlusive Disease Due to Embolization from Left Ventricular Thrombus Caused by Myocarditis. BMC Cardiovasc. Disord. 2021, 21, 220. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, T.C.; Hsueh, P.R.; Yu, F.L.; Jean, S.S.; Chen, F.L.; Ou, T.Y.; Lee, W.S. Co-Occurrence of Leriche Syndrome and Antiphospholipid Syndrome in a Man with Refractory Ulcers of the Lower Limbs. J. Microbiol. Immunol. Infect. 2016, 49, 309–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, K.; Beule, J.; Balzer, J.O.; Coldewey, M.; Munzel, T.; Dippold, W.; Wild, P. A 56-Year-Old Man with Co-Prevalence of Leriche Syndrome and Dilated Cardiomyopathy: Case Report and Review. Wien. Klin. Wochenschr. 2014, 126, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Toffon, A.; Piovesan, R.; Minniti, C.F.; Caruso, O.; Criscenti, P.; Villalta, S.; Cavallo, M. Lower Limb Ischemia: Aortoiliac Thrombosis Related to Antiphospholipid Syndrome (Aps)—Case Report and Review of the Literature. Case Rep. Surg. 2013, 2013, 536971. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Patient Data | Reference Value | |
|---|---|---|---|
| White cell count | 7.8 | -- | 3.5–11 (×109/L) |
| Neutrophil | 72.9 | -- | 40–75% |
| Lymphocyte | 20.0 | -- | 40–45% |
| Monocyte | 4.5 | -- | 2–10% |
| Eosinophil | 2.2 | -- | 1–6% |
| Hemoglobin | 15.0 | -- | 12–16 g/dL |
| Platelet counts | 102 | ↓ | 150,000–400,000/μL |
| PT | 9.5 | -- | 8.0–12.0 s |
| APTT | 29.4 | -- | 23.9–35.5 s |
| INR | 0.93 | -- | |
| FDP D-dimer | 485.04 | -- | 0–500 ng/mL |
| Blood urine nitrogen | 16 | -- | 7–18 mg/dL |
| Creatinine | 0.9 | -- | 0.55–1.02 mg/dL |
| Sodium | 132 | ↓ | 136–145 mmol/L |
| Potassium | 3.5 | -- | 3.5–5.1 mmol/L |
| Glucose | 232 | ↑ | 70–100 mg/dL |
| Alanine aminotransferase | 61 | -- | 16–63 U/L |
| High-sensitive troponin I | 22.3 | ↑ | 0–19 ng/L |
| Lactate | 0.4 | -- | 0.4–2.0 mmol/L |
| C-reactive protein | 8.32 | ↑ | 0–0.33 mg/dL |
| HbA1C | 7.5 | ↑ | 4.0–6.0% |
| Variables | Patient Data | Reference Value | |
|---|---|---|---|
| Anti-cardiolipin IgG | 140 | ↑ | 0–10 GPL U/mL |
| Anti-cardiolipin IgM | 17 | ↑ | 0–10 MPL U/mL |
| Anti-β2 glycoprotein 1 | 102 | ↑ | 0–10 U/mL |
| ANA | Negative | -- | 1:40–1:40 |
| Anti SS-A | 0.4 | -- | 0–10 U/mL |
| Anti SS-B | 0.4 | -- | 0–10 U/mL |
| Anti RNP | 1.4 | -- | 0–10 U/mL |
| Anti Sm | 1.1 | -- | 0–10 U/mL |
| Anti nDNA | 1.2 | -- | 0–15 IU/mL |
| C 4 | 24.2 | -- | 10–40 mg/dL |
| C 3 | 128 | -- | 90–180 mg/dL |
| Lupus AC | -- | ||
| LA 1 (Screening) | 90.6 | ↑ | 31–44 |
| LA 2 (Confirmation) | 39.2 | ↑ | 30–38 |
| LA 1/LA 2 ratio | 1.9 | ↑ | 0.8–1.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, J.-L.; Hou, Y.-T.; Lin, P.-C.; Chen, Y.-L.; Chien, D.-S.; Yiang, G.-T.; Wu, M.-Y. Antiphospholipid Syndrome-Induced Leriche Syndrome in a Man with Lower Limbs Sensory and Motor Defect. J. Cardiovasc. Dev. Dis. 2021, 8, 104. https://doi.org/10.3390/jcdd8090104
Hong J-L, Hou Y-T, Lin P-C, Chen Y-L, Chien D-S, Yiang G-T, Wu M-Y. Antiphospholipid Syndrome-Induced Leriche Syndrome in a Man with Lower Limbs Sensory and Motor Defect. Journal of Cardiovascular Development and Disease. 2021; 8(9):104. https://doi.org/10.3390/jcdd8090104
Chicago/Turabian StyleHong, Jeng-Luen, Yueh-Tseng Hou, Po-Chen Lin, Yu-Long Chen, Da-Sen Chien, Giou-Teng Yiang, and Meng-Yu Wu. 2021. "Antiphospholipid Syndrome-Induced Leriche Syndrome in a Man with Lower Limbs Sensory and Motor Defect" Journal of Cardiovascular Development and Disease 8, no. 9: 104. https://doi.org/10.3390/jcdd8090104