
Molecular Mechanisms Responsible for Diabetogenic Effects of COVID-19 Infection—Induction of Autoimmune Dysregulation and Metabolic Disturbances
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Viruses and Diabetes Mellitus—What Do We Know So Far?
3. COVID-19 and Diabetes Mellitus
4. COVID-19-Induced Diabetes
4.1. Type 1 Diabetes Mellitus (T1DM)
4.2. Type 2 Diabetes Mellitus (T2DM)
4.3. COVID-19-Vaccine-Induced Diabetes Mellitus
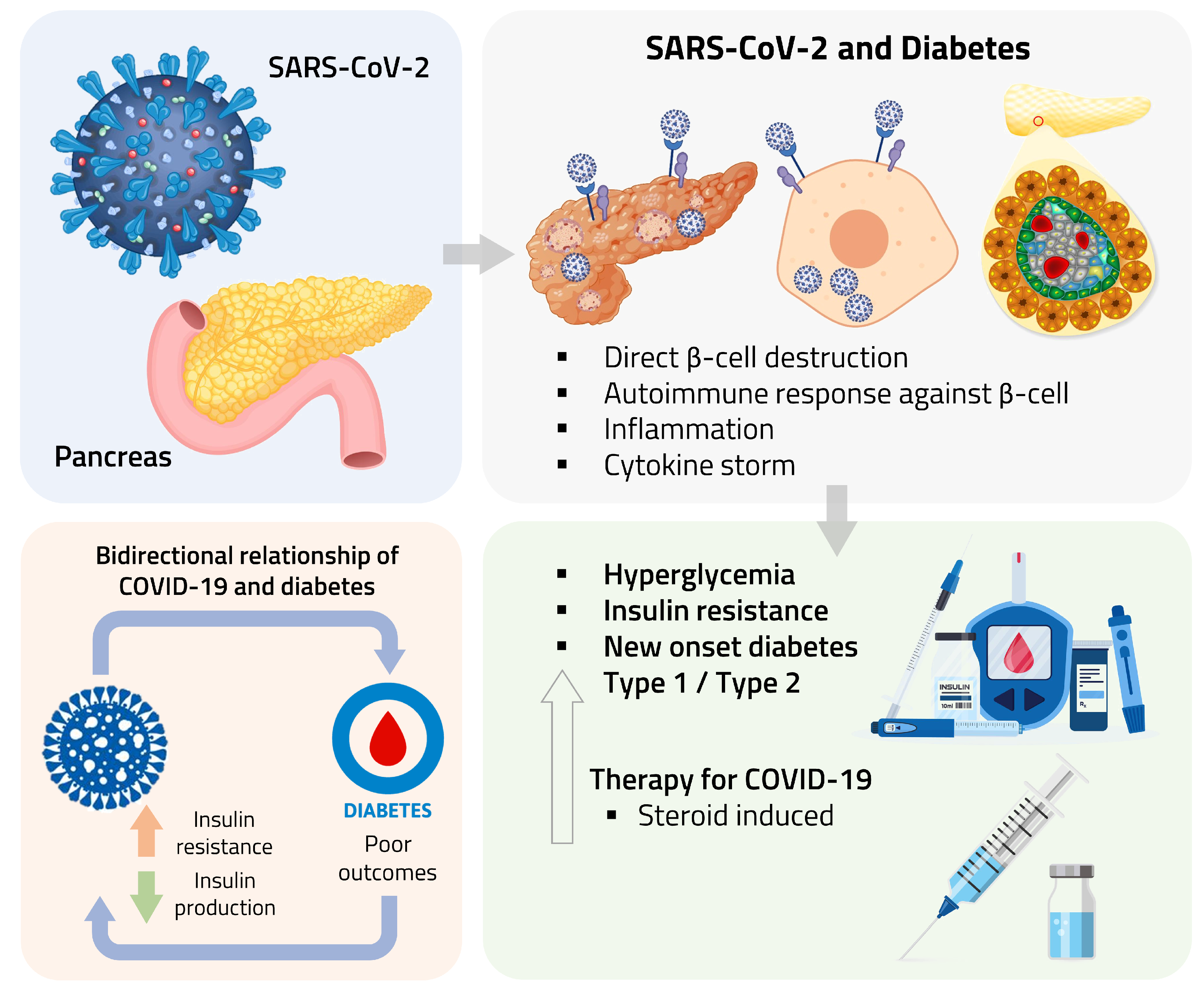
5. Underlying Pathophysiological Mechanism of COVID-19-Induced Diabetes Mellitus
5.1. Direct and Indirect -Cell Damage
5.1.1. Indirect -Cell Damage: Autoimmunity and Inflammation
5.1.2. Insulin Resistance
6. Future Directions and Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE2 | Angiotensin-Converting Enzyme 2 |
| BMI | Body Mass Index |
| COVID-19 | Coronavirus Disease 2019 |
| DKA | Diabetic Ketoacidosis |
| DNA | Deoxyribonucleic Acid |
| DPP-4 | Dipeptidyl-Peptidase 4 |
| FT4 | Free Thyroxine |
| GAD | Glutamic Acid Decarboxylase |
| HbA1c | Hemoglobin A1c |
| HDL-C | High-Density Lipoprotein Cholesterol |
| HHS | Hyperglycaemic Hyperosmolar State |
| ICU | Intensive Care Unit |
| IFN | Interferon Gamma |
| IL-6 | Interleukin 6 |
| IRS | Insulin Receptor Substrates |
| ISR | Integrated Stress Response |
| LDL-C | Low-Density Lipoprotein Cholesterol |
| NET | Neutrophil Extracellular Trap |
| REST | Repressor Element-1 Silencing Transcription factor |
| RNA | Ribonucleic Acid |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| SLE | Systemic Lupus Erythematosus |
| T1DM | Type 1 Diabetes Mellitus |
| T2DM | Type 2 Diabetes Mellitus |
| TMPRSS2 | Transmembrane Serine Protease 2 |
| TNF-alpha | Tumor Necrosis Factor Alpha |
| TSH | Thyroid-stimulating hormone |
References
- Rubino, F.; Amiel, S.A.; Zimmet, P.; Alberti, G.; Bornstein, S.; Eckel, R.H.; Mingrone, G.; Boehm, B.; Cooper, M.E.; Chai, Z.; et al. New-Onset Diabetes in COVID-19. N. Engl. J. Med. 2020, 383, 789–790. [Google Scholar] [CrossRef] [PubMed]
- Joshi, N.; Caputo, G.M.; Weitekamp, M.R.; Karchmer, A.W. Infections in patients with diabetes mellitus. N. Engl. J. Med. 1999, 341, 1906–1912. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Erener, S. Diabetes, infection risk and COVID-19. Mol. Metab. 2020, 39, 101044. [Google Scholar] [CrossRef] [PubMed]
- Carey, I.M.; Critchley, J.A.; DeWilde, S.; Harris, T.; Hosking, F.J.; Cook, D.G. Risk of Infection in Type 1 and Type 2 Diabetes Compared With the General Population: A Matched Cohort Study. Diabetes Care 2018, 41, 513–521. [Google Scholar] [CrossRef] [Green Version]
- Casqueiro, J.; Casqueiro, J.; Alves, C. Infections in patients with diabetes mellitus: A review of pathogenesis. Indian J. Endocrinol. Metab. 2012, 16 Suppl 1, S27–S36. [Google Scholar] [CrossRef]
- Zhu, L.; She, Z.G.; Cheng, X.; Qin, J.J.; Zhang, X.J.; Cai, J.; Lei, F.; Wang, H.; Xie, J.; Wang, W.; et al. Association of Blood Glucose Control and Outcomes in Patients with COVID-19 and Pre-existing Type 2 Diabetes. Cell Metab. 2020, 31, 1068–1077.e3. [Google Scholar] [CrossRef] [PubMed]
- Apicella, M.; Campopiano, M.C.; Mantuano, M.; Mazoni, L.; Coppelli, A.; Del Prato, S. COVID-19 in people with diabetes: Understanding the reasons for worse outcomes. Lancet Diabetes Endocrinol. 2020, 8, 782–792. [Google Scholar] [CrossRef]
- Ceriello, A.; De Nigris, V.; Prattichizzo, F. Why is hyperglycaemia worsening COVID-19 and its prognosis? Diabetes Obes. Metab. 2020, 22, 1951–1952. [Google Scholar] [CrossRef]
- Lazarus, G.; Audrey, J.; Wangsaputra, V.K.; Tamara, A.; Tahapary, D.L. High admission blood glucose independently predicts poor prognosis in COVID-19 patients: A systematic review and dose-response meta-analysis. Diabetes Res. Clin. Pract. 2021, 171, 108561. [Google Scholar] [CrossRef]
- Li, H.; Tian, S.; Chen, T.; Cui, Z.; Shi, N.; Zhong, X.; Qiu, K.; Zhang, J.; Zeng, T.; Chen, L.; et al. Newly diagnosed diabetes is associated with a higher risk of mortality than known diabetes in hospitalized patients with COVID-19. Diabetes Obes. Metab. 2020, 22, 1897–1906. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Ma, P.; Zhang, S.; Song, S.; Wang, Z.; Ma, Y.; Xu, J.; Wu, F.; Duan, L.; Yin, Z.; et al. Fasting blood glucose at admission is an independent predictor for 28-day mortality in patients with COVID-19 without previous diagnosis of diabetes: A multi-centre retrospective study. Diabetologia 2020, 63, 2102–2111. [Google Scholar] [CrossRef] [PubMed]
- Fadini, G.P.; Morieri, M.L.; Boscari, F.; Fioretto, P.; Maran, A.; Busetto, L.; Bonora, B.M.; Selmin, E.; Arcidiacono, G.; Pinelli, S.; et al. Newly-diagnosed diabetes and admission hyperglycemia predict COVID-19 severity by aggravating respiratory deterioration. Diabetes Res. Clin. Pract. 2020, 168, 108374. [Google Scholar] [CrossRef] [PubMed]
- Coppelli, A.; Giannarelli, R.; Aragona, M.; Penno, G.; Falcone, M.; Tiseo, G.; Ghiadoni, L.; Barbieri, G.; Monzani, F.; Virdis, A.; et al. Hyperglycemia at Hospital Admission Is Associated With Severity of the Prognosis in Patients Hospitalized for COVID-19: The Pisa COVID-19 Study. Diabetes Care 2020, 43, 2345–2348. [Google Scholar] [CrossRef] [PubMed]
- Yeung, W.C.G.; Rawlinson, W.D.; Craig, M.E. Enterovirus infection and Type 1 diabetes mellitus: Systematic review and meta-analysis of observational molecular studies. BMJ 2011, 342, 421. [Google Scholar] [CrossRef] [Green Version]
- Rewers, M.; Ludvigsson, J. Environmental risk factors for type 1 diabetes. Lancet 2016, 387, 2340–2348. [Google Scholar] [CrossRef] [Green Version]
- Hyöty, H.; Hiltunen, M.; Knip, M.; Laakkonen, M.; Vähäsalo, P.; Karjalainen, J.; Koskela, P.; Roivainen, M.; Leinikki, P.; Hovi, T. A prospective study of the role of coxsackie B and other enterovirus infections in the pathogenesis of IDDM. Childhood Diabetes in Finland (DiMe) Study Group. Diabetes 1995, 44, 652–657. [Google Scholar] [CrossRef]
- Fabrizi, F.; Martin, P.; Dixit, V.; Bunnapradist, S.; Kanwal, F.; Dulai, G. Post-transplant diabetes mellitus and HCV seropositive status after renal transplantation: Meta-analysis of clinical studies. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2005, 5, 2433–2440. [Google Scholar] [CrossRef]
- Labropoulou-Karatza, C.; Goritsas, C.; Fragopanagou, H.; Repandi, M.; Matsouka, P.; Alexandrides, T. High prevalence of diabetes mellitus among adult β-thalassaemic patients with chronic hepatitis C. Eur. J. Gastroenterol. Hepatol. 1999, 11, 1033–1036. [Google Scholar] [CrossRef]
- Mason, A.L.; Lau, J.Y.; Hoang, N.; Qian, K.; Alexander, G.J.; Xu, L.; Guo, L.; Jacob, S.; Regenstein, F.G.; Zimmerman, R.; et al. Association of diabetes mellitus and chronic hepatitis C virus infection. Hepatology 1999, 29, 328–333. [Google Scholar] [CrossRef]
- Knobler, H.; Stagnaro-Green, A.; Wallenstein, S.; Schwartz, M.; Roman, S.H. Higher incidence of diabetes in liver transplant recipients with hepatitis C. J. Clin. Gastroenterol. 1998, 26, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.H.; Brancati, F.L.; Sulkowski, M.S.; Strathdee, S.A.; Szklo, M.; Thomas, D.L. Prevalence of type 2 diabetes mellitus among persons with hepatitis C virus infection in the United States. Ann. Intern. Med. 2000, 133, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Pérez, B.; Aranda Narváez, J.M.; Santoyo Santoyo, J.; Fernández-Aguilar, J.L.; Suárez Muñoz, M.A.; González-Sánchez, A.J.; Pérez Daga, J.A.; Ramírez Plaza, C.P.; Carrasco Campos, J.; Jiménez Mazure, C.; et al. Influence of Immunosuppression and Effect of Hepatitis C Virus on New Onset of Diabetes Mellitus in Liver Transplant Recipients. Transplant. Proc. 2008, 40, 2994–2996. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, T.; Witsø, E.; Tapia, G.; Stene, L.C.; Rønningen, K.S. Self-reported lower respiratory tract infections and development of islet autoimmunity in children with the type 1 diabetes high-risk HLA genotype: The MIDIA study. Diabetes/Metab. Res. Rev. 2011, 27, 834–837. [Google Scholar] [CrossRef]
- Lönnrot, M.; Lynch, K.F.; Elding Larsson, H.; Lernmark, Å.; Rewers, M.J.; Törn, C.; Burkhardt, B.R.; Briese, T.; Hagopian, W.A.; She, J.X.; et al. Respiratory infections are temporally associated with initiation of type 1 diabetes autoimmunity: The TEDDY study. Diabetologia 2017, 60, 1931–1940. [Google Scholar] [CrossRef] [Green Version]
- Beyerlein, A.; Wehweck, F.; Ziegler, A.G.; Pflueger, M. Respiratory infections in early life and the development of islet autoimmunity in children at increased type 1 diabetes risk: Evidence from the BABYDIET study. JAMA Pediatr. 2013, 167, 800–807. [Google Scholar] [CrossRef] [Green Version]
- Al-Sayyar, A.; Hulme, K.D.; Thibaut, R.; Bayry, J.; Sheedy, F.J.; Short, K.R.; Alzaid, F. Respiratory Tract Infections in Diabetes—Lessons From Tuberculosis and Influenza to Guide Understanding of COVID-19 Severity. Front. Endocrinol. 2022, 13, 919223. [Google Scholar] [CrossRef]
- Landstra, C.P.; de Koning, E.J.P. COVID-19 and Diabetes: Understanding the Interrelationship and Risks for a Severe Course. Front. Endocrinol. 2021, 12, 649525. [Google Scholar] [CrossRef]
- Zhou, Y.; Chi, J.; Lv, W.; Wang, Y. Obesity and diabetes as high-risk factors for severe coronavirus disease 2019 (COVID-19). Diabetes/Metabolism Res. Rev. 2021, 37, e3377. [Google Scholar] [CrossRef]
- Feldman, E.L.; Savelieff, M.G.; Hayek, S.S.; Pennathur, S.; Kretzler, M.; Pop-Busui, R. COVID-19 and Diabetes: A Collision and Collusion of Two Diseases. Diabetes 2020, 69, 2549–2565. [Google Scholar] [CrossRef]
- Wu, C.T.; Lidsky, P.V.; Xiao, Y.; Lee, I.T.; Cheng, R.; Nakayama, T.; Jiang, S.; Demeter, J.; Bevacqua, R.J.; Chang, C.A.; et al. SARS-CoV-2 infects human pancreatic β cells and elicits β cell impairment. Cell Metab. 2021, 33, 1565–1576.e5. [Google Scholar] [CrossRef] [PubMed]
- Rajpal, A.; Rahimi, L.; Ismail-Beigi, F. Factors leading to high morbidity and mortality of COVID-19 in patients with type 2 diabetes. J. Diabetes 2020, 12, 895–908. [Google Scholar] [CrossRef] [PubMed]
- Morra, M.E.; Van Thanh, L.; Kamel, M.G.; Ghazy, A.A.; Altibi, A.M.A.; Dat, L.M.; Thy, T.N.X.; Vuong, N.L.; Mostafa, M.R.; Ahmed, S.I.; et al. Clinical outcomes of current medical approaches for Middle East respiratory syndrome: A systematic review and meta-analysis. Rev. Med. Virol. 2018, 28, e1977. [Google Scholar] [CrossRef]
- Brufsky, A. Hyperglycemia, hydroxychloroquine, and the COVID-19 pandemic. J. Med. Virol. 2020, 92, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Umpierrez, G.E.; Isaacs, S.D.; Bazargan, N.; You, X.; Thaler, L.M.; Kitabchi, A.E. Hyperglycemia: An independent marker of in-hospital mortality in patients with undiagnosed diabetes. J. Clin. Endocrinol. Metab. 2002, 87, 978–982. [Google Scholar] [CrossRef]
- Yang, J.K.; Feng, Y.; Yuan, M.Y.; Yuan, S.Y.; Fu, H.J.; Wu, B.Y.; Sun, G.Z.; Yang, G.R.; Zhang, X.L.; Wang, L.; et al. Plasma glucose levels and diabetes are independent predictors for mortality and morbidity in patients with SARS. Diabet. Med. J. Br. Diabet. Assoc. 2006, 23, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Korytkowski, M.; Antinori-Lent, K.; Drincic, A.; Hirsch, I.B.; McDonnell, M.E.; Rushakoff, R.; Muniyappa, R. A Pragmatic Approach to Inpatient Diabetes Management during the COVID-19 Pandemic. J. Clin. Endocrinol. Metab. 2020, 105, 3076–3087. [Google Scholar] [CrossRef]
- Knapp, S. Diabetes and Infection: Is There a Link? Gerontology 2013, 59, 99–104. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Lambadiari, V.; Kousathana, F.; Raptis, A.; Katogiannis, K.; Kokkinos, A.; Ikonomidis, I. Pre-Existing Cytokine and NLRP3 Inflammasome Activation and Increased Vascular Permeability in Diabetes: A Possible Fatal Link With Worst COVID-19 Infection Outcomes? Front. Immunol. 2020, 11, 557235. [Google Scholar] [CrossRef] [PubMed]
- Toki, S.; Goleniewska, K.; Reiss, S.; Zhang, J.; Bloodworth, M.H.; Stier, M.T.; Zhou, W.; Newcomb, D.C.; Ware, L.B.; Stanwood, G.D.; et al. Glucagon-like peptide 1 signaling inhibits allergen-induced lung IL-33 release and reduces group 2 innate lymphoid cell cytokine production in vivo. J. Allergy Clin. Immunol. 2018, 142, 1515–1528.e8. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Pavlidis, G.; Lambadiari, V.; Kousathana, F.; Varoudi, M.; Spanoudi, F.; Maratou, E.; Parissis, J.; Triantafyllidi, H.; Dimitriadis, G.; et al. Early detection of left ventricular dysfunction in first-degree relatives of diabetic patients by myocardial deformation imaging: The role of endothelial glycocalyx damage. Int. J. Cardiol. 2017, 233, 105–112. [Google Scholar] [CrossRef]
- Lim, S.; Bae, J.H.; Kwon, H.S.; Nauck, M.A. COVID-19 and diabetes mellitus: From pathophysiology to clinical management. Nat. Rev. Endocrinol. 2021, 17, 11–30. [Google Scholar] [CrossRef] [PubMed]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.D.; Sacco, C.; Bertuzzi, A. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef]
- Mackman, N.; Antoniak, S.; Wolberg, A.S.; Kasthuri, R.; Key, N.S. Coagulation abnormalities and thrombosis in patients infected with SARS-CoV-2 and other pandemic viruses. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2033–2044. [Google Scholar] [CrossRef] [PubMed]
- Manolis, A.S.; Manolis, T.A.; Manolis, A.A.; Papatheou, D.; Melita, H. COVID-19 Infection: Viral Macro- and Micro-Vascular Coagulopathy and Thromboembolism/Prophylactic and Therapeutic Management. J. Cardiovasc. Pharmacol. Ther. 2020, 26, 12–24. [Google Scholar] [CrossRef]
- Violi, F.; Ceccarelli, G.; Cangemi, R.; Cipollone, F.; D’Ardes, D.; Oliva, A.; Pirro, M.; Rocco, M.; Alessandri, F.; D’Ettorre, G.; et al. Arterial and venous thrombosis in coronavirus 2019 disease (COVID-19): Relationship with mortality. Intern. Emerg. Med. 2021, 16, 1231–1237. [Google Scholar] [CrossRef]
- D’Ardes, D.; Rossi, I.; Bucciarelli, B.; Allegra, M.; Bianco, F.; Sinjari, B.; Marchioni, M.; Di Nicola, M.; Santilli, F.; Guagnano, M.T.; et al. Metabolic Changes in SARS-CoV-2 Infection: Clinical Data and Molecular Hypothesis to Explain Alterations of Lipid Profile and Thyroid Function Observed in COVID-19 Patients. Life 2021, 11, 860. [Google Scholar] [CrossRef]
- Wei, X.; Zeng, W.; Su, J.; Wan, H.; Yu, X.; Cao, X.; Tan, W.; Wang, H. Hypolipidemia is associated with the severity of COVID-19. J. Clin. Lipidol. 2020, 14, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Wang, H.; Ye, G.; Cao, X.; Xu, X.; Tan, W.; Zhang, Y. Low-density lipoprotein is a potential predictor of poor prognosis in patients with coronavirus disease 2019. Metabolism 2020, 107, 154243. [Google Scholar] [CrossRef]
- Khoo, B.; Tan, T.; Clarke, S.A.; Mills, E.G.; Patel, B.; Modi, M.; Phylactou, M.; Eng, P.C.; Thurston, L.; Alexander, E.C. Thyroid function before, during, and after COVID-19. J. Clin. Endocrinol. Metab. 2021, 106, e803–e811. [Google Scholar] [CrossRef] [PubMed]
- Sardu, C.; D’Onofrio, N.; Balestrieri, M.L.; Barbieri, M.; Rizzo, M.R.; Messina, V.; Maggi, P.; Coppola, N.; Paolisso, G.; Marfella, R. Outcomes in Patients With Hyperglycemia Affected by COVID-19: Can We Do More on Glycemic Control? Diabetes Care 2020, 43, 1408–1415. [Google Scholar] [CrossRef]
- Barron, E.; Bakhai, C.; Kar, P.; Weaver, A.; Bradley, D.; Ismail, H.; Knighton, P.; Holman, N.; Khunti, K.; Sattar, N.; et al. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: A whole-population study. Lancet Diabetes Endocrinol. 2020, 8, 813–822. [Google Scholar] [CrossRef]
- McGurnaghan, S.J.; Weir, A.; Bishop, J.; Kennedy, S.; Blackbourn, L.A.K.; McAllister, D.A.; Hutchinson, S.; Caparrotta, T.M.; Mellor, J.; Jeyam, A.; et al. Risks of and risk factors for COVID-19 disease in people with diabetes: A cohort study of the total population of Scotland. Lancet Diabetes Endocrinol. 2021, 9, 82–93. [Google Scholar] [CrossRef]
- Gregory, J.M.; Slaughter, J.C.; Duffus, S.H.; Smith, T.J.; LeStourgeon, L.M.; Jaser, S.S.; McCoy, A.B.; Luther, J.M.; Giovannetti, E.R.; Boeder, S.; et al. COVID-19 Severity Is Tripled in the Diabetes Community: A Prospective Analysis of the Pandemic’s Impact in Type 1 and Type 2 Diabetes. Diabetes Care 2021, 44, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Xiang, F.; Long, B.; He, J.; Cheng, F.; Zhang, S.; Liu, Q.; Chen, Z.; Li, H.; Chen, M.; Peng, M.; et al. Impaired antibody responses were observed in patients with Type 2 diabetes mellitus after receiving the inactivated COVID-19 vaccines. Virol. J. 2023, 20, 22. [Google Scholar] [CrossRef]
- Paar, M.; Aziz, F.; Sourij, C.; Tripolt, N.J.; Kojzar, H.; Müller, A.; Pferschy, P.; Obermayer, A.; Banfic, T.; Di Geronimo Quintero, B.; et al. Only Subclinical Alterations in the Haemostatic System of People with Diabetes after COVID-19 Vaccination. Viruses 2022, 15, 10. [Google Scholar] [CrossRef]
- Bubenek-Turconi, Ş.I.; Andrei, S.; Văleanu, L.; Ştefan, M.G.; Grigoraş, I.; Copotoiu, S.; Bodolea, C.; Tomescu, D.; Popescu, M.; Filipescu, D.; et al. Clinical characteristics and factors associated with ICU mortality during the first year of the SARS-Cov-2 pandemic in Romania: A prospective, cohort, multicentre study of 9000 patients. Eur. J. Anaesthesiol. 2023, 40, 4–12. [Google Scholar] [CrossRef]
- Vardavas, C.I.; Mathioudakis, A.G.; Nikitara, K.; Stamatelopoulos, K.; Georgiopoulos, G.; Phalkey, R.; Leonardi-Bee, J.; Fernandez, E.; Carnicer-Pont, D.; Vestbo, J.; et al. Prognostic factors for mortality, intensive care unit and hospital admission due to SARS-CoV-2: A systematic review and metaanalysis of cohort studies in Europe. Eur. Respir. Rev. 2022, 31, 220098. [Google Scholar] [CrossRef]
- Sathish, T.; Kapoor, N.; Cao, Y.; Tapp, R.J.; Zimmet, P. Proportion of newly diagnosed diabetes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Obes. Metab. 2021, 23, 870–874. [Google Scholar] [CrossRef]
- Sathish, T.; Chandrika Anton, M. Newly diagnosed diabetes in patients with mild to moderate COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 569–571. [Google Scholar] [CrossRef]
- Boddu, S.K.; Aurangabadkar, G.; Kuchay, M.S. New onset diabetes, Type 1 diabetes and COVID-19. Diabetes Metab. Syndr. 2020, 14, 2211–2217. [Google Scholar] [CrossRef]
- Unsworth, R.; Wallace, S.; Oliver, N.S.; Yeung, S.; Kshirsagar, A.; Naidu, H.; Kwong, R.M.W.; Kumar, P.; Logan, K.M. New-onset type 1 diabetes in children during COVID-19: Multicenter regional findings in the U.K. Diabetes Care 2020, 43, e170–e171. [Google Scholar] [CrossRef]
- Kamrath, C.; Mönkemöller, K.; Biester, T.; Rohrer, T.R.; Warncke, K.; Hammersen, J.; Holl, R.W. Ketoacidosis in Children and Adolescents With Newly Diagnosed Type 1 Diabetes During the COVID-19 Pandemic in Germany. JAMA 2020, 324, 801–804. [Google Scholar] [CrossRef] [PubMed]
- Cheong, C.W.; Chen, C.L.; Li, C.H.; Seak, C.J.; Tseng, H.J.; Hsu, K.H.; Ng, C.J.; Chien, C.Y. Two-stage prediction model for in-hospital mortality of patients with influenza infection. BMC Infect. Dis. 2021, 21, 451. [Google Scholar] [CrossRef] [PubMed]
- Andrade, F.B.; Gualberto, A.; Rezende, C.; Percegoni, N.; Gameiro, J.; Hottz, E.D. The Weight of Obesity in Immunity from Influenza to COVID-19. Front. Cell. Infect. Microbiol. 2021, 11, 638852. [Google Scholar] [CrossRef]
- Shill, M.C.; Mohsin, M.N.A.B.; Showdagor, U.; Hasan, S.N.; Zahid, M.Z.I.; Khan, S.I.; Hossain, M.; Rahman, G.M.S.; Reza, H.M. Microbial sensitivity of the common pathogens for UTIs are declining in diabetic patients compared to non-diabetic patients in Bangladesh: An institution-based retrospective study. Heliyon 2023, 9, e12897. [Google Scholar] [CrossRef]
- Wong, J.W.H.; Xu, R.H.; Ramm, O.; Tucker, L.Y.; Zaritsky, E.F. Urinary Tract Infections Among Gender Diverse People Assigned Female at Birth on Testosterone. Urogynecology 2023, 29, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Morbach, S.; Eckhard, M.; Lobmann, R.; Müller, E.; Reike, H.; Risse, A.; Rümenapf, G.; Spraul, M. Diabetic Foot Syndrome. Exp. Clin. Endocrinol. Diabetes 2023, 131, 84–93. [Google Scholar] [CrossRef]
- Wu, H.; Lau, E.S.; Yang, A.; Zhang, X.; Fan, B.; Ma, R.C.; Kong, A.P.; Chow, E.; So, W.Y.; Chan, J.C.; et al. Age-specific population attributable risk factors for all-cause and cause-specific mortality in Type 2 diabetes: An analysis of a 6-year prospective cohort study of over 360,000 people in Hong Kong. PLoS Med. 2023, 20, e1004173. [Google Scholar] [CrossRef] [PubMed]
- Beumer, M.C.; Koch, R.M.; van Beuningen, D.; OudeLashof, A.M.; van de Veerdonk, F.L.; Kolwijck, E.; van der Hoeven, J.G.; Bergmans, D.C.; Hoedemaekers, C.W.E. Influenza virus and factors that are associated with ICU admission, pulmonary co-infections and ICU mortality. J. Crit. Care 2019, 50, 59–65. [Google Scholar] [CrossRef]
- Metwally, A.A.; Mehta, P.; Johnson, B.S.; Nagarjuna, A.; Snyder, M.P. COVID-19–Induced New-Onset Diabetes: Trends and Technologies. Diabetes 2021, 70, 2733–2744. [Google Scholar] [CrossRef]
- Montefusco, L.; Ben Nasr, M.; D’Addio, F.; Loretelli, C.; Rossi, A.; Pastore, I.; Daniele, G.; Abdelsalam, A.; Maestroni, A.; Dell’Acqua, M.; et al. Acute and long-term disruption of glycometabolic control after SARS-CoV-2 infection. Nat. Metab. 2021, 3, 774–785. [Google Scholar] [CrossRef]
- Ghosh, A.; Anjana, R.M.; Shanthi Rani, C.S.; Jeba Rani, S.; Gupta, R.; Jha, A.; Gupta, V.; Kuchay, M.S.; Luthra, A.; Durrani, S.; et al. Glycemic parameters in patients with new-onset diabetes during COVID-19 pandemic are more severe than in patients with new-onset diabetes before the pandemic: NOD COVID India Study. Diabetes Metab. Syndr. 2021, 15, 215–220. [Google Scholar] [CrossRef]
- Tittel, S.R.; Rosenbauer, J.; Kamrath, C.; Ziegler, J.; Reschke, F.; Hammersen, J.; Mönkemöller, K.; Pappa, A.; Kapellen, T.; Holl, R.W. Did the COVID-19 lockdown affect the incidence of pediatric type 1 diabetes in Germany? Diabetes Care 2020, 43, e172–e173. [Google Scholar] [CrossRef] [PubMed]
- Salmi, H.; Heinonen, S.; Hästbacka, J.; Lääperi, M.; Rautiainen, P.; Miettinen, P.J.; Vapalahti, O.; Hepojoki, J.; Knip, M. New-onset type 1 diabetes in Finnish children during the COVID-19 pandemic. Arch. Dis. Child. 2022, 107, 180–185. [Google Scholar] [CrossRef]
- Shrestha, D.B.; Budhathoki, P.; Raut, S.; Adhikari, S.; Ghimire, P.; Thapaliya, S.; Rabaan, A.A.; Karki, B.J. New-onset diabetes in COVID-19 and clinical outcomes: A systematic review and meta-analysis. World J. Virol. 2021, 10, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Mumtaz, M.; Maxwell, A.J.; Isaacs, S.R.; Laiho, J.E.; Rawlinson, W.D.; Hyöty, H.; Craig, M.E.; Kim, K.W. Respiratory infections and Type 1 diabetes: Potential roles in pathogenesis. Rev. Med. Virol. 2023, 33, e2429. [Google Scholar] [CrossRef]
- Omotosho, Y.B.; Ying, G.W.; Stolar, M.; Mallari, A.J.P. COVID-19-Induced Diabetic Ketoacidosis in an Adult with Latent Autoimmune Diabetes. Cureus 2021, 13, e12690. [Google Scholar] [CrossRef]
- Marchand, L.; Pecquet, M.; Luyton, C. Type 1 diabetes onset triggered by COVID-19. Acta Diabetol. 2020, 57, 1265–1266. [Google Scholar] [CrossRef] [PubMed]
- Ssentongo, P.; Zhang, Y.; Witmer, L.; Chinchilli, V.M.; Ba, D.M. Association of COVID-19 with diabetes: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 20191. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, X.; Chen, J.; Zuo, X.; Zhang, H.; Deng, A. COVID-19 infection may cause ketosis and ketoacidosis. Diabetes Obes. Metab. 2020, 22, 1935–1941. [Google Scholar] [CrossRef] [PubMed]
- Gentile, S.; Strollo, F.; Mambro, A.; Ceriello, A. COVID-19, ketoacidosis and new-onset diabetes: Are there possible cause and effect relationships among them? Diabetes Obes. Metab. 2020, 22, 2507–2508. [Google Scholar] [CrossRef]
- Rivero-Martín, M.J.; Rivas-Mercado, C.M.; Ceñal-González-Fierro, M.J.; López-Barrena, N.; Lara-Orejas, E.; Alonso-Martín, D.; Alfaro-Iznaola, C.; Alcázar-Villar, M.J.; Sánchez-Escudero, V.; González-Vergaz, A. Severity of new-onset type 1 diabetes in children and adolescents during the coronavirus-19 disease pandemic. Endocrinol. Diabetes y Nutr. 2022, 69, 810–815. [Google Scholar] [CrossRef]
- Sathish, T.; Tapp, R.J.; Cooper, M.E.; Zimmet, P. Potential metabolic and inflammatory pathways between COVID-19 and new-onset diabetes. Diabetes Metab. 2021, 47, 101204. [Google Scholar] [CrossRef]
- Alomar, F.A. Methylglyoxal in COVID-19-induced hyperglycemia and new-onset diabetes. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 8152–8171. [Google Scholar] [CrossRef]
- Nunez Lopez, Y.O.; Iliuk, A.; Casu, A.; Parikh, A.; Smith, J.S.; Corbin, K.; Lupu, D.; Pratley, R.E. Extracellular vesicle proteomics and phosphoproteomics identify pathways for increased risk in patients hospitalized with COVID-19 and type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2023, 197, 110565. [Google Scholar] [CrossRef]
- Stidsen, J.V.; Green, A.; Rosengaard, L.; Højlund, K. Risk of severe COVID-19 infection in persons with diabetes during the first and second waves in Denmark: A nationwide cohort study. Front. Endocrinol. 2022, 13, 1025699. [Google Scholar] [CrossRef]
- Loza, A.; Wong-Chew, R.M.; Jiménez-Corona, M.E.; Zárate, S.; López, S.; Ciria, R.; Palomares, D.; García-López, R.; Iša, P.; Taboada, B.; et al. Two-year follow-up of the COVID-19 pandemic in Mexico. Front. Public Health 2023, 10, 1050673. [Google Scholar] [CrossRef]
- Uchihara, M.; Sugiyama, T.; Bouchi, R.; Matsunaga, N.; Asai, Y.; Gatanaga, H.; Ohsugi, M.; Ohmagari, N.; Kajio, H.; Ueki, K. Association of acute-to-chronic glycemic ratio and outcomes in patients with COVID-19 and undiagnosed diabetes mellitus: A retrospective nationwide cohort study. J. Diabetes Investig. 2023, 14, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Uchihara, M.; Bouchi, R.; Kodani, N.; Saito, S.; Miyazato, Y.; Umamoto, K.; Sugimoto, H.; Kobayashi, M.; Hikida, S.; Akiyama, Y.; et al. Impact of newly diagnosed diabetes on coronavirus disease 2019 severity and hyperglycemia. J. Diabetes Investig. 2022, 13, 1086–1093. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Vázquez, A.; Bello-Chavolla, O.Y.; Ortiz-Brizuela, E.; Campos-Muñoz, A.; Mehta, R.; Villanueva-Reza, M.; Bahena-López, J.P.; Antonio-Villa, N.E.; González-Lara, M.F.; Ponce De León, A.; et al. Impact of undiagnosed Type 2 diabetes and pre-diabetes on severity and mortality for SARS-CoV-2 infection. BMJ Open Diabetes Res. Care 2021, 9, e002026. [Google Scholar] [CrossRef]
- Miller, L.E.; Bhattacharyya, R.; Miller, A.L. Diabetes mellitus increases the risk of hospital mortality in patients with COVID-19: Systematic review with meta-analysis. Medicine 2020, 99, e22439. [Google Scholar] [CrossRef]
- Sindi, A.A.; Tashkandi, W.A.; Jastaniah, M.W.; Bashanfar, M.A.; Fakhri, A.F.; Alsallum, F.S.; Alguydi, H.B.; Elhazmi, A.; Al-Khatib, T.A.; Alawi, M.M.; et al. Impact of diabetes mellitus and co-morbidities on mortality in patients with COVID-19: A single-center retrospective study. Saudi Med. J. 2023, 44, 67–73. [Google Scholar] [CrossRef]
- Zhang, T.; Mei, Q.; Zhang, Z.; Walline, J.H.; Liu, Y.; Zhu, H.; Zhang, S. Risk for newly diagnosed diabetes after COVID-19: A systematic review and meta-analysis. BMC Med. 2022, 20, 444. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, R.M.; Labad, J.; Sears, A.V.; Williamson, R.M.; Strachan, M.W.J.; Deary, I.J.; Lowe, G.D.O.; Price, J.F.; Walker, B.R. Glucocorticoid treatment and impaired mood, memory and metabolism in people with diabetes: The Edinburgh Type 2 Diabetes Study. Eur. J. Endocrinol. 2012, 166, 861–868. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Park, S.; Oh, K.; Choi, H.; Jeong, E.K. Changes in the management of hypertension, diabetes mellitus, and hypercholesterolemia in Korean adults before and during the COVID-19 pandemic: Data from the 2010–2020 Korea National Health and Nutrition Examination Survey. Epidemiol. Health 2023, 45, e2023014. [Google Scholar] [CrossRef]
- Carr, M.J.; Wright, A.K.; Leelarathna, L.; Thabit, H.; Milne, N.; Kanumilli, N.; Ashcroft, D.M.; Rutter, M.K. Impact of COVID-19 on diagnoses, monitoring, and mortality in people with type 2 diabetes in the UK. Lancet Diabetes Endocrinol. 2021, 9, 413–415. [Google Scholar] [CrossRef]
- Carr, M.J.; Wright, A.K.; Leelarathna, L.; Thabit, H.; Milne, N.; Kanumilli, N.; Ashcroft, D.M.; Rutter, M.K. Impact of COVID-19 restrictions on diabetes health checks and prescribing for people with type 2 diabetes: A UK-wide cohort study involving 618 161 people in primary care. BMJ Qual. Saf. 2022, 31, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Capra, M.E.; Stanyevic, B.; Giudice, A.; Monopoli, D.; Decarolis, N.M.; Esposito, S.; Biasucci, G. The Effects of COVID-19 Pandemic and Lockdown on Pediatric Nutritional and Metabolic Diseases: A Narrative Review. Nutrients 2022, 15, 88. [Google Scholar] [CrossRef]
- Quinn, L.M.; Wong, F.S.; Narendran, P. Environmental Determinants of Type 1 Diabetes: From Association to Proving Causality. Front. Immunol. 2021, 12, 737964. [Google Scholar] [CrossRef] [PubMed]
- Chee, Y.J.; Ng, S.J.H.; Yeoh, E. Diabetic ketoacidosis precipitated by COVID-19 in a patient with newly diagnosed diabetes mellitus. Diabetes Res. Clin. Pract. 2020, 164, 108166. [Google Scholar] [CrossRef] [PubMed]
- Taplin, C.; Barker, J. Autoantibodies in type 1 diabetes. Autoimmunity 2008, 41, 11–18. [Google Scholar] [CrossRef]
- Steenblock, C.; Hassanein, M.; Khan, E.G.; Yaman, M.; Kamel, M.; Barbir, M.; Lorke, D.E.; Rock, J.A.; Everett, D.; Bejtullah, S.; et al. Diabetes and COVID-19: Short- and Long-Term Consequences. Horm. Metab. Res. 2022, 54, 503–509. [Google Scholar] [CrossRef]
- Mamtani, M.; Athavale, A.; Abraham, M.; Vernik, J.; Amarah, A.; Ruiz, J.; Joshi, A.; Itteera, M.; Zhukovski, S.; Madaiah, R.; et al. Association of hyperglycaemia with hospital mortality in nondiabetic COVID-19 patients: A cohort study. Diabetes Metab. 2021, 47, 101254. [Google Scholar] [CrossRef]
- Chourasia, P.; Goyal, L.; Kansal, D.; Roy, S.; Singh, R.; Mahata, I.; Sheikh, A.B.; Shekhar, R. Risk of New-Onset Diabetes Mellitus as a Post-COVID-19 Condition and Possible Mechanisms: A Scoping Review. J. Clin. Med. 2023, 12, 1159. [Google Scholar] [CrossRef] [PubMed]
- Bally, K.; Ji, B.; Soni, L. COVID-19 Vaccine-Induced Latent Autoimmune Diabetes in Adults. Cureus 2023, 15, e33762. [Google Scholar] [CrossRef]
- Lin, R.; Lin, Y.W.; Chen, M.H. Fulminant Type 1 Diabetes Mellitus after SARS-CoV-2 Vaccination: A Case Report. Vaccines 2022, 10, 1905. [Google Scholar] [CrossRef]
- Kshetree, B.; Lee, J.; Acharya, S. COVID-19 Vaccine-Induced Rapid Progression of Prediabetes to Ketosis-Prone Diabetes Mellitus in an Elderly Male. Cureus 2022, 14, e28830. [Google Scholar] [CrossRef]
- Moon, H.; Suh, S.; Park, M.K. Adult-Onset Type 1 Diabetes Development Following COVID-19 mRNA Vaccination. J. Korean Med. Sci. 2023, 38, e12. [Google Scholar] [CrossRef]
- Abu-Rumaileh, M.A.; Gharaibeh, A.M.; Gharaibeh, N.E. COVID-19 Vaccine and Hyperosmolar Hyperglycemic State. Cureus 2021, 13, e14125. [Google Scholar] [CrossRef] [PubMed]
- Edwards, A.E.; Vathenen, R.; Henson, S.M.; Finer, S.; Gunganah, K. Acute hyperglycaemic crisis after vaccination against COVID-19: A case series. Diabet. Med. J. Br. Diabet. Assoc. 2021, 38, e14631. [Google Scholar] [CrossRef]
- Mishra, A.; Ghosh, A.; Dutta, K.; Tyagi, K.; Misra, A. Exacerbation of hyperglycemia in patients with type 2 diabetes after vaccination for COVID19: Report of three cases. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102151. [Google Scholar] [CrossRef] [PubMed]
- Wan, E.Y.F.; Chui, C.S.L.; Mok, A.H.Y.; Xu, W.; Yan, V.K.C.; Lai, F.T.T.; Li, X.; Wong, C.K.H.; Chan, E.W.Y.; Lui, D.T.W.; et al. mRNA (BNT162b2) and Inactivated (CoronaVac) COVID-19 Vaccination and Risk of Adverse Events and Acute Diabetic Complications in Patients with Type 2 Diabetes Mellitus: A Population-Based Study. Drug Saf. 2022, 45, 1477–1490. [Google Scholar] [CrossRef] [PubMed]
- Gouda, N.; Dimitriadou, M.; Sotiriou, G.; Christoforidis, A. The impact of COVID-19 vaccination on glycaemic control in children and adolescents with type 1 diabetes mellitus on continuous glucose monitoring. Acta Diabetol. 2022, 59, 1609–1614. [Google Scholar] [CrossRef]
- López-Contreras, J.E.; Paredes-Casillas, P.; Morales-Romero, J.; Castillo-Vélez, F.E.; Lona-Reyes, J.C.; Bedolla-Barajas, M. Incidence and factors associated with early and late adverse reactions after the first dose of Pfizer-BioNTech vaccine among healthcare workers. Cir. Cir. 2023, 91, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Mallhi, T.H.; Khan, Y.H.; Butt, M.H.; Salman, M.; Tanveer, N.; Alotaibi, N.H.; Alzarea, A.I.; Alanazi, A.S. Surveillance of Side Effects after Two Doses of COVID-19 Vaccines among Patients with Comorbid Conditions: A Sub-Cohort Analysis from Saudi Arabia. Medicina 2022, 58, 1799. [Google Scholar] [CrossRef]
- Heald, A.H.; Jenkins, D.A.; Williams, R.; Mudaliar, R.N.; Naseem, A.; Davies, K.A.B.; Gibson, J.M.; Peng, Y.; Ollier, W. COVID-19 Vaccination and Diabetes Mellitus: How Much Has It Made a Difference to Outcomes Following Confirmed COVID-19 Infection? Diabetes Ther. Res. Treat. Educ. Diabetes Relat. Disord. 2023, 14, 193–204. [Google Scholar] [CrossRef]
- Kwan, A.C.; Ebinger, J.E.; Botting, P.; Navarrette, J.; Claggett, B.; Cheng, S. Association of COVID-19 Vaccination With Risk for Incident Diabetes After COVID-19 Infection. JAMA Netw. Open 2023, 6, e2255965. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Shen, P.; Tao, Y.; Zhang, W.; Xu, B.; Bi, Y.; Han, Z.; Zhou, Y.H. Reduced antibody response to COVID-19 vaccine composed of inactivated SARS-CoV-2 in diabetic individuals. Front. Public Health 2022, 10, 1025901. [Google Scholar] [CrossRef] [PubMed]
- Virgilio, E.; Trevisan, C.; Abbatecola, A.; Malara, A.; Palmieri, A.; Fedele, G.; Stefanelli, P.; Leone, P.; Schiavoni, I.; Maggi, S.; et al. Diabetes Affects Antibody Response to SARS-CoV-2 Vaccination in Older Residents of Long-term Care Facilities: Data From the GeroCovid Vax Study. Diabetes Care 2022, 45, 2935–2942. [Google Scholar] [CrossRef]
- van den Berg, J.M.; Remmelzwaal, S.; Blom, M.T.; van Hoek, B.A.C.E.; Swart, K.M.A.; Overbeek, J.A.; Burchell, G.L.; Herings, R.M.C.; Elders, P.J.M. Effectiveness of COVID-19 Vaccines in Adults with Diabetes Mellitus: A Systematic Review. Vaccines 2022, 11, 24. [Google Scholar] [CrossRef]
- D’Onofrio, L.; Fogolari, M.; Amendolara, R.; Siena, A.; De Fata, R.; Davini, F.; Coraggio, L.; Mignogna, C.; Moretti, C.; Maddaloni, E.; et al. Reduced early response to SARS-CoV2 vaccination in people with type 1 and type 2 diabetes, a 6 months follow-up study: The CoVaDiab study I. Diabetes/Metabolism Res. Rev. 2023, 39, e3601. [Google Scholar] [CrossRef]
- Steenblock, C.; Richter, S.; Berger, I.; Barovic, M.; Schmid, J.; Schubert, U.; Jarzebska, N.; von Mässenhausen, A.; Linkermann, A.; Schürmann, A.; et al. Viral infiltration of pancreatic islets in patients with COVID-19. Nat. Commun. 2021, 12, 3534. [Google Scholar] [CrossRef] [PubMed]
- Reiterer, M.; Rajan, M.; Gómez-Banoy, N.; Lau, J.D.; Gomez-Escobar, L.G.; Ma, L.; Gilani, A.; Alvarez-Mulett, S.; Sholle, E.T.; Chandar, V.; et al. Hyperglycemia in acute COVID-19 is characterized by insulin resistance and adipose tissue infectivity by SARS-CoV-2. Cell Metab. 2021, 33, 2174–2188.e5. [Google Scholar] [CrossRef]
- Ali Abdelhamid, Y.; Kar, P.; Finnis, M.E.; Phillips, L.K.; Plummer, M.P.; Shaw, J.E.; Horowitz, M.; Deane, A.M. Stress hyperglycaemia in critically ill patients and the subsequent risk of diabetes: A systematic review and meta-analysis. Crit. Care 2016, 20, 301. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Tang, X.; Uhl, S.; Zhang, T.; Xue, D.; Li, B.; Vandana, J.J.; Acklin, J.A.; Bonnycastle, L.L.; Narisu, N.; Erdos, M.R.; et al. SARS-CoV-2 infection induces beta cell transdifferentiation. Cell Metab. 2021, 33, 1577–1591.e7. [Google Scholar] [CrossRef]
- Müller, J.A.; Groß, R.; Conzelmann, C.; Krüger, J.; Merle, U.; Steinhart, J.; Weil, T.; Koepke, L.; Bozzo, C.P.; Read, C.; et al. SARS-CoV-2 infects and replicates in cells of the human endocrine and exocrine pancreas. Nat. Metab. 2021, 3, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Ahlqvist, E.; Storm, P.; Käräjämäki, A.; Martinell, M.; Dorkhan, M.; Carlsson, A.; Vikman, P.; Prasad, R.B.; Aly, D.M.; Almgren, P.; et al. Novel subgroups of adult-onset diabetes and their association with outcomes: A data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol. 2018, 6, 361–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First Case of 2019 Novel Coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef]
- Caruso, P.; Longo, M.; Esposito, K.; Maiorino, M.I. Type 1 diabetes triggered by covid-19 pandemic: A potential outbreak? Diabetes Res. Clin. Pract. 2020, 164, 108219. [Google Scholar] [CrossRef]
- Christen, U.; Edelmann, K.H.; McGavern, D.B.; Wolfe, T.; Coon, B.; Teague, M.K.; Miller, S.D.; Oldstone, M.B.; Von Herrath, M.G. A viral epitope that mimics a self antigen can accelerate but not initiate autoimmune diabetes. J. Clin. Investig. 2004, 114, 1290–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dotan, A.; Muller, S.; Kanduc, D.; David, P.; Halpert, G.; Shoenfeld, Y. The SARS-CoV-2 as an instrumental trigger of autoimmunity. Autoimmun. Rev. 2021, 20, 102792. [Google Scholar] [CrossRef]
- Santos, A.; Magro, D.O.; Evangelista-Poderoso, R.; Saad, M.J.A. Diabetes, obesity, and insulin resistance in COVID-19: Molecular interrelationship and therapeutic implications. Diabetol. Metab. Syndr. 2021, 13, 23. [Google Scholar] [CrossRef]
- Montezano, A.C.; Nguyen Dinh Cat, A.; Rios, F.J.; Touyz, R.M. Angiotensin II and Vascular Injury. Curr. Hypertens. Rep. 2014, 16, 431. [Google Scholar] [CrossRef]
- Govender, N.; Khaliq, O.P.; Moodley, J.; Naicker, T. Insulin resistance in COVID-19 and diabetes. Prim. Care Diabetes 2021, 15, 629–634. [Google Scholar] [CrossRef]
- He, X.; Liu, C.; Peng, J.; Li, Z.; Li, F.; Wang, J.; Hu, A.; Peng, M.; Huang, K.; Fan, D.; et al. COVID-19 induces new-onset insulin resistance and lipid metabolic dysregulation via regulation of secreted metabolic factors. Signal Transduct. Target. Ther. 2021, 6, 427. [Google Scholar] [CrossRef]
- Cron, R.Q.; Caricchio, R.; Chatham, W.W. Calming the cytokine storm in COVID-19. Nat. Med. 2021, 27, 1674–1675. [Google Scholar] [CrossRef]
- Hirano, T.; Murakami, M. COVID-19: A New Virus, but a Familiar Receptor and Cytokine Release Syndrome. Immunity 2020, 52, 731–733. [Google Scholar] [CrossRef] [PubMed]
- Šestan, M.; Marinović, S.; Kavazović, I.; Cekinović, Đ.; Wueest, S.; Turk Wensveen, T.; Brizić, I.; Jonjić, S.; Konrad, D.; Wensveen, F.M.; et al. Virus-Induced Interferon-γ Causes Insulin Resistance in Skeletal Muscle and Derails Glycemic Control in Obesity. Immunity 2018, 49, 164–177.e6. [Google Scholar] [CrossRef] [Green Version]
- Calcaterra, V.; Bosoni, P.; Dilillo, D.; Mannarino, S.; Fiori, L.; Fabiano, V.; Carlucci, P.; Di Profio, E.; Verduci, E.; Mameli, C.; et al. Impaired Glucose-Insulin Metabolism in Multisystem Inflammatory Syndrome Related to SARS-CoV-2 in Children. Children 2021, 8, 384. [Google Scholar] [CrossRef] [PubMed]
- Ilias, I.; Diamantopoulos, A.; Pratikaki, M.; Botoula, E.; Jahaj, E.; Athanasiou, N.; Tsipilis, S.; Zacharis, A.; Vassiliou, A.G.; Vassiliadi, D.A.; et al. Glycemia, Beta-Cell Function and Sensitivity to Insulin in Mildly to Critically Ill COVID-19 Patients. Medicina 2021, 57, 68. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Type of Study | Country | Number of Cases | Results |
|---|---|---|---|---|
| Sathish et al. [62] | Meta-analysis | China, Italy, US | 3711 patients | 14.4% of the population had new-onset diabetes |
| Sathish et al. [63] | Retrospective study | India | 102 patients | 20.6% of the population had new-onset diabetes |
| Li et al. [11] | Retrospective study | China | 453 patients | 20.8% of the population had new-onset diabetes |
| Unsworth et al. [65] | Retrospective study | UK | 30 children | 80% increase in new-onset T1DM |
| Tittel et al. [77] | Prospective study | Germany | Children from 216 paediatric diabetes centres | T1DM incidence increased from 16.4 per 100,000 to 22.2 per 100,000 |
| Salmi et al. [78] | Retrospective study | Finland | Children admitted to PICU due to new-onset diabetes compared with the pre-pandemic period | The number of children admitted to PICU due to new-onset diabetes increased from 6.25 in 2016 to 20 in 2020. |
| Montefusco et al. [75] | Retrospective study | Italy | 551 patients | 46% were hyperglycaemic |
| Kamrath et al. [66] | Prospective study | Germany | 532 newly diagnosed T1DM | The frequency of diabetic ketoacidosis was 44.7% |
| Fadini et al. [13] | Retrospective study | Italy | 413 patients | 5% had new-onset diabetes |
| Ghosh et al. [76] | Retrospective study | India | 555 patients with new-onset diabetes | Patients with new-onset diabetes had worse glycaemic parameters |
| Shrestha et al. [79] | Meta-analysis | US, China, France, India, Italy | 1943 patients across seven studies | The mortality rate in COVID-19-associated diabetes patients was 25% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grubišić, B.; Švitek, L.; Ormanac, K.; Sabo, D.; Mihaljević, I.; Bilić-Ćurčić, I.; Omanović Kolarić, T. Molecular Mechanisms Responsible for Diabetogenic Effects of COVID-19 Infection—Induction of Autoimmune Dysregulation and Metabolic Disturbances. Int. J. Mol. Sci. 2023, 24, 11576. https://doi.org/10.3390/ijms241411576
Grubišić B, Švitek L, Ormanac K, Sabo D, Mihaljević I, Bilić-Ćurčić I, Omanović Kolarić T. Molecular Mechanisms Responsible for Diabetogenic Effects of COVID-19 Infection—Induction of Autoimmune Dysregulation and Metabolic Disturbances. International Journal of Molecular Sciences. 2023; 24(14):11576. https://doi.org/10.3390/ijms241411576
Chicago/Turabian StyleGrubišić, Barbara, Luka Švitek, Klara Ormanac, Dea Sabo, Ivica Mihaljević, Ines Bilić-Ćurčić, and Tea Omanović Kolarić. 2023. "Molecular Mechanisms Responsible for Diabetogenic Effects of COVID-19 Infection—Induction of Autoimmune Dysregulation and Metabolic Disturbances" International Journal of Molecular Sciences 24, no. 14: 11576. https://doi.org/10.3390/ijms241411576