
Does an eHealth Intervention Reduce Complications and Healthcare Resources? A mHeart Single-Center Randomized-Controlled Trial
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
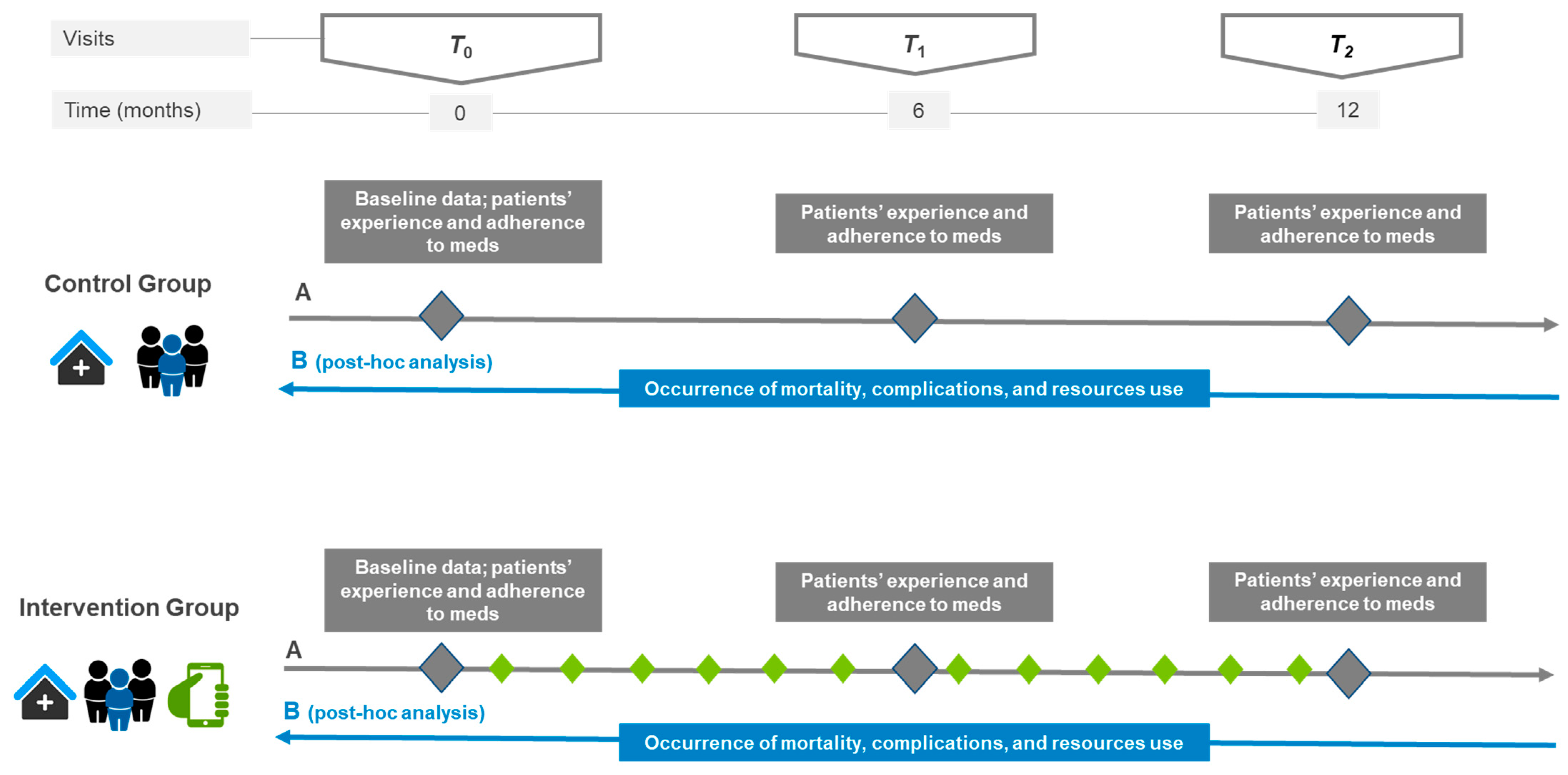
2.1. Trial Design and Ethical Aspects
2.2. Participants
2.3. In-Clinic Visits and Interventions
2.4. Outcomes
2.4.1. Health Outcomes
2.4.2. Use of Resources
2.5. Analysis
2.5.1. Descriptive Analysis
2.5.2. Analysis by Objectives
3. Results
3.1. Patient Description
3.2. Mortality and Complications during Follow-Up in the Overall Population
3.3. Differences in Health Outcomes between Patients on Intervention and the Control Group
3.4. Healthcare Resource Use during Follow-Up in the Overall Population
3.5. Differences in Healthcare Resource Use between Patients in the Intervention and Control Groups
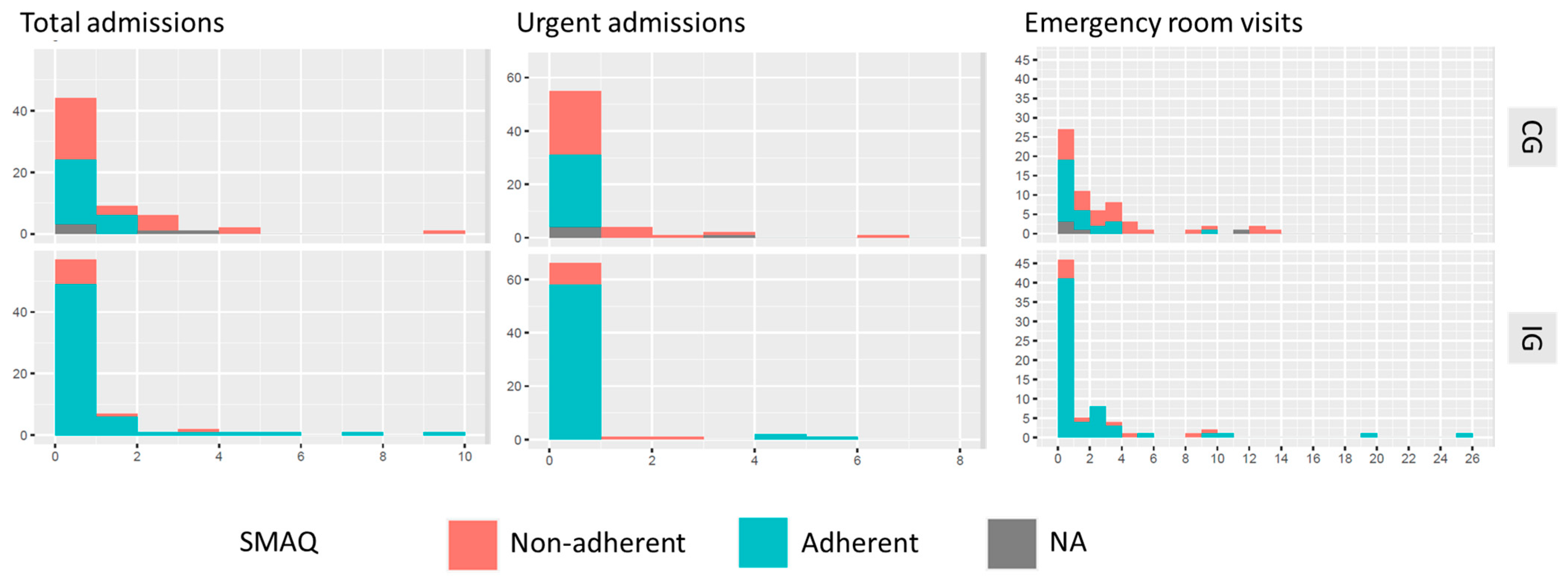
3.6. Differences in Complications and Healthcare Resource Use between Adherent and Non-Adherent Immunosuppressive Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gomis-Pastor, M.; Mingell, E.R.; Perez, S.M.; Loidi, V.B.; Lopez, L.L.; Bassons, A.D.; Pousa, A.A.; Ribera, A.F.; Ferrero-Gregori, A.; Perich, L.G.; et al. Multimorbidity and medication complexity: New challenges in heart transplantation. Clin. Transplant. 2019, 33, e13682. [Google Scholar] [CrossRef]
- Pantuzza, L.L.; Ceccato, M.D.G.B.; Silveira, M.R.; Junqueira, L.M.R.; Reis, A.M.M. Association between medication regimen complexity and pharmacotherapy adherence: A systematic review. Eur. J. Clin. Pharmacol. 2017, 73, 1475–1489. [Google Scholar] [CrossRef]
- Poltronieri, N.V.G.; Moreira, R.S.L.; Schirmer, J.; Roza, B.A. Medication non-adherence in heart transplant patients. Rev. Esc. Enferm. USP 2020, 54, e03644. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhou, H.; Nelson, R.S.; Han, Y.; Wang, Y.; Xiang, H.; Cai, J.; Zhang, J.; Yuan, Y. Prevalence and Risk Factors of Immunosuppressant Nonadherence in Heart Transplant Recipients: A Single-Center Cross-Sectional Study. Patient Prefer. Adherence 2019, 13, 2185–2193. [Google Scholar] [CrossRef] [PubMed]
- De Geest, S.; Abraham, I.; Moons, P.; Vandeputte, M.; Van Cleemput, J.; Evers, G.; Daenen, W.; Vanhaecke, J. Late acute rejection and subclinical noncompliance with cyclosporine therapy in heart transplant recipients. J. Heart Lung Transplant. 1998, 17, 854–863. [Google Scholar]
- Dobbels, F.; De Geest, S.; van Cleemput, J.; Droogne, W.; Vanhaecke, J. Effect of late medication non-compliance on outcome after heart transplantation: A 5-year follow-up. J. Heart Lung Transplant. 2004, 23, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- De Geest, S.; Moons, P.; Dobbels, F.; Martin, S.; Vanhaecke, J. Profiles of patients who experienced a late acute rejection due to nonadherence with immunosuppressive therapy. J. Cardiovasc. Nurs. 2001, 16, 1–14. [Google Scholar] [CrossRef]
- Pinsky, B.W.; Takemoto, S.K.; Lentine, K.L.; Burroughs, T.E.; Schnitzler, M.A.; Salvalaggio, P.R. Transplant Outcomes and Economic Costs Associated with Patient Noncompliance to Immunosuppression. Am. J. Transpl. 2009, 9, 2597–2606. [Google Scholar] [CrossRef]
- Shi, Y.-X.; Liu, C.-X.; Liu, F.; Zhang, H.-M.; Yu, M.-M.; Jin, Y.-H.; Shang, S.-M.; Fu, Y.-X. Efficacy of Adherence-Enhancing Interventions for Immunosuppressive Therapy in Solid Organ Transplant Recipients: A Systematic Review and Meta-Analysis Based on Randomized Controlled Trials. Front. Pharmacol. 2020, 11, 578887. [Google Scholar] [CrossRef]
- Han, A.; Min, S.-I.; Ahn, S.; Min, S.-K.; Hong, H.-J.; Han, N.; Kim, Y.S.; Ahn, C.; Ha, J. Mobile medication manager application to improve adherence with immunosuppressive therapy in renal transplant recipients: A randomized controlled trial. PLoS ONE 2019, 14, e0224595. [Google Scholar] [CrossRef]
- Levine, D.; Torabi, J.; Choinski, K.; Rocca, J.P.; Graham, J.A. Transplant surgery enters a new era: Increasing immunosuppressive medication adherence through mobile apps and smart watches. Am. J. Surg. 2019, 218, 18–20. [Google Scholar] [CrossRef] [PubMed]
- Geramita, E.M.; Dabbs, A.J.D.; DiMartini, A.F.; Pilewski, J.M.; Switzer, G.E.; Posluszny, D.M.; Myaskovsky, L.; Dew, M.A. Impact of a Mobile Health Intervention on Long-term Nonadherence After Lung Transplantation: Follow-up After a Randomized Controlled Trial. Transplantation 2020, 104, 640–651. [Google Scholar] [CrossRef] [PubMed]
- Ritterband, L.M.; Andersson, G.; Christensen, H.M.; Carlbring, P.; Cuijpers, P.; Potts, H.; Van Der Slikke, J.H. Directions for the International Society for Research on Internet Interventions (ISRII). J. Med. Internet Res. 2006, 8, e23. [Google Scholar] [CrossRef] [PubMed]
- Gomis-Pastor, M.; Mirabet, S.; Roig, E.; Lopez, L.; Brossa, V.; Galvez-Tugas, E.; Rodriguez-Murphy, E.; Feliu, A.; Ontiveros, G.; Garcia-Cuyàs, F.; et al. Interdisciplinary Mobile Health Model to Improve Clinical Care After Heart Transplantation: Implementation Strategy Study. JMIR Cardio 2020, 4, e19065. [Google Scholar] [CrossRef]
- Gomis-Pastor, M.; Roig, E.; Mirabet, S.; De Pourcq, J.T.; Conejo, I.; Feliu, A.; Brossa, V.; Lopez, L.; Ferrero-Gregori, A.; Barata, A.; et al. A Mobile App (mHeart) to Detect Medication Nonadherence in the Heart Transplant Population: Validation Study. JMIR mHealth uHealth 2020, 8, e15957. [Google Scholar] [CrossRef]
- Gomis-Pastor, M.; Perez, S.M.; Minguell, E.R.; Loidi, V.B.; Lopez, L.L.; Abarca, S.R.; Tugas, E.G.; Mas-Malagarriga, N.; Bafalluy, M.M. Mobile Health to Improve Adherence and Patient Experience in Heart Transplantation Recipients: The mHeart Trial. Healthcare 2021, 9, 463. [Google Scholar] [CrossRef]
- Eysenbach, G. CONSORT-EHEALTH: Improving and standardizing evaluation reports of Web-based and mobile health in-terventions. J. Med. Internet Res. 2011, 13, e126. [Google Scholar] [CrossRef]
- Clinapsis: Clinical Epidemiology and Healthcare Services. Available online: http://www.clinapsis.com/index.php/auth/login/?l=en (accessed on 5 July 2022).
- Conn, V.S.; Enriquez, M.; Ruppar, T.M.; Chan, K.C. Meta-analyses of Theory Use in Medication Adherence Intervention Research. Am. J. Health Behav. 2016, 40, 155–171. [Google Scholar] [CrossRef]
- Mehra, M.R.; Crespo-Leiro, M.G.; Dipchand, A.; Ensminger, S.M.; Hiemann, N.E.; Kobashigawa, J.A.; Madsen, J.; Parameshwar, J.; Starling, R.C.; Uber, P.A. International Society for Heart and Lung Transplantation working formulation of a standardized nomenclature for cardiac allograft vasculopathy—2010. J. Heart Lung Transplant. 2010, 29, 717–727. [Google Scholar] [CrossRef]
- Public Data Analysis for Health Research and Innovation Program (PADRIS). Available online: https://aquas.gencat.cat/en/ambits/analitica-dades/padris/ (accessed on 5 July 2022).
- Lund, L.H.; Edwards, L.B.; Dipchand, A.I.; Goldfarb, S.; Kucheryavaya, A.Y.; Levvey, B.J.; Meiser, B.; Rossano, J.W.; Yusen, R.D.; Stehlik, J. The Registry of the International Society for Heart and Lung Transplantation: Thirty-third Adult Heart Transplantation Report—2016; Focus Theme: Primary Diagnostic Indications for Transplant. J. Heart Lung Transplant. 2016, 35, 1158–1169. [Google Scholar] [CrossRef]
- Feng, K.Y.; Henricksen, E.J.; Wayda, B.; Moayedi, Y.; Lee, R.; Han, J.; Multani, A.; Yang, W.; Purewal, S.; Puing, A.G.; et al. Impact of diabetes mellitus on clinical outcomes after heart transplantation. Clin. Transplant. 2021, 35, e14460. [Google Scholar] [CrossRef] [PubMed]
- McGillicuddy, J.W.; Gregoski, M.J.; Weiland, A.K.; Rock, R.A.; Brunner-Jackson, B.M.; Patel, S.K.; Thomas, B.S.; Taber, D.J.; Chavin, K.D.; Baliga, P.K.; et al. Mobile Health Medication Adherence and Blood Pressure Control in Renal Transplant Recipients: A Proof-of-Concept Randomized Controlled Trial. JMIR Res. Protoc. 2013, 2, e32. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Singh, A.; Collins, B.; Fatima, A.; Qamar, A.; Gupta, A.; Hainer, J.; Klein, J.; Jarolim, P.; Di Carli, M.; et al. Causes of Troponin Elevation and Associated Mortality in Young Patients. Am. J. Med. 2017, 131, 284–292.e1. [Google Scholar] [CrossRef] [PubMed]
- Dabbs, A.D.; Song, M.K.; Myers, B.A.; Li, R.; Hawkins, R.P.; Pilewski, J.M.; Bermudez, C.A.; Aubrecht, J.; Begey, A.; Connolly, M. A Randomized Controlled Trial of a Mobile Health Intervention to Promote Self-Management After Lung Transplantation. Am. J. Transplant. 2016, 16, 2172–2180. [Google Scholar] [CrossRef] [PubMed]
- Reese, P.P.; Bloom, R.D.; Trofe-Clark, J.; Mussell, A.; Leidy, D.; Levsky, S.; Zhu, J.; Yang, L.; Wang, W.; Troxel, A.; et al. Automated Reminders and Physician Notification to Promote Immunosuppression Adherence Among Kidney Transplant Recipients: A Randomized Trial. Am. J. Kidney Dis. 2017, 69, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Schenkel, F.A.; Barr, M.L.; McCloskey, C.C.; Possemato, T.; O’Conner, J.; Sadeghi, R.; Bembi, M.; Duong, M.; Patel, J.; Hackmann, A.E.; et al. Use of a Bluetooth tablet-based technology to improve outcomes in lung transplantation: A pilot study. Am. J. Transplant. 2020, 20, 3649–3657. [Google Scholar] [CrossRef]
- Tian, M.; Wang, B.; Xue, Z.; Dong, D.; Liu, X.; Wu, R.; Yu, L.; Xiang, J.; Zhang, X.; Zhang, X.; et al. Telemedicine for Follow-up Management of Patients After Liver Transplantation: Cohort Study. JMIR Med. Inform. 2021, 9, e27175. [Google Scholar] [CrossRef]
- Dharnidharka, V.R.; Stablein, D.M.; Harmon, W.E. Post-transplant infections now exceed acute rejection as cause for hospitaliza-tion: A report of the NAPRTCS. Am. J. Transplant. 2004, 4, 384–389. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Num. Cardiovascular Comorbidities | CG Non-Adherent | CG Adherent | IG Non-Adherent | IG Adherent |
|---|---|---|---|---|
| Without comorbidities | 22 | 22 | 8 | 45 |
| 1 | 8 | 2 | 2 | 16 |
| 2 | 0 | 2 | 0 | 0 |
| 3 | 1 | 0 | 0 | 0 |
| 4 | 0 | 1 | 0 | 0 |
| Variables, n/N (%) | IG | CG | All Patients | p Valor |
|---|---|---|---|---|
| Deceased patients | 3/71 (4.2) | 6/63 (9.5) | 9/134 (6.7) | 0.4 |
| Transplant complication | ||||
| Cardiac graft vasculopathy | 39/71 (54.9) | 31/58 (53.4) | 70/129 (54.3) | 1 |
| Revascularization | 7/71 (9.9) | 8/58 (13.8) | 15/129 (11.6) | 0.3 |
| Echocardiographic alteration (LVEF) | 2/71 (2.8) | 8/58 (13.8) | 10/129 (7.8) | 0.02 |
| Cardiovascular events * | 2/568 ± (0.35) | 12/504 ± (2.4) | 14/1072 (1.3) | 0.006 |
| Infections ** | 5/29 (17.2) | 17/30 (56.0) | 22/59 (37.3) | 0.03 |
| Dialysis | 3/71 (4.2) | 3/58 (5.2) | 6/129 (4.7) | 1 |
| Renal dysfunction (GF < 60 mL/min) | 32/71 (45.1) | 30/58 (51.7) | 62/129 (48.1) | 0.3 |
| Analytical endpoints | ||||
| High LDL cholesterol | 3/71 (4.2) | 0/58 (0) | 3/129 (2.3) | 0.2 |
| High Hba1c | 29/71 (40.8) | 34/57 (59.6) | 63/128 (49.2) | 0.03 |
| High triglycerides | 22/71 (40.8) | 21/58 (36.2) | 43/129 (33.3) | 0.3 |
| High hs-cTnT | 34/66 (51.5) | 40/58 (69.0) | 74/124 (59.7) | 0.01 |
| Variables, n/N (%) | IG | CG | All Patients | p Valor |
|---|---|---|---|---|
| Hospital admissions | 23/71 (32.4) | 33/58 (56.9) | 56/129 (43.4) | 0.004 |
| Urgent hospital admissions | 12/71 (16.9) | 24/58 (41.4) | 36/129 (27.9) | 0.002 |
| Emergency room visits | 36/71 (50.7) | 40/58 (69.0) | 76/129 (58.9) | 0.03 |
| Primary care visits | ||||
| Total primary care visits | 62/71 (87.3) | 55/58 (98.4) | 117/129 (90.7) | 0.1 |
| Unscheduled primary care visits | 59/71 (83.1) | 54/58 (93.1) | 113/129 (87.6) | 0.07 |
| Variables, n/N (%) | Adherent | Non-Adherent | All Patients | p Valor |
|---|---|---|---|---|
| Health outcomes | ||||
| Deceased patients | 4/88 (4.5) | 1/41 (2.4) | 5/129 (3.9) | 0.7 |
| Transplant complication | ||||
| Cardiac graft vasculopathy | 52/88 (59.1) | 18/41 (43.9) | 70/129 (54.3) | 0.08 |
| Revascularization | 10/88 (11.4) | 5/41 (12.2) | 15/129 (11.6) | 1 |
| Echocardiographic alteration (LVEF) | 7/88 (8.0) | 3/41 (7.3) | 10/129 (7.8) | 1 |
| Cardiovascular events * | 6/704 ± (0.85) | 8/328 ± (2.4) | 14/1073 (1.3) | 0.04 |
| Infections ** | 9/88 (10.2) | 13/41 (31.7) | 22/129 (17.0) | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomis-Pastor, M.; Mirabet Perez, S.; De Dios Lopez, A.; Brossa Loidi, V.; Lopez Lopez, L.; Pelegrin Cruz, R.; Mangues Bafalluy, M.A. Does an eHealth Intervention Reduce Complications and Healthcare Resources? A mHeart Single-Center Randomized-Controlled Trial. J. Cardiovasc. Dev. Dis. 2023, 10, 77. https://doi.org/10.3390/jcdd10020077
Gomis-Pastor M, Mirabet Perez S, De Dios Lopez A, Brossa Loidi V, Lopez Lopez L, Pelegrin Cruz R, Mangues Bafalluy MA. Does an eHealth Intervention Reduce Complications and Healthcare Resources? A mHeart Single-Center Randomized-Controlled Trial. Journal of Cardiovascular Development and Disease. 2023; 10(2):77. https://doi.org/10.3390/jcdd10020077
Chicago/Turabian StyleGomis-Pastor, Mar, Sonia Mirabet Perez, Anna De Dios Lopez, Vicenç Brossa Loidi, Laura Lopez Lopez, Rebeca Pelegrin Cruz, and Mª Antonia Mangues Bafalluy. 2023. "Does an eHealth Intervention Reduce Complications and Healthcare Resources? A mHeart Single-Center Randomized-Controlled Trial" Journal of Cardiovascular Development and Disease 10, no. 2: 77. https://doi.org/10.3390/jcdd10020077