
Peripheral mRNA Expression and Prognostic Significance of Emotional Stress Biomarkers in Metastatic Breast Cancer Patients
 ,
,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Psychometric Stress Evaluation
2.3. Blood Sampling and Data Collection
2.4. Quantitative RT-PCR for Gene Expression Profiling
2.4.1. RNA Extraction and cDNA Synthesis
2.4.2. Primers for RT-PCR
2.4.3. Quantification of Gene Expression
2.5. Survival Analysis of Breast Cancer Patients Using a Kaplan–Meier Plotter
2.6. Statistical Analysis
3. Results
3.1. Distress Screening Using QSC R-10
3.2. Expression and Prognostic Significance of Stress-Related Genes in Breast Cancer
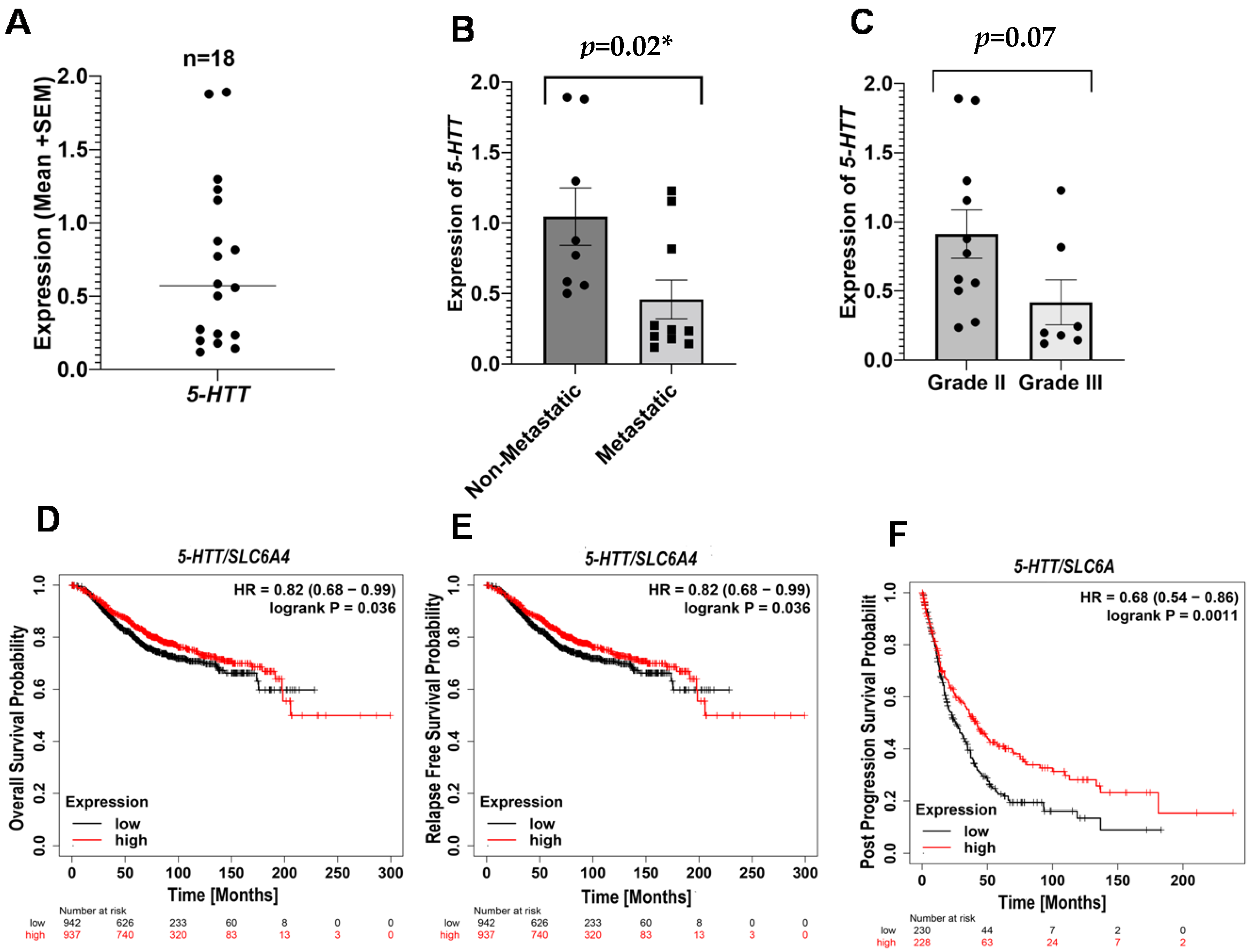
3.2.1. Serotonin Transporter (5-HTT) in Breast Cancer
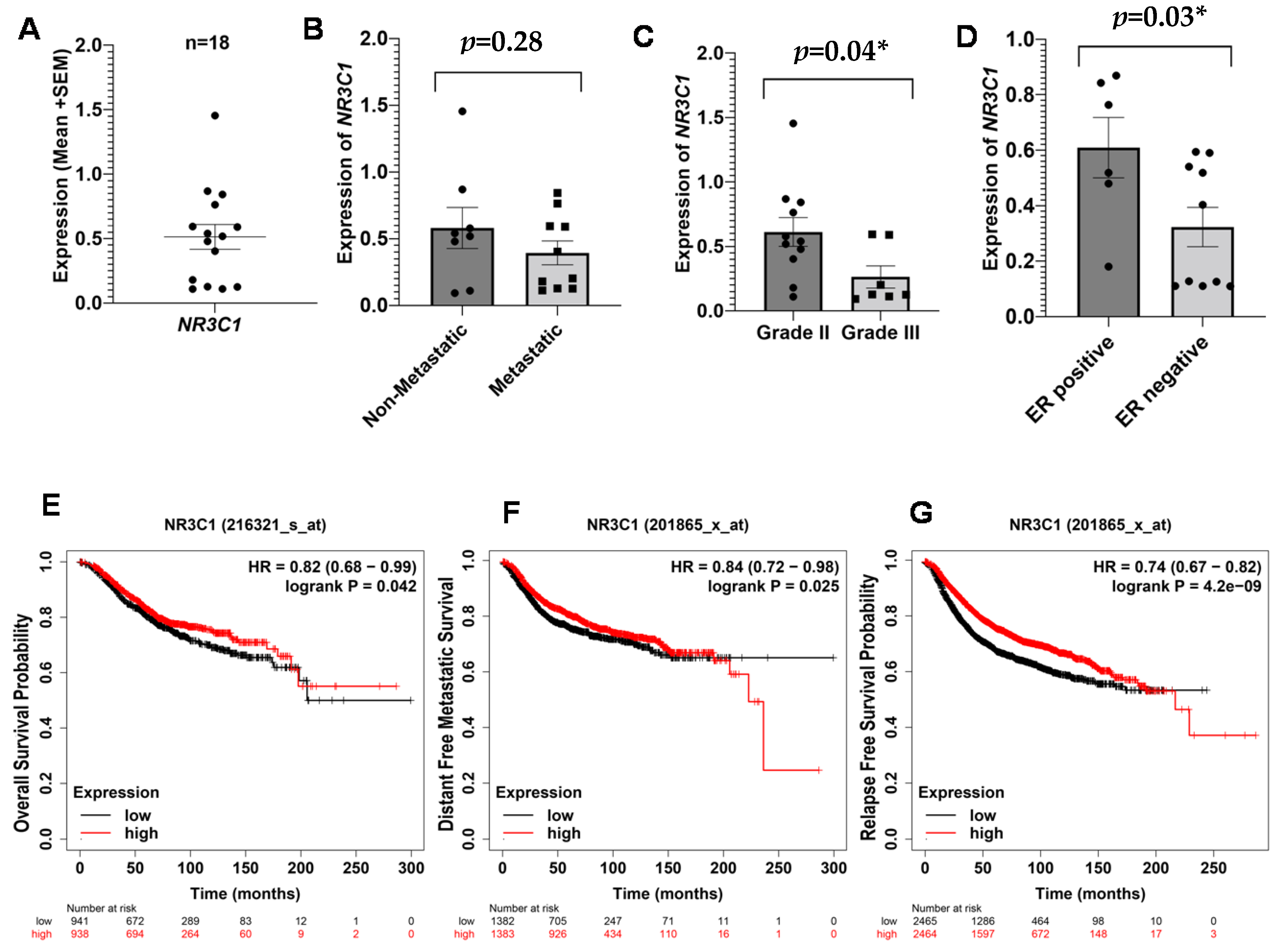
3.2.2. NR3C1 in Breast Cancer
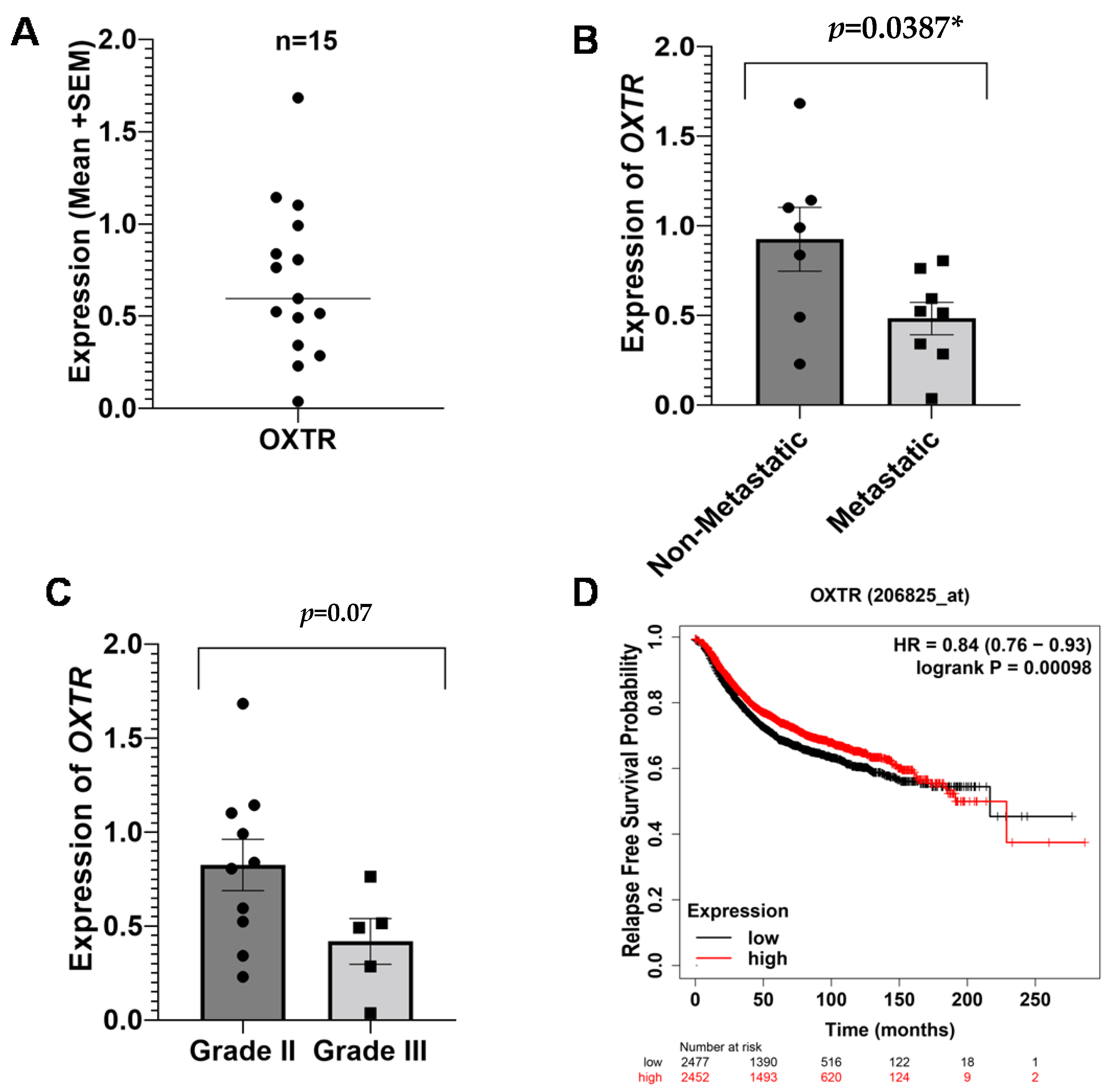
3.2.3. Oxytocin Receptor (OXTR) in Breast Cancer
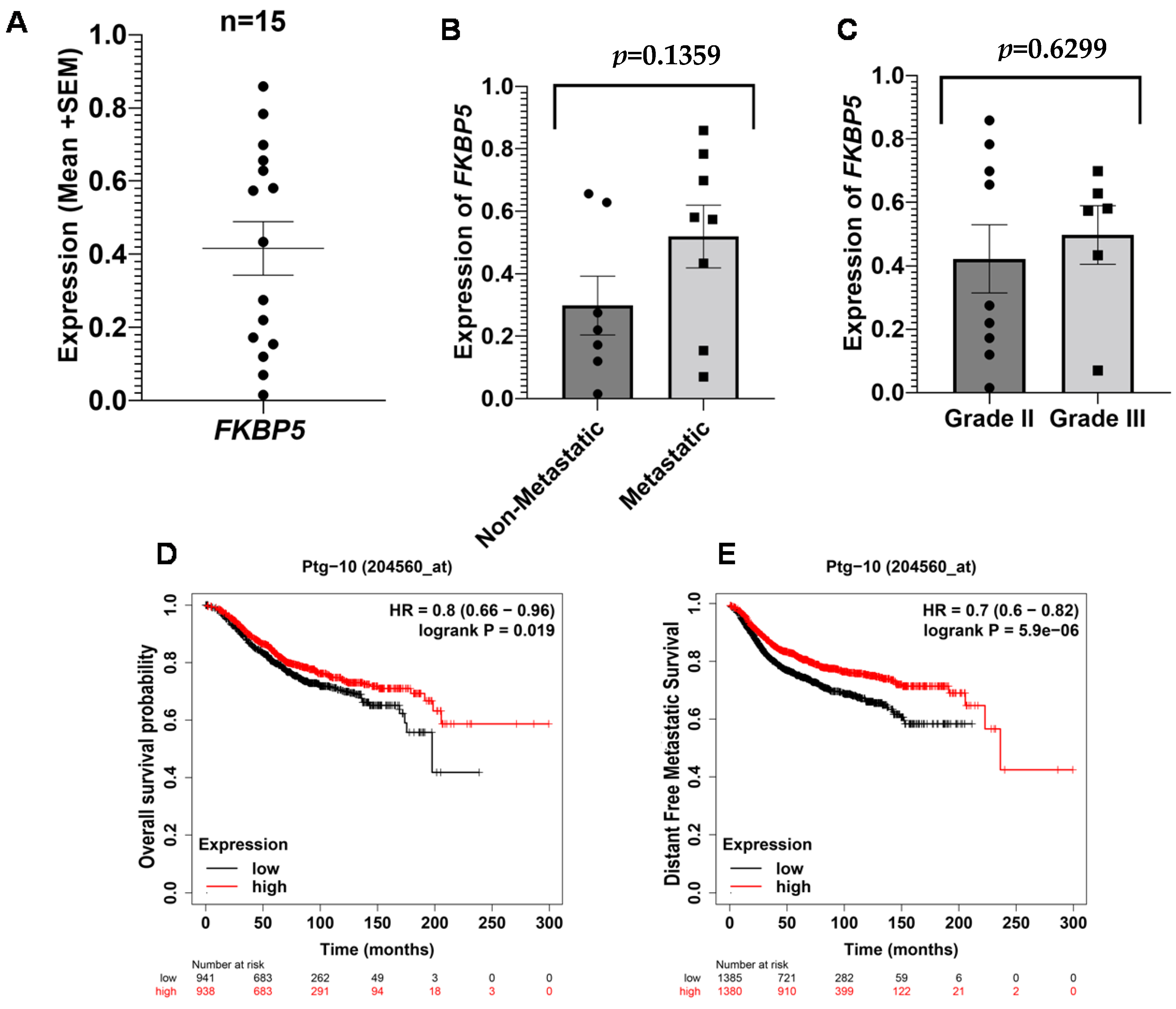
3.2.4. FKBP Prolyl Isomerase 5 (FKBP5/Ptg-10) in Breast Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kreiberg, M.; Bandak, M.; Lauritsen, J.; Andersen, K.K.; Skøtt, J.W.; Johansen, C.; Agerbaek, M.; Holm, N.V.; Lau, C.J.; Daugaard, G. Psychological stress in long-term testicular cancer survivors: A Danish nationwide cohort study. J. Cancer Surviv. 2020, 14, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.; Yip, A. Hans Selye (1907–1982): Founder of the stress theory. Singap. Med. J. 2018, 59, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Wang, C.; Wang, W.; Dong, H.; Hou, P.; Tang, Y. Chronic mild stress impairs cognition in mice: From brain homeostasis to behavior. Life Sci. 2008, 82, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Antoni, M.H.; Dhabhar, F.S. The impact of psychosocial stress and stress management on immune responses in patients with cancer. Cancer 2019, 125, 1417–1431. [Google Scholar] [CrossRef] [PubMed]
- Van Oers, H.; Schlebusch, L. Indicators of psychological distress and body image disorders in female patients with breast cancer. J. Mind Med. Sci. 2020, 7, 179–188. [Google Scholar] [CrossRef]
- Palesh, O.; Scheiber, C.; Kesler, S.; Mustian, K.; Koopman, C.; Schapira, L. Management of side effects during and post-treatment in breast cancer survivors. Breast J. 2018, 24, 167–175. [Google Scholar] [CrossRef]
- Redeker, N.S.; Lev, E.L.; Ruggiero, J. Insomnia, fatigue, anxiety, depression, and quality of life of cancer patients undergoing chemotherapy. Sch. Inq. Nurs. Pract. 2000, 14, 275–290. [Google Scholar]
- Ma, Y.; Rosenheck, R.; He, H. Psychological stress among health care professionals during the 2019 novel coronavirus disease Outbreak: Cases from online consulting customers. Intensive Crit. Care Nurs. 2020, 61, 102905. [Google Scholar] [CrossRef]
- Hackett, R.A.; Steptoe, A. Type 2 diabetes mellitus and psychological stress—A modifiable risk factor. Nat. Rev. Endocrinol. 2017, 13, 547–560. [Google Scholar] [CrossRef]
- Wirtz, P.H.; von Känel, R. Psychological stress, inflammation, and coronary heart disease. Curr. Cardiol. Rep. 2017, 19, 111. [Google Scholar] [CrossRef]
- Jang, H.-J.; Boo, H.-J.; Lee, H.J.; Min, H.-Y.; Lee, H.-Y. Chronic stress facilitates lung tumorigenesis by promoting exocytosis of IGF2 in lung epithelial cells. Cancer Res. 2016, 76, 6607–6619. [Google Scholar] [CrossRef] [PubMed]
- Zong, J.C.; Wang, X.; Zhou, X.; Wang, C.; Chen, L.; Yin, L.J.; He, B.C.; Deng, Z.L. Gut-derived serotonin induced by depression promotes breast cancer bone metastasis through the RUNX2/PTHrP/RANKL pathway in mice. Oncol. Rep. 2016, 35, 739–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, H.; Li, C.; He, Y.; Griffin, R.; Ye, Q.; Li, L. Chronic stress promotes oral cancer growth and angiogenesis with increased circulating catecholamine and glucocorticoid levels in a mouse model. Oral Oncol. 2015, 51, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Eliwa, H.; Brizard, B.; Le Guisquet, A.-M.; Hen, R.; Belzung, C.; Surget, A. Adult neurogenesis augmentation attenuates anhedonia and HPA axis dysregulation in a mouse model of chronic stress and depression. Psychoneuroendocrinology 2021, 124, 105097. [Google Scholar] [CrossRef]
- Ma, L.; Shen, Q.; Yang, S.; Xie, X.; Xiao, Q.; Yu, C.; Cao, L.; Fu, Z. Effect of chronic corticosterone-induced depression on circadian rhythms and age-related phenotypes in mice. Acta Biochim. Biophys. Sin. 2018, 50, 1236–1246. [Google Scholar] [CrossRef]
- Otto-Meyer, S.; Lumibao, J.; Kim, E.; Ladomersky, E.; Zhai, L.; Lauing, K.L.; Scholtens, D.M.; Penedo, F.; Amidei, C.; Lukas, R.V. The interplay among psychological distress, the immune system, and brain tumor patient outcomes. Curr. Opin. Behav. Sci. 2019, 28, 44–50. [Google Scholar] [CrossRef]
- Toh, T.B.; Lim, J.J.; Chow, E.K.-H. Epigenetics in cancer stem cells. Mol. Cancer 2017, 16, 29. [Google Scholar] [CrossRef] [Green Version]
- Peng, H.; Zhu, Y.; Strachan, E.; Fowler, E.; Bacus, T.; Roy-Byrne, P.; Goldberg, J.; Vaccarino, V.; Zhao, J. Childhood trauma, DNA methylation of stress-related genes, and depression: Findings from two monozygotic twin studies. Psychosom. Med. 2018, 80, 599. [Google Scholar] [CrossRef]
- Senf, B.; Grabowski, K.; Spielmann, N.; Fettel, J. Quality of life and distress assessed with self and external assessment screening tools in patients with hematologic malignancies attending treatment in an acute hospital. Qual. Life Res. 2020, 29, 3375–3385. [Google Scholar] [CrossRef]
- Antiabong, J.F.; Ngoepe, M.G.; Abechi, A.S. Semi-quantitative digital analysis of polymerase chain reaction-electrophoresis gel: Potential applications in low-income veterinary laboratories. Vet. World 2016, 9, 935. [Google Scholar] [CrossRef]
- Zheng, H.; Zhang, G.; Zhang, L.; Wang, Q.; Li, H.; Han, Y.; Xie, L.; Yan, Z.; Li, Y.; An, Y.; et al. Comprehensive review of web servers and bioinformatics tools for cancer prognosis analysis. Front. Oncol. 2020, 10, 68. [Google Scholar] [CrossRef] [PubMed]
- Motavalli, R.; Majidi, T.; Pourlak, T.; Abediazar, S.; Shoja, M.M.; Vahed, S.Z.; Etemadi, J. The clinical significance of the glucocorticoid receptors: Genetics and epigenetics. J. Steroid Biochem. Mol. Biol. 2021, 213, 105952. [Google Scholar] [CrossRef]
- Binder, E.B. The role of FKBP5, A co-chaperone of the glucocorticoid receptor in the pathogenesis and therapy of affective and anxiety disorders. Psychoneuroendocrinology 2009, 34, S186–S195. [Google Scholar] [CrossRef]
- Wilker, S.; Pfeiffer, A.; Kolassa, S.; Elbert, T.; Lingenfelder, B.; Ovuga, E.; Papassotiropoulos, A.; De Quervain, D.; Kolassa, I.-T. The role of FKBP5 genotype in moderating long-term effectiveness of exposure-based psychotherapy for posttraumatic stress disorder. Transl. Psychiatry 2014, 4, e403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dammann, G.; Teschler, S.; Haag, T.; Altmüller, F.; Tuczek, F.; Dammann, R.H. Increased DNA methylation of neuropsychiatric genes occurs in borderline personality disorder. Epigenetics 2011, 6, 1454–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.; Zheng, G.; Wiley, J.W. Epigenetic regulation of genes that modulate chronic stress-induced visceral pain in the peripheral nervous system. Gastroenterology 2015, 148, 148–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unternaehrer, E.; Luers, P.; Mill, J.; Dempster, E.; Meyer, A.H.; Staehli, S.; Lieb, R.; Hellhammer, D.H.; Meinlschmidt, G. Dynamic changes in DNA methylation of stress-associated genes (OXTR, BDNF) after acute psychosocial stress. Transl. Psychiatry 2012, 2, e150. [Google Scholar] [CrossRef] [Green Version]
- Holmes, A.; Yang, R.J.; Lesch, K.-P.; Crawley, J.N.; Murphy, D.L. Mice lacking the serotonin transporter exhibit 5-HT1A receptor-mediated abnormalities in tests for anxiety-like behavior. Neuropsychopharmacology 2003, 28, 2077–2088. [Google Scholar] [CrossRef] [Green Version]
- Klenova, E.; Scott, A.C.; Roberts, J.; Shamsuddin, S.; Lovejoy, E.A.; Bergmann, S.; Bubb, V.J.; Royer, H.-D.; Quinn, J.P. YB-1 and CTCF differentially regulate the 5-HTT polymorphic intron 2 enhancer which predisposes to a variety of neurological disorders. J. Neurosci. 2004, 24, 5966–5973. [Google Scholar] [CrossRef] [Green Version]
- Mustafa, M.; Lee, J.-Y.; Kim, M.H. CTCF negatively regulates HOXA10 expression in breast cancer cells. Biochem. Biophys. Res. Commun. 2015, 467, 828–834. [Google Scholar] [CrossRef]
- Maud, C.; Ryan, J.; McIntosh, J.E.; Olsson, C.A. The role of oxytocin receptor gene (OXTR) DNA methylation (DNAm) in human social and emotional functioning: A systematic narrative review. BMC Psychiatry 2018, 18, 154. [Google Scholar] [CrossRef]
- Li, D.; San, M.; Zhang, J.; Yang, A.; Xie, W.; Chen, Y.; Lu, X.; Zhang, Y.; Zhao, M.; Feng, X.; et al. Oxytocin receptor induces mammary tumorigenesis through prolactin/p-STAT5 pathway. Cell Death Dis. 2021, 12, 588. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Muttenthaler, M. High Oxytocin Receptor Expression Linked to Increased Cell Migration and Reduced Survival in Patients with Triple-Negative Breast Cancer. Biomedicines 2022, 10, 1595. [Google Scholar] [CrossRef] [PubMed]
- Mifsud, K.R.; Saunderson, E.A.; Spiers, H.; Carter, S.D.; Trollope, A.F.; Mill, J.; Reul, J.M. Rapid down-regulation of glucocorticoid receptor gene expression in the dentate gyrus after acute stress in vivo: Role of DNA methylation and microRNA activity. Neuroendocrinology 2017, 104, 157–169. [Google Scholar] [CrossRef]
- Man, X.; Li, Q.; Wang, B.; Zhang, H.; Zhang, S.; Li, Z. DNMT3A and DNMT3B in Breast Tumorigenesis and Potential Therapy. Front. Cell Dev. Biol. 2022, 10, 916725. [Google Scholar] [CrossRef] [PubMed]
- Pang, Y.; Liu, J.; Li, X.; Xiao, G.; Wang, H.; Yang, G.; Li, Y.; Tang, S.C.; Qin, S.; Du, N.; et al. MYC and DNMT 3A-mediated DNA methylation represses micro RNA-200b in triple negative breast cancer. J. Cell. Mol. Med. 2018, 22, 6262–6274. [Google Scholar] [CrossRef] [Green Version]
- Roll, J.D.; Rivenbark, A.G.; Jones, W.D.; Coleman, W.B. DNMT3b overexpression contributes to a hypermethylator phenotype in human breast cancer cell lines. Mol. Cancer 2008, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.G.; Gao, M.-Q.; Kang, S.; Choi, Y.P.; Lee, J.H.; Kim, J.E.; Han, H.H.; Mun, S.G.; Cho, N.H. Mechanical compression induces VEGFA overexpression in breast cancer via DNMT3A-dependent miR-9 downregulation. Cell Death Dis. 2017, 8, e2646. [Google Scholar] [CrossRef] [Green Version]
- Cha, N.; Jia, B.; He, Y.; Luan, W.; Bao, W.; Han, X.; Gao, W.; Gao, Y. MicroRNA-124 suppresses the invasion and proliferation of breast cancer cells by targeting TFAP4. Oncol. Lett. 2021, 21, 271. [Google Scholar] [CrossRef]
- Shi, P.; Chen, C.; Li, X.; Wei, Z.; Liu, Z.; Liu, Y. MicroRNA-124 suppresses cell proliferation and invasion of triple negative breast cancer cells by targeting STAT3. Mol. Med. Rep. 2019, 19, 3667–3675. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.-L.; Chao, C.C. Linking the immunophilin FKBP5 to taxol resistance in ovarian cancer. Cancer Cell Microenviron. 2015, 2, e692. [Google Scholar] [CrossRef]
- Li, L.; Lou, Z.; Wang, L. The role of FKBP5 in cancer aetiology and chemoresistance. Br. J. Cancer 2011, 104, 19–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, N.-K.; Huang, S.-L.; Chang, P.-Y.; Lu, H.-P.; Chao, C.C.-K. Transcriptomic profiling of taxol-resistant ovarian cancer cells identifies FKBP5 and the androgen receptor as critical markers of chemotherapeutic response. Oncotarget 2014, 5, 11939. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Zhang, Q.-X.; Pei, D.-S.; Xu, F.; Li, Y.; Yu, R.-T. FK506-binding protein 5 inhibits proliferation and stimulates apoptosis of glioma cells. Arch. Med. Sci. 2015, 11, 1074–1080. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Patients (n) |
|---|---|
| Age | |
| Less Than 35 | 5 |
| 35–45 | 10 |
| 45–55 | 12 |
| Above 55 | 5 |
| Family History | |
| Present | 8 |
| Not present | 24 |
| Mastectomy | |
| Yes | 21 |
| No | 11 |
| Tumor Grade | |
| II | 20 |
| III | 12 |
| Metastasis | |
| Yes | 18 |
| No | 14 |
| ER status | |
| Positive | 13 |
| Negative | 15 |
| Unknown | 4 |
| PR status | |
| Positive | 11 |
| Negative | 21 |
| HER2 neu status | |
| Positive | 12 |
| Negative | 20 |
| Gene | Forward Primer | Reverse Primer | Product Size |
|---|---|---|---|
| NR3C1 | 5′GCTGGAATGAACCTGGAAG3′ | 5′ACAGTGACACCAGGGTAGGG3′ | 157 bp |
| FKBP5 | 5′ACTGTTGCTGAGCAGGGA3′ | 5′CCATGCCTTGATGACTTGGC3′ | 221 bp |
| 5-HTT | 5′ATCATCCTTTCTGTCCTGCTGG3′ | 5′CCGGACCAAGAGAGAAGAAGAT3′ | 151 bp |
| OXTR | 5′ CCTTCATCGTGTGCTGGAC 3′ | 5′ CGAGTTCGTGGAAGAGGTG3′ | 174 bp |
| ACTIN | 5′ CCATGTACGTTGCTATCCAG 3′ | 5′ CCATCTCTTGCTCGAAGTC3′ | 295 bp |
| Variables (n) | Mean Scores | p-Value |
|---|---|---|
| Age | ||
| <35 (n = 5) | 3.30 ± 0.20 a,b | 0.0365 * |
| 35–45 (n = 10) | 3.59 ± 0.37 a | |
| 45–55 (n = 12) | 3.15 ± 0.34 b | |
| >55 (n = 5) | 3.17 ± 0.31 b | |
| Mastectomy | ||
| Yes (n = 21) | 3.45 ± 0.35 a | 0.03 * |
| No (n = 11) | 3.05 ± 0.38 b | |
| Illness duration | ||
| <6 months (n = 9) | 3.58 ± 0.29 a | 0.0011 ** |
| 6 months–2 years (n = 6) | 3.18 ± 0.14 b,c | |
| 2 years–3.5 years (n = 9) | 3.41 ± 0.42 a,b | |
| >3.5 years (n = 8) | 2.98 ± 0.19 c | |
| Metastasis | ||
| Yes (n = 18) | 3.38 ± 0.36 | 0.14 NS |
| No (n = 14) | 3.22 ± 0.41 |
| Gene Name | AFFY METRIX ID | OS p | HR | RFS p | HR | DFMS p | HR | PPS p | HR |
|---|---|---|---|---|---|---|---|---|---|
| NR3C1 | 201865_x_at | 0.0003 * | 0.72 | 4.2 × 10−9 * | 0.74 | 0.4 | 0.92 | 0.13 | 0.8 |
| 5-HTT | 207519_at | 0.03 * | 0.82 | 4.3 × 10−14 * | 0.6 | 0.1 | 0.85 | 0.0011 * | 0.72 |
| OXTR | 206825_at | 0.09 | 0.85 | 0.0009 * | 0.84 | 0.5 | 0.91 | 0.6 | 0.9 |
| FKBP5 | 204560_at | 0.01 * | 0.78 | 0.32 | 1.06 | 5.9 × 10−6 * | 0.78 | 0.4 | 0.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiaz, T.; Nadeem, M.S.; Afzal, O.; Altamimi, A.S.A.; Alzarea, S.I.; Almalki, W.H.; Khan, H.A.; Iahtisham-Ul-Haq; Hanook, S.; Kazmi, I.; et al. Peripheral mRNA Expression and Prognostic Significance of Emotional Stress Biomarkers in Metastatic Breast Cancer Patients. Int. J. Mol. Sci. 2022, 23, 14097. https://doi.org/10.3390/ijms232214097
Fiaz T, Nadeem MS, Afzal O, Altamimi ASA, Alzarea SI, Almalki WH, Khan HA, Iahtisham-Ul-Haq, Hanook S, Kazmi I, et al. Peripheral mRNA Expression and Prognostic Significance of Emotional Stress Biomarkers in Metastatic Breast Cancer Patients. International Journal of Molecular Sciences. 2022; 23(22):14097. https://doi.org/10.3390/ijms232214097
Chicago/Turabian StyleFiaz, Tahreem, Muhammad Shahid Nadeem, Obaid Afzal, Abdulmalik S. A. Altamimi, Sami I. Alzarea, Waleed Hassan Almalki, Hafsa Ahmed Khan, Iahtisham-Ul-Haq, Sharoon Hanook, Imran Kazmi, and et al. 2022. "Peripheral mRNA Expression and Prognostic Significance of Emotional Stress Biomarkers in Metastatic Breast Cancer Patients" International Journal of Molecular Sciences 23, no. 22: 14097. https://doi.org/10.3390/ijms232214097