

Poor Compliance of Diabetic Patients with AI-Enabled E-Health Self-Care Management in Saudi Arabia


1
Faculty of Engineering and Information Technology, University of Technology Sydney, Sydney, NSW 2007, Australia
2
Faculty of Computer and Information Systems, Islamic University of Madinah, Medina 42351, Saudi Arabia
3
Department of Information Science, College of Computer and Information Systems, Umm Al-Qura University, Makkah 24382, Saudi Arabia
*
Author to whom correspondence should be addressed.
Information 2022, 13(11), 509; https://doi.org/10.3390/info13110509
Submission received: 29 August 2022
/
Revised: 10 October 2022
/
Accepted: 18 October 2022
/
Published: 25 October 2022
(This article belongs to the Special Issue Data Science in Health Services)
Abstract
:Still in its nascent stage, the Kingdom of Saudi Arabia’s self-care system lacks most features of a state-of-the-art e-health care system. With the Industrial Revolution 4.0 and the expanding use of artificial intelligence (AI), e-health initiatives in Saudi Arabia are increasing, which is compelling academics, clinicians, and policymakers to develop a better understanding of e-health trends, their efficacy, and their high impact areas. An increase in the number of diabetic patients in the Kingdom demands improvements to the current e-health care system, where the capability to manage diabetic patients is still in its infancy. In this survey, a total of 210 valid responses were obtained for analysis. SPSS version 27.0 was used for the quantitative analysis. The main technique used to address the aims of the data analysis was Spearman’s correlation analysis. This study indicated that the compliance rate with prescribed medication, blood glucose monitoring, and insulin injections from hospitals is increasing, with the highest rates found for Jeddah City. However, diet control and physical activity compliance levels were found to be poorly combined, predominantly due to the lower number of registered patients in the e-health care system. This non-compliance trends with selected variables (education and income) and highlights the dire need for improvement to the current health system by the inclusion of the latest technology, including big data, cloud computing, and the Internet of Things (IoT). Hence, this study suggests the implementation of government-regulated e-health care systems on mobile-based policies. The study revealed the experience of patients using e-health systems, which could be used to improve their efficacy and durability. More research needs to be conducted to address the deficiencies in the current e-health care system regarding diabetes care, and how it can be integrated into the healthcare system in general.
Keywords:
diabetes; self-care; e-health; Saudi Arabia; big data; cloud computing; internet of things1. Introduction
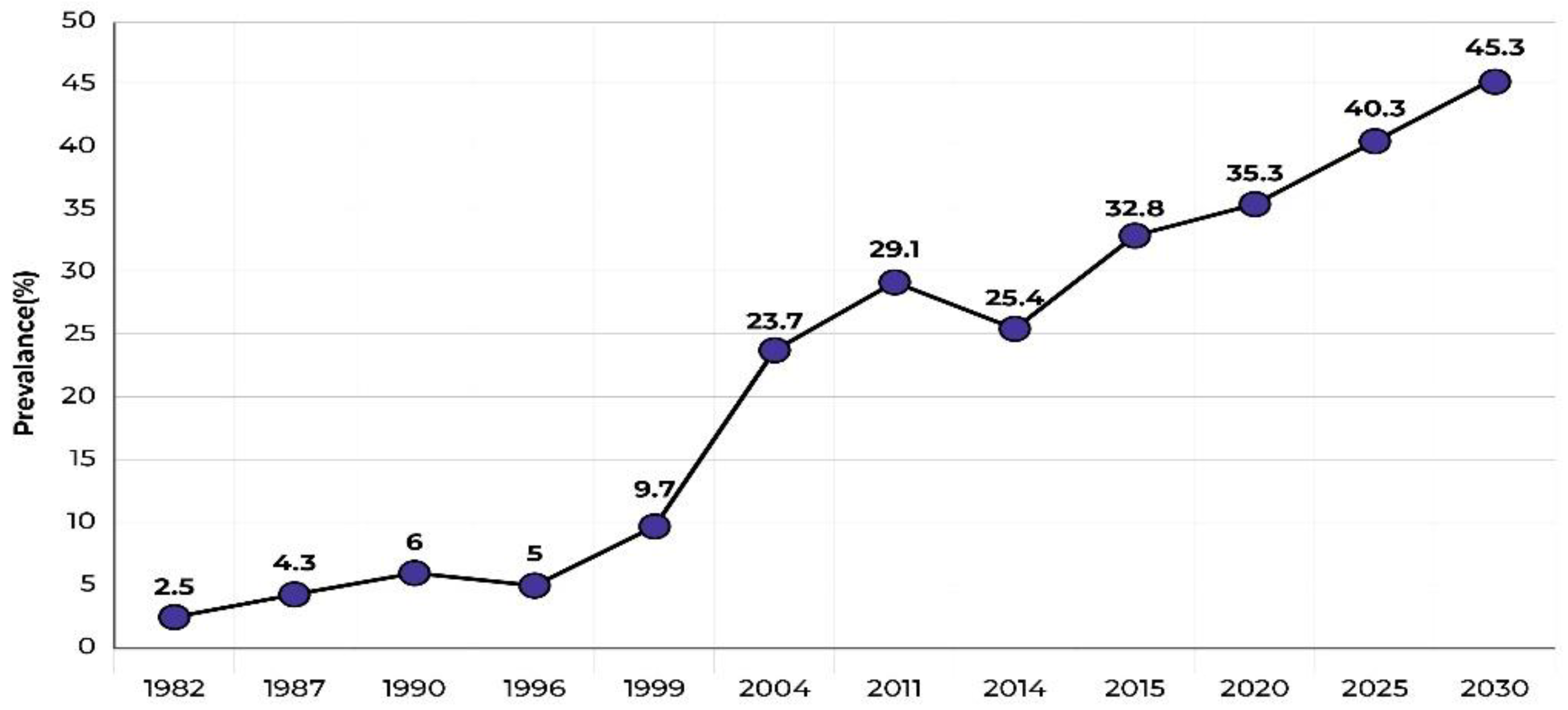
According to the International Diabetes Federation (IDF) [1], in 2021, there were approximately 537 million adult diabetic patients (20–79 years) globally, representing a prevalence rate of 10.5%. This number is expected to reach 783 million by 2045, increasing the prevalence rate to 12.2%. In the Kingdom of Saudi Arabia, approximately 4.3 million people aged 20–79 years had diabetes in 2021, which represents a 17.7% prevalence rate. Additionally, it is estimated that there are nearly 1.3 million undiagnosed diabetic persons in the country, including approximately 27,884 children and adolescents. According to the IDF [1], the prevalence rate in Saudi Arabia is expected to double by 2045 (see Figure 1).
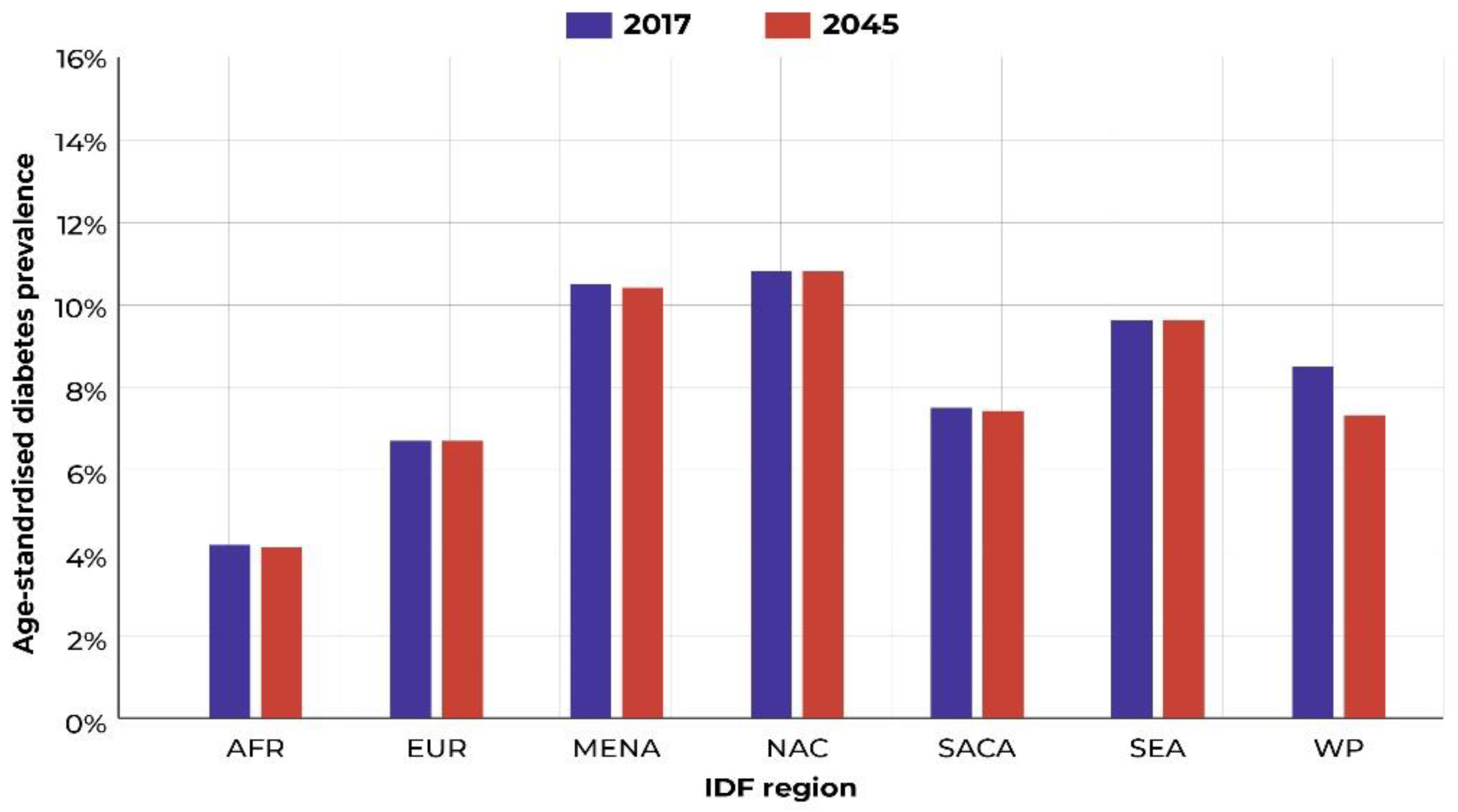
While no country-wide report is available for the Middle East and North Africa (MENA) region, which includes Saudi Arabia, the age-adjusted prevalence rate is expected to increase from 18.1% in 2021 to 20.5% by 2045. With a current rate of 17.7% in Saudi Arabia, the impact could be much higher (see Figure 2).
The healthcare burden of the nation is also expected to rise considerably, thus diverting funds from economic development. Therefore, it is essential to implement strategies to reduce the prevalence of diabetes and prevent any further increases. Information technology (IT)-based e-health self-management may be one of the solutions to this problem, and it can be used in healthcare applications such as electronic patient records (EPRs), self-management of chronic diseases, and providing remote communities with accessibility to healthcare (telemedicine). The World Health Organization (WHO, Geneva, Switzerland) [3] defines e-health as “the use of information and communication technologies (ICT) for health”. Eysenbach [4] defines e-health as “an emerging field in the intersection of medical informatics, public health, and business, referring to health services and information delivered or enhanced through the Internet and related technologies. In a broader sense, the term characterizes not only a technical development, but also a state-of-mind, a way of thinking, an attitude, and a commitment for networked, global thinking, to improve health care regionally, and worldwide by using information and communication technology”.
An e-health system has many advantages, including increased efficiency of care and cost reduction, as well as saving on lost labour productivity and labour markets [5], and the dual advantage of enabling health and care delivery [6]. In the context of treating patients with diabetes, e-health will allow for easier interventions in diet control and physical activity to maintain weight at a personal level, with better checks by physicians [7].
Despite these advantages, the achievements of e-health have been modest due to certain barriers, especially those pertaining to access [8]. These barriers have been attributed to the failure to incorporate a holistic approach [9], lack of interoperability [10,11], lack of integration [10], lack of a business approach [12,13], lack of standards [14], insufficient understanding of end-user needs [15], faulty maintenance of the system [16,17,18], and privacy and security issues related to moving patient electronic health records (EHRs) to a cloud infrastructure [18,19]. The challenges of e-health have resulted in a low level of end-user acceptance, difficulty in integrating e-health with other health systems, difficulty in catering for diverse types of users, inadequate feedback to developers, low levels of sustainable adoption and, consequently, a lack of success [20] and the possibility of some e-health applications being harmful to patients [21].
The WHO ranks Saudi Arabia seventh globally and second in the Middle East for the Diabetes Patient Prevalence Index. An estimated seven million Saudis are already diabetic [22]. The alarming increase in the number of diabetic patients in Saudi Arabia is of great concern, with the number increasing drastically over the past 30 years. Moreover, diabetes management in Saudi Arabia faces immense challenges, including an increasing prevalence among young adults and even children, macro and microvascular complications, delays in diagnosis, and a lack of awareness. Another study revealed the compliance and non-compliance of diabetic patients in Saudi Arabia depending upon the duration of medication, hypertension, and education level of patients, as well as psychological factors. The predominant factors for non-compliance were anti-diabetic treatment, long-term and multi-drug treatment, lower education level, hypertension, and non-adherence to an exercise and diet regimen [23]. Non-compliance with multi-drug regimens is higher, while greater compliance towards dietary instructions than exercise was observed (64.66%), which was higher in Alexandria, Egypt, and Palestine, whereas the compliance rate to an exercise regime was lower in Egypt (51.7%) [2].
Therefore, a complete and inclusive government-regulated nationwide approach to treating diabetes is required. This study proposed the enhanced adaptation of an automated system to create easy check-up mechanisms, along with timely delivery of medication. To accomplish this, the proposed study suggests the implementation of a government-regulated e-health care system on mobile-based policies that utilises the latest technologies, such as big data, cloud computing, and the Internet of Things (IoT).
In the context of Saudi Arabia, the e-health system is currently limited to creating silos of health records and some service facilitations for self-care systems. On the research side, there have been a few scoping works related to e-health [2,21]. No published e-health model for self-care for Saudi diabetes patients is currently available. This paper reports the results of a quantitative survey study conducted as part of the project. This survey was conducted as an initial assessment of the compliance levels of self-managed diabetic patients regarding the medical advice given to them.
2. Literature Survey
Several studies conducted by Alanzi [24] showed that young people are inclined towards the usage of mobile technologies and social networking for the self-management of diabetes. Similar claims were made by Alotaibi [25], who developed a mobile application called SAED for the self-management of young diabetic patients. The application was validated based on it effectively reducing patients’ HbA1C levels in a pilot study conducted by Alotaibi [26]. E-health, when mediated by smartphones to facilitate the self-management of chronic problems [27], is known as m-health [28]. There has been growth in the usage of mobile phone technologies and applications developed for tracking healthcare as part of m-health, which was previously known as e-health [29,30]. The involvement of mobile technologies such as smartphones, tablets, and PDAs in healthcare has drastically improved health practices [31]. Having a centralised healthcare system has helped patients customise their health services [32]. This helps them to access treatment, prescriptions, consultations, and their health status easily. This new system of healthcare has many benefits in comparison to traditional health services; however, despite these benefits, people in Saudi Arabia and its cities remain unsure of its significance. Out of all people who were asked, only 46% had healthcare applications on their phones [33,34]. Although the survey by Atallah [35] was conducted only on a small group of people, the results showed that the usage of m-health applications is currently very low.
The lack of knowledge about m-health has a negative effect on Saudi healthcare. The government needs to educate all stakeholders (patients and healthcare practitioners) about the usefulness and importance of m-health. The government should also enforce the use of technology in all healthcare domains, since some fields, such as cardiovascular diseases and mental healthcare, have neglected the role of technology completely [36]. To effectively manage diabetes, patients need to have a working knowledge of technology and systems. Patients need to be taught self-reliance so that they can manage their diabetes on their own without the need to use public healthcare or attend hospitals frequently. Patients must keep track of tasks, such as monitoring blood sugar (glucose) levels and administering insulin or other medications, which can be accomplished more easily when an application is tracking the patient’s treatment [37,38]. Saad [39] demonstrated that self-care practices were effective in this context.
The process of making appointments at a clinic, purchasing drugs, and visiting hospitals for consultations is currently being conducted manually in Saudi Arabia, resulting in increased healthcare expenditure [40]. Additionally, patients with chronic diseases such as diabetes must visit health centres for treatment in person, unlike in countries such as the United States (US), which offer consultations and assistance virtually, as well as in person. The use of technology for self-care management could decrease the rate of mortality and increase the standard of healthcare. The use of mobile technologies offers an inexpensive way to share information with doctors and healthcare providers [41]. It also increases the possibility of behaviour tracking and follow-up in real time by using the geographic location feature of smart devices. Based on the experiences of developed countries, such as the US and Australia, e-health or m-health apps can be declared valid tools for diabetes self-management, since the US government has already approved the use of such applications [42].
The clinical decision support system (CDSS) significantly improves the overall process of self-care and patient outcomes (20%) [43]. For verified results and medication error prevention, reliable evidence based on the impact of the CDSS on patient self-care is required. This reporting inefficiency can be overcome with the inclusion of patient feedback on outcome indicators and educational information, combined with case management, which seems to be the most effective strategy (i.e., the chronic care model) [44].
3. Artificial Intelligence and Self Compliance in Diabetic Patients
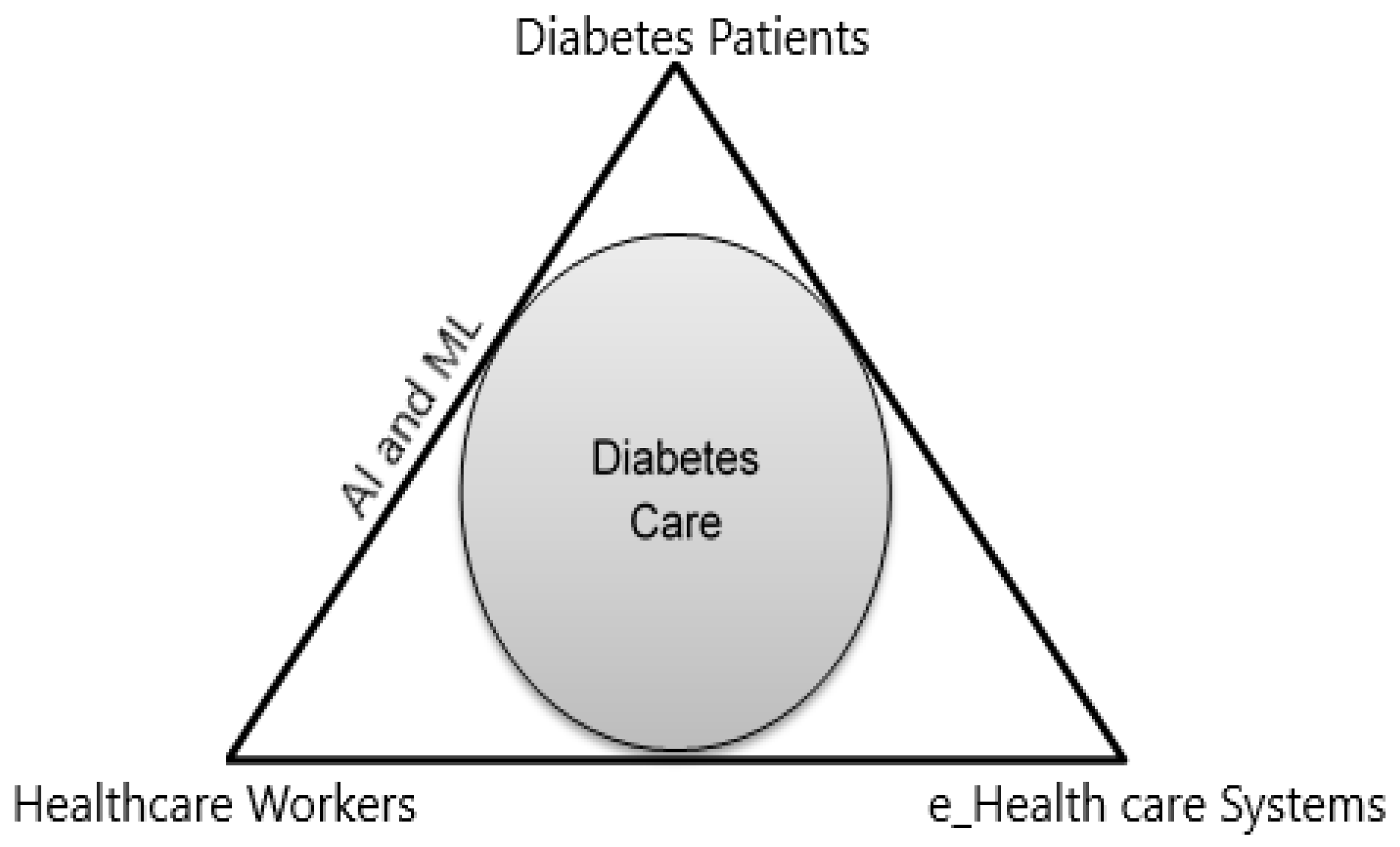
Artificial intelligence (AI) has a variety of applications in e-health and is gradually changing the dimensions of medical practice. Machine learning (ML) can also help healthcare organisations meet growing medical demands, improve operations, and lower costs. With the introduction of the latest methods of data acquisition, AI applications have been utilised in areas that were ignored earlier. Since ML derives patterns from the given data, these innovations can help healthcare practitioners detect and treat diseases more efficiently and with more precision and personalised care for patients [45]. Since AI mimics human cognitive functions, it has brought a paradigm shift to the healthcare sector because of the progress in analytics techniques [46]. In recent times, since AI has been embedded into devices such as smartwatches, it has proved to be of great help in tracking medical conditions via blood pressure, heart rate, and oxygen levels. In diabetic patients, such devices help monitor the heart rate, thus assisting in avoiding coronary artery disease. Diabetic patients are more prone to heart disease, such as heart attacks or stroke, and require constant monitoring [46]. AI can potentially affect and improve three major dimensions of diabetes care: e-health care systems, health workers, and diabetes patients (see Figure 3).
Another important aspect of self-care in diabetes management is exercise. AI can help patents meet their exercise requirements, since AI in devices such as smartwatches can count the number of steps walked or miles run. Appropriate hours of sleep are important for diabetic patients, and a feature of all wearable devices is the ability to track sleep cycles. Making smart use of AI, a diabetic patient can track his or her calorie intake and eating habits and follow meal plans, which are otherwise very difficult to manage [47].
Applying the theory of preventive care and easy disease detection, the implementation of AI in healthcare is cost-effective because it helps patients detect potential hazards sooner, and thus reduces patients’ overall healthcare expenditure. A diabetic patient can improve his or her health condition by implementing AI in his or her healthcare schedule [47].
4. Levels of Practice in Self-Management
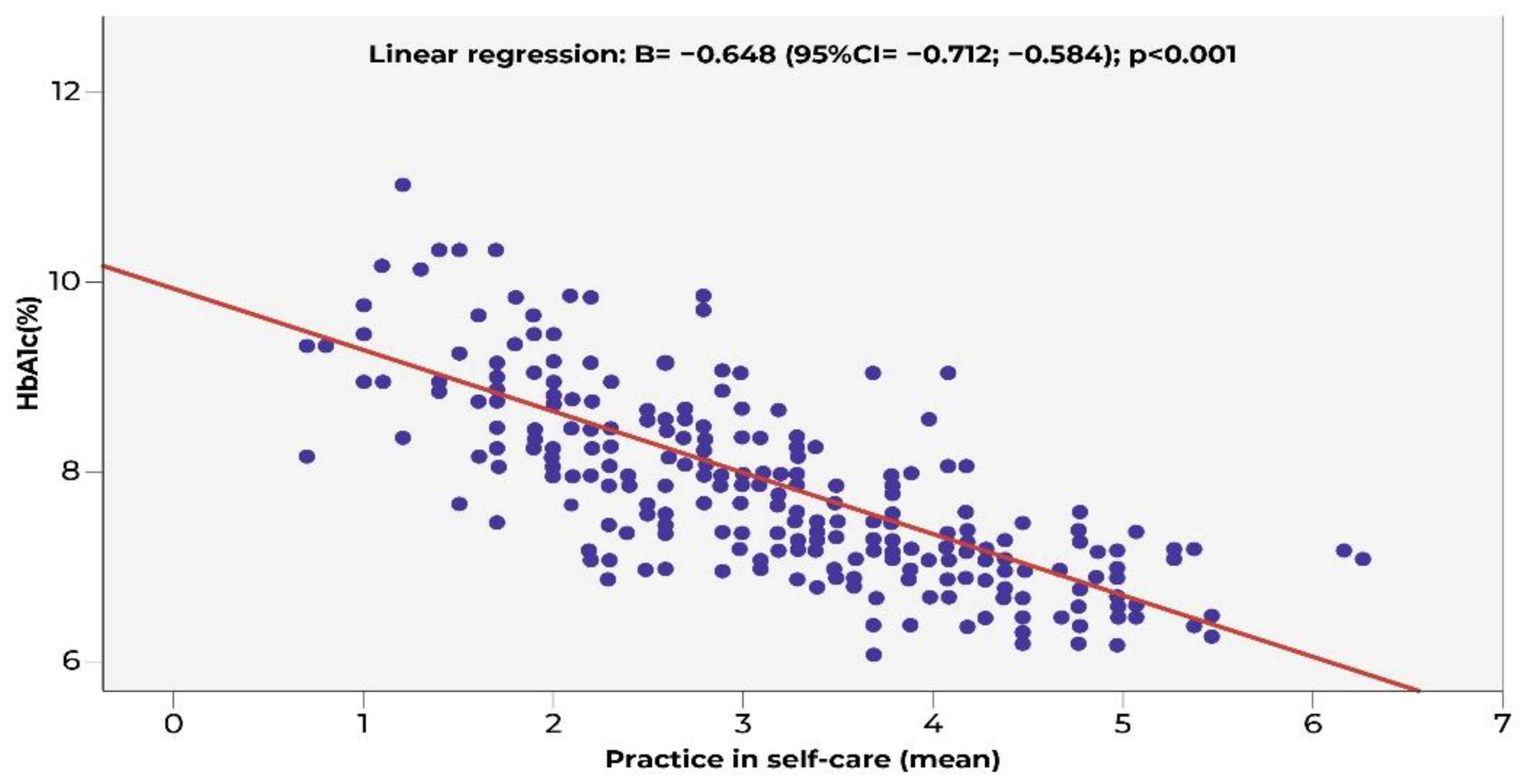
This study explores different methods to determine the practice level in diabetes self-care management based on a Summary of Diabetes Self-Care Activities (SDSCA) score [48]. A good practice score is obtained by adherence to prescribed medication, which is roughly more than five days per week. However, there is a sharp decline in the score when other dimensions of self-care are neglected, e.g., diet, working out, footcare, and glucose monitoring. An overall SDSCA analysis found that 75% of the population scored ≤4, with an average mean score of 3.13, which is quite low [48] (see Figure 4 below).
Another study showed a similar trend in subscale scores using the SDSCA scale. A study conducted by AlJohani [49] showed a high medication adherence score of 6.26 days per week, while the other dimensions of self-care, such as diet, working out, footcare, and glucose monitoring, showed a reasonably low score of between 2.24 and 3.60. The overall mean score was slightly higher than that observed by Al Qahtani [48]. A study conducted in Al Hada, around the Makkah province, showed a similar trend [50]. The highest index of self-care was scored for medication adherence (94.7%), while footcare received a score of 53.4% and working out and diet control scored approximately 41–42%. Blood glucose monitoring, however, yielded the lowest score of 22.4%.
5. Methodology
For this study, a quantitative questionnaire survey was conducted. The survey included a sample of diabetic patients from Jeddah. No precise data are currently available on the number of diabetic patients in this region. Jeddah had a population of 4.076 million in 2017 [51]. The national average diabetes prevalence rate among Saudi adults is 17.5% [52]. If this incidence level applies to Jeddah, the population of diabetic patients may be estimated to be over 700,000. Hence, it follows that the size of the population is adequate for a desirable sample size.
The contact information of the diabetes patients selected for the sample (n = 210) was obtained from hospitals in the Jeddah area. From a composite list, several survey participants who met the inclusion and exclusion criteria were selected for the sample. The following inclusion and exclusion criteria were used to select the sample:
- (a)
- Inclusion: Patients aged 18 years or older (adults), Saudi citizens, male and female, with more than one year of treatment for diabetes.
- (b)
- Exclusion: Patients below 18 years of age, non-Saudi citizens, less than one year of diabetes treatment.
We obtained data from King Abdulaziz Medical City Hospital. The study design was approved by the Ethics Committee of the University of Technology Sydney, ethics application number: ETH19-3842. Before recruitment in the study, the participants received a thorough explanation of the design and objectives of the study, and those willing to participate provided written informed consent.
For the survey, the patients registered on the CDSS, accessible through smartphone applications, were selected, and compliance was checked. All hospital-required ethical protocols were followed. A questionnaire was developed following the CHERRIES guidelines, using the literature to evaluate the reliability of the questionnaire [53]. A pilot study with a draft questionnaire was finalized based on feedback from discussion with doctors, the head of the diabetic clinic, data scientists, and e-health system enablers, and distributed online among the selected participants using their contact details. The questionnaire was conducted in Arabic and comprised queries regarding the behaviour of the patient with regard to medications, dietary precautions, and difficulty following the prescribed treatment. To evaluate the performance of the e-health system, questions related to ease of use of the system were asked, along with the use of the e-health system. A four-point Likert-type scale was used to evaluate the response of patients towards the e-health system and diabetic precautionary measurements. A total of 210 valid responses were obtained for analysis. SPSS version 27.0 was used for the quantitative analysis.
The categorical responses of all questions (nominal or ordinal) in terms of the frequency distributions (counts and percentages) were tabulated. Summarisation of the curve was based on the location of the majority of the responses (more than 50% of the participants). The skewness of all the distributions was recorded where applicable (whether located at the highest frequencies). All statistics were summarised (e.g., standard deviations or means) based on whether the variable was normally distributed for questions with continuous responses.
The main technique used to address the aims of the data analysis was Spearman’s correlation analysis, as it is a useful technique with which to test for associations between a pair of variables when some variables might be ordinal or not normally distributed [54]. Dummy variables were created from demographics and other questions to allow for a correlation analysis to be carried out. A 0.05 level of significance was used as the criterion for statistical significance. A correlation matrix was created across all variables, including demographics. The results are discussed below.
6. Results
6.1. Demographic Profile
Most of the respondents were females (n = 121, 58.5%), between 25 and 50 years old (n = 115, 54.8%), had completed a bachelor’s degree or diploma (n = 120, 57.4%), were unemployed (n = 100, 50.5%), and were earning less than 8000 Saudi riyals per month (n = 106, 59.9%).
6.2. Diabetes Status
Most of the sample had been diabetic for more than five years (n = 146, 70.2%).
6.3. Outpatient Treatment Status
The prescribed and actual compliance levels of outpatient prescriptions for home care by diabetes patients are tabulated in Table 1.
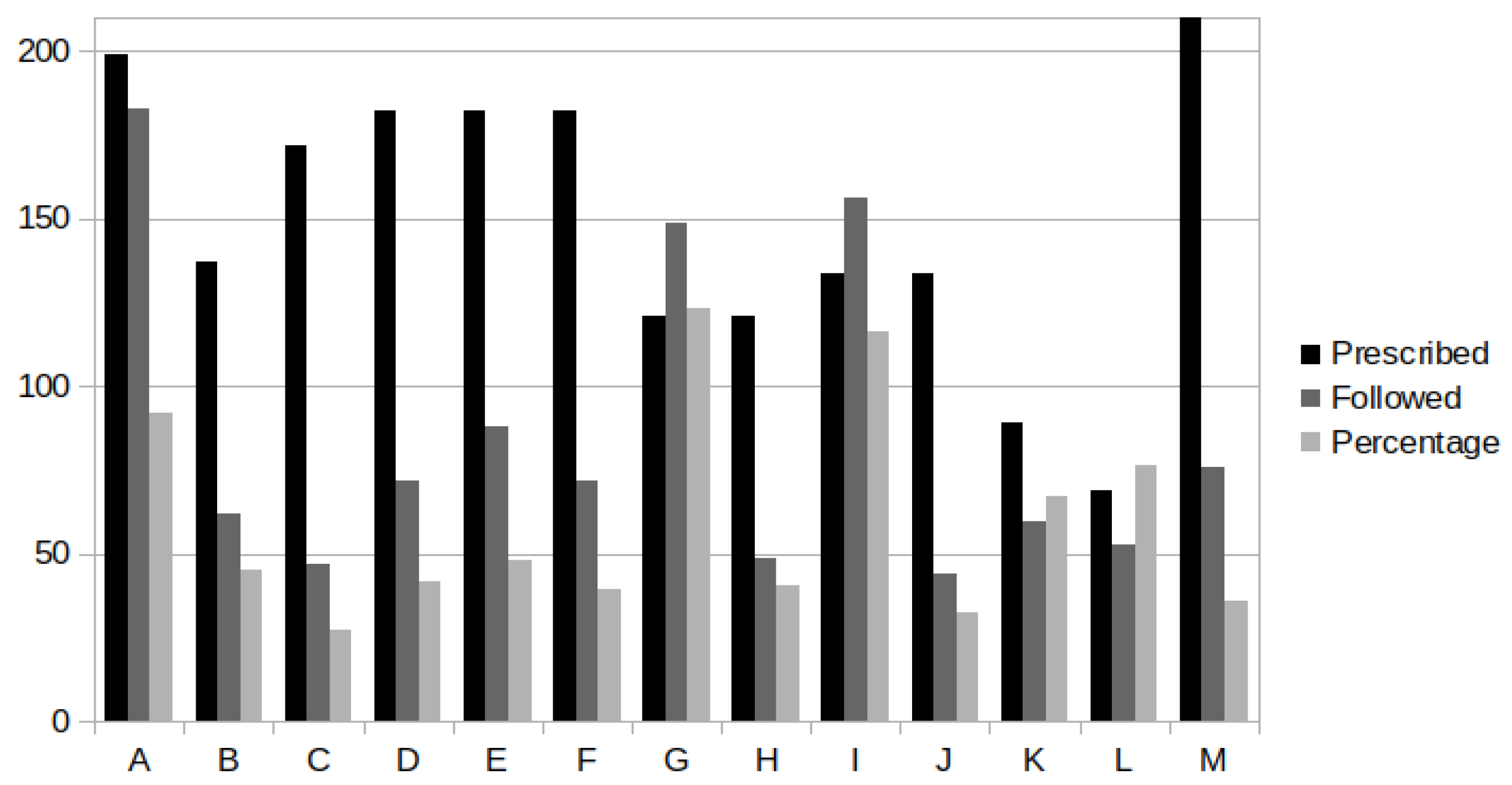
The above findings showed that there was poor compliance with prescribed diet control and daily exercise. The patients’ compliance levels were doubly poor, in that not only did they not follow what their doctors prescribed, they also self-medicated. However, most of the patients in the sample complied with the medical treatment regime. A self-care programme was prescribed for 182 participants out of the sample of 210. It was found that less than 50% had registered for e-health systems. One reason for this may be that less than half of the hospitals (about 40%) had such systems in place, thereby raising the issue of accessibility discussed in previous sections. The number of participants who monitored their blood glucose levels and used insulin injections exceeded those who were prescribed these treatments. The non-compliance level of the patients’ self-care (using an e-health management system) was higher. However, very few of them reported this to the hospitals through an e-health system. Poor compliance was also noted in the case of daily diet regulation and daily workouts. Only one-third of the participants reported any abnormal conditions to the hospital. From the data, therefore, it may be inferred that the current state of self-care behaviour among Saudi diabetic patients is not favourable for implementing e-health systems for self-care (Figure 5 below).
Further, the data showed that both the experience of and the attitude towards e-health systems were internally consistent, and therefore eligible for further analysis. Use of the e-health system refers to how frequently the system is used and for how long, while attitude towards the e-health system helps with the evaluation of the ease of the use of the system. Whether the patient feels using an e-health system is difficult determines if it is user friendly. The mean responses collected about experiences and attitudes tended towards positive, generally just above neutral. Of the 23 correlation coefficients for experience and attitude with demographic factors, only three were significant, as shown in Table 2.
It may be noteworthy that the values of the correlation coefficients were very low. This may indicate interference of other factors in the relationship. The low level of relationship may reflect the results obtained in Table 1.
7. Discussion
The results from this study suggest that the existing self-care model among people with diabetes in Saudi Arabia may be ill-suited for implementing an e-health system for self-care. Applying the business concepts of Eysenbach [4], it can be argued that loopholes exist in the implementation of self-management systems. This reflects the patients’ lack of compliance, as is evident from Table 1. The weak association found between higher education and low-income levels with experience and attitude towards e-health (Table 2) may not impact improvement of patient compliance deficits.
The experience and attitudes of the participants in this study may be attributed to the inadequacies of the self-care system in Saudi Arabia, which have been discussed in earlier sections. Although Saudi Arabia has implemented a self-care system, support for e-health elements is lacking. One of the reasons may be the inadequate knowledge among care staff and community health workers regarding their role in self-care [55]. This could be addressed by training these groups in self-care aspects, including enabling the monitoring of the compliance levels of patients. Such interventions may be useful for patients as they allow care staff and health workers to suitably advise them at the local level.
Another reason could be that the patients were left to themselves and were not connected with the physician, as only 72 of the 88 patients who were using the self-care programme reported the existence of an e-health system in their hospitals (Table 1). The importance of this connection for the success of self-care systems, even when EHRs have been implemented, was demonstrated by Hess [56]. Even a simple WhatsApp service accessed via a patient’s smartphone may prove successful. Blaya [57] highlighted the importance of not only this communication, but also the communication between the various institutions and groups within the self-care system. However, there is no evidence that Saudi Arabia has facilitated this.
The correlation between participants who reported they had a positive experience with participants who had higher education (Table 2) might indicate that some patients could not understand the nuances of the self-care system. Low literacy levels were associated with such a problem in the findings of Winterlich [58]. Therefore, the inclusion of a coaching component in the self-care system may be useful, as educational qualifications need not be related to understanding the medical aspects of diabetes self-care. Providing training or coaching to prospective beneficiaries may address this gap and allow ease of use by a larger section of the population. In the survey data, 34% of the participants had only a high school education or lower. Since this part of the sample was also representative of a section of the country’s population, coaching sessions could prove to be a valuable component in facilitating the larger adoption of e-health in Saudi Arabia. Additionally, the survey found that most of the participants complied with medical prescriptions, blood glucose monitoring, and insulin injections. This could perhaps be because they were afraid of the consequences of not complying with them. The above findings can be seen together as the participants complying with the three most strongly recommended actions and ignoring the value of diet and exercise to their wellbeing. Other reasons may be their family context, busy work schedules, and social interactions.
One of the features of the self-care system is that it minimises face-to-face consultations with physicians. However, it is precisely this interaction that may convince patients of the importance of diet control and physical activity. Adherence to these guidelines would also have been easier during consultations with physicians. A study conducted by King [59] showed that diabetes patients tend to opt to conduct self-care not as a preference but as a forced choice. When direct interaction is difficult, even a daily text messages through mobile phones as a constant reminder would have facilitated better compliance. Rapid alert messages may prove useful for reporting major complications in the self-care system [60].
The above-discussed shortcomings are noted for e-health care in general but may also be applied to the context of Saudi Arabia. This is because the country does not yet treat e-health care as a national priority and lacks supportive laws, regulations, policies, institutions, and strategies for e-health implementation [61].
8. Conclusions
An initial assessment of the compliance levels of self-care among diabetic patients on medical prescriptions in Saudi Arabia revealed poor compliance, especially in relation to diet regulation and physical activity. Additionally, the e-health system was implemented in limited hospitals, thereby limiting its access and reach. Although Saudi Arabia has implemented a self-care system, its e-health system has yet to be widely adopted. This may be facilitated by supportive government laws, regulations, policies, strategies, institutions, and technology, all of which are required for successful e-health implementation in Saudi Arabia.
Since e-health enabled through m-health has many benefits, as described by many authors [62,63], Saudi Arabia may choose to implement e-health using this method. This will aid in connecting patients with their clinics and medications. The digital feedback method provided by the patient alongside doctor examination will enhance the efficacy of the e-health system. This could directly link the patient with a diabetic counsellor, providing sustained motivation and guidance on the above-mentioned compliance indicators (diet and exercise). Technologies such as big data, cloud computing, and the IOT may also be utilised. Telehealth and CDSS for patients located in remote and inaccessible areas [64,65,66] also need to be considered to ensure the success of such an initiative. Education level, consistent encouragement, and advice played a significant role in dietary and exercise adherence. Through an appropriate educational and training programme, patient dependence on e-health systems, feasibility of e-health system utilisation, and patient knowledge of diabetes should be increased.
9. Limitations
This study sought to assess the levels of compliance with self-care for diabetes patients in Saudi Arabia. For this study, the sample was restricted to adult diabetic populations in Jeddah. This may limit the generalisability of the findings. Furthermore, the response size was 210. Additionally, for all the items of the questionnaire, there were missing responses ranging from 1 to 3 and, in a few cases, much higher. Hence, only valid frequencies were considered for each item. This means that the sample size may not have been adequate to ensure sufficient precision. Finally, the questions were mostly related to self-care rather than e-health specifically; therefore, the survey responses may not adequately measure e-health in diabetes self-care.
Author Contributions
F.A. conceptualized and designed the study. V.G. supervised the study. R.A. assessed the data analysis and reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of University of Technology Sydney (protocol code ETH19-3842, 26 February 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- International Diabetes Federation (IDF). Diabetes Facts & Figures. 9 December 2021. Available online: https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html (accessed on 6 October 2022).
- Robert, A.A.; Aldawish, M. The Worrying Trend of Diabetes Mellitus in Saudi Arabia: An Urgent Call to Action. Curr. Diabetes Rev. 2020, 16, 204–210. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). eHealth at WHO. 2019. Available online: https://www.who.int/ehealth/en/ (accessed on 15 January 2022).
- Eysenbach, G. What is e-health? J. Med. Internet Res. 2001, 3, e20. [Google Scholar] [CrossRef] [PubMed]
- Thestrup, J.; Gergely, T.; Beck, P. Exploring New Care Models in Diabetes Management and Therapy with a Wireless Mobile eHealth Platform. In MobiHealth 2011: Wireless Mobile Communication and Healthcare; Lecture Notes of the Institute for Computer Sciences, Social Informatics and Telecommunications Engineering Series; Nikita, K., Lin, J., Fotiadis, D., Arredondo, W.M., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; Volume 83, pp. 203–210. [Google Scholar] [CrossRef]
- Kaufman, N.; Khurana, I.; Holmen, H.; Torbjørnsen, A.; Wahl, A.; Jenum, A.; Småstuen, M.C.; Årsand, E.; Ribu, L.; Harrison, S.; et al. Using digital health technology to prevent and treat diabetes. Diabetes Technol. Ther. 2016, 18, S56–S68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- From, K. The Emergence of Personalised E-Health Care. Open Access Government UK. 12 April 2018. Available online: https://www.openaccessgovernment.org/emergence-personalised-ehealth-care/44428/ (accessed on 20 February 2022).
- Cahn, A.; Akirov, A.; Raz, I. Digital health technology and diabetes management. J. Diabetes 2018, 10, 10–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Gemert-Pijnen, J.E.; Nijland, N.; van Limburg, M.; Ossebaard, H.C.; Kelders, S.M.; Eysenbach, G.; Seydel, E.R. A holistic framework to improve the uptake and impact of eHealth technologies. J. Med. Internet Res. 2011, 13, e111. [Google Scholar] [CrossRef] [PubMed]
- Adenuga, O.A.; Kekwaletswe, R.M.; Coleman, A. eHealth integration and interoperability issues: Towards a solution through enterprise architecture. Health Inf. Sci. Syst. 2015, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Weber-Jahnke, J.; Peyton, L.; Topaloglou, T. eHealth system interoperability. Inf. Syst. Front. 2012, 14, 1–3. [Google Scholar] [CrossRef]
- Kuziemsky, C.E.; Weber-Jahnke, J.H. An eBusiness-based framework for eHealth interoperability. J. Emerg. Technol. Web Intell. 2009, 1, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Rejeb, O.; Bastide, R.; Lamine, E.; Marmier, F.; Pingaud, H. A model driven engineering approach for business continuity management in e-Health systems. In Proceedings of the 6th IEEE International Conference on Digital Ecosystems and Technologies (DEST), Campione d’Italia, Italy, 18–20 June 2012; pp. 1–7. [Google Scholar] [CrossRef]
- Bourquard, K.; Le Gall, F.; Cousin, P. Standards for interoperability in digital health: Selection and implementation in an eHealth project. In Requirements Engineering for Digital Health; Fricker, S., Thümmler, C., Gavras, A., Eds.; Springer: Cham, Switzerland, 2015; pp. 95–115. [Google Scholar] [CrossRef]
- Kayser, L.; Kushniruk, A.; Osborne, R.H.; Norgaard, O.; Turner, P. Enhancing the effectiveness of consumer-focused health information technology systems through eHealth literacy: A framework for understanding users’ needs. JMIR Hum. Factors 2015, 2, e9. [Google Scholar] [CrossRef] [Green Version]
- Inverardi, P.; Mori, M. Requirements models at run-time to support consistent system evolutions. In Proceedings of the 2nd International Workshop on Requirements@ Run.Time, Trento, Italy, 30 August 2011; pp. 1–8. [Google Scholar] [CrossRef]
- Vasilyeva, E.; Pechenizkiy, M.; Puuronen, S. Towards the framework of adaptive user interfaces for eHealth. In Proceedings of the 18th IEEE Symposium on Computer-Based Medical Systems (CBMS’05), Dublin, Ireland, 23–24 June 2005; pp. 139–144. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, J.J.; La Torre, I.D.; Fernández, G.; López-Coronado, M. Analysis of the security and privacy requirements of cloud-based electronic health records systems. J. Med. Internet Res. 2013, 15, e186. [Google Scholar] [CrossRef]
- Alturki, R.; Alyamani, H.J.; Ikram, M.A.; Rahman, M.A.; Alshehri, M.D.; Khan FHaleem, M. Sensor-Cloud Architecture: A Taxonomy of Security Issues in Cloud-Assisted Sensor Networks. IEEE Access 2021, 9, 89344–89359. [Google Scholar] [CrossRef]
- Grundy, J.; Abdelrazek, M.; Curumsing, M.K. Vision: Improved development of mobile eHealth applications. In Proceedings of the IEEE/ACM 5th International Conference on Mobile Software Engineering and Systems (MOBILESoft), Gothenburg, Sweden, 27 May–3 June 2018; pp. 219–223. [Google Scholar]
- Heffernan, K.J.; Chang, S.; Maclean, S.T.; Callegari, E.T.; Garland, S.M.; Reavley, N.J.; Varigos, G.A.; Wark, J.D. Guidelines and recommendations for developing interactive eHealth apps for complex messaging in health promotion. JMIR Mhealth Uhealth 2016, 4, e14. [Google Scholar] [CrossRef]
- Al Hayek, A.A.; Robert, A.A.; Al Dawish, M.A.; Zamzami, M.M.; Sam, A.E.; Alzaid, A.A. Impact of an education program on patient anxiety, depression, glycemic control, and adherence to self-care and medication in type 2 diabetes. J. Fam. Community Med. 2013, 20, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.R.; Al-Abdul Lateef, Z.N.; Al Aithan, M.A.; Bu-Khamseen, M.A.; Al Ibrahim, I.; Khan, S.A. Factors contributing to non-compliance among diabetics attending primary health centers in the Al Hasa district of Saudi Arabia. J. Fam. Community Med. 2012, 19, 26–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alanzi, T.M.; Istepanian, R.S.; Philip, N.; Sungoor, A. A study on perception of managing diabetes mellitus through social networking in the Kingdom of Saudi Arabia. In Proceedings of the XIII Mediterranean Conference on Medical and Biological Engineering and Computing, Seville, Spain, 25–28 September 2013; Romero, L.R., Ed.; Springer: Cham, Switzerland, 2014. [Google Scholar]
- Alotaibi, M.M. A study on the needs for educating and managing fasting diabetes through mobile health in the Kingdom of Saudi Arabia. Int. J. Comput. Syst. 2015, 2, 95–98. [Google Scholar]
- Alotaibi, M.M.; Istepanian, R.; Philip, N. A mobile diabetes management and educational system for type-2 diabetics in Saudi Arabia (SAED). Mhealth 2016, 2, 33. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, E.; Yunus, F.; Househ, M. The impact of mobile phone screen size on user comprehension of health information. Stud. Health Technol. Inform. 2013, 190, 154–156. [Google Scholar] [PubMed]
- Hoque, M.R. An Empirical Study of Mhealth Adoption in a Developing Country: The Moderating Effect of Gender Concern. BMC Med. Inform. Decis. Mak. 2016, 16, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alturki, R.; Gay, V. The Development of an Arabic Weight-Loss App Akser Waznk: Qualitative Results. JMIR Form. Res. 2019, 3, e11785. [Google Scholar] [CrossRef] [Green Version]
- Alturki, R.; Gay, V. Usability Attributes for Mobile Applications: A Systematic Review. In Recent Trends and Advances in Wireless and IoT-enabled Networks; Springer: Cham, Switzerland, 2019; pp. 53–62. [Google Scholar]
- Alturki, R.; Gay, V. A Systematic Review on What Features Should be supported by Fitness Apps and Wearables to Help Users Overcome Obesity. Int. J. Res. Eng. Technol. 2016, 5, 197–206. [Google Scholar]
- Kariuki, E.G.; Okanda, P. Adoption of M-Health and Usability Challenges in M-Health Applications in Kenya: Case of Uzazi Poa M-Health Prototype Application. In Proceedings of the 2017 IEEE AFRICON, Cape Town, South Africa, 18–20 September 2017; pp. 530–535. [Google Scholar]
- Zhang, X.; Han, X.; Dang, Y.; Meng, F.; Guo, X.; Lin, J. User acceptance of mobile health services from users’ perspectives: The role of self-efficacy and response-efficacy in technology acceptance. Inform. Health Soc. Care 2017, 42, 194–206. [Google Scholar] [CrossRef] [PubMed]
- Crico, C.; Renzi, C.; Graf, N.; Buyx, A.; Kondylakis, H.; Koumakis, L.; Pravettoni, G. mHealth and Telemedicine Apps: In Search of a Common Regulation. ecancerMedicalscience 2018, 12, 853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atallah, N.; Khalifa, M.; El Metwally, A.; Househ, M. The Prevalence and Usage of Mobile Health Applications among Mental Health Patients in Saudi Arabia. Comput. Methods Programs Biomed. 2018, 156, 163–168. [Google Scholar] [CrossRef]
- Abid, A. M-Health Technologies to Be Key Enablers of Saudi Digital Transformation Process: Expert. Retrieved 12 April 2019. Available online: http://www.arabnews.com/node/1465921/saudi-arabia (accessed on 20 March 2022).
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. Role of self-care in management of diabetes mellitus. J. Diabetes Metab. Disord. 2013, 12, 14. [Google Scholar] [CrossRef] [Green Version]
- Alanazi, F.; Gay, V.; Alanazi, M.; Alturki, R. Modelling Health Process and System Requirements Engineering for Better eHealth Services in Saudi Arabia. Int. J. Adv. Comput. Sci. Appl. 2021, 12, 9–11. [Google Scholar] [CrossRef]
- Saad, A.M.; Younes, Z.M.; Ahmed, H.; Brown, J.A.; Al Owesie, R.M.; Hassoun, A.A. Self-efficacy, self-care and glycaemic control in Saudi Arabian patients with type 2 diabetes mellitus: A cross-sectional survey. Diabetes Res. Clin. Pract. 2018, 137, 28–36. [Google Scholar] [CrossRef]
- Al-Hanawi, M.K.; Alsharqi, O.; Almazrou, S.; Vaidya, K. Healthcare Finance in the Kingdom of Saudi Arabia: A Qualitative Study of Householders’ Attitudes. Appl. Health Econ. Health Policy 2018, 16, 55–64. [Google Scholar] [CrossRef]
- Patrick, K.; Griswold, W.G.; Raab, F.; Intille, S.S. Health and the Mobile Phone. Am. J. Prev. Med. 2008, 35, 177–181. [Google Scholar] [CrossRef]
- Brzan, P.P.; Rotman, E.; Pajnkihar, M.; Klanjsek, P. Mobile Applications for Control and Self Management of Diabetes: A Systematic Review. J. Med. Syst. 2016, 40, 210. [Google Scholar] [CrossRef]
- Schwartz, J.M.; Moy, A.J.; Rossetti, S.C.; Elhadad, N.; Cato, K.D. Clinician involvement in research on machine learning-based predictive clinical decision support for the hospital setting: A scoping review. J. Am. Med. Inform. Assoc. 2021, 28, 653–663. [Google Scholar] [CrossRef]
- Cleveringa, F.G.W.; Gorter, K.J.; van den Donk, M.; van Gijsel, J.; Rutten, G.E.H.M. Computerized Decision Support Systems in Primary Care for Type 2 Diabetes Patients Only Improve Patients’ Outcomes when Combined with Feedback on Performance and Case Management: A Systematic Review. Diabetes Technol. Ther. 2013, 15, 180–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, K.H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial intelligence in healthcare: Past, present and future. BMJ J. 2017, 2, 230–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- North West Primary Care. 5 Ways Smart Watches Can Improve Your Health. 2020. Available online: https://www.nwpc.com (accessed on 29 July 2022).
- Alqahtani, A.H.; Alzahrani, A.S.; Alzahrani, S.H.; Alqahtani, S.M.; AlOtaibi, A.F.; Khan, A.A. Levels of Practice and Determinants of Diabetes Self-Care in Primary Health Care in Jeddah City, Saudi Arabia. Cureus 2020, 12, e8816. [Google Scholar] [CrossRef] [PubMed]
- Al Johani, K.A.; Kendall, G.E.; Snider, P.D. Self-management practices among type 2 diabetes patients attending primary health-care centres in Medina, Saudi Arabia. East. Mediterr. Health J. 2015, 21, 621–628. [Google Scholar] [CrossRef]
- Sabbah, K.O.A.; Al-Shehri, A.A. Practice and perception of self-management among diabetics in Taif, KSA: Impact of demographic factors. Int. J. Med. Sci. Public Health 2014, 3, 277–285. [Google Scholar] [CrossRef] [Green Version]
- World Population Review. Jeddah Population. 2019. Available online: http://worldpopulationreview.com/world-cities/jeddah-population/ (accessed on 12 December 2021).
- ArabNews. Diabetes: Saudi Arabia’s Growing Health Problem. 12 April 2019. Available online: http://www.arabnews.com/node/1481756/saudi-arabia (accessed on 17 November 2021).
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet ESurveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Pearson: London, UK, 2007. [Google Scholar]
- Darkins, A.; Ryan, P.; Kobb, R.; Foster, L.; Edmonson, E.; Wakefield, B.; Lancaster, A.E. Coordination/Home Telehealth: The systematic implementation of health informatics, home telehealth, and disease management to support the care of veteran patients with chronic conditions. Telemed. e-Health 2008, 14, 1118–1126. [Google Scholar] [CrossRef] [Green Version]
- Hess, R.; Bryce, C.L.; Paone, S.; Fischer, G.; McTigue, K.M.; Olshansky, E.; Zickmund, S.; Fitzgerald, K.; Siminerio, L. Exploring challenges and potentials of personal health records in diabetes self-management: Implementation and initial assessment. Telemed. e-Health 2007, 13, 509–518. [Google Scholar] [CrossRef] [Green Version]
- Blaya, J.A.; Fraser, H.S.; Holt, B. E-health technologies show promise in developing countries. Health Aff. 2010, 29, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Winterlich, A.; Stevenson, I.; Waldren, A.; Dawson, T. Diabetes Digital Coach: Developing an infrastructure for e-health self-management tools. In Proceedings of the 9th International Conference on Developments in eSystems Engineering (DeSE), Liverpool, UK, 31 August–2 September 2016; pp. 68–73. [Google Scholar] [CrossRef]
- King, D.K.; Doty, A.; Martin, C.; Boggs, J.M.; Faber, A.J.; Geno, C.R.; Glasgow, R.E. What patients want: Relevant health information technology for diabetes self-management. Health Technol. 2012, 2, 147–157. [Google Scholar] [CrossRef]
- Su, C.-J.; Wu, C.-Y. JADE implemented mobile multi-agent based, distributed information platform for pervasive health care monitoring. Appl. Soft Comput. 2011, 11, 315–325. [Google Scholar] [CrossRef]
- Ricciardi, L.; Mostashari, F.; Murphy, J.; Daniel, J.G.; Siminerio, E.P. A National Action Plan To Support Consumer Engagement Via E-Health. Health Aff. 2013, 32, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, F.; Gay, V. e-Health for Diabetes Self-Management in Saudi Arabia: Barriers and Solutions. In Proceedings of the 36th International Business Information Management Association Conference (IBIMA), Granada, Spain, 4–5 November 2020; ISBN 978-0-9998551-5-7. [Google Scholar]
- Aikens, J.E.; Rosland, A.M.; Piette, J.D. Improvements in illness self-management and psychological distress associated with telemonitoring support for adults with diabetes. Prim. Care Diabetes 2015, 9, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciemins, E.; Coon, P.; Peck, R.; Holloway, B.; Min, S.J. Using telehealth to provide diabetes care to patients in rural Montana: Findings from the promoting realistic individual self-management program. Telemed. e-Health 2011, 17, 596–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aldahmash, A.M.; Ahmed, Z.; Qadri, F.R.; Thapa, S.; AlMuammar, A.M. Implementing a connected health intervention for remote patient monitoring in Saudi Arabia and Pakistan: Explaining ‘the what’and ‘the how’. Glob. Health 2019, 15, 20. [Google Scholar] [CrossRef]
- Sweileh, W.; Aker, O.; Hamooz, S. Rate of Compliance among Patients with Diabetes Mellitus and Hypertension. An-Najah Univ. J. Res. 2005, 19, 1–12. [Google Scholar]
Figure 1.
Age-standardised prevalence of diabetes per IDF region for 2017 and 2045 (18–99 years) [1].
Figure 1.
Age-standardised prevalence of diabetes per IDF region for 2017 and 2045 (18–99 years) [1].

Figure 2.
Prevalence and future prediction of diabetes mellitus in Saudi Arabia [2].
Figure 2.
Prevalence and future prediction of diabetes mellitus in Saudi Arabia [2].

Figure 3.
AI and ML in diabetes care.

Figure 4.
A significant negative relationship is shown in the linear regression of the function of the SDSCA score.
Figure 4.
A significant negative relationship is shown in the linear regression of the function of the SDSCA score.

Figure 5.
Graphical representation of the compliance level of prescribed treatment by survey participants.
Figure 5.
Graphical representation of the compliance level of prescribed treatment by survey participants.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Compliance levels for a prescribed treatment by survey participants.
| Description | Prescribed | Followed | Percentage | |
|---|---|---|---|---|
| A | Medical treatment | 199 | 183 | 92.0 |
| B | Diet control (quantity and type of daily consumed food) | 137 | 62 | 45.3 |
| C | Daily exercise | 172 | 47 | 27.3 |
| D | Self-care programme | 182 | 72 | 42 |
| E | Registered in the hospital e-health system | 182 | 88 | 48.4 |
| F | Hospital with e-health self-care management system | 182 | 72 | 39.6 |
| G | Regular blood glucose monitoring | 121 | 149 | 123.1 |
| H | Blood glucose reporting hospital through e-health | 121 | 49 | 40.5 |
| I | Insulin injection | 134 | 156 | 116.4 |
| J | Injection reporting hospital through e-health | 134 | 44 | 32.8 |
| K | Daily diet regulation | 89 | 60 | 67.4 |
| L | Daily work-out | 69 | 53 | 76.8 |
| M | Abnormal conditions reported | 210 | 76 | 36.2 |
Table 2.
Significant correlation coefficients for experience and attitude with some demographic factors.
Table 2.
Significant correlation coefficients for experience and attitude with some demographic factors.
| Variable | Correlation Co-Efficient |
|---|---|
| Experience with e-health system versus attitude about e-health system | 0.555 ** |
| Experience with e-health system versus higher education (postgraduate) | 0.160 * |
| Attitude about e-health system and participants with low incomes (<8000 riyals) | 0.166 * |
Note: * means significant at 0.05 level; ** means significant at 0.01 level.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Alanazi, F.; Gay, V.; Alturki, R. Poor Compliance of Diabetic Patients with AI-Enabled E-Health Self-Care Management in Saudi Arabia. Information 2022, 13, 509. https://doi.org/10.3390/info13110509
AMA Style
Alanazi F, Gay V, Alturki R. Poor Compliance of Diabetic Patients with AI-Enabled E-Health Self-Care Management in Saudi Arabia. Information. 2022; 13(11):509. https://doi.org/10.3390/info13110509
Chicago/Turabian StyleAlanazi, Fuhid, Valerie Gay, and Ryan Alturki. 2022. "Poor Compliance of Diabetic Patients with AI-Enabled E-Health Self-Care Management in Saudi Arabia" Information 13, no. 11: 509. https://doi.org/10.3390/info13110509
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.