
An Overview of Circulating Cell-Free Nucleic Acids in Diagnosis and Prognosis of Triple-Negative Breast Cancer
 , ,
, , 
Abstract
:1. Clinical and Molecular Characterization of Triple-Negative Breast Cancer
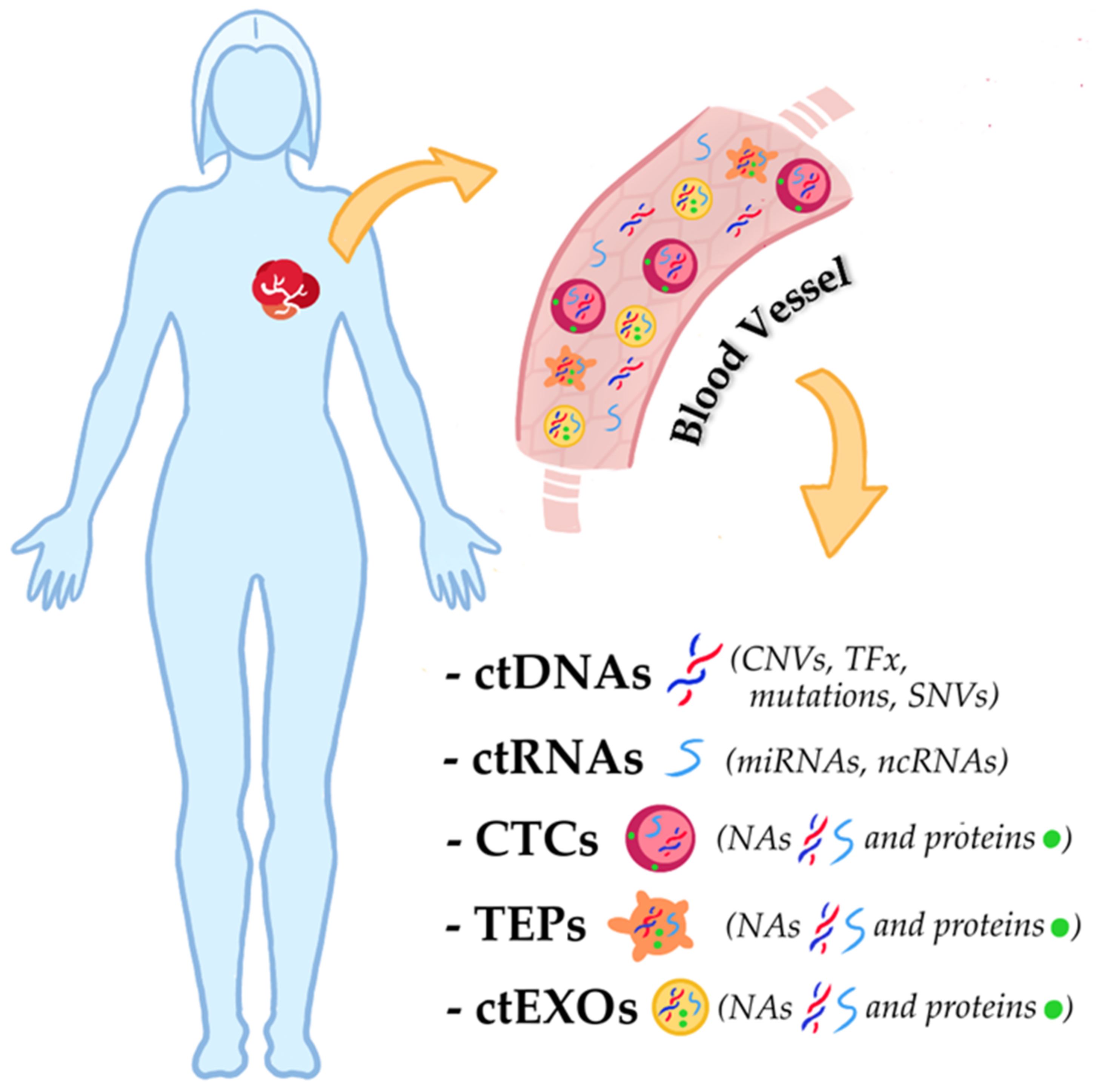
2. Liquid Biopsy and Circulating Cell-Free Nucleic Acids in TNBC
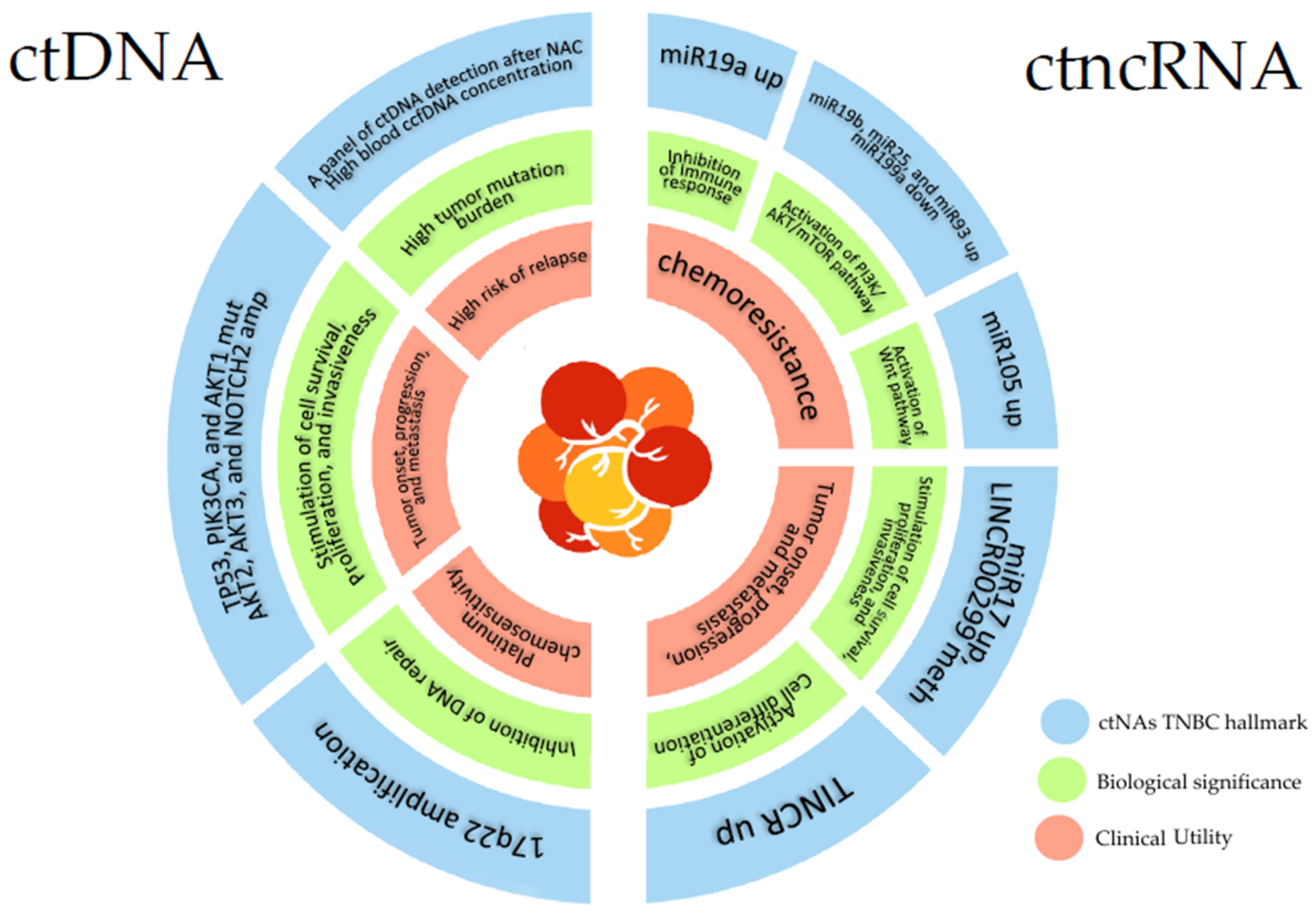
2.1. Circulating Cell-Free Tumor DNA in TNBC
2.2. Circulating Cell-Free Tumor Non-Coding RNA in TNBC

{kind=link}
{kind=link}
| Number of Patients and Controls/Age | Clinical Features at Sample Collection (Number of Patients) | Source of ctRNA (Analyte) | Target | Method | Main Findings | Ref. |
|---|---|---|---|---|---|---|
| 9 TNBC, 37 PR+/ER+ patients/TNBC: 56.48 yrs, PR+/ER+: 52.53 yrs. | All metastatic patients analyzed before surgery | Serum (ctmiRNA) | Expression of miR21, miR10b, miRNA-200c | qRT-PCR | Higher expression of miRNA 200c in ER+/PR+ patients than in TNBC ones. | [64] |
| 36 TNBC, 16 LumA, 41 LumB, 34 HC/BC: 46 ± 10.55 yrs; HC: 29 ± 7.5 yrs | Metastatic (23), non-metastatic (70); all patients analyzed before surgery and therapy | Plasma (ctmiRNA) | Expression of 84 breast cancer-related miRNAs | MIHS-109Z miScript miRNA Array Human panel, qRT-PCR | miR19a, miR19b, miR93, miR25, miR22 and miR210 have a higher expression in TNBC than lumA/B cancers and HC. MiR199a is under-expressed in TNBC than LumA/B and HCs. The overexpression of miR-93, miR-210, miR19a, and miR19b is associated with significantly worse OS. | [67] |
| 74 TNBC, 44 non-TNBC, 12 HC | All patients analyzed during NAC | Plasma (ctmiRNA) | Expression of miR93 and miR105 | qRT-PCR | miR93 and miR105 have a higher expression in TNBC than in non-TNBC patients. Overexpression of miR93 and miR105 is correlated with poor survival in TNBC patients. | [72] |
| 8 TNBC, 20 HC/TNBC: 55.4 yrs HC: 49 yrs | All metastatic patients analyzed before and during NAC | Serum; urine (ctmiRNA) | Expression of Let-7a; let-7e; miR-7, miR-9, miR-15a, miR-17, miR-18a, miR-19b, miR-21, miR-30b, miR-222 and miR-320c | qRT-PCR | Overexpression of let7a, let7e, miR21B and under-expression of miR15a, miR17, miR18a, miR19b, miR30b in TNBC serum compared to HC serum. Under-expression of miR18a, miR19b, miR30b, miR-222b, miR-320c in TNBC urine compared to HC urine. | [73] |
| 11 TNBC, 11 HER2+, 24 LumA, 20 LumB, 16 HC/BC: 47 yrs, HC: 45 yrs | Stage I (10), stage II (31), stage III (25); all patients analyzed before surgery and NAC | Plasma (ctmiRNA) | ctmiRNA expression profile | miScript miRNA PCR array human cancer Pathway Finder kit; miScript SYBR Green PCR kit | Specific Mirnoma signature for each BC subtype: LumA (miR-29b dw, miR-155 up, miR-181c dw), LumB (miR-148a dw, let-7d up, miR-92a up, let-7b up, miR-15a dw), HER2+ (miR-125b up, miR-134 dw, miR-143 up, miR-135b dw) and TNBC (miR-17 up, miR-150 dw, miR-210 up, miR-372 dw, let-7f dw, miR-133b up, miR-146b up, miR-7 up). | [76] |
| 72 TNBC, 105 non-TNBC, 60 BBD, 86 HC/TNBC: 46 < 50 yrs, 26 > 50 yrs, non-TNBC: 62 > 50 yrs, 43 > 50 yrs, BBD: 38 < 50 yrs, 22 > 50 yrs, HC: 53 < 50 yrs, 33 > 50 yrs | TNBC: stage I-II (42), stage III-IV (30); non-TNBC: stage I-II (59), stage III-IV (46) | Serum (ctlncRNA) | Expression of TINCR | qRT-PCR | TINCR is overexpressed in TNBC patients and is associated with worse clinicopathologic features than in other BC groups or controls (BBC; HC). | [81] |
| 57 TNBC, 124 HC/17 TNBC and 32 HC: 20–44 yrs; 10 TNBC and 17 HC: 45–49 yrs; 7 TNBC and 14 HC: 50–54 yrs; 7 TNBC and 19 HC: 55–59 yrs; 3 TNBC and 7 HC: 60–64 yrs; 8 TNBC and 21 HC: 65–69 yrs; 5 TNBC and 14 HC: >70 yrs | Stage 0 (1), stage I (13), stage II (26), stage III (9), stage IV (2), unknown (6); relapsed (18), metastatic (2) | Plasma (ctlncRNA) | A panel of specific methylation from a discovery set | MethyLight droplet digital PCR (ddPCR) | LINC00299 is hypermethylated in TNBC compared to HC. | [82] |
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BLIS | Basal-like triple-negative breast cancer |
| ccfDNAs | Circulating cell-free DNAs |
| ccfNAs | Circulating cell-free nucleic acids |
| cfDI | Circulating cell-free DNA integrity |
| CTCs | Circulating tumor cells |
| ctDNAs | Circulating cell-free tumor DNAs |
| ctmiRNAs | Circulating cell-free tumor microRNAs |
| ctmRNAs | Circulating cell-free tumor messenger RNAs |
| ctNAs | Circulating cell-free tumor nucleic acids |
| ctncRNAs | Circulating cell-free tumor non-coding RNAs |
| ER+ | Estrogen receptor-positive breast cancer |
| HER2+ | HER2-positive breast cancer |
| HR+ | Hormone receptor-positive breast cancer |
| IM | Immuno modulatory triple-negative breast cancer |
| LAR | Luminal androgen receptor triple-negative breast cancer |
| MAF | Mutant allele frequencies |
| MES | Mesenchymal-like triple-negative breast cancer |
| NAC | Neo-adjuvant chemotherapy |
| PARPi | PARP inhibitor |
| PR+ | Progesterone receptor-positive breast cancer |
| TFx | Tumor fraction of circulating cell-free DNA |
| TNBC | Triple-negative breast cancer |
| tncRNAs | Tumor non-coding RNAs |
| VAF | Variant allele frequencies |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E.; ESMO Guidelines Committee. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burstein, H.J.; Curigliano, G.; Thürlimann, B.; Weber, W.P.; Poortmans, P.; Regan, M.M.; Senn, H.J.; Winer, E.P.; Gnant, M. Panelists of the St Gallen Consensus Conference Customizing local and systemic therapies for women with early breast cancer: The St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1216–1235. [Google Scholar] [CrossRef]
- Rossing, M.; Pedersen, C.B.; Tvedskov, T.; Vejborg, I.; Talman, M.L.; Rǿnn, O.; Kroman, N.; Niels, K.; Nielsen, F.C.; Jensen, M.B.; et al. Clinical implications of intrinsic molecular subtypes of breast cancer for sentinel node status. Sci. Rep. 2021, 11, 2259. [Google Scholar] [CrossRef]
- Giaquinto, A.N.; Sung, H.; Miller, K.D.; Kramer, J.L.; Newman, L.A.; Minihan, A.; Jemal, A.; Siegel, R.L. Breast Cancer Statistics, 2022. CA Cancer J. Clin. 2022, 72, 524–541. [Google Scholar] [CrossRef]
- Skandan, S.P. 5 year Overall survival of triple negative breast cancer: A single institution experience. J. Clin. Oncol. 2017, 34. [Google Scholar] [CrossRef]
- Borri, F.; Granaglia, A. Pathology of triple negative breast cancer. Semin. Cancer Biol. 2021, 72, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Bergin, A.R.T.; Loi, S. Triple-negative breast cancer: Recent treatment advances. F1000Research 2019, 8, 1342. [Google Scholar] [CrossRef] [Green Version]
- Yin, L.; Duan, J.-J.; Bian, X.-W.; Yu, S.-C. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res. 2020, 22, 61. [Google Scholar] [CrossRef]
- Bou Zerdan, M.; Ghorayeb, T.; Saliba, F.; Allam, S.; Bou Zerdan, M.; Yaghi, M.; Bilani, N.; Jaafar, R.; Nahleh, Z. Triple Negative Breast Cancer: Updates on Classification and Treatment in 2021. Cancers 2022, 14, 1253. [Google Scholar] [CrossRef]
- Jaafar, R.; Mnich, K.; Dolan, S.; Hillis, J.; Almanza, A.; Logue, S.E.; Samali, A.; Gorman, A.M. RIP2 enhances cell survival by activation of NF-ĸB in triple negative breast cancer cells. Biochem. Biophys. Res. Commun. 2018, 497, 115–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrido-Castro, A.C.; Lin, N.U.; Polyak, K. Insights into Molecular Classifications of Triple-Negative Breast Cancer: Improving Patient Selection for Treatment. Cancer Discov. 2019, 9, 176–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geenen, J.J.J.; Linn, S.C.; Beijnen, J.H.; Schellens, J.H.M. PARP Inhibitors in the Treatment of Triple-Negative Breast Cancer. Clin. Pharmacokinet. 2018, 57, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Cortesi, L.; Rugo, H.S.; Jackisch, C. An Overview of PARP Inhibitors for the Treatment of Breast Cancer. Target. Oncol. 2021, 16, 255–282. [Google Scholar] [CrossRef]
- Kaufman, B.; Shapira-Frommer, R.; Schmutzler, R.K.; Audeh, M.W.; Friedlander, M.; Balmaña, J.; Mitchell, G.; Fried, G.; Stemmer, S.M.; Hubert, A.; et al. Olaparib monotherapy in patients with advanced cancer and a germline BRCA1/2 mutation. J. Clin. Oncol. 2015, 33, 244–250. [Google Scholar] [CrossRef]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef]
- Heimes, A.S.; Schmidt, M. Atezolizumab for the treatment of triple-negative breast cancer. Expert Opin. Investig. Drugs 2019, 28, 1–5. [Google Scholar] [CrossRef]
- Lei, Q.; Wang, D.; Sun, K.; Wang, L.; Zhang, Y. Resistance Mechanisms of Anti-PD1/PDL1 Therapy in Solid Tumors. Front. Cell Dev. Biol. 2020, 8, 672. [Google Scholar] [CrossRef]
- Emens, L.A.; Adams, S.; Barrios, C.H.; Diéras, V.; Iwata, H.; Loi, S.; Rugo, H.S.; Schneeweiss, A.; Winer, E.P.; Patel, S.; et al. First-line atezolizumab plus nab-paclitaxel for unresectable, locally advanced, or metastatic triple-negative breast cancer: IMpassion130 final overall survival analysis. Ann. Oncol. 2021, 32, 983–993. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.-A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Okazaki, S.; Sasaki, T.; Yasuda, S.; Abe, M.; Yoshida, N.; Yoshida, R.; Ishibashi, K.; Minami, Y.; Okumura, S.; Chiba, S.; et al. The feasibility of circulating tumor DNA analysis as a marker of recurrence in triple-negative breast cancer. Oncol. Lett. 2021, 21, 420. [Google Scholar] [CrossRef]
- Pascual, J.; Turner, N.C. Targeting the PI3-kinase pathway in triple-negative breast cancer. Ann. Oncol. 2019, 30, 1051–1060. [Google Scholar] [CrossRef] [Green Version]
- Ranucci, R. Cell-free DNA: Applications in different diseases. Methods Mol. Biol. 2019, 1909, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Poulet, G.; Massias, J.; Taly, V. Liquid Biopsy: General Concepts. Acta Cytol. 2019, 63, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Bode, A.M.; Dong, Z. Circulating tumor cells: Moving biological insights into detection. Theranostics 2017, 7, 2606–2619. [Google Scholar] [CrossRef] [PubMed]
- Siravegna, G.; Marsoni, S.; Siena, S.; Bardelli, A. Integrating liquid biopsies into the management of cancer. Nat. Rev. Clin. Oncol. 2017, 14, 531–548. [Google Scholar] [CrossRef] [PubMed]
- In’t Veld, S.G.J.G.; Wurdinger, T. Tumor-educated platelets. Blood 2019, 133, 2359–2364. [Google Scholar] [CrossRef]
- Contreras-Naranjo, J.C.; Wu, H.J.; Ugaz, V.M. Microfluidics for exosome isolation and analysis: Enabling liquid biopsy for personalized medicine. Lab A Chip 2017, 17, 3558–3577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, B.; Lei, Y.; Wang, J.; Zhu, L.; Wu, Y.; Zhang, H.; Wu, L.; Zhang, P.; Yang, C. Microfluidic-Based Exosome Analysis for Liquid Biopsy. Small Methods 2021, 5, e2001131. [Google Scholar] [CrossRef]
- Bachet, J.B.; Bouché, O.; Taieb, J.; Dubreuil, O.; Garcia, M.L.; Meurisse, A.; Normand, C.; Gornet, J.M.; Artru, P.; Louafi, S.; et al. RAS mutation analysis in circulating tumor DNA from patients with metastatic colorectal cancer: The AGEO RASANC prospective multicenter study. Ann. Oncol. 2018, 29, 1211–1219. [Google Scholar] [CrossRef]
- Sobhani, N.; Generali, D.; Zanconati, F.; Bortul, M.; Scaggiante, B. Cell-free DNA integrity for the monitoring of breast cancer: Future perspectives? World J. Clin. Oncol. 2018, 9, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.; Tran, N. miRNA interplay: Mechanisms and consequences in cancer. Dis. Model. Mech. 2021, 14, dmm047662. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.M.D.; Han, D.S.C.; Jiang, P.; Chiu, R.W.K. Epigenetics, fragmentomics, and topology of cell-free DNA in liquid biopsies. Science 2021, 372, eaaw3616. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Zhao, H. Next-generation sequencing in liquid biopsy: Cancer screening and early detection. Hum. Genom. 2019, 13, 34. [Google Scholar] [CrossRef] [Green Version]
- Mauri, D.; Kamposioras, K.; Matthaios, D.; Tolia, M.; Nixon, I.; Dambrosio, M.; Zarkavelis, G.; Papadimitriou, K.; Petricevic, B.; Kountourakis, P.; et al. Next-Generation Sequencing of Circulating Tumor DNA Can Optimize Second-Line Treatment in RAS Wild-Type Metastatic Colorectal Cancer after Progression on anti-EGFR Therapy: Time to Rethink Our Approach. Oncol. Res. Treat. 2022, 45, 216–221. [Google Scholar] [CrossRef]
- Bos, M.K.; Nasserinejad, K.; Jansen, M.P.H.M.; Angus, L.; Atmodimedjo, P.N.; de Jonge, E.; Dinjens, W.N.M.; van Schaik, R.H.N.; del Re, M.; Dubbink, H.J.; et al. Comparison of variant allele frequency and number of mutant molecules as units of measurement for circulating tumor DNA. Mol. Oncol. 2021, 15, 57–66. [Google Scholar] [CrossRef]
- Tsui, D.W.Y.; Cheng, M.L.; Shady, M.; Yang, J.L.; Stephens, D.; Won, H.; Srinivasan, P.; Huberman, K.; Meng, F.; Jing, X.; et al. Tumor fraction-guided cell-free DNA profiling in metastatic solid tumor patients. Genome Med. 2021, 13, 96. [Google Scholar] [CrossRef]
- Cailleux, F.; Agostinetto, E.; Lambertini, M.; Rothé, F.; Wu, H.T.; Balcioglu, M.; Kalashnikova, E.; Vincent, D.; Viglietti, G.; Gombos, A.; et al. Circulating Tumor DNA After Neoadjuvant Chemotherapy in Breast Cancer Is Associated With Disease Relapse. JCO Precis. Oncol. 2022, 6, e2200148. [Google Scholar] [CrossRef] [PubMed]
- Coombes, R.C.; Page, K.; Salari, R.; Hastings, R.K.; Armstrong, A.; Ahmed, S.; Ali, S.; Cleator, S.; Kenny, L.; Stebbing, J.; et al. Personalized Detection of Circulating Tumor DNA Antedates Breast Cancer Metastatic Recurrence. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 4255–4263. [Google Scholar] [CrossRef] [Green Version]
- Park, K.; Woo, M.; Kim, J.E.; Ahn, J.-H.; Jung, K.H.; Roh, J.; Gong, G.; Kim, S.-B. Efficacy of assessing circulating cell-free DNA using a simple fluorescence assay in patients with triple-negative breast cancer receiving neoadjuvant chemotherapy: A prospective observational study. Oncotarget 2017, 9, 3875. [Google Scholar] [CrossRef] [PubMed]
- Ortolan, E.; Appierto, V.; Silvestri, M.; Miceli, R.; Veneroni, S.; Folli, S.; Pruneri, G.; Vingiani, A.; Belfiore, A.; Cappelletti, V.; et al. Blood-based genomics of triple-negative breast cancer progression in patients treated with neoadjuvant chemotherapy. ESMO Open 2021, 6, 100086. [Google Scholar] [CrossRef]
- Wongchenko, M.J.; Kim, S.-B.; Saura, C.; Oliveira, M.; Lipson, D.; Kennedy, M.; Greene, M.; Breese, V.; Mani, A.; Xu, N.; et al. Circulating Tumor DNA and Biomarker Analyses from the LOTUS Randomized Trial of First-Line Ipatasertib and Paclitaxel for Metastatic Triple-Negative Breast Cancer. JCO Precis. Oncol. 2020, 4, 1012–1024. [Google Scholar] [CrossRef]
- Jacob, S.; Davis, A.A.; Gerratana, L.; Velimirovic, M.; Shah, A.N.; Wehbe, F.; Katam, N.; Zhang, Q.; Flaum, L.; Siziopikou, K.P.; et al. The use of serial circulating tumor DNA to detect resistance alterations in progressive metastatic breast cancer. Clin. Cancer Res. 2021, 27, 1361–1370. [Google Scholar] [CrossRef]
- Aggarwal, C.; Thompson, J.C.; Black, T.A.; Katz, S.I.; Fan, R.; Yee, S.S.; Chien, A.L.; Evans, T.L.; Bauml, J.M.; Alley, E.W.; et al. Clinical Implications of Plasma-Based Genotyping with the Delivery of Personalized Therapy in Metastatic Non-Small Cell Lung Cancer. JAMA Oncol. 2019, 5, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Chu, D.; Paoletti, C.; Gersch, C.; VanDenBerg, D.A.; Zabransky, D.J.; Cochran, R.L.; Wong, H.Y.; Toro, P.V.; Cidado, J.; Croessmann, S.; et al. ESR1 mutations in circulating plasma tumor DNA from metastatic breast cancer patients. Clin. Cancer Res. 2016, 22, 993–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cossu-Rocca, P.; Orrù, S.; Muroni, M.R.; Sanges, F.; Sotgiu, G.; Ena, S.; Pira, G.; Murgia, L.; Manca, A.; Uras, M.G.; et al. Analysis of PIK3CA mutations and activation pathways in triple negative breast cancer. PLoS ONE 2015, 10, 0141763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, N.; Pearson, A.; Sharpe, R.; Lambros, M.; Geyer, F.; Lopez-Garcia, M.A.; Natrajan, R.; Marchio, C.; Iorns, E.; Mackay, A.; et al. FGFR1 amplification drives endocrine therapy resistance and is a therapeutic target in breast cancer. Cancer Res. 2010, 70, 2085–2094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, P.H.; Wang, M.Y.; Lo, C.; Tsai, L.W.; Yen, T.C.; Huang, T.Y.; Huang, W.C.; Yang, K.; Chen, C.K.; Fan, S.C.; et al. Circulating Tumor DNA as a Predictive Marker of Recurrence for Patients with Stage II-III Breast Cancer Treated with Neoadjuvant Therapy. Front. Oncol. 2021, 11, 736769. [Google Scholar] [CrossRef] [PubMed]
- Cavallone, L.; Aguilar-Mahecha, A.; Lafleur, J.; Brousse, S.; Aldamry, M.; Roseshter, T.; Lan, C.; Alirezaie, N.; Bareke, E.; Majewski, J.; et al. Prognostic and predictive value of circulating tumor DNA during neoadjuvant chemotherapy for triple negative breast cancer. Sci. Rep. 2020, 10, 14704. [Google Scholar] [CrossRef]
- Pariyar, M.; Johns, A.; Thorne, R.F.; Scott, R.J.; Avery-Kiejda, K.A. Copy number variation in triple negative breast cancer samples associated with lymph node metastasis. Neoplasia 2021, 23, 743–753. [Google Scholar] [CrossRef]
- Yeow, Z.Y.; Lambrus, B.G.; Marlow, R.; Zhan, K.H.; Durin, M.A.; Evans, L.T.; Scott, P.M.; Phan, T.; Park, E.; Ruiz, L.A.; et al. Targeting TRIM37-driven centrosome dysfunction in 17q23-amplified breast cancer. Nature 2020, 585, 447–452. [Google Scholar] [CrossRef]
- Bärlund, M.; Tirkkonen, M.; Forozan, F.; Tanner, M.M.; Kallioniemi, O.; Kallioniemi, A. Increased copy number at 17q22-q24 by CGH in breast cancer is due to high-level amplification of two separate regions. Genes Chromosom. Cancer 1997, 20, 372–376. [Google Scholar] [CrossRef]
- Ka, N.L.; Na, T.Y.; Na, H.; Lee, M.H.; Park, H.S.; Hwang, S.; Kim, I.Y.; Seong, J.K.; Lee, M.O. NR1D1 recruitment to sites of DNA damage inhibits repair and is associated with chemosensitivity of breast cancer. Cancer Res. 2017, 77, 2453–2463. [Google Scholar] [CrossRef] [Green Version]
- Manning, A.L.; Ganem, N.J.; Bakhoum, S.F.; Wagenbach, M.; Wordeman, L.; Compton, D.A. The kinesin-13 proteins Kif2a, Kif2b, and Kif2c/MCAK have distinct roles during mitosis in human cells. Mol. Biol. Cell 2007, 18, 2970–2979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collier, K.A.; Asad, S.; Tallman, D.; Jenison, J.; Rajkovic, A.; Mardis, E.R.; Parsons, H.A.; Tolaney, S.M.; Winer, E.P.; Lin, N.U.; et al. Association of 17q22 Amplicon Via Cell-Free DNA with Platinum Chemotherapy Response in Metastatic Triple-Negative Breast Cancer. JCO Precis. Oncol. 2021, 5, 1777–1787. [Google Scholar] [CrossRef]
- Stover, D.G.; Parsons, H.A.; Ha, G.; Freeman, S.S.; Barry, W.T.; Guo, H.; Choudhury, A.D.; Gydush, G.; Reed, S.C.; Rhoades, J.; et al. Association of Cell-Free DNA Tumor Fraction and Somatic Copy Number Alterations with Survival in Metastatic Triple-Negative Breast Cancer. J. Clin. Oncol. 2018, 36, 543–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herzog, H.; Dogan, S.; Aktas, B.; Nel, I. Targeted Sequencing of Plasma-Derived vs. Urinary cfDNA from Patients with Triple-Negative Breast Cancer. Cancers 2022, 14, 4101. [Google Scholar] [CrossRef] [PubMed]
- Oshi, M.; Murthy, V.; Takahashi, H.; Huyser, M.; Okano, M.; Tokumaru, Y.; Rashid, O.M.; Matsuyama, R.; Endo, I.; Takabe, K. Urine as a source of liquid biopsy for cancer. Cancers 2021, 13, 2652. [Google Scholar] [CrossRef]
- Kimura, T. Non-coding Natural Antisense RNA: Mechanisms of Action in the Regulation of Target Gene Expression and Its Clinical Implications. Yakugaku Zasshi 2020, 140, 687–700. [Google Scholar] [CrossRef]
- Yan, H.; Bu, P. Non-coding RNA in cancer. Essays Biochem. 2021, 65, 625–639. [Google Scholar] [CrossRef]
- Panni, S.; Lovering, R.C.; Porras, P.; Orchard, S. Non-coding RNA regulatory networks. Biochim. Biophys. Acta Gene Regul. Mech. 2020, 1863, 194417. [Google Scholar] [CrossRef]
- Anastasiadou, E.; Jacob, L.S.; Slack, F.J. Non-coding RNA networks in cancer. Nat. Rev. Cancer 2017, 18, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Szilágyi, M.; Pös, O.; Márton, É.; Buglyó, G.; Soltész, B.; Keserű, J.; Penyige, A.; Szemes, T.; Nagy, B. Circulating cell-free nucleic acids: Main characteristics and clinical application. Int. J. Mol. Sci. 2020, 21, 6827. [Google Scholar] [CrossRef] [PubMed]
- Niedźwiecki, S.; Piekarski, J.; Szymańska, B.; Pawłowska, Z.; Jeziorski, A. Serum levels of circulating miRNA-21, miRNA-10b and miRNA-200c in triple-negative breast cancer patients. Ginekol. Pol. 2018, 89, 415–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anfossi, S.; Giordano, A.; Gao, H.; Cohen, E.N.; Tin, S.; Wu, Q.; Garza, R.J.; Debeb, B.G.; Alvarez, R.H.; Valero, V.; et al. High serum miR-19a levels are associated with inflammatory breast cancer and are predictive of favorable clinical outcome in patients with metastatic HER2+ inflammatory breast cancer. PLoS ONE 2014, 9, 83113. [Google Scholar] [CrossRef] [PubMed]
- Berber, U.; Yilmaz, I.; Narli, G.; Haholu, A.; Kucukodaci, Z.; Demirel, D. MiR-205 and miR-200c: Predictive micro RNAs for lymph node metastasis in triple negative breast cancer. J. Breast Cancer 2014, 17, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Qattan, A.; Al-Tweigeri, T.; Alkhayal, W.; Suleman, K.; Tulbah, A.; Amer, S. Clinical identification of dysregulated circulating microRNAs and their implication in drug response in triple negative breast cancer (TNBC) by target gene network and meta-analysis. Genes 2021, 12, 549. [Google Scholar] [CrossRef]
- Wishart, D.S.; Knox, C.; Guo, A.C.; Shrivastava, S.; Hassanali, M.; Stothard, P.; Chang, Z.; Woolsey, J. DrugBank: A comprehensive resource for in silico drug discovery and exploration. Nucleic Acids Res. 2006, 34, D668–D672. [Google Scholar] [CrossRef]
- Chen, H.; Pan, H.; Qian, Y.; Zhou, W.; Liu, X. MiR-25-3p Promotes the Proliferation of Triple Negative Breast Cancer by TargetingBTG2. Mol. Cancer 2018, 17, 4. [Google Scholar] [CrossRef]
- Grossman, R.L.; Heath, A.P.; Ferretti, V.; Varmus, H.E.; Lowy, D.R.; Kibbe, W.A.; Staudt, L.M. Toward a Shared Vision for Cancer Genomic Data. N. Engl. J. Med. 2016, 375, 1109–1112. [Google Scholar] [CrossRef]
- Zang, C.; Zhao, F.; Hua, L.; Pu, Y. The miR-199a-3p regulates the radioresistance of esophageal cancer cells via targeting the AK4 gene. Cancer Cell Int. 2018, 18, 186. [Google Scholar] [CrossRef] [Green Version]
- Li, H.Y.; Liang, J.L.; Kuo, Y.L.; Lee, H.H.; Calkins, M.J.; Chang, H.T.; Lin, F.C.; Chen, Y.C.; Hsu, T.I.; Hsiao, M.; et al. miR-105/93-3p promotes chemoresistance and circulating miR-105/93-3p acts as a diagnostic biomarker for triple negative breast cancer. Breast Cancer Res. 2017, 19, 133. [Google Scholar] [CrossRef]
- Triantafyllou, A.; Dovrolis, N.; Zografos, E.; Theoforopoulos, C.; Zografos, G.C.; Michalopoulos, N.V.; Gazouli, M. Circulating miRNA Expression Profiling in Breast Cancer Molecular Subtypes: Applying Machine Learning Analysis in Bioinformatics. Cancer Diagn. Progn. 2022, 2, 739–749. [Google Scholar] [CrossRef]
- Moi, L.; Braaten, T.; Al-Shibli, K.; Lund, E.; Busund, L.R. Differential expression of the miR-17-92 cluster and miR-17 family in breast cancer according to tumor type; results from the Norwegian Women and Cancer (NOWAC) study. J. Transl. Med. 2019, 17, 334. [Google Scholar] [CrossRef] [Green Version]
- Sugita, B.M.; Rodriguez, Y.; Fonseca, A.S.; Nunes Souza, E.; Kallakury, B.; Cavalli, I.J.; Ribeiro, E.M.S.F.; Aneja, R.; Cavalli, L.R. MiR-150-5p Overexpression in Triple-Negative Breast Cancer Contributes to the In Vitro Aggressiveness of This Breast Cancer Subtype. Cancers 2022, 14, 2156. [Google Scholar] [CrossRef]
- Ritter, A.; Hirschfeld, M.; Berner, K.; Rücker, G.; Jäger, M.; Weiss, D.; Medl, M.; Nöthling, C.; Gassner, S.; Asberger, J.; et al. Circulating non-coding RNA-biomarker potential in neoadjuvant chemotherapy of triple negative breast cancer? Int. J. Oncol. 2020, 56, 47–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, T.; Grote, P. Beyond the RNA-dependent function of LncRNA genes. eLife 2020, 9, e60583. [Google Scholar] [CrossRef]
- Moonmuang, S.; Chaiyawat, P.; Jantrapirom, S.; Pruksakorn, D.; lo Piccolo, L. Circulating long non-coding RNAs as novel potential biomarkers for osteogenic sarcoma. Cancers 2021, 13, 4214. [Google Scholar] [CrossRef] [PubMed]
- Kretz, M. TINCR, staufen1, and cellular differentiation. RNA Biol. 2013, 10, 1597–1601. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Du, Y.; Hu, X.; Zhao, L.; Xia, W. Up-regulation of ceRNA TINCR by SP1 contributes to tumorigenesis in breast cancer. BMC Cancer 2018, 18, 367. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, S.; Xiao, H.; Deng, X. Serum lncRNA TINCR Serve as a Novel Biomarker for Predicting the Prognosis in Triple-Negative Breast Cancer. Technol. Cancer Res. Treat. 2020, 19, 1533033820965574. [Google Scholar] [CrossRef]
- Bermejo, J.L.; Huang, G.; Manoochehri, M.; Mesa, K.G.; Schick, M.; Silos, R.G.; Ko, Y.D.; Brüning, T.; Brauch, H.; Lo, W.Y.; et al. Long intergenic noncoding RNA 299 methylation in peripheral blood is a biomarker for triple-negative breast cancer. Epigenomics 2019, 11, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.Y. GATA3: A master of many trades in immune regulation. Trends Immunol. 2014, 35, 233–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mace, E.; Hsu, A.; Monaco-Shawer, L.; Makedonas, G.; Rosen, J.; Dropulic, L.; Cohen, J.; Frenkel, E.; Bagwell, J.; Sullivan, J.; et al. Mutations in GATA2 cause human NK cell deficiency with specific loss of the CD56bright subset. Blood 2013, 121, 2669–2677. [Google Scholar] [CrossRef] [Green Version]
- Tay, T.K.Y.; Tan, P.H. Liquid biopsy in breast cancer: A focused review. Arch. Pathol. Lab. Med. 2021, 145, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Zhang, Y.; Ren, Q.; Wang, X.; Zhu, J.; Yin, F.; Li, Z.; Zhang, M. Tetrahedral DNA nanostructure based biosensor for high-performance detection of circulating tumor DNA using all-carbon nanotube transistor. Biosens. Bioelectron. 2022, 197, 113785. [Google Scholar] [CrossRef] [PubMed]
- Fan, T.; Mao, Y.; Sun, Q.; Liu, F.; Lin, J.S.; Liu, Y.; Cui, J.; Jiang, Y. Branched rolling circle amplification method for measuring serum circulating microRNA levels for early breast cancer detection. Cancer Sci. 2018, 109, 2897–2906. [Google Scholar] [CrossRef] [PubMed]


| Number of Patients and Controls/Age | Clinical Features at Sample Collection (Number of Patients) | Source of ctDNA | Target | Method | Main Finding | Ref. |
|---|---|---|---|---|---|---|
| 13 TNBC, 11 HER2+, 20 ER+/57% patients < 50 yrs, 43% > 50 yrs | Stage II (31) and Stage III (14); all patients analyzed at pre- and post-NAC, pre- and post-surgical resection | Plasma | A panel of personalized tumor-informed DNA variants | bespoke multiplex polymerase chain reaction NGS ctDNA assay, Signater | Higher ctDNA detection at baseline (before NAC) in TNBC patients than in HER2+ and ER+. Shorter EFS for patients with high VAF after NAC time point and beyond. | [38] |
| 72 TNBC/46 yrs (25–71) | Stage I (5), Stage II (43), Stage III (23), Stage IV (1), 18 relapsed; all patients analyzed pre- and post-NAC | Plasma | cfDNA concentration | SYBR Gold Nucleic Acid Gel Stain | The average cfDNA concentration decreased significantly after NAC. Patients with a cfDNA concentration > 264 ng/mL have a higher risk of relapse. | [40] |
| 31 TNBC/19 patients < 50 yrs, 12 patients > 50 yrs | Stage II (24), Stage III (7), metastatic (9), relapsed (1); all patients analyzed before and after NAC | Plasma | A panel of personalized tumor-informed DNA mutations | IonAmpliSeq Cancer Hotspot Panel v2 CHPv2, ddPCR | The detection ctDNA after NAC resulted in shorter EFS. | [41] |
| 89 TNBC/54 yrs (26–81) | All metastatic patients analyzed before and during treatment with Ipatasertib plus placitaxel | Plasma | cfDNA genomic profile | FoundationACT hybrid capture NGS assays, FoundationOne hybrid capture NGS assays | Patients with PIK3CA or AKT1 mutations had 100% concordance between ctDNA and tissue sequencing. Patients with PIK3CA/AKT mutations have a higher improvement in PFS after treatment with Ipatasertib than patients without mutations. High VAF on-treatment was associated with worse PFS. | [42] |
| 22 TNBC, 44 HR+, 20 HER2+, (progression group, PG); 6 TNBC, 54 HR+, 2 HER2+, (control group, CG)/ 19 PG and 10 CG patients < 45 yrs, 51 PG and 36 CG patients: 45–65 yrs, 17 PG and 16 CG patients > 65 yrs | All metastatic patients analyzed at three different time points during the disease clinical management | Plasma | A panel of NCNN-recommended genes mutations and CNVs | Guardant360 NGS assay | Increase in MAF at different time points was associated with events of tumor progression. TP53, PIK3CA (for TNBC), ESR1, FGFR1, AR, and ERBB2 (for HR+) are key alterations associated with progression and chemotherapy resistance. The changes in TP53, PIK3CA, ERBB2, EGFR, ESR1, CCNE1, MYC, NF1, MET, and KIT showed high concordance (approximately 80%) between plasma and tissue. | [43] |
| 25 TNBC, 29 HER2+, 41 ER+ 25 TNBC, 29 HER2+, 41 ER+/TNBC: 52 ± 10.2 yrs; HER2+: 49.3 ± 8.7 yrs; ER+: 49.2 ± 7.8 yrs | Stage II and III patients analyzed before and after NAC-surgery | Plasma | TP53, PI3KCA, HER2, GATA3, CDH1, PTEN, AKT1, ESR1, S100A7-9, ZNF703, B2M, CCND1, c-MYC mutations and CNVs | QIAseq Targeted DNAPanel, Illumina MiSeq Reagent Kit v2, 2 × 150 bp reads, OncoCNV | Detection of ctDNA after NAC led to short RFS. The RFS of TNBC patients was shorter than in HER2+ patients. | [48] |
| 26 TNBC/15 patients < 50 yrs; 11 patients > 50 yrs | Unknown (2), Stage I (1), Stage II (19), Stage III (4); all patients analyzed before, during, and after NAC | Plasma | A personalized panel of 4–5 tumor-informed variants | Whole exome sequencing (WES), ddPCR | ctDNA detection during NAC was strongly predictive of residual tumor at the surgery. ctDNA detection at the end of NAC indicated significantly worse relapse-free survival and overall survival. | [49] |
| 58 TNBC/45 yrs | Stage I (12), Stage II (33), Stage III (17), Stage IV (8); all patients are treated with cisplatin alone or in combination with paclitaxel | Plasma | amplification of 17q22 | Gistic 2.0 | Patients with 17q22 amplification have a better PFS after cisplatin treatment. | [55] |
| 164 TNBC/34 patients < 40 yrs, 62 patients: 40–50 years, 45 patients: 50–60 yrs, 20 patients > 60 yrs | Stage I (22), Stage II (80), Stage III (43), Stage IV (16); all metastatic patients received NAC treatment | Plasma | cfDNA genomic profile, CN of 25 breast cancer-related genes | Low coverage whole genomic sequencing | TFx > 10% was associated with significantly worse OS. A higher amplification rate for AKT2, AKT3, and NOTCH2 was seen in metastasis compared to paired primary tumors. | [56] |
| 15 TNBC/48 yrs | Early-stage patients analyzed after NAC and before surgical resection | Plasma; urine | A panel of 93 breast cancer-related genes mutations | QIAseq Human Breast cancer PaneL, Illumina NGS | Mutations of NF1, CHEK2, KMT2C, and PTEN shown in paired blood and urine biopsy. | [57] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tierno, D.; Grassi, G.; Zanconati, F.; Bortul, M.; Scaggiante, B. An Overview of Circulating Cell-Free Nucleic Acids in Diagnosis and Prognosis of Triple-Negative Breast Cancer. Int. J. Mol. Sci. 2023, 24, 1799. https://doi.org/10.3390/ijms24021799
Tierno D, Grassi G, Zanconati F, Bortul M, Scaggiante B. An Overview of Circulating Cell-Free Nucleic Acids in Diagnosis and Prognosis of Triple-Negative Breast Cancer. International Journal of Molecular Sciences. 2023; 24(2):1799. https://doi.org/10.3390/ijms24021799
Chicago/Turabian StyleTierno, Domenico, Gabriele Grassi, Fabrizio Zanconati, Marina Bortul, and Bruna Scaggiante. 2023. "An Overview of Circulating Cell-Free Nucleic Acids in Diagnosis and Prognosis of Triple-Negative Breast Cancer" International Journal of Molecular Sciences 24, no. 2: 1799. https://doi.org/10.3390/ijms24021799