
In Vivo Validation of Restored Chordal Biomechanics After Mitral Ring Annuloplasty in a Rare Ovine Case of Natural Chronic Functional Mitral Regurgitation

 , , ,
, , ,
Abstract
:1. Introduction
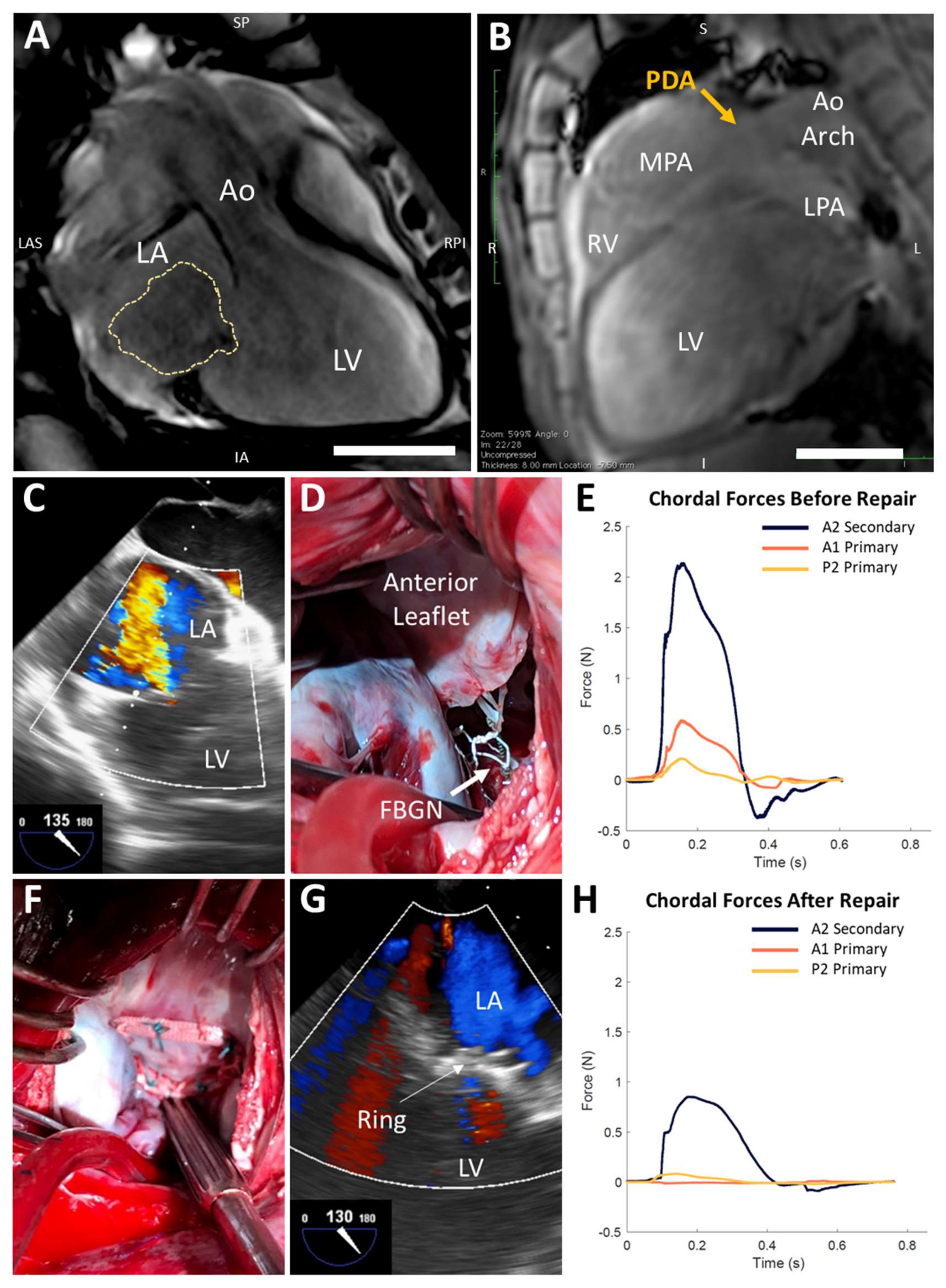
2. Case Report
3. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Imbrie-Moore, A.M.; Paullin, C.C.; Paulsen, M.J.; Grady, F.; Wang, H.; Hironaka, C.E.; Farry, J.M.; Lucian, H.J.; Woo, Y.J. A novel 3D-Printed preferential posterior mitral annular dilation device delineates regurgitation onset threshold in an ex vivo heart simulator. Med Eng. Phys. 2020, 77, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Siefert, A.W.; Rabbah, J.-P.M.; Pierce, E.L.; Kunzelman, K.S.; Yoganathan, A.P. Quantitative Evaluation of Annuloplasty on Mitral Valve Chordae Tendineae Forces to Supplement Surgical Planning Model Development. Cardiovasc. Eng. Technol. 2014, 5, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.L.; Nygaard, H.; Fontaine, A.A.; Hasenkam, J.; He, S.; Andersen, N.T.; Yoganathan, A.P. Chordal force distribution determines systolic mitral leaflet configuration and severity of functional mitral regurgitation. J. Am. Coll. Cardiol. 1999, 33, 843–853. [Google Scholar] [CrossRef] [Green Version]
- Stapleton, L.M.; Steele, A.N.; Wang, H.; Hernandez, H.L.; Yu, A.C.; Paulsen, M.J.; Smith, A.A.A.; Roth, G.A.; Thakore, A.D.; Lucian, H.J.; et al. Use of a supramolecular polymeric hydrogel as an effective post-operative pericardial adhesion barrier. Nat. Biomed. Eng. 2019, 3, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, M.; Bae, J.H.; Imbrie-Moore, A.M.; Wang, H.; Hironaka, C.; Farry, J.; Lucian, H.; Thakore, A.D.; Cutkosky, M.R.; Woo, Y.J. Development and Ex Vivo Validation of Novel Force-Sensing Neochordae for Measuring Chordae Tendineae Tension in the Mitral Valve Apparatus Using Optical Fibers With Embedded Bragg Gratings. J. Biomech. Eng. 2019, 142, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, D.J. The Patent Ductus Arteriosus in Term Infants, Children, and Adults. Semin. Perinatol. 2012, 36, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Chen, T.; Chen, L.; Qin, Y.; Zhao, X. Safety and Efficacy of Transcatheter Closure of Patent Ductus Arteriosus With Severe Mitral Regurgitation in Adults. J. Invasive Cardiol. 2016, 28, 30–33. [Google Scholar] [PubMed]
- Kheiwa, A.; Ross, R.D.; Kobayashi, D. Reversal of severe mitral regurgitation by device closure of a large patent ductus arteriosus in a premature infant. Cardiol. Young 2016, 27, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Halleran, J.L.; Baumwart, R.D.; Dugat, D.R.; Streeter, R.N.; Phillips, H. Surgical ligation of patent ductus arteriosus in a dorper sheep. Veter. Surg. 2018, 48, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Shiota, T.; Jones, M.; Teien, D.E.; Yamada, I.; Passafini, A.; Ge, S.; Sahn, D.J. Dynamic change in mitral regurgitant orifice area: Comparison of color doppler echocardiographic and electromagnetic flowmeter-based methods in a chronic animal model. J. Am. Coll. Cardiol. 1995, 26, 528–536. [Google Scholar] [CrossRef] [Green Version]
- Rankin, J.S.; Nicholas, L.M.; Kouchoukos, N.T. Experimental mitral regurgitation: Effects on left ventricular function before and after elimination of chronic regurgitation in the dog. J. Thorac. Cardiovasc. Surg. 1975, 70, 478–488. [Google Scholar] [CrossRef]
- Gorman, J.H.; Gorman, R.C.; Jackson, B.M.; Enomoto, Y.; John-Sutton, M.G.S.; Edmunds, L.H. Annuloplasty ring selection for chronic ischemic mitral regurgitation: Lessons from the ovine model. Ann. Thorac. Surg. 2003, 76, 1556–1563. [Google Scholar] [CrossRef]
- Paulsen, M.; Imbrie-Moore, A.M.; Wang, H.; Bae, J.H.; Hironaka, C.E.; Farry, J.; Lucian, H.J.; Thakore, A.D.; MacArthur, J.W.; Cutkosky, M.R.; et al. Mitral chordae tendineae force profile characterization using a posterior ventricular anchoring neochordal repair model for mitral regurgitation in a three-dimensional-printed ex vivo left heart simulator. Eur. J. Cardio-Thoracic Surg. 2019, 57, 535–544. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Left Heart Measurements | MR Sheep | Healthy Sheep |
|---|---|---|
| Left Atrium Diameter | 5.26 cm | 2.83 ± 0.24 cm |
| Left Atrium Volume | 229.0 mL | 31.5 ± 8.2 mL |
| Left Ventricle Diameter | 7.94 cm | 4.49 ± 0.30 cm |
| Left Ventricle Volume | 368.9 mL | 103.6 ± 17.9 mL |
| Mitral Annulus Diameter | 5.57 cm | 3.08 ± 0.07 cm |
| Mitral Annulus Area | 24.3 cm2 | 6.7 ± 1.5 cm2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Paulsen, M.J.; Imbrie-Moore, A.M.; Tada, Y.; Bergamasco, H.; Baker, S.W.; Shudo, Y.; Ma, M.; Woo, Y.J. In Vivo Validation of Restored Chordal Biomechanics After Mitral Ring Annuloplasty in a Rare Ovine Case of Natural Chronic Functional Mitral Regurgitation. J. Cardiovasc. Dev. Dis. 2020, 7, 17. https://doi.org/10.3390/jcdd7020017
Wang H, Paulsen MJ, Imbrie-Moore AM, Tada Y, Bergamasco H, Baker SW, Shudo Y, Ma M, Woo YJ. In Vivo Validation of Restored Chordal Biomechanics After Mitral Ring Annuloplasty in a Rare Ovine Case of Natural Chronic Functional Mitral Regurgitation. Journal of Cardiovascular Development and Disease. 2020; 7(2):17. https://doi.org/10.3390/jcdd7020017
Chicago/Turabian StyleWang, Hanjay, Michael J. Paulsen, Annabel M. Imbrie-Moore, Yuko Tada, Hunter Bergamasco, Sam W. Baker, Yasuhiro Shudo, Michael Ma, and Y. Joseph Woo. 2020. "In Vivo Validation of Restored Chordal Biomechanics After Mitral Ring Annuloplasty in a Rare Ovine Case of Natural Chronic Functional Mitral Regurgitation" Journal of Cardiovascular Development and Disease 7, no. 2: 17. https://doi.org/10.3390/jcdd7020017