
Liquid Biopsy in Hepatocellular Carcinoma: The Significance of Circulating Tumor Cells in Diagnosis, Prognosis, and Treatment Monitoring

Abstract
:1. Introduction
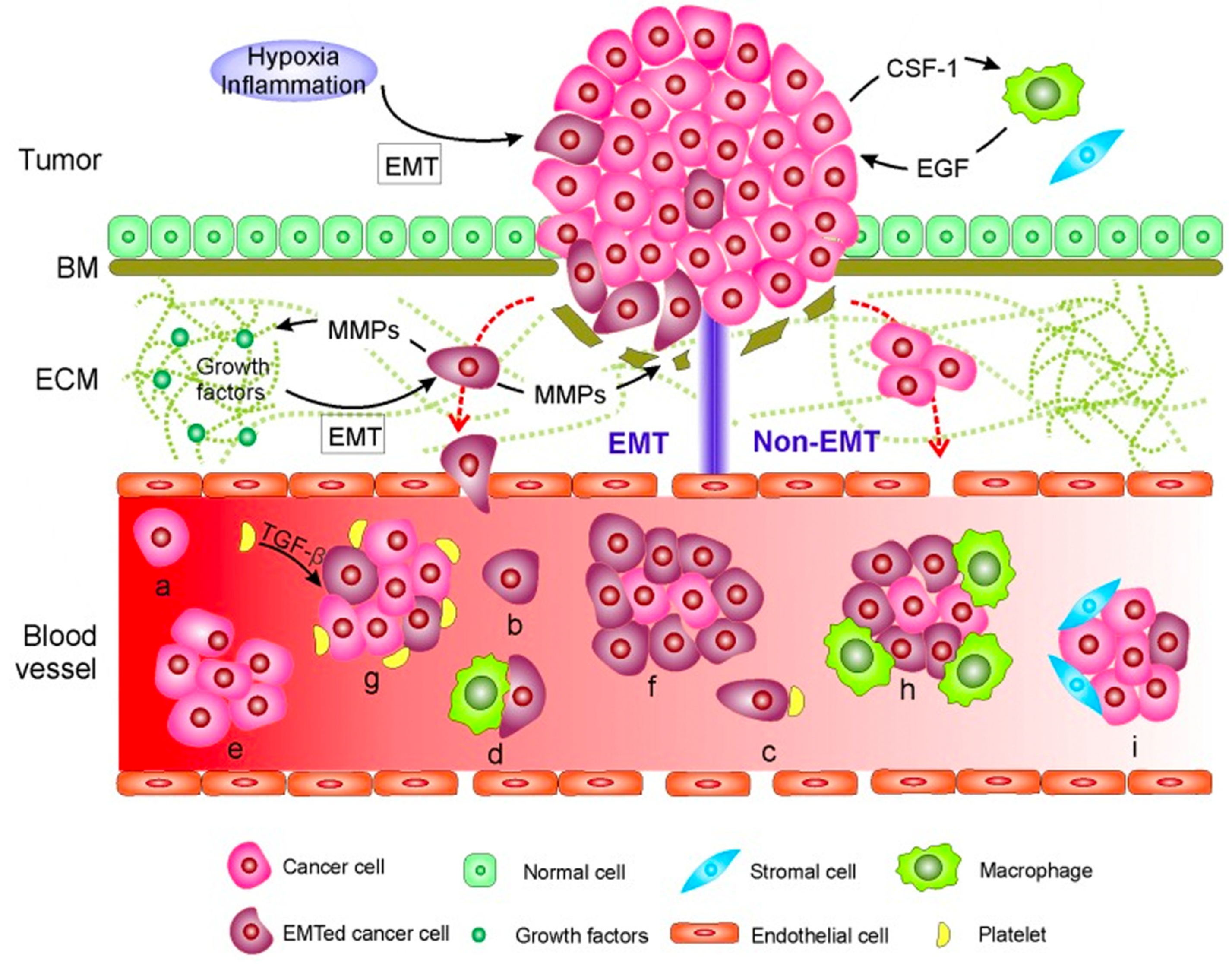
2. Circulating Tumor Cells-Definition and Biology
3. Techniques of Isolation
4. Clinical Application of Circulating Tumor Cells
4.1. Circulating Tumor Cells for Early Detection
4.2. Circulating Tumor Cells for Prognostication
4.3. Circulating Tumor Cells in Setting of Treatment
4.3.1. In the Setting of Liver Resection
4.3.2. Determining Surgical Margins Prior to Liver Resection
4.3.3. In the Setting of Liver-Directed Therapies
4.3.4. In the Setting of Liver Transplantation
4.3.5. In the Setting of Systemic Therapy
4.4. Clinical Trials Investigating the Use of Circulating Tumor Cells in the Context of Hepatocellular Carcinoma
5. Challenges and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Glossary
| AFP | alpha-fetoprotein |
| Anoikis | programmed cell death upon detachment of cells from the extracellular matrix and neighboring cells |
| ASGPR | asialoglycoprotein receptor |
| BCLC | Barcelona clinic liver cancer |
| C6/MMSN-GPC3 | CTC capturing system that utilizes immunomagnetic fluorescent nanodevices targeting GPC3 |
| CECs | circulating epithelial cells |
| cHCC-CCA | combined hepatocellular-cholangiocarcinoma |
| CPS1 | carbamoyl phosphate synthetase 1 |
| CSCs | : cancer stem cells |
| CT | computed tomography |
| CTCs | circulating tumor cells - tumor cells that have detached from the primary tumor and circulate in the bloodstream |
| CTC-WBC | clusters composed of CTCs and white blood cells circulating in the bloodstream |
| ctDNA | circulating tumor DNA - tumor-derived fragmented DNA originating from primary or metastatic cancer sites. |
| DFS | disease-free survival |
| EHM | extrahepatic metastasis |
| EMT | epithelial-to-mesenchymal transition – a cellular process in which epithelial cells acquire mesenchymal phenotypes and behavior |
| EpCAM | epithelial cell adhesion molecule |
| ER | early recurrence |
| FISH | fluorescence in situ hybridization |
| FMSA | flexible micro spring array |
| GNB4 | guanine nucleotide-binding protein subunit beta-4 |
| GPC3 | glypican-3 |
| HCC | hepatocellular carcinoma |
| HKR | higher karyoplasmic ratio |
| ICAM | intercellular adhesion molecule |
| ISET | isolation by size of tumor cells |
| ISH | in situ hybridization |
| LDT | liver-directed therapy |
| Liquid biopsy | A laboratory test conducted on a blood, urine, or other body fluid sample to detect cancer cells derived from a tumor or small fragments of DNA, RNA, or other molecules released by tumor cells |
| LR | liver resection |
| LT | liver transplantation |
| MACS | magnetic-activated cell separation |
| M-CTCs | mesenchymal phenotype of CTCs |
| MELD | model for end-stage liver disease |
| MMP | matrix-metalloproteinase |
| MVI | microvascular invasion |
| MWA | microwave ablation |
| MRI | magnetic resonance imaging |
| mPVI | macroscopic portal vein invasion |
| NAFLD | nonalcoholic fatty liver disease |
| NLR | neutrophil-lymphocyte ratio |
| OLT | orthotopic liver transplantation |
| ORR | objective response rate |
| OS | overall survival |
| PAFC | photoacoustic flow cytometry |
| P-CK | pan-cytokeratin |
| PFS | progression-free survival |
| R0 resection | surgical margin microscopically-negative for residual tumor |
| RFA | radiofrequency ablation |
| RFS | relapse-free survival |
| RT-PCR | reverse transcription-polymerase chain reaction |
| SE-iFISH | subtraction enrichment and immunostaining-fluorescence in situ hybridization |
| SERS | surface-enhanced Raman scattering |
| sMVP | surface major vault protein |
| TACE | transarterial chemoembolization |
| TARE | transarterial radioembolization |
| TFS | tumor-free survival |
| TTR | time-to-recurrence |
| Tumor-derived exosomes | small extracellular vesicles secreted by cancer cells |
| TNM | tumor (T), nodes (N), and metastases |
| UCSF | University of California San Francisco |
| US | ultrasonography |
| VEGF | vascular endothelial growth factor |
References
- Available online: https://gco.iarc.fr/today/data/factsheets/cancers/11-Liver-fact-sheet.pdf (accessed on 12 June 2023).
- Dasgupta, P.; Henshaw, C.; Youlden, D.R.; Clark, P.J.; Aitken, J.F.; Baade, P.D. Global Trends in Incidence Rates of Primary Adult Liver Cancers: A Systematic Review and Meta-Analysis. Front. Oncol. 2020, 10, 171. [Google Scholar] [CrossRef]
- El-Serag, H.B. Epidemiology of Viral Hepatitis and Hepatocellular Carcinoma. Gastroenterology 2012, 142, 1264–1273.e1. [Google Scholar] [CrossRef]
- Kim, D.Y.; Han, K.-H. Epidemiology and Surveillance of Hepatocellular Carcinoma. Liver Cancer 2012, 1, 2–14. [Google Scholar] [CrossRef] [PubMed]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the Epidemic of Nonalcoholic Fatty Liver Disease Demonstrates an Exponential Increase in Burden of Disease. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Perz, J.F.; Armstrong, G.L.; Farrington, L.A.; Hutin, Y.J.F.; Bell, B.P. The Contributions of Hepatitis B Virus and Hepatitis C Virus Infections to Cirrhosis and Primary Liver Cancer Worldwide. J. Hepatol. 2006, 45, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular Carcinoma. Nat. Rev. Dis. Prim. 2021, 7, 6. [Google Scholar] [CrossRef]
- Kow, A.W.C. Transplantation versus Liver Resection in Patients with Hepatocellular Carcinoma. Transl. Gastroenterol. Hepatol. 2019, 4, 33. [Google Scholar] [CrossRef]
- Cucchetti, A.; Piscaglia, F.; Cescon, M.; Colecchia, A.; Ercolani, G.; Bolondi, L.; Pinna, A.D. Cost-Effectiveness of Hepatic Resection versus Percutaneous Radiofrequency Ablation for Early Hepatocellular Carcinoma. J. Hepatol. 2013, 59, 300–307. [Google Scholar] [CrossRef]
- Golfieri, R.; Garzillo, G.; Ascanio, S.; Renzulli, M. Focal Lesions in the Cirrhotic Liver: Their Pivotal Role in Gadoxetic Acid-Enhanced MRI and Recognition by the Western Guidelines. Dig. Dis. 2014, 32, 696–704. [Google Scholar] [CrossRef]
- Granito, A.; Facciorusso, A.; Sacco, R.; Bartalena, L.; Mosconi, C.; Cea, U.V.; Cappelli, A.; Antonino, M.; Modestino, F.; Brandi, N.; et al. TRANS-TACE: Prognostic Role of the Transient Hypertransaminasemia after Conventional Chemoembolization for Hepatocellular Carcinoma. J. Pers. Med. 2021, 11, 1041. [Google Scholar] [CrossRef]
- Guarino, M.; Viganò, L.; Ponziani, F.R.; Giannini, E.G.; Lai, Q.; Morisco, F.; Special Interest Group on Hepatocellular carcinoma and new anti-HCV therapies” of the Italian Association for the Study of the Liver. Recurrence of Hepatocellular Carcinoma after Direct Acting Antiviral Treatment for Hepatitis C Virus Infection: Literature Review and Risk Analysis. Dig. Liver Dis. 2018, 50, 1105–1114. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.G.; Lampertico, P.; Nahon, P. Epidemiology and Surveillance for Hepatocellular Carcinoma: New Trends. J. Hepatol. 2020, 72, 250–261. [Google Scholar] [CrossRef]
- Villanueva, A.; Minguez, B.; Forner, A.; Reig, M.; Llovet, J.M. Hepatocellular Carcinoma: Novel Molecular Approaches for Diagnosis, Prognosis, and Therapy. Annu. Rev. Med. 2010, 61, 317–328. [Google Scholar] [CrossRef]
- Toyoda, H.; Kumada, T.; Tada, T.; Sone, Y.; Kaneoka, Y.; Maeda, A. Tumor Markers for Hepatocellular Carcinoma: Simple and Significant Predictors of Outcome in Patients with HCC. Liver Cancer 2015, 4, 126–136. [Google Scholar] [CrossRef]
- Baig, J.A.; Alam, J.M.; Mahmood, S.R.; Baig, M.; Shaheen, R.; Sultana, I.; Waheed, A. Hepatocellular Carcinoma (HCC) and Diagnostic Significance of A-Fetoprotein (AFP). J. Ayub Med. Coll. Abbottabad 2009, 21, 72–75. [Google Scholar]
- Hua, Y.; Dong, J.; Hong, J.; Wang, B.; Yan, Y.; Li, Z. Clinical Applications of Circulating Tumor Cells in Hepatocellular Carcinoma. Front. Oncol. 2022, 12, 968591. [Google Scholar] [CrossRef]
- Renzulli, M.; Golfieri, R.; Bologna Liver Oncology Group (BLOG). Proposal of a New Diagnostic Algorithm for Hepatocellular Carcinoma Based on the Japanese Guidelines but Adapted to the Western World for Patients under Surveillance for Chronic Liver Disease. J. Gastroenterol. Hepatol. 2016, 31, 69–80. [Google Scholar] [CrossRef]
- Sherman, M. Limitations of Screening for Hepatocellular Carcinoma. Hepatic Oncol. 2014, 1, 161–163. [Google Scholar] [CrossRef]
- Andersson, K.L.; Salomon, J.A.; Goldie, S.J.; Chung, R.T. Cost Effectiveness of Alternative Surveillance Strategies for Hepatocellular Carcinoma in Patients with Cirrhosis. Clin. Gastroenterol. Hepatol. 2008, 6, 1418–1424. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Renzulli, M.; Pecorelli, A.; Brandi, N.; Brocchi, S.; Tovoli, F.; Granito, A.; Carrafiello, G.; Ierardi, A.M.; Golfieri, R. The Feasibility of Liver Biopsy for Undefined Nodules in Patients under Surveillance for Hepatocellular Carcinoma: Is Biopsy Really a Useful Tool? J. Clin. Med. Res. 2022, 11, 4399. [Google Scholar] [CrossRef] [PubMed]
- Friemel, J.; Rechsteiner, M.; Frick, L.; Böhm, F.; Struckmann, K.; Egger, M.; Moch, H.; Heikenwalder, M.; Weber, A. Intratumor Heterogeneity in Hepatocellular Carcinoma. Clin. Cancer Res. 2015, 21, 1951–1961. [Google Scholar] [PubMed]
- Kuhn, P.; Bethel, K. A Fluid Biopsy as Investigating Technology for the Fluid Phase of Solid Tumors. Phys. Biol. 2012, 9, 010301. [Google Scholar] [CrossRef]
- Siravegna, G.; Marsoni, S.; Siena, S.; Bardelli, A. Integrating Liquid Biopsies into the Management of Cancer. Nat. Rev. Clin. Oncol. 2017, 14, 531–548. [Google Scholar]
- Adeniji, N.; Dhanasekaran, R. Current and Emerging Tools for Hepatocellular Carcinoma Surveillance. Hepatol. Commun. 2021, 5, 1972–1986. [Google Scholar] [PubMed]
- Temraz, S.; Nasr, R.; Mukherji, D.; Kreidieh, F.; Shamseddine, A. Liquid Biopsy Derived Circulating Tumor Cells and Circulating Tumor DNA as Novel Biomarkers in Hepatocellular Carcinoma. Expert Rev. Mol. Diagn. 2022, 22, 507–518. [Google Scholar] [CrossRef]
- Keller, L.; Pantel, K. Unravelling Tumour Heterogeneity by Single-Cell Profiling of Circulating Tumour Cells. Nat. Rev. Cancer 2019, 19, 553–567. [Google Scholar]
- Tr, A. A Case of Cancer in Which Cells Similar to Those in the Tumours Were Seen in the Blood after Death. Australas. Med. J. 1869, 14, 146. [Google Scholar]
- Camara, O.; Kavallaris, A.; Nöschel, H.; Rengsberger, M.; Jörke, C.; Pachmann, K. Seeding of Epithelial Cells into Circulation during Surgery for Breast Cancer: The Fate of Malignant and Benign Mobilized Cells. World J. Surg. Oncol. 2006, 4, 67. [Google Scholar]
- McDonald, D.M.; Baluk, P. Significance of Blood Vessel Leakiness in Cancer. Cancer Res. 2002, 62, 5381–5385. [Google Scholar] [PubMed]
- Joosse, S.A.; Gorges, T.M.; Pantel, K. Biology, Detection, and Clinical Implications of Circulating Tumor Cells. EMBO Mol. Med. 2015, 7, 1–11. [Google Scholar] [PubMed]
- Chen, L.; Bode, A.M.; Dong, Z. Circulating Tumor Cells: Moving Biological Insights into Detection. Theranostics 2017, 7, 2606–2619. [Google Scholar] [CrossRef]
- Celià-Terrassa, T.; Kang, Y. Distinctive Properties of Metastasis-Initiating Cells. Genes Dev. 2016, 30, 892–908. [Google Scholar] [PubMed]
- Thiery, J.P.; Acloque, H.; Huang, R.Y.J.; Nieto, M.A. Epithelial-Mesenchymal Transitions in Development and Disease. Cell 2009, 139, 871–890. [Google Scholar]
- Pencheva, N.; Tavazoie, S.F. Control of Metastatic Progression by microRNA Regulatory Networks. Nat. Cell Biol. 2013, 15, 546–554. [Google Scholar]
- Tam, W.L.; Weinberg, R.A. The Epigenetics of Epithelial-Mesenchymal Plasticity in Cancer. Nat. Med. 2013, 19, 1438–1449. [Google Scholar]
- Conley, S.J.; Gheordunescu, E.; Kakarala, P.; Newman, B.; Korkaya, H.; Heath, A.N.; Clouthier, S.G.; Wicha, M.S. Antiangiogenic Agents Increase Breast Cancer Stem Cells via the Generation of Tumor Hypoxia. Proc. Natl. Acad. Sci. USA 2012, 109, 2784–2789. [Google Scholar] [CrossRef]
- Kessenbrock, K.; Plaks, V.; Werb, Z. Matrix Metalloproteinases: Regulators of the Tumor Microenvironment. Cell 2010, 141, 52–67. [Google Scholar]
- Godinho, S.A.; Picone, R.; Burute, M.; Dagher, R.; Su, Y.; Leung, C.T.; Polyak, K.; Brugge, J.S.; Théry, M.; Pellman, D. Oncogene-like Induction of Cellular Invasion from Centrosome Amplification. Nature 2014, 510, 167–171. [Google Scholar] [CrossRef]
- Sun, Y.-F.; Guo, W.; Xu, Y.; Shi, Y.-H.; Gong, Z.-J.; Ji, Y.; Du, M.; Zhang, X.; Hu, B.; Huang, A.; et al. Circulating Tumor Cells from Different Vascular Sites Exhibit Spatial Heterogeneity in Epithelial and Mesenchymal Composition and Distinct Clinical Significance in Hepatocellular Carcinoma. Clin. Cancer Res. 2018, 24, 547–559. [Google Scholar] [CrossRef]
- Zimmermann, A. Invasion Patterns and Metastatic Patterns of Hepatocellular Carcinoma. In Tumors and Tumor-Like Lesions of the Hepatobiliary Tract; Springer: Cham, Switzerland, 2017; pp. 91–119. [Google Scholar]
- Moldogazieva, N.T.; Zavadskiy, S.P.; Terentiev, A.A. Genomic Landscape of Liquid Biopsy for Hepatocellular Carcinoma Personalized Medicine. Cancer Genom. Proteom. 2021, 18, 369–383. [Google Scholar] [CrossRef]
- Bhan, I.; Haber, D.A.; Chung, R.T.; Ting, D.T. Liquid Biopsy in Hepatocellular Carcinoma. In Hepatocellular Carcinoma: Translational Precision Medicine Approaches; Hoshida, Y., Ed.; Humana Press: Cham, Switzerland, 2019; ISBN 9783030215392. [Google Scholar]
- Espejo-Cruz, M.L.; González-Rubio, S.; Zamora-Olaya, J.; Amado-Torres, V.; Alejandre, R.; Sánchez-Frías, M.; Ciria, R.; De la Mata, M.; Rodríguez-Perálvarez, M.; Ferrín, G. Circulating Tumor Cells in Hepatocellular Carcinoma: A Comprehensive Review and Critical Appraisal. Int. J. Mol. Sci. 2021, 22, 13073. [Google Scholar] [CrossRef]
- Lin, D.; Shen, L.; Luo, M.; Zhang, K.; Li, J.; Yang, Q.; Zhu, F.; Zhou, D.; Zheng, S.; Chen, Y.; et al. Circulating Tumor Cells: Biology and Clinical Significance. Signal Transduct. Target. Ther. 2021, 6, 404. [Google Scholar] [PubMed]
- Chen, J.; Cao, S.-W.; Cai, Z.; Zheng, L.; Wang, Q. Epithelial-Mesenchymal Transition Phenotypes of Circulating Tumor Cells Correlate with the Clinical Stages and Cancer Metastasis in Hepatocellular Carcinoma Patients. Cancer Biomark. 2017, 20, 487–498. [Google Scholar]
- Ou, H.; Huang, Y.; Xiang, L.; Chen, Z.; Fang, Y.; Lin, Y.; Cui, Z.; Yu, S.; Li, X.; Yang, D. Circulating Tumor Cell Phenotype Indicates Poor Survival and Recurrence After Surgery for Hepatocellular Carcinoma. Dig. Dis. Sci. 2018, 63, 2373–2380. [Google Scholar]
- Eschrich, J.; Kobus, Z.; Geisel, D.; Halskov, S.; Roßner, F.; Roderburg, C.; Mohr, R.; Tacke, F. The Diagnostic Approach towards Combined Hepatocellular-Cholangiocarcinoma-State of the Art and Future Perspectives. Cancers 2023, 15, 301. [Google Scholar] [CrossRef]
- Ahn, J.C.; Teng, P.-C.; Chen, P.-J.; Posadas, E.; Tseng, H.-R.; Lu, S.C.; Yang, J.D. Detection of Circulating Tumor Cells and Their Implications as a Biomarker for Diagnosis, Prognostication, and Therapeutic Monitoring in Hepatocellular Carcinoma. Hepatology 2021, 73, 422–436. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; Yang, Y.; Miao, H.; Redublo, P.; Liu, H.; Liu, W.; Huang, Y.-W.; Teng, P.-C.; Zhang, C.; Zhang, R.Y.; et al. Discovery and Characterization of Circulating Tumor Cell Clusters in Neuroendocrine Tumor Patients Using Nanosubstrate-Embedded Microchips. Biosens. Bioelectron. 2022, 199, 113854. [Google Scholar] [PubMed]
- Kalinich, M.; Bhan, I.; Kwan, T.T.; Miyamoto, D.T.; Javaid, S.; LiCausi, J.A.; Milner, J.D.; Hong, X.; Goyal, L.; Sil, S.; et al. An RNA-Based Signature Enables High Specificity Detection of Circulating Tumor Cells in Hepatocellular Carcinoma. Proc. Natl. Acad. Sci. USA 2017, 114, 1123–1128. [Google Scholar]
- Teng, P.-C.; Agopian, V.G.; Lin, T.-Y.; You, S.; Zhu, Y.; Tseng, H.-R.; Yang, J.D. Circulating Tumor Cells: A Step toward Precision Medicine in Hepatocellular Carcinoma. J. Gastroenterol. Hepatol. 2022, 37, 1179–1190. [Google Scholar] [CrossRef]
- Miller, M.C.; Doyle, G.V.; Terstappen, L.W.M.M. Significance of Circulating Tumor Cells Detected by the CellSearch System in Patients with Metastatic Breast Colorectal and Prostate Cancer. J. Oncol. 2010, 2010, 617421. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, L.; Zhang, X.; Zhang, Y.; Liu, H.; Sun, B.; Zhao, L.; Ge, N.; Qian, H.; Yang, Y.; et al. Detection of Circulating Tumor Cells in Hepatocellular Carcinoma Using Antibodies against Asialoglycoprotein Receptor, Carbamoyl Phosphate Synthetase 1 and Pan-Cytokeratin. PLoS ONE 2014, 9, e96185. [Google Scholar]
- Ferreira, M.M.; Ramani, V.C.; Jeffrey, S.S. Circulating Tumor Cell Technologies. Mol. Oncol. 2016, 10, 374–394. [Google Scholar] [PubMed]
- Nagrath, S.; Sequist, L.V.; Maheswaran, S.; Bell, D.W.; Irimia, D.; Ulkus, L.; Smith, M.R.; Kwak, E.L.; Digumarthy, S.; Muzikansky, A.; et al. Isolation of Rare Circulating Tumour Cells in Cancer Patients by Microchip Technology. Nature 2007, 450, 1235–1239. [Google Scholar] [CrossRef]
- Karabacak, N.M.; Spuhler, P.S.; Fachin, F.; Lim, E.J.; Pai, V.; Ozkumur, E.; Martel, J.M.; Kojic, N.; Smith, K.; Chen, P.-I.; et al. Microfluidic, Marker-Free Isolation of Circulating Tumor Cells from Blood Samples. Nat. Protoc. 2014, 9, 694–710. [Google Scholar]
- Vona, G.; Estepa, L.; Béroud, C.; Damotte, D.; Capron, F.; Nalpas, B.; Mineur, A.; Franco, D.; Lacour, B.; Pol, S.; et al. Impact of Cytomorphological Detection of Circulating Tumor Cells in Patients with Liver Cancer. Hepatology 2004, 39, 792–797. [Google Scholar]
- Wu, S.; Liu, S.; Liu, Z.; Huang, J.; Pu, X.; Li, J.; Yang, D.; Deng, H.; Yang, N.; Xu, J. Classification of Circulating Tumor Cells by Epithelial-Mesenchymal Transition Markers. PLoS ONE 2015, 10, e0123976. [Google Scholar] [CrossRef] [PubMed]
- Vona, G.; Sabile, A.; Louha, M.; Sitruk, V.; Romana, S.; Schütze, K.; Capron, F.; Franco, D.; Pazzagli, M.; Vekemans, M.; et al. Isolation by Size of Epithelial Tumor Cells: A New Method for the Immunomorphological and Molecular Characterization of Circulatingtumor Cells. Am. J. Pathol. 2000, 156, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Martel, J.M.; Toner, M. Inertial Focusing in Microfluidics. Annu. Rev. Biomed. Eng. 2014, 16, 371–396. [Google Scholar] [CrossRef]
- Abonnenc, M.; Manaresi, N.; Borgatti, M.; Medoro, G.; Fabbri, E.; Romani, A.; Altomare, L.; Tartagni, M.; Rizzo, R.; Baricordi, O.; et al. Programmable Interactions of Functionalized Single Bioparticles in a Dielectrophoresis-Based Microarray Chip. Anal. Chem. 2013, 85, 8219–8224. [Google Scholar] [PubMed]
- Liu, Z.; Guo, W.; Zhang, D.; Pang, Y.; Shi, J.; Wan, S.; Cheng, K.; Wang, J.; Cheng, S. Circulating Tumor Cell Detection in Hepatocellular Carcinoma Based on Karyoplasmic Ratios Using Imaging Flow Cytometry. Sci. Rep. 2016, 6, 39808. [Google Scholar] [PubMed]
- Chen, J.-F.; Ho, H.; Lichterman, J.; Lu, Y.-T.; Zhang, Y.; Garcia, M.A.; Chen, S.-F.; Liang, A.-J.; Hodara, E.; Zhau, H.E.; et al. Subclassification of Prostate Cancer Circulating Tumor Cells by Nuclear Size Reveals Very Small Nuclear Circulating Tumor Cells in Patients with Visceral Metastases. Cancer 2015, 121, 3240–3251. [Google Scholar] [PubMed]
- Went, P.T.; Lugli, A.; Meier, S.; Bundi, M.; Mirlacher, M.; Sauter, G.; Dirnhofer, S. Frequent EpCam Protein Expression in Human Carcinomas. Hum. Pathol. 2004, 35, 122–128. [Google Scholar] [CrossRef]
- Yang, J.-C.; Hu, J.-J.; Li, Y.-X.; Luo, W.; Liu, J.-Z.; Ye, D.-W. Clinical Applications of Liquid Biopsy in Hepatocellular Carcinoma. Front. Oncol. 2022, 12, 781820. [Google Scholar]
- Li, Y.-M.; Xu, S.-C.; Li, J.; Han, K.-Q.; Pi, H.-F.; Zheng, L.; Zuo, G.-H.; Huang, X.-B.; Li, H.-Y.; Zhao, H.-Z.; et al. Epithelial-Mesenchymal Transition Markers Expressed in Circulating Tumor Cells in Hepatocellular Carcinoma Patients with Different Stages of Disease. Cell Death Dis. 2013, 4, e831. [Google Scholar] [CrossRef]
- Hamaoka, M.; Kobayashi, T.; Tanaka, Y.; Mashima, H.; Ohdan, H. Clinical Significance of Glypican-3-Positive Circulating Tumor Cells of Hepatocellular Carcinoma Patients: A Prospective Study. PLoS ONE 2019, 14, e0217586. [Google Scholar]
- Xu, W.; Cao, L.; Chen, L.; Li, J.; Zhang, X.-F.; Qian, H.-H.; Kang, X.-Y.; Zhang, Y.; Liao, J.; Shi, L.-H.; et al. Isolation of Circulating Tumor Cells in Patients with Hepatocellular Carcinoma Using a Novel Cell Separation Strategy. Clin. Cancer Res. 2011, 17, 3783–3793. [Google Scholar]
- Chu, Q.; Mu, W.; Lan, C.; Liu, Y.; Gao, T.; Guan, L.; Fang, Y.; Zhang, Z.; Liu, Y.; Liu, Y.; et al. High-Specific Isolation and Instant Observation of Circulating Tumour Cell from HCC Patients via Glypican-3 Immunomagnetic Fluorescent Nanodevice. Int. J. Nanomed. 2021, 16, 4161–4173. [Google Scholar]
- Zhu, L.; Lin, H.; Wan, S.; Chen, X.; Wu, L.; Zhu, Z.; Song, Y.; Hu, B.; Yang, C. Efficient Isolation and Phenotypic Profiling of Circulating Hepatocellular Carcinoma Cells via a Combinatorial-Antibody-Functionalized Microfluidic Synergetic-Chip. Anal. Chem. 2020, 92, 15229–15235. [Google Scholar] [CrossRef]
- Court, C.M.; Hou, S.; Winograd, P.; Segel, N.H.; Li, Q.W.; Zhu, Y.; Sadeghi, S.; Finn, R.S.; Ganapathy, E.; Song, M.; et al. A Novel Multimarker Assay for the Phenotypic Profiling of Circulating Tumor Cells in Hepatocellular Carcinoma. Liver Transpl. 2018, 24, 946–960. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, L.; Zhang, J.; Zhou, M.; Tang, Y.; He, G.; Lu, Y.; Wang, Z.; Pan, M. Diagnostic Value of Different Phenotype Circulating Tumor Cells in Hepatocellular Carcinoma. J. Gastrointest. Surg. 2019, 23, 2354–2361. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.-C.; Luo, Z.-C.; Gao, Y.-X.; Li, Y.; Peng, Q.; Gao, Y. Twist Expression in Circulating Hepatocellular Carcinoma Cells Predicts Metastasis and Prognoses. Biomed. Res. Int. 2018, 2018, 3789613. [Google Scholar] [CrossRef]
- Bahnassy, A.A.; Zekri, A.-R.N.; El-Bastawisy, A.; Fawzy, A.; Shetta, M.; Hussein, N.; Omran, D.; Ahmed, A.A.S.; El-Labbody, S.S. Circulating Tumor and Cancer Stem Cells in Hepatitis C Virus-Associated Liver Disease. World J. Gastroenterol. 2014, 20, 18240–18248. [Google Scholar] [CrossRef] [PubMed]
- Bhan, I.; Mosesso, K.; Goyal, L.; Philipp, J.; Kalinich, M.; Franses, J.W.; Choz, M.; Oklu, R.; Toner, M.; Maheswaran, S.; et al. Detection and Analysis of Circulating Epithelial Cells in Liquid Biopsies From Patients With Liver Disease. Gastroenterology 2018, 155, 2016–2018.e11. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Xu, Z.; Kong, F.; Huang, X.; Xiao, Y.; Zhou, W.; Ye, S.; Ye, Q. Circulating Tumour Cell Combined with DNA Methylation for Early Detection of Hepatocellular Carcinoma. Front. Genet. 2022, 13, 1065693. [Google Scholar] [CrossRef]
- El-Mezayen, H.A.; El-Kassas, M.; El-Taweel, F.M.; Metwally, F.M.; Ghonaim, N.A.; Zahran, R.F. Diagnostic Performance of Circulating Tumor Cells for Predicting of Hepatocellular Carcinoma in Hepatitis C Virus-High Risk Patients: Role of Liquid Biopsy. Asian Pac. J. Cancer Prev. 2022, 23, 2541–2549. [Google Scholar] [CrossRef]
- Armakolas, A.; Dimopoulou, V.; Nezos, A.; Stamatakis, G.; Samiotaki, M.; Panayotou, G.; Tampaki, M.; Stathaki, M.; Dourakis, S.; Koskinas, J. Cellular, Molecular and Proteomic Characteristics of Early Hepatocellular Carcinoma. Curr. Issues Mol. Biol. 2022, 44, 4714–4734. [Google Scholar] [CrossRef]
- Fan, S.T.; Yang, Z.F.; Ho, D.W.Y.; Ng, M.N.P.; Yu, W.C.; Wong, J. Prediction of Posthepatectomy Recurrence of Hepatocellular Carcinoma by Circulating Cancer Stem Cells: A Prospective Study. Ann. Surg. 2011, 254, 569–576. [Google Scholar] [CrossRef]
- Fang, Z.-T.; Zhang, W.; Wang, G.-Z.; Zhou, B.; Yang, G.-W.; Qu, X.-D.; Liu, R.; Qian, S.; Zhu, L.; Liu, L.-X.; et al. Circulating Tumor Cells in the Central and Peripheral Venous Compartment—Assessing Hematogenous Dissemination after Transarterial Chemoembolization of Hepatocellular Carcinoma. OncoTargets Ther. 2014, 7, 1311–1318. [Google Scholar] [CrossRef]
- Guo, J.; Yao, F.; Lou, Y.; Xu, C.; Xiao, B.; Zhou, W.; Chen, J.; Hu, Y.; Liu, Z. Detecting Carcinoma Cells in Peripheral Blood of Patients with Hepatocellular Carcinoma by Immunomagnetic Beads and Rt-PCR. J. Clin. Gastroenterol. 2007, 41, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Yang, X.-R.; Sun, Y.-F.; Shen, M.-N.; Ma, X.-L.; Wu, J.; Zhang, C.-Y.; Zhou, Y.; Xu, Y.; Hu, B.; et al. Clinical Significance of EpCAM mRNA-Positive Circulating Tumor Cells in Hepatocellular Carcinoma by an Optimized Negative Enrichment and qRT-PCR-Based Platform. Clin. Cancer Res. 2014, 20, 4794–4805. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Sun, Y.-F.; Shen, M.-N.; Ma, X.-L.; Wu, J.; Zhang, C.-Y.; Zhou, Y.; Xu, Y.; Hu, B.; Zhang, M.; et al. Circulating Tumor Cells with Stem-Like Phenotypes for Diagnosis, Prognosis, and Therapeutic Response Evaluation in Hepatocellular Carcinoma. Clin. Cancer Res. 2018, 24, 2203–2213. [Google Scholar] [CrossRef]
- Kelley, R.K.; Magbanua, M.J.M.; Butler, T.M.; Collisson, E.A.; Hwang, J.; Sidiropoulos, N.; Evason, K.; McWhirter, R.M.; Hameed, B.; Wayne, E.M.; et al. Circulating Tumor Cells in Hepatocellular Carcinoma: A Pilot Study of Detection, Enumeration, and next-Generation Sequencing in Cases and Controls. BMC Cancer 2015, 15, 206. [Google Scholar] [CrossRef]
- Liu, S.; Li, N.; Yu, X.; Xiao, X.; Cheng, K.; Hu, J.; Wang, J.; Zhang, D.; Cheng, S.; Liu, S. Expression of Intercellular Adhesion Molecule 1 by Hepatocellular Carcinoma Stem Cells and Circulating Tumor Cells. Gastroenterology 2013, 144, 1031–1041.e10. [Google Scholar] [CrossRef] [PubMed]
- Schulze, K.; Gasch, C.; Staufer, K.; Nashan, B.; Lohse, A.W.; Pantel, K.; Riethdorf, S.; Wege, H. Presence of EpCAM-Positive Circulating Tumor Cells as Biomarker for Systemic Disease Strongly Correlates to Survival in Patients with Hepatocellular Carcinoma. Int. J. Cancer 2013, 133, 2165–2171. [Google Scholar] [CrossRef]
- Sun, Y.-F.; Xu, Y.; Yang, X.-R.; Guo, W.; Zhang, X.; Qiu, S.-J.; Shi, R.-Y.; Hu, B.; Zhou, J.; Fan, J. Circulating Stem Cell-like Epithelial Cell Adhesion Molecule-Positive Tumor Cells Indicate Poor Prognosis of Hepatocellular Carcinoma after Curative Resection. Hepatology 2013, 57, 1458–1468. [Google Scholar] [CrossRef]
- Xue, F.; Shi, S.; Zhang, Z.; Xu, C.; Zheng, J.; Qin, T.; Qian, Z.; Zhao, X.; Tong, Y.; Xia, L.; et al. Application of a Novel Liquid Biopsy in Patients with Hepatocellular Carcinoma Undergoing Liver Transplantation. Oncol. Lett. 2018, 15, 5481–5488. [Google Scholar] [CrossRef]
- Yao, F.; Guo, J.-M.; Xu, C.-F.; Lou, Y.-L.; Xiao, B.-X.; Zhou, W.-H.; Chen, J.; Hu, Y.-R.; Liu, Z.; Hong, G.-F. Detecting AFP mRNA in Peripheral Blood of the Patients with Hepatocellular Carcinoma, Liver Cirrhosis and Hepatitis. Clin. Chim. Acta 2005, 361, 119–127. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, B.; Wu, J.; Zhang, C.; Zhou, Y.; Yang, X.; Zhou, J.; Guo, W.; Fan, J. Association of Preoperative EpCAM Circulating Tumor Cells and Peripheral Treg Cell Levels with Early Recurrence of Hepatocellular Carcinoma Following Radical Hepatic Resection. BMC Cancer 2016, 16, 506. [Google Scholar] [CrossRef]
- Cui, K.; Ou, Y.; Shen, Y.; Li, S.; Sun, Z. Clinical Value of Circulating Tumor Cells for the Diagnosis and Prognosis of Hepatocellular Carcinoma (HCC): A Systematic Review and Meta-Analysis. Medicine 2020, 99, e22242. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.L.; Zhu, P.; Makarova, O.V.; Martin, S.S.; Charpentier, M.; Chumsri, S.; Li, S.; Amstutz, P.; Tang, C.-M. The Systematic Study of Circulating Tumor Cell Isolation Using Lithographic Microfilters. RSC Adv. 2014, 9, 4334–4342. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zhang, C.; Wang, G.; Cheng, B.; Wang, Y.; Chen, F.; Chen, Y.; Feng, M.; Xiong, B. Aptamer-Mediated Transparent-Biocompatible Nanostructured Surfaces for Hepotocellular Circulating Tumor Cells Enrichment. Theranostics 2016, 6, 1877–1886. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Rong, Y.; Yi, K.; Huang, L.; Chen, M.; Wang, F. Circulating Tumor Cells in Hepatocellular Carcinoma: Single-Cell Based Analysis, Preclinical Models, and Clinical Applications. Theranostics 2020, 10, 12060–12071. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-T.; Sun, N.; Kim, M.; Wang, J.J.; Tran, B.V.; Zhang, R.Y.; Qi, D.; Zhang, C.; Chen, P.-J.; Sadeghi, S.; et al. Circulating Tumor Cell-Based Messenger RNA Scoring System for Prognostication of Hepatocellular Carcinoma: Translating Tissue-Based Messenger RNA Profiling Into a Noninvasive Setting. Liver Transpl. 2022, 28, 200–214. [Google Scholar] [CrossRef]
- Chen, J.; Luo, Y.; Xi, X.; Li, H.; Li, S.; Zheng, L.; Yang, D.; Cai, Z. Circulating Tumor Cell Associated White Blood Cell Cluster as a Biomarker for Metastasis and Recurrence in Hepatocellular Carcinoma. Front. Oncol. 2022, 12, 931140. [Google Scholar] [CrossRef]
- Qi, L.-N.; Xiang, B.-D.; Wu, F.-X.; Ye, J.-Z.; Zhong, J.-H.; Wang, Y.-Y.; Chen, Y.-Y.; Chen, Z.-S.; Ma, L.; Chen, J.; et al. Circulating Tumor Cells Undergoing EMT Provide a Metric for Diagnosis and Prognosis of Patients with Hepatocellular Carcinoma. Cancer Res. 2018, 78, 4731–4744. [Google Scholar] [CrossRef]
- Yang, X.; Ni, H.; Lu, Z.; Zhang, J.; Zhang, Q.; Ning, S.; Qi, L.; Xiang, B. Mesenchymal Circulating Tumor Cells and Ki67: Their Mutual Correlation and Prognostic Implications in Hepatocellular Carcinoma. BMC Cancer 2023, 23, 10. [Google Scholar] [CrossRef]
- Befeler, A.S.; Di Bisceglie, A.M. Hepatocellular Carcinoma: Diagnosis and Treatment. Gastroenterology 2002, 122, 1609–1619. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M.; American Association for the Study of Liver Diseases. Management of Hepatocellular Carcinoma: An Update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef]
- Llovet, J.M.; Fuster, J.; Bruix, J.; Barcelona-Clínic Liver Cancer Group. The Barcelona Approach: Diagnosis, Staging, and Treatment of Hepatocellular Carcinoma. Liver Transpl. 2004, 10, S115–S120. [Google Scholar] [CrossRef] [PubMed]
- Laube, R.; Sabih, A.-H.; Strasser, S.I.; Lim, L.; Cigolini, M.; Liu, K. Palliative Care in Hepatocellular Carcinoma. J. Gastroenterol. Hepatol. 2021, 36, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Zhong, Z.; Tan, H.-Y.; Wang, N.; Feng, Y. The Significance of Circulating Tumor Cells in Patients with Hepatocellular Carcinoma: Real-Time Monitoring and Moving Targets for Cancer Therapy. Cancers 2020, 12, 1734. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhang, Z.; Zhou, H.; Leng, C.; Hou, B.; Zhou, C.; Hu, X.; Wang, J.; Chen, X. Preoperative Circulating Tumor Cells to Predict Microvascular Invasion and Dynamical Detection Indicate the Prognosis of Hepatocellular Carcinoma. BMC Cancer 2020, 20, 1047. [Google Scholar] [CrossRef]
- Yu, J.-J.; Xiao, W.; Dong, S.-L.; Liang, H.-F.; Zhang, Z.-W.; Zhang, B.-X.; Huang, Z.-Y.; Chen, Y.-F.; Zhang, W.-G.; Luo, H.-P.; et al. Effect of Surgical Liver Resection on Circulating Tumor Cells in Patients with Hepatocellular Carcinoma. BMC Cancer 2018, 18, 835. [Google Scholar] [CrossRef]
- von Felden, J.; Schulze, K.; Krech, T.; Ewald, F.; Nashan, B.; Pantel, K.; Lohse, A.W.; Riethdorf, S.; Wege, H. Circulating Tumor Cells as Liquid Biomarker for High HCC Recurrence Risk after Curative Liver Resection. Oncotarget 2017, 8, 89978–89987. [Google Scholar] [CrossRef]
- Ha, Y.; Kim, T.H.; Shim, J.E.; Yoon, S.; Jun, M.J.; Cho, Y.-H.; Lee, H.C. Circulating Tumor Cells Are Associated with Poor Outcomes in Early-Stage Hepatocellular Carcinoma: A Prospective Study. Hepatol. Int. 2019, 13, 726–735. [Google Scholar] [CrossRef]
- Xie, Y.L.; Yang, Z.; Feng, X.; Yang, Q.; Ye, L.S.; Li, X.B.; Tang, H.; Zhang, Y.C.; Liu, W.; Zhang, T.; et al. Association of Phenotypic Transformation of Circulating Tumor Cells and Early Recurrence in Patients with Hepatocellular Carcinoma Following Liver Transplantation. Asian J. Surg. 2022, 45, 435–440. [Google Scholar] [CrossRef]
- Sun, Y.-F.; Wang, P.-X.; Cheng, J.-W.; Gong, Z.-J.; Huang, A.; Zhou, K.-Q.; Hu, B.; Gao, P.-T.; Cao, Y.; Qiu, S.-J.; et al. Postoperative Circulating Tumor Cells: An Early Predictor of Extrahepatic Metastases in Patients with Hepatocellular Carcinoma Undergoing Curative Surgical Resection. Cancer Cytopathol. 2020, 128, 733–745. [Google Scholar] [CrossRef]
- Wang, Z.; Luo, L.; Cheng, Y.; He, G.; Peng, B.; Gao, Y.; Jiang, Z.-S.; Pan, M. Correlation Between Postoperative Early Recurrence of Hepatocellular Carcinoma and Mesenchymal Circulating Tumor Cells in Peripheral Blood. J. Gastrointest. Surg. 2018, 22, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Qi, L.-N.; Ma, L.; Chen, Y.-Y.; Chen, Z.-S.; Zhong, J.-H.; Gong, W.-F.; Lu, Y.; Xiang, B.-D.; Li, L.-Q. Outcomes of Anatomical versus Non-Anatomical Resection for Hepatocellular Carcinoma according to Circulating Tumour-Cell Status. Ann. Med. 2020, 52, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Ni, H.-H.; Yang, X.-H.; Yang, C.-L.; Zhang, Q.; Xu, J.-X.; Qi, L.-N.; Xiang, B.-D. Combination of Preoperative Circulating Tumor Cell Count and Neutrophil-Lymphocyte Ratio for Prognostic Prediction in Hepatocellular Carcinoma Patients after Curative Hepatectomy. Biomed. Res. Int. 2022, 2022, 7305953. [Google Scholar] [CrossRef] [PubMed]
- Ogle, L.F.; Orr, J.G.; Willoughby, C.E.; Hutton, C.; McPherson, S.; Plummer, R.; Boddy, A.V.; Curtin, N.J.; Jamieson, D.; Reeves, H.L. Imagestream Detection and Characterisation of Circulating Tumour Cells—A Liquid Biopsy for Hepatocellular Carcinoma? J. Hepatol. 2016, 65, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Li, G.; Han, C.; Han, Q.; Shang, L.; Su, H.; Han, B.; Gong, Y.; Lu, G.; Peng, T. Circulating Tumor Cells as a Potential Biomarker for Postoperative Clinical Outcome in HBV-Related Hepatocellular Carcinoma. Cancer Manag. Res. 2018, 10, 5639–5647. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhu, Y.; Li, Y.; Liu, K.; He, F.; Xu, S.; Li, X.; Li, L.; Hu, J.; Liu, Y. Combined Detection of Circulating Tumor Cells, α-Fetoprotein Heterogene-3 and α-Fetoprotein in the Early Diagnosis of HCC for the Prediction of Efficacy, Prognosis, Recurrence after Microwave Ablation. Infect. Agents Cancer 2021, 16, 28. [Google Scholar] [CrossRef]
- Vogl, T.J.; Riegelbauer, L.J.; Oppermann, E.; Kostantin, M.; Ackermann, H.; Trzmiel, A.; Stein, S.; Eichler, K.; Zharov, V.P.; Roy, D.; et al. Early Dynamic Changes in Circulating Tumor Cells and Prognostic Relevance Following Interventional Radiological Treatments in Patients with Hepatocellular Carcinoma. PLoS ONE 2021, 16, e0246527. [Google Scholar] [CrossRef]
- Wu, X.; Yang, C.; Yu, H.; Cao, F.; Shan, Y.; Zhao, W. The Predictive Values of Serum Dickkopf-1 and Circulating Tumor Cells in Evaluating the Efficacy of Transcatheter Arterial Chemoembolization Treatment on Hepatocellular Carcinoma. Medicine 2019, 98, e16579. [Google Scholar] [CrossRef]
- Shen, J.; Wang, W.-S.; Zhu, X.-L.; Ni, C.-F. High Epithelial Cell Adhesion Molecule-Positive Circulating Tumor Cell Count Predicts Poor Survival of Patients with Unresectable Hepatocellular Carcinoma Treated with Transcatheter Arterial Chemoembolization. J. Vasc. Interv. Radiol. 2018, 29, 1678–1684. [Google Scholar] [CrossRef]
- Chen, M.; Xu, R.; Wu, L.; Chen, X. Relationship between Circulating Tumor Cells Undergoing EMT and Short-Term Efficacy Following Interventional Treatment in Patients with Hepatocellular Carcinoma. J. Interv. Med. 2020, 3, 146–150. [Google Scholar] [CrossRef]
- Verna, E.C.; Patel, Y.A.; Aggarwal, A.; Desai, A.P.; Frenette, C.; Pillai, A.A.; Salgia, R.; Seetharam, A.; Sharma, P.; Sherman, C.; et al. Liver Transplantation for Hepatocellular Carcinoma: Management after the Transplant. Am. J. Transpl. 2020, 20, 333–347. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Lin, X.; Chen, C.; Chen, Y.; Zhao, Q.; Wu, L.; Wang, D.; Ma, Y.; Ju, W.; Chen, M.; et al. Analysis of Preoperative Circulating Tumor Cells for Recurrence in Patients with Hepatocellular Carcinoma after Liver Transplantation. Ann. Transl. Med. 2020, 8, 1067. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.-X.; Xu, Y.; Sun, Y.-F.; Cheng, J.-W.; Zhou, K.-Q.; Wu, S.-Y.; Hu, B.; Zhang, Z.-F.; Guo, W.; Cao, Y.; et al. Detection of Circulating Tumour Cells Enables Early Recurrence Prediction in Hepatocellular Carcinoma Patients Undergoing Liver Transplantation. Liver Int. 2021, 41, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Brandi, N.; Renzulli, M. The Synergistic Effect of Interventional Locoregional Treatments and Immunotherapy for the Treatment of Hepatocellular Carcinoma. Int. J. Mol. Sci. 2023, 24, 8598. [Google Scholar] [CrossRef]
- Nel, I.; Baba, H.A.; Ertle, J.; Weber, F.; Sitek, B.; Eisenacher, M.; Meyer, H.E.; Schlaak, J.F.; Hoffmann, A.-C. Individual Profiling of Circulating Tumor Cell Composition and Therapeutic Outcome in Patients with Hepatocellular Carcinoma. Transl. Oncol. 2013, 6, 420–428. [Google Scholar] [CrossRef]
- Li, J.; Shi, L.; Zhang, X.; Sun, B.; Yang, Y.; Ge, N.; Liu, H.; Yang, X.; Chen, L.; Qian, H.; et al. pERK/pAkt Phenotyping in Circulating Tumor Cells as a Biomarker for Sorafenib Efficacy in Patients with Advanced Hepatocellular Carcinoma. Oncotarget 2016, 7, 2646–2659. [Google Scholar] [CrossRef]
- Winograd, P.; Hou, S.; Court, C.M.; Lee, Y.-T.; Chen, P.-J.; Zhu, Y.; Sadeghi, S.; Finn, R.S.; Teng, P.-C.; Wang, J.J.; et al. Hepatocellular Carcinoma-Circulating Tumor Cells Expressing PD-L1 Are Prognostic and Potentially Associated With Response to Checkpoint Inhibitors. Hepatol. Commun. 2020, 4, 1527–1540. [Google Scholar] [CrossRef]
- Su, K.; Guo, L.; He, K.; Rao, M.; Zhang, J.; Yang, X.; Huang, W.; Gu, T.; Xu, K.; Liu, Y.; et al. PD-L1 Expression on Circulating Tumor Cells Can Be a Predictive Biomarker to PD-1 Inhibitors Combined with Radiotherapy and Antiangiogenic Therapy in Advanced Hepatocellular Carcinoma. Front. Oncol. 2022, 12, 873830. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, X.; Zhang, J.; Sun, B.; Zheng, L.; Li, J.; Liu, S.; Sui, G.; Yin, Z. Microfluidic Chip for Isolation of Viable Circulating Tumor Cells of Hepatocellular Carcinoma for Their Culture and Drug Sensitivity Assay. Cancer Biol. Ther. 2016, 17, 1177–1187. [Google Scholar] [CrossRef]
- Hsieh, C.-H.; Yeh, C.-T.; Huang, Y.-H.; Lai, M.-W. Circulating Tumor Cells Derived from Advanced Hepatocellular Carcinoma Rapidly Develop Resistance to Cytotoxic Chemotherapy. Anticancer Res. 2022, 42, 2479–2486. [Google Scholar] [CrossRef]
- Circulating Tumor Cell Capture for Early Diagnosis and Postoperative Tumor Recurrence Monitoring of Liver Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT04688606 (accessed on 29 May 2023).
- Circulating Tumor Cell Detection in Hepatocellular Carcinoma. Available online: https://clinicaltrials.gov/ct2/show/NCT05297955 (accessed on 29 May 2023).
- Frequency of Circulating Tumor Cells (CTCs) and Amount of Cell-Free DNA (cfDNA) in Cirrhotic Patients with Hepatocellular Carcinoma (HCC). Available online: https://clinicaltrials.gov/ct2/show/NCT03162198 (accessed on 29 May 2023).
- A Trial of Adjuvant Therapy after Hepatocarcinoma Resection Based on Folate Receptor-Positive Circulating Tumor Cells. Available online: https://clinicaltrials.gov/ct2/show/NCT04521491 (accessed on 29 May 2023).
- Circulating Tumor Cells for Hepatocellular Carcinoma—Full Text View—ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT01930383 (accessed on 29 May 2023).
- The Role of Circulating Tumor Cells as Markers of Advanced Disease and Prognosis in HCC. Available online: https://clinicaltrials.gov/ct2/show/NCT04800497 (accessed on 29 May 2023).
- Prognostic Value of Liver Cancer CTCs Isolated by a Novel Microfluidic Platform. Available online: https://clinicaltrials.gov/ct2/show/NCT05242237 (accessed on 29 May 2023).
- Circulating Tumor Cells and Tumor DNA in HCC and NET. Available online: https://clinicaltrials.gov/ct2/show/NCT02973204 (accessed on 29 May 2023).
- Relationship between Circulating Tumor Stem Cells and the Clinical Pathology. Available online: https://clinicaltrials.gov/ct2/show/NCT02727673 (accessed on 29 May 2023).
- Hong, B.; Zu, Y. Detecting Circulating Tumor Cells: Current Challenges and New Trends. Theranostics 2013, 3, 377–394. [Google Scholar] [CrossRef] [PubMed]
- Lalmahomed, Z.S.; Kraan, J.; Gratama, J.W.; Mostert, B.; Sleijfer, S.; Verhoef, C. Circulating Tumor Cells and Sample Size: The More, the Better. J. Clin. Oncol. 2010, 28, e288–e289. [Google Scholar] [CrossRef] [PubMed]
- Attard, G.; de Bono, J.S. Utilizing Circulating Tumor Cells: Challenges and Pitfalls. Curr. Opin. Genet. Dev. 2011, 21, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Mani, S.A.; Guo, W.; Liao, M.-J.; Eaton, E.N.; Ayyanan, A.; Zhou, A.Y.; Brooks, M.; Reinhard, F.; Zhang, C.C.; Shipitsin, M.; et al. The Epithelial-Mesenchymal Transition Generates Cells with Properties of Stem Cells. Cell 2008, 133, 704–715. [Google Scholar] [CrossRef]
- Parkinson, D.R.; Dracopoli, N.; Petty, B.G.; Compton, C.; Cristofanilli, M.; Deisseroth, A.; Hayes, D.F.; Kapke, G.; Kumar, P.; Lee, J.S.; et al. Considerations in the Development of Circulating Tumor Cell Technology for Clinical Use. J. Transl. Med. 2012, 10, 138. [Google Scholar] [CrossRef]
- Neumann, M.H.D.; Bender, S.; Krahn, T.; Schlange, T. CtDNA and CTCs in Liquid Biopsy—Current Status and Where We Need to Progress. Comput. Struct. Biotechnol. J. 2018, 16, 190–195. [Google Scholar] [CrossRef]
- Pelizzaro, F.; Cardin, R.; Penzo, B.; Pinto, E.; Vitale, A.; Cillo, U.; Russo, F.P.; Farinati, F. Liquid Biopsy in Hepatocellular Carcinoma: Where Are We Now? Cancers 2021, 13, 2274. [Google Scholar] [CrossRef] [PubMed]
- Labgaa, I.; Villanueva, A.; Dormond, O.; Demartines, N.; Melloul, E. The Role of Liquid Biopsy in Hepatocellular Carcinoma Prognostication. Cancers 2021, 13, 659. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Immunoaffinity | Biophysical | Enrichment-Free Techniques |
|---|---|---|
| Immunomagnetic based techniques | Microfiltration based techniques | ImageStream |
| CellSearch | Isolation by Size of Tumor cells (ISET) | Photoacoustic flow cytometry (PAFC) |
| Magnetic-activated cell separation (MACS) | ScreenCell | ELISPOT assay |
| Surface-enhanced Raman scattering (SERS) | CellSieve | |
| Subtraction enrichment and immunostaining-fluorescence in situ hybridization (SE-iFISH) | Flexible micro spring array (FMSA) | |
| CanPatrol (Microfiltration followed RNA in situ hybridization) | ||
| Microfluid based techniques | Density gradient centrifugation-based techniques | |
| CTC-Chip | Ficoll-Paque | |
| NanoVelcro | OncoQuick | |
| RosetteSep CTC Enrichment Cocktail | ||
| Immunomagnetic as well as Microfluid based techniques | Dielectrophoresis based techniques | |
| CTC-iChip | DEPArray |
| Scheme | Region | Year of Study | Type of Study | Patients with HCC | Controls | Sensitivity | Technique of Isolation |
|---|---|---|---|---|---|---|---|
| Armakolas et al. [81] | Greece | 2022 | Prospective study | 89 | 28 cirrhotic patients | Sensitivity: 46% | qRT-PCR and IF (EPCAM, vimentin, AFP and sMVP) |
| Bahsanny et al. [77] | Egypt | 2014 | Prospective study | 120 | 30 with chronic hepatitis C, 33 healthy controls | CK19(+) CTCs: 87.1%/82.5% | Flow cytometry (CK19, CD133 and CD90) and RT-PCR |
| CD90(+) CTCs: 82.5%/89.6% | |||||||
| CD133(+) CTCs: 40.0%/6.3% | |||||||
| Bahn et al. [78] | USA | 2018 | Prospective study | 54 | 39 with chronic liver disease, 10 healthy controls | 81% (CTC ≥ 5/10 mL) | CTC-iChip followed by IF staining for glypican-3 |
| Cheng et al. [75] | China | 2015–2017 | Prospective study | 113 | 57 with chronic liver disease | Total CTCs ≥ 3: sensitivity 62%, specificity 90%, Epithelial CTCs ≥ 1: sensitivity: 45 %, specificity: 79% | CanPatrol |
| Mixed CTCs ≥ 2: sensitivity: 53.1%, specificity: 82.5%, Mesenchymal CTCs ≥ 1: sensitivity: 49.6%, specificity: 87.7% | |||||||
| Chu et al. [72] | China | 2021 | Prospective study | 20 | 3 healthy volunteers | Cell recovery increased from 42% to 80.3% compared with MACS® Beads | Glypican-3 (GPC3)-based immunomagnetic fluorescent system |
| Fan et al. [82] | China | 2005–2009 | Prospective study | 82 | - | Sensitivity: 68.3% | Multicolor flow cytometry—CSCs (CD45 − CD90 + CD44+) |
| Fang et al. [83] | China | 2012–2013 | Prospective study | 42 | - | CTCs (≥1/5 mL): 74%/100% | CellSearch |
| Guo et al. [84] | China | 2006 | Prospective study | 44 | 7 healthy controls | AFP mRNA (sensitivity, specificity, diagnostic accuracy): 50%, 76.5%, 86.7% | RT-PCR followed by CD45 and Ber-EP4 immunomagnetic beads |
| Guo et al. [85] | China | 2012–2013 | Prospective study | 299 | 71 healthy donors, 24 with benign tumor, and 25 with chronic hepatitis B and/or liver cirrhosis | EpCAM-mRNA (+) CTCs (sensitivity, specificity): 42.6%/96.7% | CellSearch and qRT-PCR |
| Guo et al. [86] | China | 2012–2015 | Multicenter Clinical Trial | 395 | 201 with chronic hepatitis B and/or liver cirrhosis, 100 with benign liver lesions, 210 healthy controls | Sensitivity/specificity: 72.5%/95% | Multimarker qRT-RNA detection platform |
| Kalinch et al. [52] | USA | 2017 | Prospective study | 63 | 26 with chronic liver disease, 34 healthy donors | Out of 15 patients who were tested for both AFP and CTC scores, 33% were detected by both assays, 27% were detected by CTC score alone, and 7% were detected by AFP alone. Either the AFP or CTC score was positive in 67% | CTC-iChip RNA-based digital qRT-PCR |
| Kelley et al. [87] | USA | 2011–2012 | Prospective study | 20 | 10 with non-malignant liver disease | 1 CTC/7.5 mL | CellSearch |
| AFP ≥ 400 ng/mL: sensitivity 70%, AFP < 400 ng/mL: | |||||||
| Sensitivity: 10% | |||||||
| Li et al. [56] | China | 2013 | Prospective study | 27 | 34 with benign liver disease/hepatitis/cirrhosis and 15 healthy volunteers. | Sensitivity: 89% | anti-ASGPR, CPS1 and P-CK antibodies |
| Liang et al. [79] | China | 2020–2022 | Prospective study | 17 | 11 cases of HBV-related decompensated cirrhosis | 70.6%/90.9% | CTCBIOPSY device |
| Liu et al. [88] | China | 2013 | Prospective study | 60 | -- | High CD45-ICAM-1+ cell frequency (>0.157%)–50% | CD45-ICAM-1+ |
| Schulze et al. [89] | Germany | 2013 | Prospective study | 59 | 19 with cirrhosis or benign hepatic tumor | Sensitivity: 30.5% | CellSearch |
| Sun et al. [90] | China | 2010–2011 | Prospective study | 123 | 20 healthy volunteers | CTC ≥ 2: 71%/80% | CellSearch |
| Xu et al. [71] | China | 2009 | Prospective study | 85 | 37 with benign liver diseases | CTC positivity: 81% | ASGPR (+) |
| Xue et al. [91] | China | 2014–2015 | Prospective study | 30 | 10 healthy volunteers | Cellsearch-CTCs: 27%/100%; iFISH-CTCs: 70%/100% | CellSearch and iFISH (CK+/DAPI+/CD45−) |
| Yao et al. [92] | China | 2003–2004 | Prospective study | 49 | 18 healthy donors, 16 with cirrhosis, 20 with hepatitis | Sensitivity: 72.1% | CD45 and Ber-EP4 immunomagnetic beads followed by AFP mRNA-nested RT-PCR |
| Yin et al. [76] | China | 2015–2017 | Prospective study | 80 | 10 healthy volunteers | Sensitivity: 77.5% | CanPatrol |
| Zhou et al. [93] | China | 2012 | Prospective study | 49 | - | CTC ≥ 2: 34.6%/100% | EpCAM mRNA+ CTC detection and qRT-PCR |
| Zhu et al. [73] | China | 2019 | Prospective study | 45 | Six healthy donors and six with benign tumors | ≥1.5 CTCs/2 mL: 97.8%/100% | Microfluidic synergetic-chip (anti-ASGPR and anti-EpCAM) |
| Study | Region | Year of Study | Type of Study | HCC Patient Number | Technique of Isolation | Key Findings |
|---|---|---|---|---|---|---|
| Chen et al. [99] | China | 2014–2020 | Retrospective analysis | 136 | CanPatrol, filtration and multiple mRNA ISH | CTC-WBC cluster ≥ 1/5 mL was associated with distant metastasis, tumor relapse and a shorter RFS |
| Kelly et al. [87] | USA | 2011–2012 | Prospective study | 20 | CellSearch | CTCs ≥ 1 per 7.5 mL was associated with AFP ≥ 400 ng/mL and vascular invasion |
| Liu et al. [88] | China | 2013 | Prospective study | 60 | CD45-ICAM-1+ | High frequency of CD45-ICAM-1+ cells (≥0.157%) was associated with a shorter DFS and OS. It is an independent risk factor for poor outcomes, including portal vein tumor thrombus and the presence of ascites |
| Sun et al. [90] | China | 2010–2011 | Prospective study | 123 | CellSearch | CTCs ≥ 2 per 7.5 mL was found to be significantly associated with aggressive HCC phenotypes |
| Schulze et al. [89] | Germany | 2013 | Prospective study | 59 | CellSearch | The presence of CTCs was associated with shorter OS advanced BCLC stage (stage C), microscopic vascular invasion, and elevated AFP ≥ 400 ng/mL |
| Vona et al. [60] | France | 2004 | Prospective study | 44 | ISET method | The presence of CTCs was associated with diffuse tumors and portal tumor thrombosis. |
| Yang et al. [101] | China | 2014–2017 | Prospective study | 105 | CanPatrol | M-CTC positivity was associated with AFP ≥ 400 ng/mL, tumor size ≥ 5 cm, the presence of multiple tumors, poorly differentiated tumors, incomplete tumor capsule, BCLC stage B or C, microvascular invasion and portal vein tumor thrombosis |
| Study | Region | Year of Study | Type of Study | HCC Patient Number | Technique of Isolation | Key Findings |
|---|---|---|---|---|---|---|
| Court et al. [74] | USA | 2015–2016 | Prospective study | 61 | NanoVelcro assay (ASGPR, Glypican-3, EpCAM) | Vimentin (+) CTCs associated with OS, PFS and portended faster time to recurrence |
| Fan et al. [82] | China | 2005–2009 | Prospective study | 82 | Multicolor flow cytometry—CSCs (CD45 − CD90 + CD44+) | Circulating CSCs > 0.01% predicted: intrahepatic recurrence, extrahepatic recurrence, lower 2-year RFS and OS |
| Guo et al. [86] | China | 2012–2015 | Multicenter clinical trial | 395 | Multimarker qRT-RNA detection platform | Persistently positive CTCs after resection were associated with a higher recurrence rate. CTC load/5 mL > 0.80 was associated with a significantly shorter TTR |
| Ha et al. [111] | South Korea | 2014–2016 | Prospective study | 105 | Tapered slit flter (TSF) platform | Increased CTCs after surgery were associated with a higher level of recurrence. Positive ΔCTC was associated with shorter OS and higher recurrence among patients with low AFP levels and cirrhosis |
| Hamaoka et al. [70] | Japan | 2015–2016 | Prospective study | 85 | Glypican-3(+) | CTCs ≥ 5 was an independent predictor of mPVI and poor prognosis. |
| Ni et al. [116] | China | 2014–2017 | Retrospective study | 97 | CanPatrol, filtration | CTC < 20 and NLR < 2.15 were associated with longer OS. Patients were classified into CTC-NLR (0), CTC-NLR (1), and into CTC-NLR (2). CTC-NLR (0) was associated with the best OS, whereas CTC-NLR (2) had the worst OS |
| Ogle et al. [117] | UK | 2012–2015 | Prospective study | 69 | IF (EpCAM, CK, AFP and GPC3) and size | CTC > 1 per 4 mL blood post treatment was significantly associated with a poorer survival: 7.5 months for >1 CTC versus > 34 months for patients with <1 CTC |
| Ou et al. [49] | China | 2013–2016 | Prospective study | 165 | CanPatrol | Mesenchymal CTCs were associated with high levels of AFP, multiple tumors, advanced TNM and BCLC stage, presence of embolus or micro embolus and the shortest relapse-free survival |
| Qi et al. [115] | China | 2014–2017 | Retrospective study | 136 | CanPatrol | TFS was higher with low CTCs count and M- and E/M-negative phenotypes. High pre-resection CTC count and M- and E/M-positivity associated with extrahepatic and multi-intrahepatic recurrence. |
| Qi et al. [100] | China | 2014–2016 | Prospective trial | 112 | CanPatrol | Post operative CTC count ≥ 16 and M-CTC ≥ 2% were associated with early recurrence, multi-intrahepatic recurrence, and lung metastasis. Postoperative CTC monitoring showed an increase in CTC count and M-CTC % before clinically detectable recurrence nodules appeared. |
| Sun et al. [90] | China | 2010–2011 | Prospective study | 123 | CellSearch | Preoperative CTC (7.5 mL) of ≥2 was an independent prognostic factor for tumor recurrence |
| Sun et al. [42] | China | 2013–2015 | Prospective study | 73 | CellSearch | The presence of CTCs in the hepatic vein, along with the presence of CTM, was an independent prognostic factor for the development of lung metastasis. |
| Von Felden et al. [110] | Germany | 2011–2015 | Prospective study | 61 | CellSearch | CTC-positivity was associated with a higher risk of recurrence and a shorter RFS |
| Wang et al. [114] | China | 2014–2016 | Prospective study | 62 | CanPatrol | Mesenchymal CTC positivity was associated with ER and shortened postoperative disease-free survival |
| Xie et al. [112] | China | 2016–2019 | Retrospective study | 66 | CanPatrol | Recurrence rates of postoperative interstitial CTC-positive and CTC-negative groups: 1-year recurrence: 21.7% vs. 10.8% 2-year recurrence: 37.5% vs. 10.8% 3-year recurrence: 55.5% vs. 10.8%, 1 -, 2- and 3-year recurrence rates of interstitial CTC in the increasing group were 25.2%, 36.9% and 66.9% 1-year recurrence: 21.7% vs. 10.8% |
| Ye et al. [118] | China | 2014–2017 | Prospective study | 42 | CanPatrol | Postoperative CTC counts (≥2 and ≥5) and pre/postoperative change in CTC counts were significantly associated with PFS |
| Yu et al. [109] | China | 2013–2015 | Prospective study | 139 | CellSearch | Increase in postoperative CTC counts (from preoperative CTC < 2 to postoperative CTC ≥ 2) is associated with shorter DFS and OS |
| Zhou et al. [93] | China | 2012 | Prospective study | 49 | EpCAM mRNA (+) | Post-operative CTC ≥ 2.22 was an independent prognostic biomarker for early recurrence |
| Study | Region | Year of Study | Type of Study | HCC Patient Number | Technique of Isolation | Key Findings |
|---|---|---|---|---|---|---|
| Trans arterial Chemoembolization (TACE) | ||||||
| Chen et al. [123] | China | 2017–2018 | Retrospective analysis | 107; treated with TACE and MWA | Cyttel method | Pretreatment CTC count and EMT phenotypes were not predictive of short-term efficacy. Comprehensive therapy reduced the total CTC and mesenchymal CTC count |
| Guo et al. [85] | China | 2012–2013 | Prospective study | 299 HCC; 157-curative resection, 76-TACE, and 66-radio therapy | EpCAM (mRNA+) | Pretreatment CTC level showed prognostic significance in patients treated with resection, TACE, and radiotherapy. Preoperative detectable EpCAM mRNA+ CTCs had significantly shorter TTR and higher recurrence rates. A decrease in CTC levels after treatment reflected tumor response. Persistent positive CTCs (preoperative and postoperative) was associated with higher recurrence rates. |
| Shen et al. [122] | China | 2014–2015 | Prospective study | 89 | CellSearch | Pretreatment CTC counts were independent predictors of OS and PFS. |
| Wu et al. [121] | China | 2012–2014 | Retrospective analysis | 155 | Immunomagnetic beads and FISH (chromosome 8 amplification) | Positive preoperative CTCs were associated with lower OS, DFS, and 5-year survival rates |
| Microwave ablation (MWA) | ||||||
| Zhou et al. [119] | China | 2014–2017 | Prospective study | 105 | CellSearch | Combined detection of serum AFP, AFP-L3, CTCs improves the prediction of recurrence after MWA |
| Study | Region | Year of Study | Type of Study | HCC Patient Number | Technique of Isolation | Key Findings |
|---|---|---|---|---|---|---|
| Chen et al. [125] | China | 2016–2019 | Retrospective study | 50 | Negative enrichment (anti-CD45) and iFISH | CTCs positivity correlated with tumor size, AFP level, tumor grade and recurrence. CTC-negative vs. CTC-positive: 1-year DFS: 91.6% vs. 61.5% (p = 0.02), 1-year OS: 88.5% s. 91.7% (p = 0.75) |
| Court et al. [74] | USA | 2015–2016 | Prospective study | 61 | NanoVelcro assay (ASGPR, Glypican-3, EpCAM) | Vimentin (+) CTCs accurately discriminated early-stage, LT eligible patients from locally advanced/metastatic, LT ineligible patients |
| Wang et al. [126] | China | 2017–2019 | Prospective study | 193 | ChimeraX-i120, anti-EpCAM, anti-pan-CK | Post-operative CTC count ≥ 1 per 5 mL predicts recurrence after LT |
| Xue et al. [91] | China | 2014–2015 | Prospective study | 30 | iFISH and CellSearch | iFISH-CTCs < 5/7.5 mL associated with increased RFS |
| Study | Region | Year of Study | Type of Study | HCC Patient Number | Technique of Isolation | Key Findings |
|---|---|---|---|---|---|---|
| Li et al. [129] | China | 2017 | Prospective study | 63 | CD45- and pAkt1/2/3 or pERK1/2+ | ≥40% pERK+/pAkt− CTCs showed longer PFS and response to Sorafenib treatment |
| Su et al. [131] | China | 2022 | Prospective study | 47 | CytoSorter | Patients with <2 PD-L1+ CTCs exhibited a higher ORR and longer OS compared to those with ≥2 PD-L1+ CTCs. PD-L1-positive CTCs were an independent predictive biomarker for OS in patients receiving triple therapy. |
| Winograd et al. [130] | USA | 2014–2017 | Prospective study | 102 | NanoVelcro Chip | PD-L1+ CTCs are primarily detected in advanced-stage HCC and independently predict OS when controlling for the MELD score, AFP levels, and tumor stage. |
| Study | Region | Year of Study | Type of Study | HCC Patient Number | Technique of Isolation | Key Findings |
|---|---|---|---|---|---|---|
| NCT04688606 [134] | China | 2020–2021 | Retrospective study | 300 | CTCBIOPSY to detect CTC number (including interventional therapy, tumor resection, or LT) 1–3 days before, 1 month after surgery, and 6 months after surgery | To evaluate the clinical significance of CTCs in HCC screening and postoperative recurrence monitoring |
| NCT05297955 [135] | China | 2013–2022 | Retrospective study | 458 | CellSearch to detect CTC number in patients undergoing liver cancer surgery during perioperative period | CTC levels before and after surgery were significantly correlated with OS and DFS. Preoperative CTC correlated with disease-related clinical parameters, while postoperative CTC was an independent prognostic indicator |
| NCT03162198 [136] | India | 2017–2018 | Cross sectional study | 53 | Unclear | To detect CTC number in cirrhotic HCC patients and to correlate CTC number with tumor size, number, and BCLC stage |
| NCT04521491 [137] | China | 2020–2023? | Randomized Controlled Study | 184 | Unclear | To analyze the effect of postoperative FOLFOX4 therapy after HCC resection based on folate receptor-positive CTCs. Patients were randomized to postoperative FOLFOX4 group and no FOLFOX4 group. The time to recurrence, the OS as well as the incidence of complications after therapy was observed |
| NCT01930383 [138] | Taiwan | 2013–2015 | Prospective study | 150 | Microfluidic disk platform | To explore the correlation between CTC number and clinical characteristics; to compare the patterns of molecular aberrations between CTC and HCC tumor tissue; and to measure the changes in CTCs numbers and molecular aberrations before and after targeted therapy |
| NCT04800497 [139] | Italy | 2019–2024 | Prospective study | 200 | FACSymphony™ and subsequently by EpCAM, N-cadherin and CD90 | To evaluate the association between CTCs and DFS/OS |
| NCT05242237 [140] | China | 2021–2024 | Prospective study | 300 | Microfluidic Platform: Cellomics CTC-100 cell sorter | To determine the relationship between the CTC number and prognosis/treatment response, detect mutation, copy number variation and mutation load in CTC cells using single-cell whole genome sequencing technology, and use bioinformatics analysis of CTC heterogeneity and its relationship with clinical outcome |
| NCT02973204 [141] | Denmark | 2016–2020 | Prospective study | 30 | Flow cytometry | Treatment response; To correlate between the CTC number and survival in HCC patients treated with Sorafenib |
| NCT02727673 [142] | China | 2012–2014 | Prospective Randomized Trial | 500 | Unclear | To investigate the relationship between CSCs and postoperative recurrence/metastasis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaik, M.R.; Sagar, P.R.; Shaik, N.A.; Randhawa, N. Liquid Biopsy in Hepatocellular Carcinoma: The Significance of Circulating Tumor Cells in Diagnosis, Prognosis, and Treatment Monitoring. Int. J. Mol. Sci. 2023, 24, 10644. https://doi.org/10.3390/ijms241310644
Shaik MR, Sagar PR, Shaik NA, Randhawa N. Liquid Biopsy in Hepatocellular Carcinoma: The Significance of Circulating Tumor Cells in Diagnosis, Prognosis, and Treatment Monitoring. International Journal of Molecular Sciences. 2023; 24(13):10644. https://doi.org/10.3390/ijms241310644
Chicago/Turabian StyleShaik, Mohammed Rifat, Prem Raj Sagar, Nishat Anjum Shaik, and Navkiran Randhawa. 2023. "Liquid Biopsy in Hepatocellular Carcinoma: The Significance of Circulating Tumor Cells in Diagnosis, Prognosis, and Treatment Monitoring" International Journal of Molecular Sciences 24, no. 13: 10644. https://doi.org/10.3390/ijms241310644