
Interventional Oncology and Immuno-Oncology: Current Challenges and Future Trends
 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Percutaneous Treatment and Immuno-Oncology
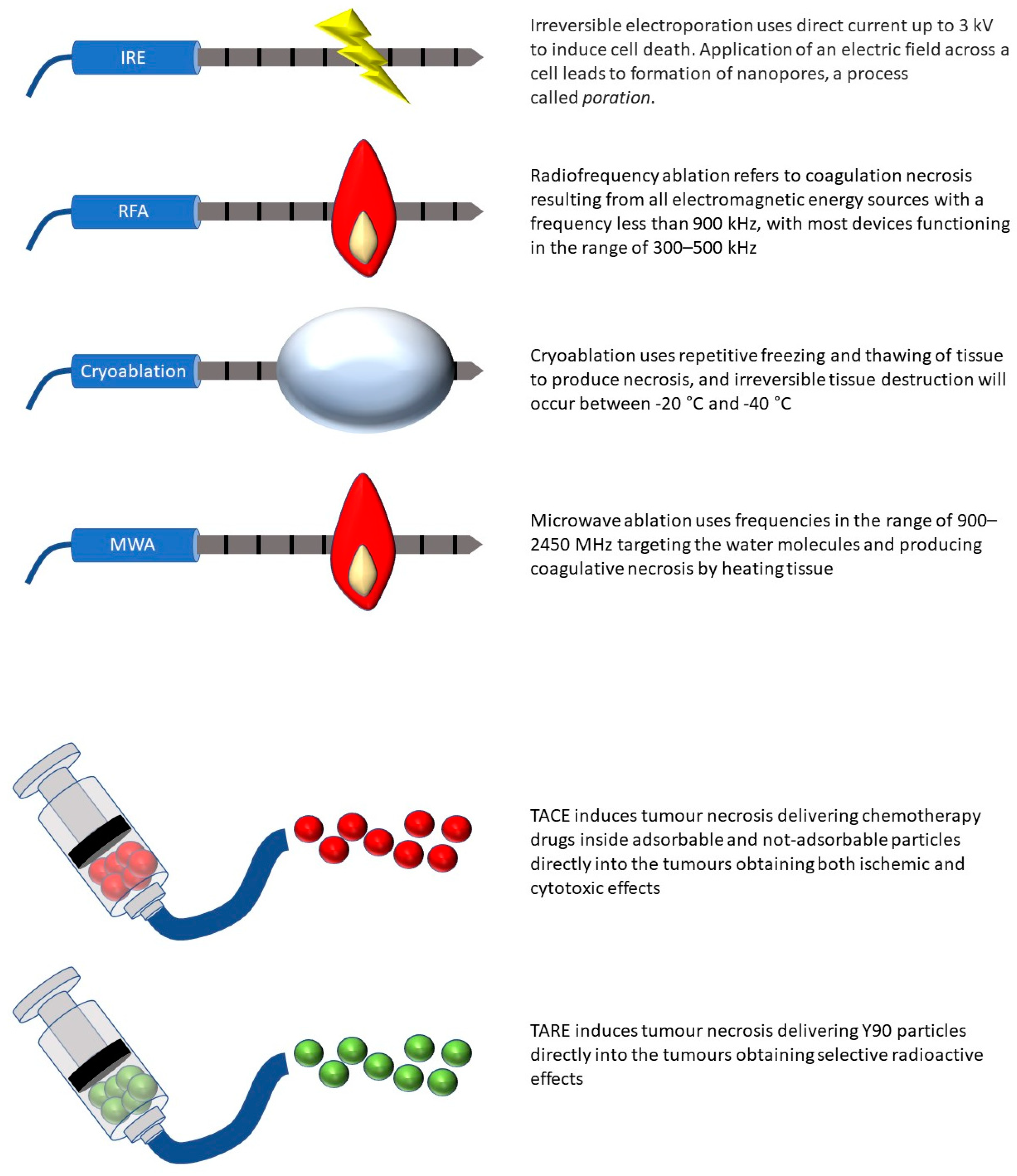
2.1. Radiofrequency Ablation (RFA)
2.2. Cryoablation
2.3. Irreversible Electroporation (IRE)
2.4. Microwave Ablation (MWA)
2.5. High-Intensity Focal Ultrasound (HIFU) and Laser-Induced Thermotherapy (LiTT)
3. Endovascular Treatments and Immuno-Oncology
3.1. Transarterial Chemoembolization (TACE)
3.2. Transarterial Radioembolization (TARE)
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Erinjeri, J.P.; Fine, G.C.; Adema, G.J.; Ahmed, M.; Chapiro, J.; Brok, M.D.; Duran, R.; Hunt, S.J.; Johnson, D.T.; Ricke, J.; et al. Immunotherapy and the Interventional Oncologist: Challenges and Opportunities—A Society of Interventional Oncology White Paper. Radiology 2019, 292, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Helmberger, T. The evolution of interventional oncology in the 21st century. Br. J. Radiol. 2020, 93, 20200112. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation Barcelona Clinic Liver Cancer (BCLC) staging system: The 2022 update. J. Hepatol. 2021, 76, 681–693. [Google Scholar] [CrossRef]
- Campbell, S.C.; Clark, P.E.; Chang, S.S.; Karam, J.A.; Souter, L.; Uzzo, R.G. Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-Up: AUA Guideline: Part I. J. Urol. 2021, 206, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.C.; Uzzo, R.G.; Karam, J.A.; Chang, S.S.; Clark, P.E.; Souter, L. Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-up: AUA Guideline: Part II. J. Urol. 2021, 206, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Lucatelli, P.; Iezzi, R.; De Rubeis, G.; Goldberg, S.N.; Bilbao, J.I.; Sami, A.; Akhan, O.; Giuliante, F.; Pompili, M.; Tagliaferri, L.; et al. Immuno-oncology and interventional oncology: A winning combination. The latest scientific evidence. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 5343–5350. [Google Scholar]
- Ridouani, F.; Srimathveeravalli, G. Percutaneous image-guided ablation: From techniques to treatments. Presse Med. 2019, 48, e219–e231. [Google Scholar] [CrossRef]
- Liao, J.; Xiao, J.; Zhou, Y.; Liu, Z.; Wang, C. Effect of transcatheter arterial chemoembolization on cellular immune function and regulatory T cells in patients with hepatocellular carcinoma. Mol. Med. Rep. 2015, 12, 6065–6071. [Google Scholar] [CrossRef]
- Leuchte, K.; Staib, E.; Thelen, M.; Gödel, P.; Lechner, A.; Zentis, P.; Garcia-Marquez, M.; Waldschmidt, D.; Datta, R.R.; Wahba, R.; et al. Microwave ablation enhances tumor-specific immune response in patients with hepatocellular carcinoma. Cancer Immunol. Immunother. 2020, 70, 893–907. [Google Scholar] [CrossRef]
- Zeng, P.; Shen, D.; Zeng, C.-H.; Chang, X.-F.; Teng, G.-J. Emerging Opportunities for Combining Locoregional Therapy with Immune Checkpoint Inhibitors in Hepatocellular Carcinoma. Curr. Oncol. Rep. 2020, 22, 76. [Google Scholar] [CrossRef]
- Hickey, R.M.; Kulik, L.M.; Nimeiri, H.; Kalyan, A.; Kircher, S.; Desai, K.; Riaz, A.; Lewandowski, R.J.; Salem, R. Immuno-oncology and Its Opportunities for Interventional Radiologists: Immune Checkpoint Inhibition and Potential Synergies with Interventional Oncology Procedures. J. Vasc. Interv. Radiol. 2017, 28, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Krokidis, M.E.; Orsi, F.; Katsanos, K.; Helmberger, T.; Adam, A. CIRSE Guidelines on Percutaneous Ablation of Small Renal Cell Carcinoma. Cardiovasc. Interv. Radiol. 2016, 40, 177–191. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; de Lope, C.R.; Bruix, J. Current Strategy for Staging and Treatment: The BCLC Update and Future Prospects. Semin. Liver Dis. 2010, 30, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Pereira, P.L.; Salvatore, M.; Cardiovascular and Interventional Radiological Society of Europe (CIRSE). Standards of Practice: Guidelines for Thermal Ablation of Primary and Secondary Lung Tumors. Cardiovasc. Interv. Radiol. 2012, 35, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Gangi, A.; Tsoumakidou, G.; Buy, X.; Quoix, E. Quality Improvement Guidelines for Bone Tumour Management. Cardiovasc. Interv. Radiol. 2010, 33, 706–713. [Google Scholar] [CrossRef]
- Rangamuwa, K.; Leong, T.; Weeden, C.; Asselin-Labat, M.-L.; Bozinovski, S.; Christie, M.; John, T.; Antippa, P.; Irving, L.; Steinfort, D. Thermal ablation in non-small cell lung cancer: A review of treatment modalities and the evidence for combination with immune checkpoint inhibitors. Transl. Lung Cancer Res. 2021, 10, 2842–2857. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Matsutani, N.; Nakayama, T.; Dejima, H.; Uehara, H.; Kawamura, M. Immunological effect of local ablation combined with immunotherapy on solid malignancies. Chin. J. Cancer 2017, 36, 49. [Google Scholar] [CrossRef]
- Vanlangenakker, N.; Berghe, T.V.; Krysko, D.; Festjens, N.; Vandenabeele, P. Molecular Mechanisms and Pathophysiology of Necrotic Cell Death. Curr. Mol. Med. 2008, 8, 207–220. [Google Scholar] [CrossRef]
- Brok, M.H.M.G.M.D.; Sutmuller, R.P.M.; van der Voort, R.; Bennink, E.J.; Figdor, C.G.; Ruers, T.J.M.; Adema, G.J. In Situ Tumor Ablation Creates an Antigen Source for the Generation of Antitumor Immunity. Cancer Res. 2004, 64, 4024–4029. [Google Scholar] [CrossRef]
- Takahashi, Y.; Izumi, Y.; Matsutani, N.; Dejima, H.; Nakayama, T.; Okamura, R.; Uehara, H.; Kawamura, M. Optimized magnitude of cryosurgery facilitating anti-tumor immunoreaction in a mouse model of Lewis lung cancer. Cancer Immunol. Immunother. 2016, 65, 973–982. [Google Scholar] [CrossRef]
- Liang, S.; Niu, L.; Xu, K.; Wang, X.; Liang, Y.; Zhang, M.; Chen, J.; Lin, M. Tumor cryoablation in combination with natural killer cells therapy and Herceptin in patients with HER2-overexpressing recurrent breast cancer. Mol. Immunol. 2017, 92, 45–53. [Google Scholar] [CrossRef] [PubMed]
- McArthur, H.L.; Diab, A.; Page, D.B.; Yuan, J.; Solomon, S.B.; Sacchini, V.; Comstock, C.; Durack, J.C.; Maybody, M.; Sung, J.; et al. A Pilot Study of Preoperative Single-Dose Ipilimumab and/or Cryoablation in Women with Early-Stage Breast Cancer with Comprehensive Immune Profiling. Clin. Cancer Res. 2016, 22, 5729–5737. [Google Scholar] [CrossRef]
- Si, T.; Guo, Z.; Hao, X. Combined Cryoablation and GM-CSF Treatment for Metastatic Hormone Refractory Prostate Cancer. J. Immunother. 2009, 32, 86–91. [Google Scholar] [CrossRef]
- Yuanying, Y.; Lizhi, N.; Feng, M.; Xiaohua, W.; Jianying, Z.; Fei, Y.; Feng, J.; Lihua, H.; Jibing, C.; Jialiang, L.; et al. Therapeutic outcomes of combining cryotherapy, chemotherapy and DC-CIK immunotherapy in the treatment of metastatic non-small cell lung cancer. Cryobiology 2013, 67, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Niu, L.-Z.; Li, J.-L.; Zeng, J.-Y.; Mu, F.; Liao, M.-T.; Yao, F.; Li, L.; Liu, C.-Y.; Chen, J.-B.; Zuo, J.-S.; et al. Combination treatment with comprehensive cryoablation and immunotherapy in metastatic hepatocellular cancer. World J. Gastroenterol. 2013, 19, 3473–3480. [Google Scholar] [CrossRef] [PubMed]
- Niu, L.; Chen, J.; He, L.; Liao, M.; Yuan, Y.; Zeng, J.; Li, J.; Zuo, J.; Xu, K. Combination Treatment With Comprehensive Cryoablation and Immunotherapy in Metastatic Pancreatic Cancer. Pancreas 2013, 42, 1143–1149. [Google Scholar] [CrossRef]
- Benzon, B.; Glavaris, S.A.; Simons, B.W.; Hughes, R.M.; Ghabili, K.; Mullane, P.; Miller, R.; Nugent, K.; Shinder, B.; Tosoian, J.; et al. Combining immune check-point blockade and cryoablation in an immunocompetent hormone sensitive murine model of prostate cancer. Prostate Cancer Prostatic Dis. 2018, 21, 126–136. [Google Scholar] [CrossRef]
- Zhang, M.; Yin, T.; Lu, Y.; Feng, H. The Application of Cytidyl Guanosyl Oligodeoxynucleotide Can Affect the Antitumor Immune Response Induced by a Combined Protocol of Cryoablation and Dendritic Cells in Lewis Lung Cancer Model. Med. Sci. Monit. 2016, 22, 1309–1317. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Wang, Q.; Lu, G.; Yin, Z.; He, X.; Xu, H.; Pan, J.; Zhang, S. In-situ administration of dendritic cells following argon–helium cryosurgery enhances specific antiglioma immunity in mice. Neuroreport 2014, 25, 900–908. [Google Scholar] [CrossRef]
- Li, F.; Guo, Z.; Yu, H.; Zhang, X.; Si, T.; Liu, C.; Yang, X.; Qi, L. Anti-tumor immunological response induced by cryoablation and anti-CTLA-4 antibody in an in vivo RM-1 cell prostate cancer murine model. Neoplasma 2014, 61, 659–671. [Google Scholar] [CrossRef]
- Alteber, Z.; Azulay, M.; Cafri, G.; Vadai, E.; Tzehoval, E.; Eisenbach, L. Cryoimmunotherapy with local co-administration of ex vivo generated dendritic cells and CpG-ODN immune adjuvant, elicits a specific antitumor immunity. Cancer Immunol. Immunother. 2014, 63, 369–380. [Google Scholar] [CrossRef]
- Machlenkin, A.; Goldberger, O.; Tirosh, B.; Paz, A.; Volovitz, I.; Bar-Haim, E.; Lee, S.-H.; Vadai, E.; Tzehoval, E.; Eisenbach, L. Combined Dendritic Cell Cryotherapy of Tumor Induces Systemic Antimetastatic Immunity. Clin. Cancer Res. 2005, 11, 4955–4961. [Google Scholar] [CrossRef]
- Xu, H.; Wang, Q.; Lin, C.; Yin, Z.; He, X.; Pan, J.; Lu, G.; Zhang, S. Synergism between cryoablation and GM-CSF: Enhanced immune function of splenic dendritic cells in mice with glioma. Neuroreport 2015, 26, 346–353. [Google Scholar] [CrossRef]
- Brok, M.H.D.; Sutmuller, R.P.; Nierkens, S.; Bennink, E.J.; Toonen, L.W.; Figdor, C.G.; Ruers, T.J.; Adema, G.J. Synergy between In situ Cryoablation and TLR9 Stimulation Results in a Highly Effective In vivo Dendritic Cell Vaccine. Cancer Res. 2006, 66, 7285–7292. [Google Scholar] [CrossRef]
- Waitz, R.; Solomon, S.B.; Petre, E.N.; Trumble, A.E.; Fassò, M.; Norton, L.; Allison, J.P. Potent Induction of Tumor Immunity by Combining Tumor Cryoablation with Anti–CTLA-4 Therapy. Cancer Res. 2012, 72, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Hamamoto, S.; Okuma, T.; Yamamoto, A.; Kageyama, K.; Takeshita, T.; Sakai, Y.; Nishida, N.; Matsuoka, T.; Miki, Y. Radiofrequency Ablation and Immunostimulant OK-432: Combination Therapy Enhances Systemic Antitumor Immunity for Treatment of VX2 Lung Tumors in Rabbits. Radiology 2013, 267, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Habibi, M.; Kmieciak, M.; Graham, L.; Morales, J.K.; Bear, H.D.; Manjili, M.H. Radiofrequency thermal ablation of breast tumors combined with intralesional administration of IL-7 and IL-15 augments anti-tumor immune responses and inhibits tumor development and metastasis. Breast Cancer Res. Treat. 2008, 114, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Yu, M.; Chen, L.; Kong, P.; Li, L.; Ma, G.; Ge, H.; Cui, Y.; Li, Z.; Pan, H.; et al. Enhanced antitumor efficacy through microwave ablation in combination with immune checkpoints blockade in breast cancer: A pre-clinical study in a murine model. Diagn. Interv. Imaging 2018, 99, 135–142. [Google Scholar] [CrossRef]
- Kuang, M.; Liu, S.Q.; Saijo, K.; Uchimura, E.; Huang, L.; Leong, K.; Lu, M.D.; Huang, J.F.; Ohno, T. Microwave tumour coagulation plus in situ treatment with cytokine-microparticles: Induction of potent anti-residual tumour immunity. Int. J. Hyperth. 2005, 21, 247–257. [Google Scholar] [CrossRef]
- Vanagas, T.; Gulbinas, A.; Pundzius, J.; Barauskas, G. Radiofrequency ablation of liver tumors (I): Biological background. Medicina 2010, 46, 13. [Google Scholar] [CrossRef]
- Slovak, R.; Ludwig, J.M.; Gettinger, S.N.; Herbst, R.S.; Kim, H.S. Immuno-thermal ablations—Boosting the anticancer immune response. J. Immunother. Cancer 2017, 5, 78. [Google Scholar] [CrossRef]
- Schneider, T.; Hoffmann, H.; Dienemann, H.; Herpel, E.; Heussel, C.P.; Enk, A.H.; Ring, S.; Mahnke, K. Immune Response After Radiofrequency Ablation and Surgical Resection in Nonsmall Cell Lung Cancer. Semin. Thorac. Cardiovasc. Surg. 2016, 28, 585–592. [Google Scholar] [CrossRef]
- Mizukoshi, E.; Yamashita, T.; Arai, K.; Sunagozaka, H.; Ueda, T.; Arihara, F.; Kagaya, T.; Yamashita, T.; Fushimi, K.; Kaneko, S. Enhancement of tumor-associated antigen-specific T cell responses by radiofrequency ablation of hepatocellular carcinoma. Hepatology 2012, 57, 1448–1457. [Google Scholar] [CrossRef] [PubMed]
- Tu, J.; Ji, J.; Wu, F.; Wang, Y.; Zhang, D.; Zhao, Z.; Ying, X. Effectiveness of Combined 131I-chTNT and Radiofrequency Ablation Therapy in Treating Advanced Hepatocellular Carcinoma. Cell Biochem. Biophys. 2014, 71, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, A.C.; Sodergren, M.; Jayant, K.; Cruz, F.S.; Spalding, D.; Pai, M.; Habib, N. Radiofrequency combined with immunomodulation for hepatocellular carcinoma: State of the art and innovations. World J. Gastroenterol. 2020, 26, 2040–2048. [Google Scholar] [CrossRef]
- Gameiro, S.R.; Higgins, J.P.; Dreher, M.R.; Woods, D.L.; Reddy, G.; Wood, B.J.; Guha, C.; Hodge, J.W. Combination Therapy with Local Radiofrequency Ablation and Systemic Vaccine Enhances Antitumor Immunity and Mediates Local and Distal Tumor Regression. PLoS ONE 2013, 8, e70417. [Google Scholar] [CrossRef]
- Nakagawa, H.; Mizukoshi, E.; Iida, N.; Terashima, T.; Kitahara, M.; Marukawa, Y.; Kitamura, K.; Nakamoto, Y.; Hiroishi, K.; Imawari, M.; et al. In vivo immunological antitumor effect of OK-432-stimulated dendritic cell transfer after radiofrequency ablation. Cancer Immunol. Immunother. 2014, 63, 347–356. [Google Scholar] [CrossRef]
- Ahmed, M.; Kumar, G.; Moussa, M.; Wang, Y.; Rozenblum, N.; Galun, E.; Goldberg, S.N. Hepatic Radiofrequency Ablation–induced Stimulation of Distant Tumor Growth Is Suppressed by c-Met Inhibition. Radiology 2016, 279, 103–117. [Google Scholar] [CrossRef]
- Greten, T.F.; Mauda-Havakuk, M.; Heinrich, B.; Korangy, F.; Wood, B.J. Combined locoregional-immunotherapy for liver cancer. J. Hepatol. 2019, 70, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Iezzi, R.; Contegiacomo, A.; Posa, A.; Attempati, N.; Punzi, E.; Tanzilli, A.; Margaritora, S.; Congedo, M.T.; Cassano, A.; Bria, E.; et al. Cryoablation in Locoregional Management of Complex Unresectable Chest Neoplasms. Tomography 2021, 7, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; Oklu, R.; Sheth, R.A. Thermal Ablative Therapies and Immune Checkpoint Modulation: Can Locoregional Approaches Effect a Systemic Response? Gastroenterol. Res. Pract. 2016, 2016, 9251375. [Google Scholar] [CrossRef]
- Yakkala, C.; Denys, A.; Kandalaft, L.; Duran, R. Cryoablation and immunotherapy of cancer. Curr. Opin. Biotechnol. 2020, 65, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Shao, Q.; O’Flanagan, S.; Lam, T.; Roy, P.; Pelaez, F.; Burbach, B.J.; Azarin, S.M.; Shimizu, Y.; Bischof, J.C. Engineering T cell response to cancer antigens by choice of focal therapeutic conditions. Int. J. Hyperth. 2019, 36, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Lin, S.; Liang, J.; Zhu, Y. PD-1 blockade enhances the anti-tumor immune response induced by cryoablation in a murine model of renal cell carcinoma. Cryobiology 2019, 87, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Liang, S.; Wang, X.; Liang, Y.; Zhang, M.; Chen, J.; Niu, L.; Xu, K. Cryoablation combined with allogenic natural killer cell immunotherapy improves the curative effect in patients with advanced hepatocellular cancer. Oncotarget 2017, 8, 81967–81977. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Xu, K.; Liang, S.; Wang, X.; Liang, Y.; Zhang, M.; Chen, J.; Niu, L. Prospective study of percutaneous cryoablation combined with allogenic NK cell immunotherapy for advanced renal cell cancer. Immunol. Lett. 2017, 184, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Liang, S.-Z.; Wang, X.-H.; Liang, Y.-Q.; Zhang, M.-J.; Niu, L.-Z.; Chen, J.-B.; Li, H.-B.; Xu, K.-C. Clinical efficacy of percutaneous cryoablation combined with allogenic NK cell immunotherapy for advanced non-small cell lung cancer. Immunol. Res. 2017, 65, 880–887. [Google Scholar] [CrossRef]
- Comen, E.A.; Bryce, Y.; Page, D.B.; Solomon, S.B.; Rodine, M.; Abaya, C.D.; Morris, E.A.; Plitas, G.; El-Tamer, M.; Gemignani, M.; et al. Preoperative checkpoint inhibition (CPI) and cryoablation (Cryo) in women with early-stage breast cancer (ESBC). J. Clin. Oncol. 2019, 37, 592. [Google Scholar] [CrossRef]
- Bulvik, B.E.; Rozenblum, N.; Gourevich, S.; Ahmed, M.; Andriyanov, A.V.; Galun, E.; Goldberg, S.N. Irreversible Electroporation versus Radiofrequency Ablation: A Comparison of Local and Systemic Effects in a Small-Animal Model. Radiology 2016, 280, 413–424. [Google Scholar] [CrossRef]
- Vivas, I.; Iribarren, K.; Lozano, T.; Cano, D.; Lasarte-Cia, A.; Chocarro, S.; Gorraiz, M.; Sarobe, P.; Hervás-Stubbs, S.; Bilbao, J.I.; et al. Therapeutic Effect of Irreversible Electroporation in Combination with Poly-ICLC Adjuvant in Preclinical Models of Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2019, 30, 1098–1105. [Google Scholar] [CrossRef]
- Alnaggar, M.; Lin, M.; Mesmar, A.; Liang, S.; Qaid, A.; Xu, K.; Chen, J.; Niu, L.; Yin, Z. Allogenic Natural Killer Cell Immunotherapy Combined with Irreversible Electroporation for Stage IV Hepatocellular Carcinoma: Survival Outcome. Cell. Physiol. Biochem. 2018, 48, 1882–1893. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Qin, Z.; Du, D.; Wu, Y.; Qiu, S.; Mu, F.; Xu, K.; Chen, J. Safety and Short-Term Efficacy of Irreversible Electroporation and Allogenic Natural Killer Cell Immunotherapy Combination in the Treatment of Patients with Unresectable Primary Liver Cancer. Cardiovasc. Interv. Radiol. 2018, 42, 48–59. [Google Scholar] [CrossRef]
- Zhao, J.; Wen, X.; Tian, L.; Li, T.; Xu, C.; Wen, X.; Melancon, M.P.; Gupta, S.; Shen, B.; Peng, W.; et al. Irreversible electroporation reverses resistance to immune checkpoint blockade in pancreatic cancer. Nat. Commun. 2019, 10, 899. [Google Scholar] [CrossRef] [PubMed]
- Timmer, F.E.; Geboers, B.; Nieuwenhuizen, S.; Schouten, E.A.; Dijkstra, M.; de Vries, J.J.; Tol, M.P.V.D.; de Gruijl, T.D.; Scheffer, H.J.; Meijerink, M.R. Locally Advanced Pancreatic Cancer: Percutaneous Management Using Ablation, Brachytherapy, Intra-arterial Chemotherapy, and Intra-tumoral Immunotherapy. Curr. Oncol. Rep. 2021, 23, 68. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, J.S.S.; Ray, P.; Hayashi, T.; Whisenant, T.C.; Vicente, D.; Carson, D.A.; Miller, A.M.; Schoenberger, S.P.; White, R.R. Irreversible Electroporation Combined with Checkpoint Blockade and TLR7 Stimulation Induces Antitumor Immunity in a Murine Pancreatic Cancer Model. Cancer Immunol. Res. 2019, 7, 1714–1726. [Google Scholar] [CrossRef]
- Lin, M.; Alnaggar, M.; Liang, S.; Wang, X.; Liang, Y.; Zhang, M.; Chen, J.; Niu, L.; Xu, K. An important discovery on combination of irreversible electroporation and allogeneic natural killer cell immunotherapy for unresectable pancreatic cancer. Oncotarget 2017, 8, 101795–101807. [Google Scholar] [CrossRef]
- Pan, Q.; Hu, C.; Fan, Y.; Wang, Y.; Li, R.; Hu, X. Efficacy of irreversible electroporation ablation combined with natural killer cells in treating locally advanced pancreatic cancer. J. BUON 2020, 25, 1643–1649. [Google Scholar] [PubMed]
- Lin, M.; Zhang, X.; Liang, S.; Luo, H.; Alnaggar, M.; Liu, A.; Yin, Z.; Chen, J.; Niu, L.; Jiang, Y. Irreversible electroporation plus allogenic Vγ9Vδ2 T cells enhances antitumor effect for locally advanced pancreatic cancer patients. Signal Transduct. Target. Ther. 2020, 5, 215. [Google Scholar] [CrossRef]
- Haen, S.P.; Pereira, P.L.; Salih, H.R.; Rammensee, H.-G.; Gouttefangeas, C. More Than Just Tumor Destruction: Immunomodulation by Thermal Ablation of Cancer. Clin. Dev. Immunol. 2011, 2011, 160250. [Google Scholar] [CrossRef]
- Chen, Z.; Shen, S.; Peng, B.; Tao, J. Intratumoural GM-CSF microspheres and CTLA-4 blockade enhance the antitumour immunity induced by thermal ablation in a subcutaneous murine hepatoma model. Int. J. Hyperth. 2009, 25, 374–382. [Google Scholar] [CrossRef]
- Yu, M.-A.; Liang, P.; Yu, X.-L.; Han, Z.-Y.; Dong, X.-J.; Wang, Y.; Cheng, C.; Li, X. Multiple courses of immunotherapy with different immune cell types for patients with hepatocellular carcinoma after microwave ablation. Exp. Ther. Med. 2015, 10, 1460–1466. [Google Scholar] [CrossRef]
- Zhou, P.; Liang, P.; Dong, B.; Yu, X.; Han, Z.; Xu, Y. Phase I clinical study of combination therapy with microwave ablation and cellular immunotherapy in hepatocellular carcinoma. Cancer Biol. Ther. 2011, 11, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Kallio, R.; Sequeiros, R.; Surcel, H.-M.; Ohtonen, P.; Kiviniemi, H.; Syrjälä, H. Early cytokine responses after percutaneous magnetic resonance imaging guided laser thermoablation of malignant liver tumors. Cytokine 2006, 34, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Vogl, T.J.; Wissniowski, T.T.; Naguib, N.N.N.; Hammerstingl, R.M.; Mack, M.G.; Münch, S.; Ocker, M.; Strobel, D.; Hahn, E.G.; Hänsler, J. Activation of tumor-specific T lymphocytes after laser-induced thermotherapy in patients with colorectal liver metastases. Cancer Immunol. Immunother. 2009, 58, 1557–1563. [Google Scholar] [CrossRef]
- Inchingolo, R.; Posa, A.; Mariappan, M.; Spiliopoulos, S. Locoregional treatments for hepatocellular carcinoma: Current evidence and future directions. World J. Gastroenterol. 2019, 25, 4614–4628. [Google Scholar] [CrossRef]
- Iezzi, R.; Pompili, M.; Posa, A.; Coppola, G.; Gasbarrini, A.; Bonomo, L. Combined locoregional treatment of patients with hepatocellular carcinoma: State of the art. World J. Gastroenterol. 2016, 22, 1935–1942. [Google Scholar] [CrossRef]
- Iezzi, R.; Pompili, M.; La Torre, M.F.; Campanale, M.C.; Montagna, M.; Saviano, A.; Cesario, V.; Siciliano, M.; Annicchiarico, E.; Agnes, S.; et al. Radiofrequency ablation plus drug-eluting beads transcatheter arterial chemoembolization for the treatment of single large hepatocellular carcinoma. Dig. Liver Dis. 2015, 47, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. In Seminars in Liver Disease; Thieme Medical Publishers, Inc.: New York, NY, USA, 1999; Volume 19, pp. 329–338. [Google Scholar]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236, Erratum in J. Hepatol. 2019, 70, 817. [Google Scholar]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Pereira, P.L.; Iezzi, R.; Manfredi, R.; Carchesio, F.; Bánsághi, Z.; Brountzos, E.; Spiliopoulos, S.; Echevarria-Uraga, J.J.; Gonçalves, B.; Inchingolo, R.; et al. The CIREL Cohort: A Prospective Controlled Registry Studying the Real-Life Use of Irinotecan-Loaded Chemoembolisation in Colorectal Cancer Liver Metastases: Interim Analysis. Cardiovasc. Interv. Radiol. 2020, 44, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; van Krieken, J.H.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Lammer, J.; Malagari, K.; Vogl, T.; Pilleul, F.; Denys, A.; Watkinson, A.; Pitton, M.; Sergent, G.; Pfammatter, T.; Terraz, S.; et al. Prospective Randomized Study of Doxorubicin-Eluting-Bead Embolization in the Treatment of Hepatocellular Carcinoma: Results of the PRECISION V Study. Cardiovasc. Interv. Radiol. 2010, 33, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; De Baere, T.; Burrel, M.; Caridi, J.G.; Lammer, J.; Malagari, K.; Martin, R.C.G.; O’Grady, E.; Real, M.I.; Vogl, T.J.; et al. Transcatheter Treatment of Hepatocellular Carcinoma with Doxorubicin-loaded DC Bead (DEBDOX): Technical Recommendations. Cardiovasc. Interv. Radiol. 2012, 35, 980–985. [Google Scholar] [CrossRef]
- Ayaru, L.; Pereira, S.P.; Alisa, A.; Pathan, A.A.; Williams, R.; Davidson, B.; Burroughs, A.K.; Meyer, T.; Behboudi, S. Unmasking of α-Fetoprotein-Specific CD4+ T Cell Responses in Hepatocellular Carcinoma Patients Undergoing Embolization. J. Immunol. 2007, 178, 1914–1922. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Wang, B.; Huang, Z.-L.; Shi, M.; Yu, X.-J.; Zheng, L.; Li, S.; Li, L. Increased Circulating Th17 Cells after Transarterial Chemoembolization Correlate with Improved Survival in Stage III Hepatocellular Carcinoma: A Prospective Study. PLoS ONE 2013, 8, e60444. [Google Scholar] [CrossRef]
- Lee, H.L.; Jang, J.W.; Lee, S.W.; Yoo, S.H.; Kwon, J.H.; Nam, S.W.; Bae, S.H.; Choi, J.Y.; Han, N.I.; Yoon, S.K. Inflammatory cytokines and change of Th1/Th2 balance as prognostic indicators for hepatocellular carcinoma in patients treated with transarterial chemoembolization. Sci. Rep. 2019, 9, 3260. [Google Scholar] [CrossRef]
- Zhang, J.; Li, H.; Gao, D.; Zhang, B.; Zheng, M.; Lun, M.; Wei, M.; Duan, R.; Guo, M.; Hua, J.; et al. A prognosis and impact factor analysis of DC-CIK cell therapy for patients with hepatocellular carcinoma undergoing postoperative TACE. Cancer Biol. Ther. 2018, 19, 475–483. [Google Scholar] [CrossRef]
- Semaan, A.; Dietrich, D.; Bergheim, D.; Dietrich, J.; Kalff, J.C.; Branchi, V.; Matthaei, H.; Kristiansen, G.; Fischer, H.-P.; Goltz, D. CXCL12 expression and PD-L1 expression serve as prognostic biomarkers in HCC and are induced by hypoxia. Virchows Arch. 2016, 470, 185–196. [Google Scholar] [CrossRef]
- Sangro, B.; Gomez-Martin, C.; de la Mata, M.; Iñarrairaegui, M.; Garralda, E.; Barrera, P.; Riezu-Boj, J.I.; Larrea, E.; Alfaro, C.; Sarobe, P.; et al. A clinical trial of CTLA-4 blockade with tremelimumab in patients with hepatocellular carcinoma and chronic hepatitis C. J. Hepatol. 2013, 59, 81–88. [Google Scholar] [CrossRef]
- Duffy, A.G.; Makarova-Rusher, O.V.; Kerkar, S.P.; Kleiner, D.E.; Fioravanti, S.; Walker, M.; Carey, S.; Figg, W.D.; Steinberg, S.M.; Anderson, V.; et al. A pilot study of tremelimumab—A monoclonal antibody against CTLA-4—In combination with either trans catheter arterial chemoembolization (TACE) or radiofrequency ablation (RFA) in patients with hepatocellular carcinoma (HCC). J. Clin. Oncol. 2015, 33, 4081. [Google Scholar] [CrossRef]
- Duffy, A.G.; Ulahannan, S.V.; Makorova-Rusher, O.; Rahma, O.; Wedemeyer, H.; Pratt, D.; Davis, J.L.; Hughes, M.S.; Heller, T.; ElGindi, M.; et al. Tremelimumab in combination with ablation in patients with advanced hepatocellular carcinoma. J. Hepatol. 2016, 66, 545–551. [Google Scholar] [CrossRef]
- Salem, R.; Mazzaferro, V.; Sangro, B. Yttrium 90 radioembolization for the treatment of hepatocellular carcinoma: Biological lessons, current challenges, and clinical perspectives. Hepatology 2013, 58, 2188–2197. [Google Scholar] [CrossRef] [PubMed]
- Salem, R.; Johnson, G.E.; Kim, E.; Riaz, A.; Bishay, V.; Boucher, E.; Fowers, K.; Lewandowski, R.; Padia, S.A. Yttrium-90 Radioembolization for the Treatment of Solitary, Unresectable HCC: The LEGACY Study. Hepatology 2021, 74, 2342–2352. [Google Scholar] [CrossRef] [PubMed]
- Stella, M.; Braat, A.J.A.T.; van Rooij, R.; de Jong, H.W.A.M.; Lam, M.G.E.H. Holmium-166 Radioembolization: Current Status and Future Prospective. Cardiovasc. Interv. Radiol. 2022, 45, 1634–1645. [Google Scholar] [CrossRef]
- Bilbao, J.L.; Iezzi, R.; Goldberg, S.N.; Sami, A.; Akhan, O.; Giuliante, F.; Pompili, M.; Crocetti, L.; Malagari, K.; Valentini, V.; et al. The ten commandments of hepatic radioembolization: Expert discussion and report from Mediterranean Interventional Oncology (MIOLive) congress 2017. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 4014–4021. [Google Scholar] [PubMed]
- Riaz, A.; Lewandowski, R.J.; Kulik, L.M.; Mulcahy, M.F.; Sato, K.T.; Ryu, R.K.; Omary, R.A.; Salem, R. Complications Following Radioembolization with Yttrium-90 Microspheres: A Comprehensive Literature Review. J. Vasc. Interv. Radiol. 2009, 20, 1121–1130. [Google Scholar] [CrossRef]
- Chew, V.; Lee, Y.H.; Pan, L.; Nasir, N.J.M.; Lim, C.J.; Chua, C.; Lai, L.; Hazirah, S.N.; Lim, T.K.H.; Goh, B.K.P.; et al. Immune activation underlies a sustained clinical response to Yttrium-90 radioembolisation in hepatocellular carcinoma. Gut 2018, 68, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Zhan, C.; Ruohoniemi, D.; Shanbhogue, K.P.; Wei, J.; Welling, T.H.; Gu, P.; Park, J.S.; Dagher, N.N.; Taslakian, B.; Hickey, R.M. Safety of Combined Yttrium-90 Radioembolization and Immune Checkpoint Inhibitor Immunotherapy for Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2019, 31, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Wehrenberg-Klee, E.; Goyal, L.; Dugan, M.; Zhu, A.X.; Ganguli, S. Y-90 Radioembolization Combined with a PD-1 Inhibitor for Advanced Hepatocellular Carcinoma. Cardiovasc. Interv. Radiol. 2018, 41, 1799–1802. [Google Scholar] [CrossRef]
- Tai, W.M.D.; Loke, K.S.H.; Gogna, A.; Tan, S.H.; Ng, D.C.E.; Hennedige, T.P.; Irani, F.; Lee, J.J.X.; Too, C.W.; Ng, M.C.; et al. A phase II open-label, single-center, nonrandomized trial of Y90-radioembolization in combination with nivolumab in Asian patients with advanced hepatocellular carcinoma: CA 209-678. J. Clin. Oncol. 2020, 38, 4590. [Google Scholar] [CrossRef]


{kind=link}
| Technique | PROS | CONS |
|---|---|---|
| RFA | RFA + CpG-B increase activating lymphocytes and OS [41] RFA + monoclonal antibody increase OS [44,45] RFA + a vaccine encoding CEA produce regression of distal metastasis and increases CEA-specific CD4+ T cells [46] RFA + dendritic cells stimulated by OK-432 increase the number of CD8+ T cells infiltrating untreated secondary tumors [47] | RFA alone stimulates HGF and VEGF, increases microvascular density and tumor cell replication [48] Incomplete ablation enhances neo-angiogenesis and tumor growth [49] |
| Cryoablation | CA + anti-PDL1 drugs lead to anti-tumor immune responses and delayed tumor growth of distant untreated tumors [54] CA + CpG-B induces regression of existing secondary tumors [19] CA + immunotherapy increases OS [25] CA + allogeneic NK cells increase OS [55,56,57] CA + anti-CTLA4 and anti-PD1 increase OS [58] | Low volume and level of literature evidence compared to RFA |
| IRE | IRE + poly-ICLC increases immunogenic response and reduces tumor growth [60] IRE + allogeneic NK cell immunotherapy increases OS, PFS, and decreases AFP [61,62] IRE + anti-PD1 drug promotes CD8+ T cell infiltration and increases OS [64] IRE + anti-PD1 and TLR-7 agonist improves local response and regression of untreated lesions [65] IRE + NK cells or allogenic Vγ9Vδ2 T cell infusion improves PFS, OR, OS rates [66,67,68] | Low volume and level of literature evidence compared to RFA |
| MWA | MWA + GM-CSF increases DFS and decreases tumor volume [70] MWA + adoptive immunotherapy increases peripheral lymphocytes [72] | MWA seems to be less immunogenic compared to RFA and CA [69] |
| HIFU/LiTT | HIFU and LiTT increase cytokine levels [69,73,74] | HIFU induces less immunogenic effect compared with RFA and cryoablation [69] |
| Technique | Immunotherapy Agent | Target Lesion and Study Type |
|---|---|---|
| RFA | Monoclonal antibody [44] | Intermediate- to advanced-stage HCC in liver cancer murine model study [44]. |
| CEA-encoding vaccine [46] | Distal colorectal cancer metastasis murine model study [46] | |
| OK-432-stimulated dendritic cells transfer [47] | In vivo untreated secondary tumors [47] | |
| CA | Anti-PDL1 [54] | Distant untreated tumors in renal cell carcinoma murine model study [54] |
| CpG-B [19] | Secondary tumors in melanoma murine model study [19] | |
| Immunotherapy | Metastatic liver cancer patients [25] | |
| Allogeneic NK cells [55,56,57] | Lung cancer, renal cancer, or HCC patients [55,56,57] | |
| Anti-CTLA4 and anti-PD1 [58] | Breast cancer patients [58] | |
| IRE | Poly-ICLC [60] | Mice and rabbit HCC model study [60] |
| Allogeneic NK cells [61,62] | Patients with metastatic liver tumor [61,62] | |
| Anti-PD1 [64] | Pancreatic ductal adenocarcinoma [64] | |
| Anti-PD1 and TLR-7 agonist [65] | Pancreatic ductal adenocarcinoma murine model [65] | |
| NK cells or allogeneic Vγ9Vδ2 T cell infusion [66,67,68] | Patients with pancreatic ductal adenocarcinoma [66,67,68] | |
| MWA | GM-CSF [70] | Murine hepatoma model [70] |
| Adoptive immunotherapy [72] | HCC patients [72] |
| Technique | PROS | CONS |
|---|---|---|
| TACE | TACE + CTLA4 inhibitor increases OS [91,92] TACE + ablation and tremelimumab increases OS, reduces tumor load, reduces non-ablated or non-embolized tumors [93] | Low volume and level of literature evidence Phase-I and -II clinical trials ongoing |
| TARE | TARE + nivolumab (or nivolumab + ipilimumab) showed good results in terms of OS and PFS [100] | Low volume and level of literature evidence Phase-I and -II clinical trials ongoing |
| Technique | Immunotherapy Agent | Target Lesion and Study Type |
|---|---|---|
| TACE | CTLA4 inhibitor [91,92] | Advanced HCC patients [91,92] |
| TACE + ablation | Tremelimumab [93] | Advanced HCC patients [93] |
| TARE | Nivolumab [100] | Retrospective study on advanced HCC patients [100] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Posa, A.; Contegiacomo, A.; Ponziani, F.R.; Punzi, E.; Mazza, G.; Scrofani, A.; Pompili, M.; Goldberg, S.N.; Natale, L.; Gasbarrini, A.; et al. Interventional Oncology and Immuno-Oncology: Current Challenges and Future Trends. Int. J. Mol. Sci. 2023, 24, 7344. https://doi.org/10.3390/ijms24087344
Posa A, Contegiacomo A, Ponziani FR, Punzi E, Mazza G, Scrofani A, Pompili M, Goldberg SN, Natale L, Gasbarrini A, et al. Interventional Oncology and Immuno-Oncology: Current Challenges and Future Trends. International Journal of Molecular Sciences. 2023; 24(8):7344. https://doi.org/10.3390/ijms24087344
Chicago/Turabian StylePosa, Alessandro, Andrea Contegiacomo, Francesca Romana Ponziani, Ernesto Punzi, Giulia Mazza, Annarita Scrofani, Maurizio Pompili, Shraga Nahum Goldberg, Luigi Natale, Antonio Gasbarrini, and et al. 2023. "Interventional Oncology and Immuno-Oncology: Current Challenges and Future Trends" International Journal of Molecular Sciences 24, no. 8: 7344. https://doi.org/10.3390/ijms24087344