
Direct Oral Anticoagulants as the First Choice of Anticoagulation for Patients with Peripheral Artery Disease to Prevent Adverse Vascular Events: A Systematic Review and Meta-Analysis

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Data Sources
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Song, P.; Rudan, D.; Zhu, Y.; Fowkes, F.J.I.; Rahimi, K.; Fowkes, F.G.R.; Rudan, I. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: An updated systematic review and analysis. Lancet Glob. Health 2019, 7, e1020–e1030. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498, Erratum in: Eur. J. Intern Med. 2021, 42, 507. Erratum in: Eur. Heart J. 2021, 42, 546–547. Erratum in: Eur. Heart J. 2021, 42, 4194. [Google Scholar]
- Imberti, J.F.; Mei, D.A.; Vitolo, M.; Bonini, N.; Proietti, M.; Potpara, T.; Lip, G.Y.H.; Boriani, G. Comparing atrial fibrillation guidelines: Focus on stroke prevention, bleeding risk assessment and oral anticoagulant recommendations. Eur. J. Intern Med. 2022, 101, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bonanad, C.; Formiga, F.; Anguita, M.; Petidier, R.; Gullón, A. Oral Anticoagulant Use and Appropriateness in Elderly Patients with Atrial Fibrillation in Complex Clinical Conditions: ACONVENIENCE Study. J. Clin. Med. 2022, 11, 7423. [Google Scholar] [CrossRef]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T., Jr.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration with the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar] [CrossRef]
- Griffin, W.F.; Salahuddin, T.; O’Neal, W.T.; Soliman, E.Z. Peripheral arterial disease is associated with an increased risk of atrial fibrillation in the elderly. Europace 2015, 18, 794–798. [Google Scholar] [CrossRef]
- Proietti, M.; Farcomeni, A. Association Between Peripheral Artery Disease and Incident Risk of Atrial Fibrillation: Strong Evidence Coming from Population-Based Cohort Studies. J. Am. Heart. Assoc. 2018, 7, e009126. [Google Scholar] [CrossRef]
- Vitalis, A.; Shantsila, A.; Proietti, M.; Vohra, R.K.; Kay, M.; Olshansky, B.; Lip, G.Y. Peripheral Arterial Disease in Patients with Atrial Fibrillation: The AFFIRM Study. Am. J. Med. 2020, 134, 514–518. [Google Scholar] [CrossRef]
- Vrsalović, M.; Presečki, A.V. Atrial fibrillation and risk of cardiovascular events and mortality in patients with symptomatic peripheral artery disease: A meta-analysis of prospective studies. Clin. Cardiol. 2017, 40, 1231–1235. [Google Scholar] [CrossRef]
- Anandasundaram, B.; Lane, D.A.; Apostolakis, S.; Lip, G.Y.H. The impact of atherosclerotic vascular disease in predicting a stroke, thromboembolism and mortality in atrial fibrillation patients: A systematic review. J. Thromb. Haemost. 2013, 11, 975–987. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.V.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Ave-zum, A.; et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef]
- Lin, Y.-S.; Tung, T.-H.; Wang, J.; Chen, Y.-F.; Chen, T.-H.; Lin, M.-S.; Chi, C.-C.; Chen, M.-C. Peripheral arterial disease and atrial fibrillation and risk of stroke, heart failure hospitalization and cardiovascular death: A nationwide cohort study. Int. J. Cardiol. 2015, 203, 204–211. [Google Scholar] [CrossRef]
- Yu, A.Y.X.; Malo, S.; Svenson, L.W.; Wilton, S.B.; Hill, M.D. Temporal Trends in the Use and Comparative Effectiveness of Direct Oral Anticoagulant Agents Versus Warfarin for Nonvalvular Atrial Fibrillation: A Canadian Population-Based Study. J. Am. Heart Assoc. 2017, 6, e007129. [Google Scholar] [CrossRef]
- Botto, G.; Ameri, P.; De Caterina, R. Many Good Reasons to Switch from Vitamin K Antagonists to Non-Vitamin K Antagonists in Patients with Non-Valvular Atrial Fibrillation. J. Clin. Med. 2021, 10, 2866. [Google Scholar] [CrossRef]
- van Gorp, R.H.; Baaten, C.C.F.M.J.; Habibi, A.; Jaminon, A.M.G.; Peeters, F.E.C.M.; Leenders, P.; Crijns, H.J.G.M.C.; Heemskerk, J.W.M.; Reutelingsperger, C.P.; Spronk, H.M.; et al. Vitamin K antagonist use induces calcification and atherosclerotic plaque progression resulting in increased hypercoagulability. Eur. Heart J. Open 2021, 1, oeab017. [Google Scholar] [CrossRef]
- Beyer, C.; Wildauer, M.; Feuchtner, G.; Friedrich, G.; Hintringer, F.; Stühlinger, M.; Plank, F. Relationship of Anticoagulant Therapies on Coronary Plaque Progression: A Longitudinal CTA Analysis. JACC Cardiovasc. Imaging 2020, 13, 169–170. [Google Scholar] [CrossRef]
- Schroecksnadel, S.; Gostner, J.; Jenny, M.; Kurz, K.; Schennach, H.; Weiss, G.; Fuchs, D. Immunomodulatory effects in vitro of vitamin K antagonist acenocoumarol. Thromb. Res. 2013, 131, e264–e269. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Nakanishi, R.; Li, D.; Shaikh, K.; Shekar, C.; Osawa, K.; Nezarat, N.; Jayawardena, E.; Blanco, M.; Chen, M.; et al. Randomized trial of rivaroxaban versus warfarin in the evaluation of progression of coronary atherosclerosis. Am. Heart J. 2018, 206, 127–130. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Harrer, M.; Cuijpers, P.; Furukawa, T.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide, 1st ed.; Chapman & Hall/CRC Press: New York, NY, USA, 2021. [Google Scholar]
- Viechtbauer, W.; Cheung, M.W.-L. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 1 January 2022).
- Schwarzer, G. Meta: General Package for Meta-Analysis. 2022. Available online: https://github.com/guido-s/meta/ (accessed on 1 January 2022).
- Cuijpers, P.; Furukawa, T.; Ebert, D.D. Dmetar: Companion R Package for the Guide Doing Meta-Analysis in R. 2022. Available online: https://dmetar.protectlab.org (accessed on 1 January 2022).
- Hu, P.T.; Lopes, R.D.; Stevens, S.R.; Wallentin, L.; Thomas, L.; Alexander, J.H.; Hanna, M.; Lewis, B.S.; Verheugt, F.W.A.; Granger, C.B.; et al. Efficacy and Safety of Apixaban Compared with Warfarin in Patients with Atrial Fibrillation and Peripheral Artery Disease: Insights from the ARISTOTLE Trial. J. Am. Heart Assoc. 2017, 6, e004699. [Google Scholar] [CrossRef]
- Jones, W.S.; Hellkamp, A.S.; Halperin, J.L.; Piccini, J.P.; Breithardt, G.; Singer, D.E.; Fox, K.A.; Hankey, G.; Mahaffey, K.W.; Califf, R.M.; et al. Efficacy and safety of rivaroxaban compared with warfarin in patients with peripheral artery disease and non-valvular atrial fibrillation: Insights from ROCKET AF. Eur. Heart J. 2013, 35, 242–249. [Google Scholar] [CrossRef]
- Cunningham, J.; Giugliano, R.; Braunwald, E.; Trevisan, M.; Nordio, F.; Ophuis, T.O.; Bergovec, M.; Mercuri, M.; Ruff, C.; Bonaca, M. EDOXABAN VERSUS WARFARIN IN 841 PATIENTS WITH ATRIAL FIBRILLATION AND PERIPHERAL ARTERIAL DISEASE: INSIGHTS FROM THE ENGAGE AF-TIMI 48 TRIAL. J. Am. Coll. Cardiol. 2016, 67, 2262. [Google Scholar] [CrossRef]
- Aurshina, A.; Kibrik, P.; Eisenberg, J.; Alsheekh, A.; Hingorani, A.; Marks, N.; Ascher, E. Clinical outcomes of direct oral anticoagulants after lower extremity arterial procedures. Vascular 2017, 26, 189–193. [Google Scholar] [CrossRef]
- Baker, W.L.; Beyer-Westendorf, J.; Bunz, T.J.; Eriksson, D.; Meinecke, A.; Sood, N.A.; Coleman, C.I. Effectiveness and safety of rivaroxaban and warfarin for prevention of major adverse cardiovascular or limb events in patients with non-valvular atrial fibrillation and type 2 diabetes. Diabetes Obes. Metab. 2019, 21, 2107–2114. [Google Scholar] [CrossRef]
- Chan, Y.-H.; Lee, H.-F.; Li, P.-R.; Liu, J.-R.; Chao, T.-F.; Wu, L.-S.; Chang, S.-H.; Yeh, Y.-H.; Kuo, C.-T.; See, L.-C.; et al. Effectiveness, safety, and major adverse limb events in atrial fibrillation patients with concomitant diabetes mellitus treated with non-vitamin K antagonist oral anticoagulants. Cardiovasc. Diabetol. 2020, 19, 63. [Google Scholar] [CrossRef]
- Coleman, C.; Baker, W.L.; Meinecke, A.-K.; Eriksson, D.; Martinez, B.K.; Bunz, T.J.; Alberts, M.J. Effectiveness and safety of rivaroxaban vs. warfarin in patients with non-valvular atrial fibrillation and coronary or peripheral artery disease. Eur. Heart J.-Cardiovasc. Pharmacother. 2020, 6, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.; Freixo, C.; Gonçalves, J.; Teixeira, G.; Antunes, I.; Veiga, C.; Mendes, D.; Martins, J.; Almeida, R. Effectiveness and Safety of Rivaroxaban Compared to Acenocumarol after Infrainguinal Surgical Revascularization. Ann. Vasc. Surg. 2019, 55, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-F.; See, L.-C.; Li, P.-R.; Liu, J.-R.; Chao, T.-F.; Chang, S.-H.; Wu, L.-S.; Yeh, Y.-H.; Kuo, C.-T.; Chan, Y.-H.; et al. Non-vitamin K antagonist oral anticoagulants and warfarin in atrial fibrillation patients with concomitant peripheral artery disease. Eur. Hear. J.-Cardiovasc. Pharmacother. 2019, 7, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; Steffel, J.; Di Fusco, M.; Keshishian, A.; Luo, X.; Li, X.; Masseria, C.; Hamilton, M.; Friend, K.; Gupta, K.; et al. Effectiveness and Safety of Anticoagulants in Adults with Non-valvular Atrial Fibrillation and Concomitant Coronary/Peripheral Artery Disease. Am. J. Med. 2018, 131, 1075–1085.e4. [Google Scholar] [CrossRef] [PubMed]
- Obi, A.T.; Thompson, J.R.; Beaulieu, R.J.; Sutzko, D.C.; Osborne, N.; Albright, J.; Gallagher, K.A.; Henke, P.K. Bleeding and thrombotic outcomes associated with postoperative use of direct oral anticoagulants after open peripheral artery bypass procedures. J. Vasc. Surg. 2020, 72, 1996–2005.e4. [Google Scholar] [CrossRef] [PubMed]
- Talukdar, A.; Wang, S.K.; Czosnowski, L.; Mokraoui, N.; Gupta, A.; Fajardo, A.; Dalsing, M.; Motaganahalli, R. Safety and efficacy of rivaroxaban compared with warfarin in patients undergoing peripheral arterial procedures. J. Vasc. Surg. 2017, 66, 1143–1148. [Google Scholar] [CrossRef]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar]
- Zhu, J.; Tan, X.; Zhou, J.Z. Peripheral artery disease and clinical outcomes in patients with atrial fibrillation: A systematic review and meta-analysis. Clin. Cardiol. 2021, 44, 1050–1057. [Google Scholar] [CrossRef]
- Liao, X.-Z.; Fu, Y.-H.; Ma, J.-Y.; Zhu, W.-G.; Yuan, P. Non-Vitamin K Antagonist Oral Anticoagulants Versus Warfarin in Patients with Atrial Fibrillation and Peripheral Artery Disease: A Systematic Review and Meta-Analysis. Cardiovasc. Drugs Ther. 2020, 34, 391–399. [Google Scholar] [CrossRef]
- Pokorney, S.D.; Piccini, J.P.; Stevens, S.R.; Patel, M.R.; Pieper, K.S.; Halperin, J.L.; Breithardt, G.; Singer, D.E.; Hankey, G.J.; Hacke, W.; et al. Cause of Death and Predictors of All-Cause Mortality in Anticoagulated Patients with Nonvalvular Atrial Fibrillation: Data from ROCKET AF. J. Am. Heart Assoc. 2016, 5, e002197. [Google Scholar] [CrossRef] [PubMed]
- Kretschmer, G.; Herbst, F.; Prager, M.; Sautner, T.; Wenzl, E.; Berlakovich, G.A.; Zekert, F.; Marosi, L.; Schemper, M. A decade of oral anticoagulant treatment to maintain autologous vein grafts forfemoropopliteal atherosclerosis. Arch. Surg. 1992, 127, 1112–1115. [Google Scholar] [CrossRef] [PubMed]
- Dutch Bypass Oral anticoagulants or Aspirin (BOA) Study Group. Efficacy of oral anticoagulants compared with aspirin after infrainguinal bypass surgery (The Dutch Bypass Oral Anticoagulants or Aspirin Study): A randomised trial. Lancet 2000, 355, 346–351. [Google Scholar] [CrossRef]
- Eikelboom, J.W.; Connolly, S.J.; Bosch, J.; Dagenais, G.R.; Hart, R.G.; Shestakovska, O.; Diaz, R.; Alings, M.; Lonn, E.M.; Anand, S.S.; et al. Rivaroxaban with or without Aspirin in Stable Cardiovascular Disease. N. Engl. J. Med. 2017, 377, 1319–1330. [Google Scholar] [CrossRef]
- Kaplovitch, E.; Eikelboom, J.W.; Dyal, L.; Aboyans, V.; Abola, M.T.; Verhamme, P.; Avezum, A.; Fox, K.A.; Berkowitz, S.D.; Bangdiwala, S.I.; et al. Rivaroxaban and Aspirin in Patients with Symptomatic Lower Extremity Peripheral Artery Disease: A Subanalysis of the COMPASS Randomized Clinical Trial. JAMA Cardiol. 2021, 6, 21–29. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Bauersachs, R.M.; Anand, S.S.; Debus, E.S.; Nehler, M.R.; Patel, M.R.; Fanelli, F.; Capell, W.H.; Diao, L.; Jaeger, N.; et al. Rivaroxaban in Peripheral Artery Disease after Revascularization. N. Engl. J. Med. 2020, 382, 1994–2004. [Google Scholar] [CrossRef]
- Smith, M.C.; Lazar, A.; Schutzer, R.W.; Patel, V.I.; Bajakian, D. Patient and Procedural Factors Impacting Discharge on New Anticoagulation After Below Knee Arterial Bypass. J. Vasc. Surg. 2020, 72, e221–e223. [Google Scholar] [CrossRef]
- Ingason, A.B.; Hreinsson, J.P.; Ágústsson, A.S.; Lund, S.H.; Rumba, E.; Pálsson, D.A.; Reynisson, I.E.; Guðmundsdóttir, B.R.; Önundarson, P.T.; Björnsson, E.S. Rivaroxaban Is Associated with Higher Rates of Gastrointestinal Bleeding Than Other Direct Oral Anticoagulants: A Nationwide Propensity Score-Weighted Study. Ann. Intern. Med. 2021, 174, 1493–1502. [Google Scholar] [CrossRef]
- Wang, Y.P.; Kehar, R.; Iansavitchene, A.; Lazo-Langner, A. Bleeding Risk in Nonvalvular Atrial Fibrillation Patients Receiving Direct Oral Anticoagulants and Warfarin: A Systematic Review and Meta-Analysis of Observational Studies. TH Open 2020, 04, e145–e152. [Google Scholar] [CrossRef]
- Radadiya, D.; Devani, K.; Brahmbhatt, B.; Reddy, C. Major gastrointestinal bleeding risk with direct oral anticoagulants: Does type and dose matter?—A systematic review and network meta-analysis. Eur. J. Gastroenterol. Hepatol. 2021, 33, e50–e58. [Google Scholar] [CrossRef]
- Almas, T.; Musheer, A.; Ejaz, A.; Shaikh, F.N.; Paracha, A.A.; Raza, F.; Khan, M.S.; Masood, F.; Siddiqui, F.; Raza, S.; et al. Efficacy and safety of direct oral anticoagulants with and without Aspirin: A systematic review and Meta-analysis. IJC Heart Vasc. 2022, 40, 101016. [Google Scholar] [CrossRef]
- Gupta, K.; Trocio, J.; Keshishian, A.; Zhang, Q.; Dina, O.; Mardekian, J.; Nadkarni, A.; Shank, T.C. Effectiveness and safety of direct oral anticoagulants compared to warfarin in treatment naïve non-valvular atrial fibrillation patients in the US Department of defense population. BMC Cardiovasc. Disord. 2019, 19, 142. [Google Scholar] [CrossRef] [Green Version]
- Larsen, T.B.; Skjøth, F.; Nielsen, P.B.; Kjældgaard, J.N.; Lip, G.Y.H. Comparative effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: Propensity weighted nationwide cohort study. BMJ 2016, 353, i3189. [Google Scholar] [CrossRef]
- Yao, X.; Abraham, N.S.; Sangaralingham, L.R.; Bellolio, M.F.; McBane, R.D.; Shah, N.D.; Noseworthy, P.A. Effectiveness and Safety of Dabigatran, Rivaroxaban, and Apixaban Versus Warfarin in Nonvalvular Atrial Fibrillation. J. Am. Heart Assoc. 2016, 5, e003725. [Google Scholar] [CrossRef] [PubMed]
- Adeboyeje, G.; Sylwestrzak, G.; Barron, J.J.; White, J.; Rosenberg, A.; Abarca, J.; Crawford, G.; Redberg, R. Major Bleeding Risk During Anticoagulation with Warfarin, Dabigatran, Apixaban, or Rivaroxaban in Patients with Nonvalvular Atrial Fibrillation. J. Manag. Care Spec. Pharm. 2017, 23, 968–978. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year of Publication | Study Design | Study Population/ Indication for Anticoagualtion | DOAC Type | DOAC Dose | VKA Type (Dosed According to INR Is in Therapeutic Range) | Outcomes |
|---|---|---|---|---|---|---|---|
| Aurshina [33] | 2020 | Retrospective cohort | PAD patients after revascularization | Rivaroxaban, Apixaban, Dabigatran | NI NI NI | Warfarin | Revascularization |
| Baker [34] | 2018 | Retrospective cohort (propensity score matched) | AF patients with PAD | Rivaroxaban | 15/20 mg daily | Warfarin | Major bleeding, MALE |
| Chan * [35] | 2020 | Retrospective cohort (propensity score matched) | AF patients with PAD | Dabigatran, Rivaroxaban, Apixaban, Edoxaban | 110/150 mg twice daily 10/15/20 mg daily 2,5/5 mg twice daily 30/60 mg daily | Warfarin | Major bleeding, MALE |
| Coleman [36] | 2019 | Retrospective cohort (propensity score matched) | AF patients with PAD | Rivaroxaban | 15/20 mg daily | Warfarin | MI, Stroke/SE, Major bleeding, MALE |
| Cunningham [32] | 2016 | RCT (post hoc analysis) | AF patients with PAD | Edoxaban | 30/60 mg | Warfarin | Stroke/SE, Major bleeding, CV-Mortality |
| Ferreira [37] | 2017 | Retrospective cohort | PAD patients after revascularization | Rivaroxaban | 20 mg daily | Warfarin | Mortality, Amputation, Revascularization |
| Hu [30] | 2013 | RCT (post hoc analysis) | AF patients with PAD | Apixaban | 5 mg twice daily | Warfarin | MI, Stroke/SE, Major bleeding, Mortality, CV-Mortality |
| Jones [31] | 2018 | RCT (post hoc analysis) | AF patients with PAD | Rivaroxaban | 15/20 mg daily | Warfarin | MI, Stroke/SE, Major bleeding, Mortality, CV-Mortality |
| Lee ** [38] | 2017 | Retrospective cohort (propensity score matched) | AF patients with PAD | Dabigatran, Rivaroxaban, Apixaban, Edoxaban | 110/150 mg twice daily 10/15/20 mg daily 2,5/5 mg twice daily 30/60 mg daily | Warfarin | MI, Stroke/SE, Major bleeding, Amputation, Revascularization |
| Lopes [39] | 2018 | Retrospective cohort (propensity score matched) | AF patients with PAD | Rivaroxaban, Dabigatran, Apixaban | 10/15/20 mg daily 75/150 mg twice daily 2.5/5 mg twice daily | Warfarin | Stroke/SE, Major bleeding, Mortality |
| Obi [40] | 2018 | Retrospective cohort | PAD patients after revascularization | Not specified | NI | Not specified | Amputation, Revascularization Mortality |
| Talukadar [41] | 2019 | Retrospective cohort | PAD patients after revascularization | Rivaroxaban | NI | Warfarin | Major bleeding, Revascularization |
| First Author | Year of Publication | Age (All) (Years) | DOAC Age (Years) | VKA Age (Years) | MALE (n) | Hypertonia (n) | Diabetes (n) | Ischaemic Heart Disease (n) | Cerebrovascular Disease (n) | Chronic Renal Disease (n) | Antiplatelet Use (n) | Statin Use (n) | DOAC Patient Number (n) | VKA Patient Number (n) | Follow-Up Time (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aurshina [33] | 2017 | NI | 69 ± 11 * | 72 ± 12 * | 61 | 101 | 82 | NI | NI | NI | NI | NI | 23 | 100 | 23 ± 16 * |
| Baker [34] | 2019 | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | 16.8 (7.2–32.4) ** |
| Chan [35] | 2020 | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI |
| Coleman [36] | 2019 | 74 (65–81) ** | NI | NI | 5307 | 7144 | 3819 | 3902 | 913 | 2740 | 2325 | 5314 | 3257 | 5046 | 16.8 (7.2–32.4) ** |
| Cunningham [32] | 2016 | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI | NI |
| Ferreira [37] | 2018 | 64.8 ±NI * | 64.4 ± NI * | 65 ± NI * | 86 | 81 | 65 | 36 | 19 | 29 | 84 | NI | 40 | 69 | 12 |
| Hu [30] | 2017 | 73 (66.5–79) ** | NI | NI | 593 | 813 | 325 | 523 | 295 | NI | 378 | NI | 442 | 442 | 12 |
| Jones [31] | 2013 | 74 (67–79) ** | NI | NI | 606 | 768 | 400 | 289 | 480 | NI | 346 | NI | 401 | 438 | 24.33 (19.2–29.9) ** |
| Lee [38] | 2019 | NI | 77.4 ± 9.7 * | 77.3 ± 9.9 * | 4410 | 7115 | 4090 | 1379 | 1665 | 3226 | NI | 964 | 5768 | 2034 | NI |
| Lopes [39] | 2018 | NI | 78.9 ± 7.5 * | 79 ± 7.5 * | 16,930 | 29,455 | 13,160 | 18,634 | 8327 | 8475 | 8621 | 22,396 | 15,527 | 15,527 | 5–6 |
| NI | 77.8 ± 7.1 * | 78.2 ± 7.3* | 7708 | 13,083 | 6332 | 8393 | 3450 | 3305 | 3370 | 9503 | 6962 | 6962 | 5–6 | ||
| NI | 78.3 ± 7.4 * | 78.5 ± 7.4 * | 28,440 | 48,845 | 22,300 | 31,101 | 13,044 | 13,054 | 12,811 | 35,699 | 25,903 | 25,903 | 5–6 | ||
| Obi [40] | 2020 | NI | 66.5 (57.5–74.4) ** | 65.4 (58–73) ** | 1329 | 1773 | 811 | 1044 | 564 | 79 | 1634 | NI | 1379 | 618 | 12 |
| Talukadar [41] | 2017 | NI | 60.5 ± 15 * | 63.8 ± 14 * | 59 | NI | 28 | NI | 5 | NI | 78 | NI | 44 | 50 | NI |
| Outcome | Study Numbers and Type | Number of Patients Involved | Relative Effect (95% CI) | Quality (GRADEpro) | Comments |
|---|---|---|---|---|---|
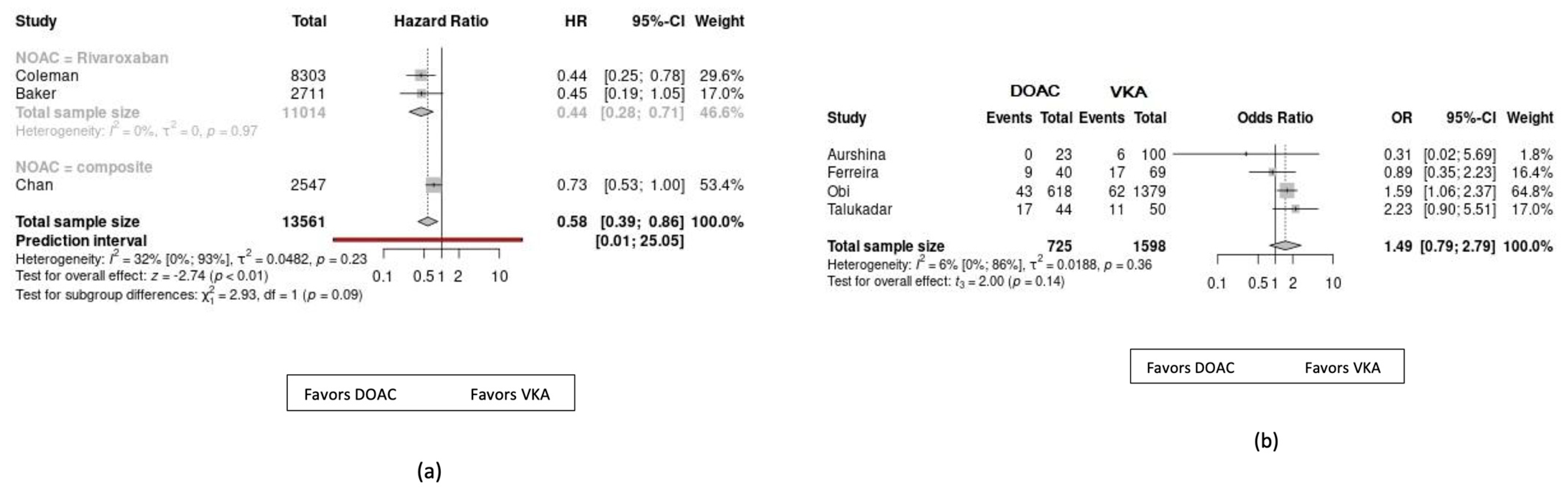
| MALE | 3 Cohorts | 13,561 | HR = 0.58; (0.39–0.86); p < 0.01 | ⨁⨁⨁⨁ High | Composite outcome of reoperation and amputation |
| Need for revascularization | 4 Cohorts | 2323 | OR = 1.49; (0.79–2.79); p = 0.14 | ⨁⨁ Low | The outcome was observed in PAD patients who were prescribed anticoagulants after arterial revascularization procedure |
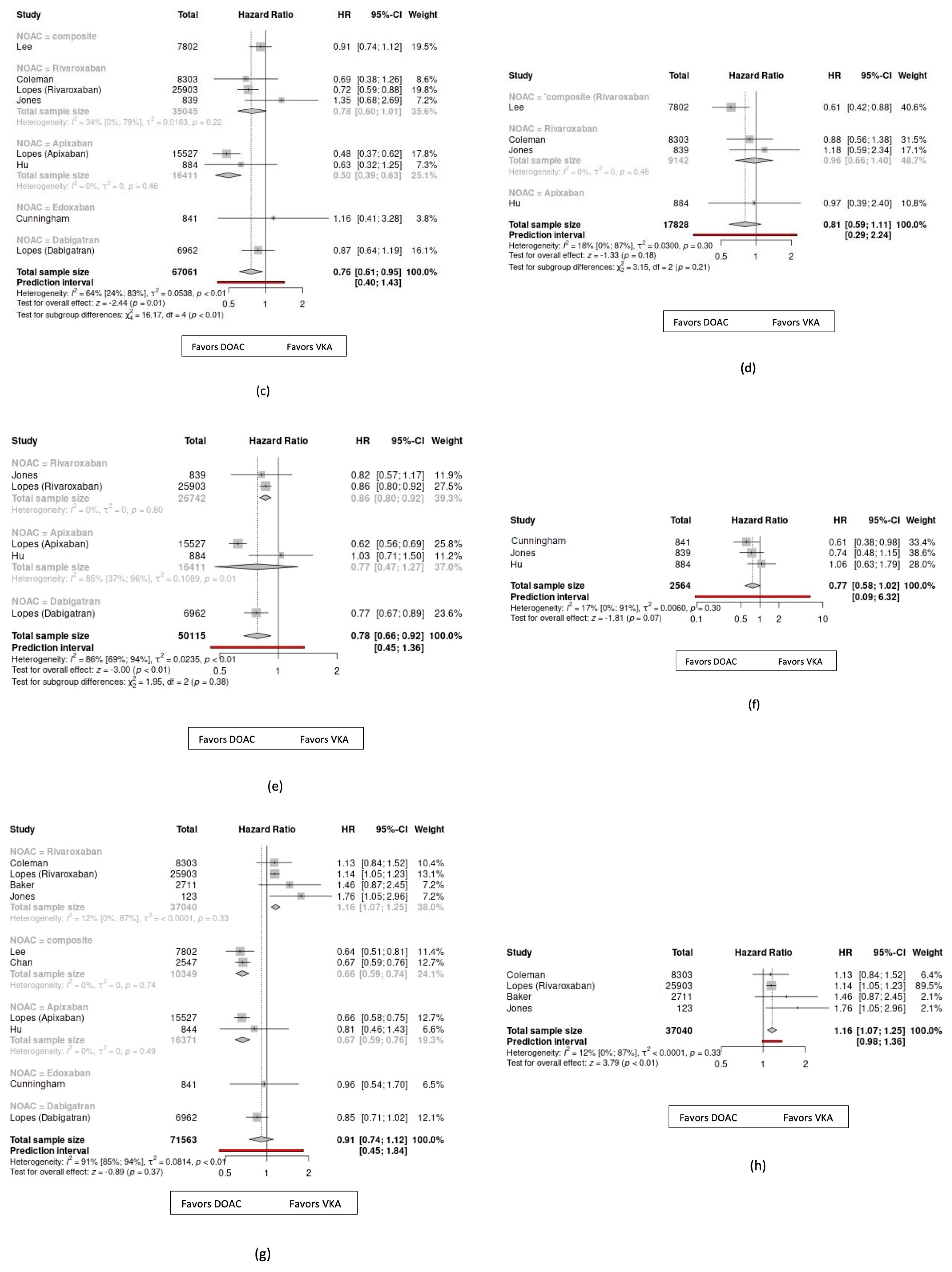
| Myocardial infarction | 3 RCTs | 17,828 | HR = 0.81; (0.59–1.11); p = 0.21 | ⨁⨁⨁⨁ High | |
| Stroke/systemic embolism | 3 RCTs 3 Cohorts | 67,061 | HR = 0.76; (0.61–0.95); p < 0.01 | ⨁⨁⨁ Moderate | |
| All-cause mortality | 2 RCTs 1 Cohorts | 50,115 | HR = 0.78; (0.66–0.92); p < 0.01 | ⨁⨁⨁ Moderate | |
| Cardiovascular mortality | 3 RCTs | 2564 | HR = 0.77; (0.58–1.02); p = 0.07 | ⨁⨁⨁⨁ High | |
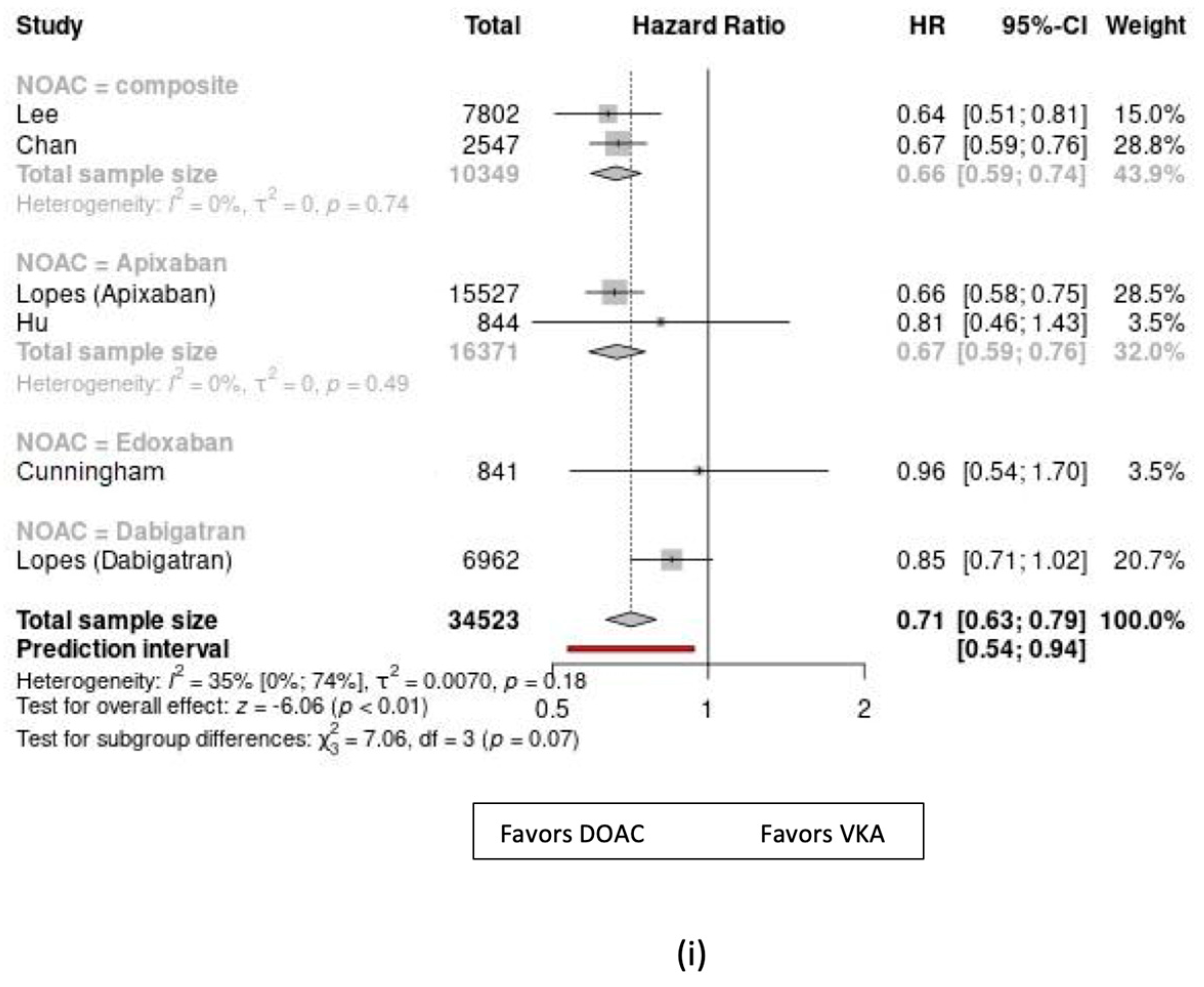
| Major bleeding | 3 RCTs 5 Cohorts | 71,563 | HR = 0.91; (0.74–1.12); p < 0.01 | ⨁⨁⨁⨁ High | The outcome was observed with high-dose Rivaroxaban (10/20 mg daily) in 34,523 patients (HR = 1.16, 1.07–1.25, p < 0.01); and with other NOAC and low-dose Rivaroxaban (2.5 or 5 mg daily) in 37,040 patients - (HR = 0.71, 0.63–0.79, p < 0.01) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomozi, E.; Nagy, R.; Fehérvári, P.; Hegyi, P.; Kiss, B.; Dembrovszky, F.; Kosztin, A.; Nardai, S.; Zima, E.; Szeberin, Z. Direct Oral Anticoagulants as the First Choice of Anticoagulation for Patients with Peripheral Artery Disease to Prevent Adverse Vascular Events: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2023, 10, 65. https://doi.org/10.3390/jcdd10020065
Pomozi E, Nagy R, Fehérvári P, Hegyi P, Kiss B, Dembrovszky F, Kosztin A, Nardai S, Zima E, Szeberin Z. Direct Oral Anticoagulants as the First Choice of Anticoagulation for Patients with Peripheral Artery Disease to Prevent Adverse Vascular Events: A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2023; 10(2):65. https://doi.org/10.3390/jcdd10020065
Chicago/Turabian StylePomozi, Enikő, Rita Nagy, Péter Fehérvári, Péter Hegyi, Boldizsár Kiss, Fanni Dembrovszky, Annamária Kosztin, Sándor Nardai, Endre Zima, and Zoltán Szeberin. 2023. "Direct Oral Anticoagulants as the First Choice of Anticoagulation for Patients with Peripheral Artery Disease to Prevent Adverse Vascular Events: A Systematic Review and Meta-Analysis" Journal of Cardiovascular Development and Disease 10, no. 2: 65. https://doi.org/10.3390/jcdd10020065