
A Comparative Study on the Effect of Acute Pharyngeal Stimulation with TRP Agonists on the Biomechanics and Neurophysiology of Swallow Response in Patients with Oropharyngeal Dysphagia


Abstract
:1. Introduction
2. Results
2.1. Demographics and Clinical Data
2.2. The Effect on Prevalence of VFS Signs
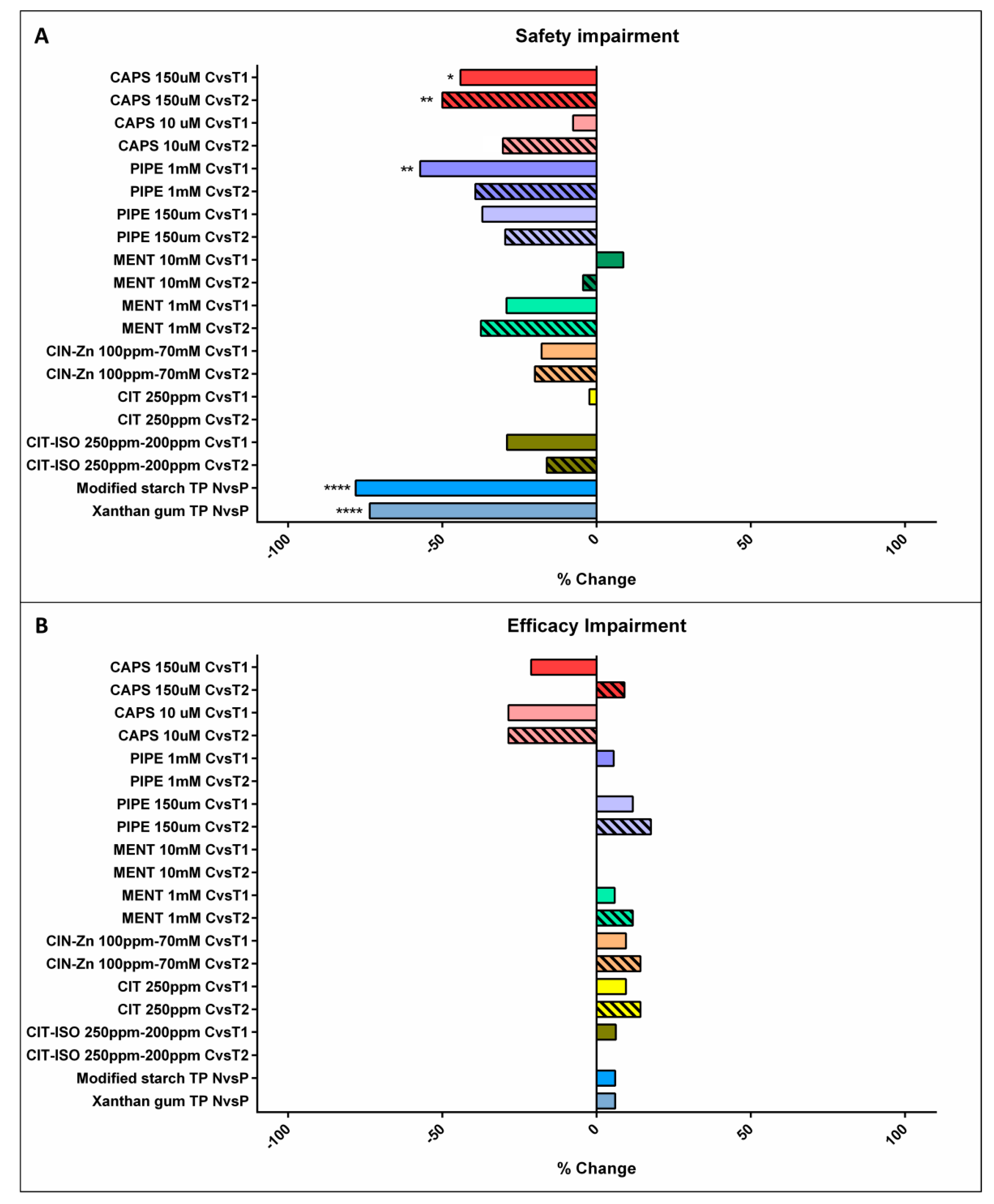
2.2.1. VFS Signs of Impaired Safety of Swallow
Effect of Increasing Viscosity
Effect of TRP Agonists
2.2.2. Efficacy Impairments
2.3. The Effects on the Biomechanics of the Swallow Response
2.3.1. The Effect on the Timing of OSR
Effect of Increasing Viscosity
TRP Agonists
2.3.2. The Effects on Bolus Velocity
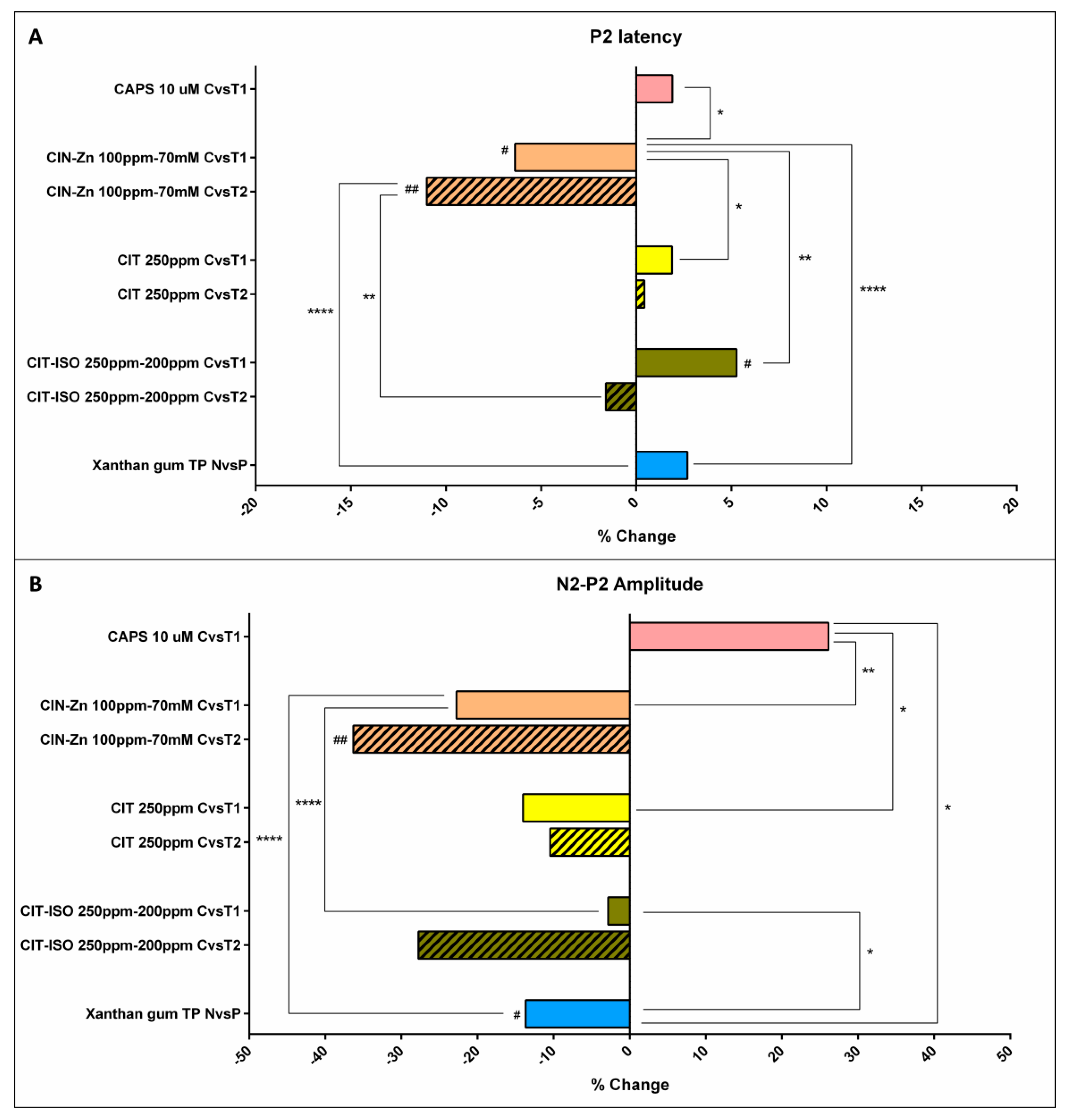
2.4. The Effects on Neurophysiology
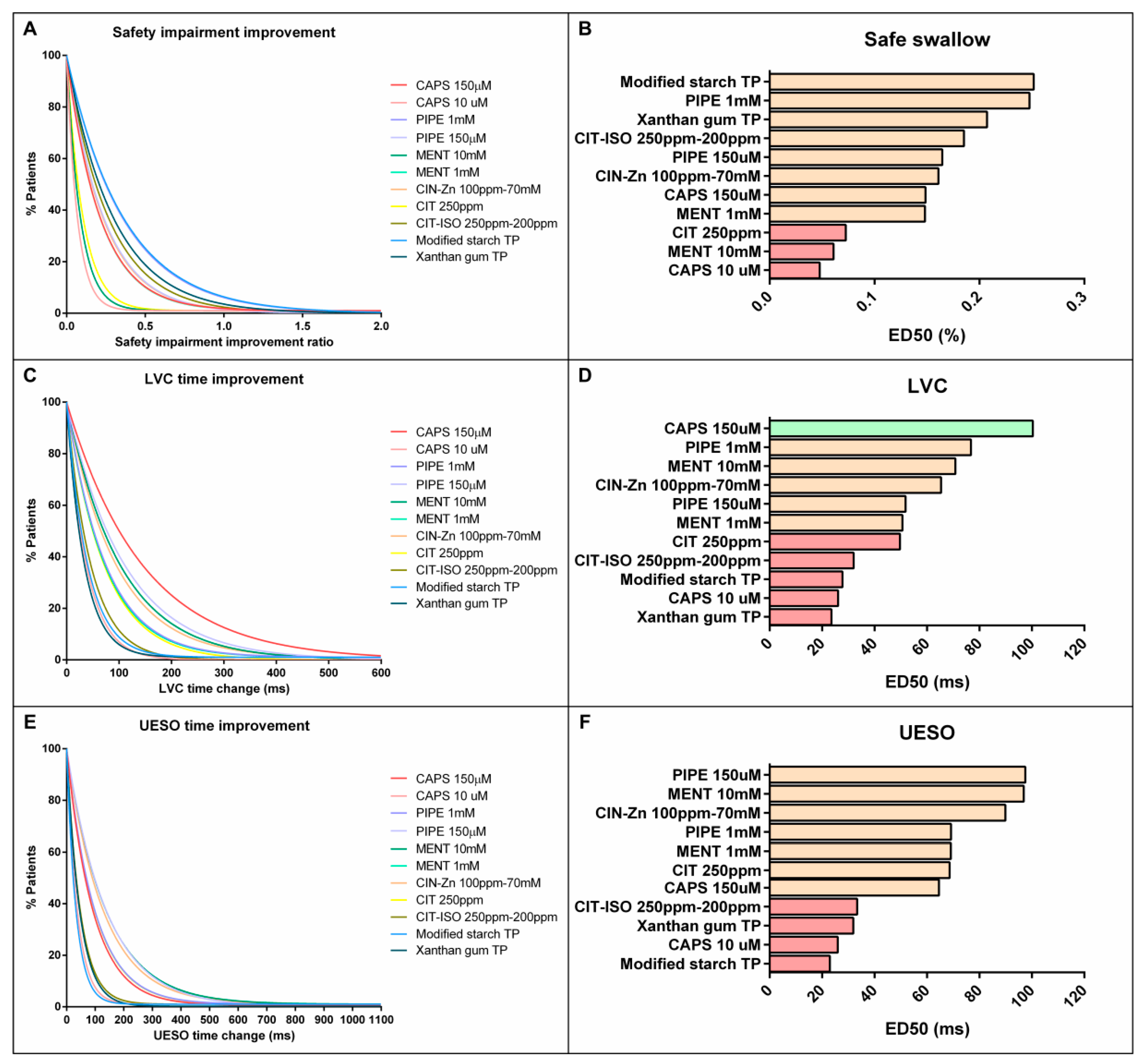
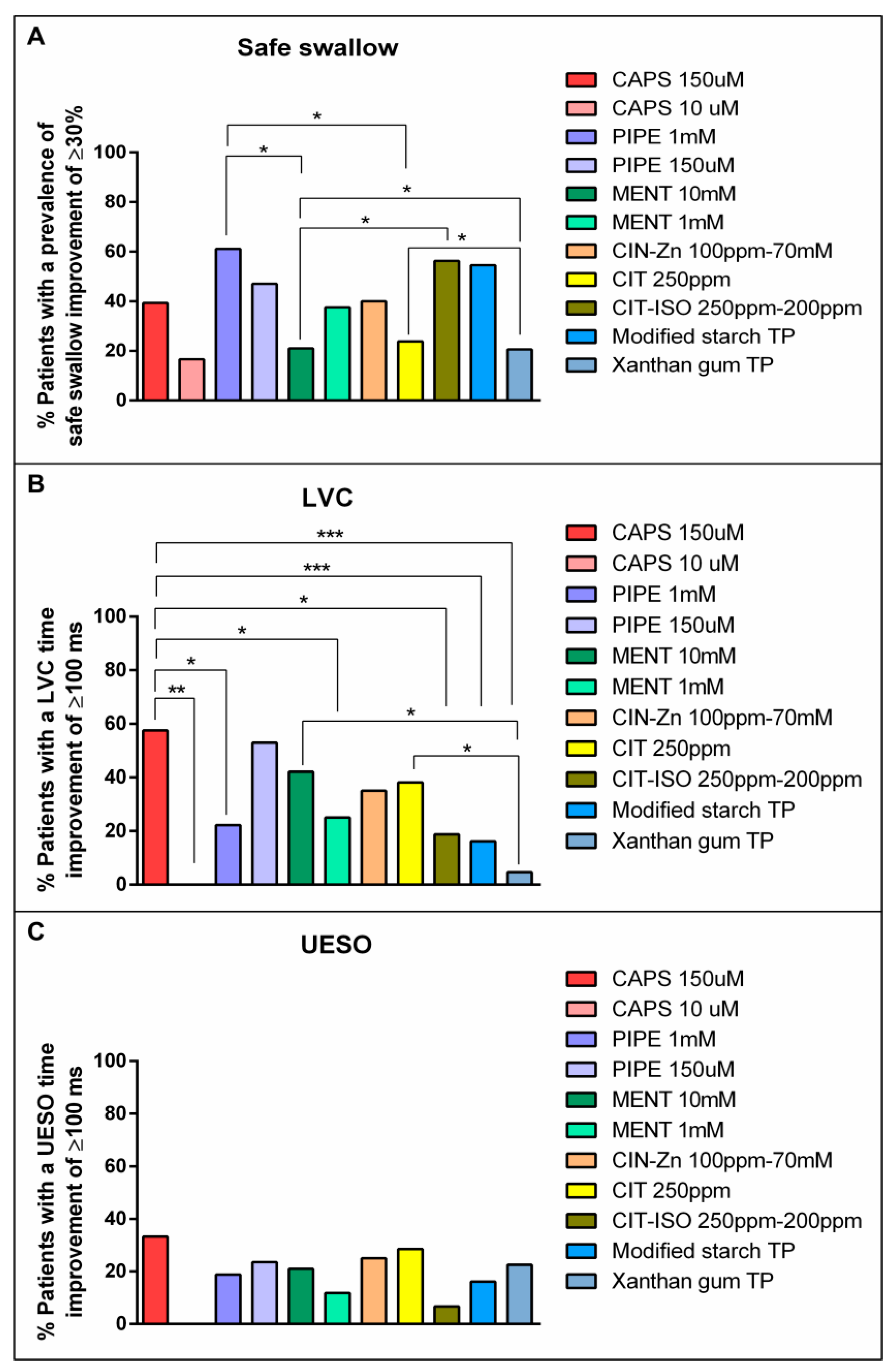
2.5. Comparison on the Effectiveness of Pharmacological Treatment
2.5.1. Effect on VFS Signs of Safety and Biomechanics of Swallow Response
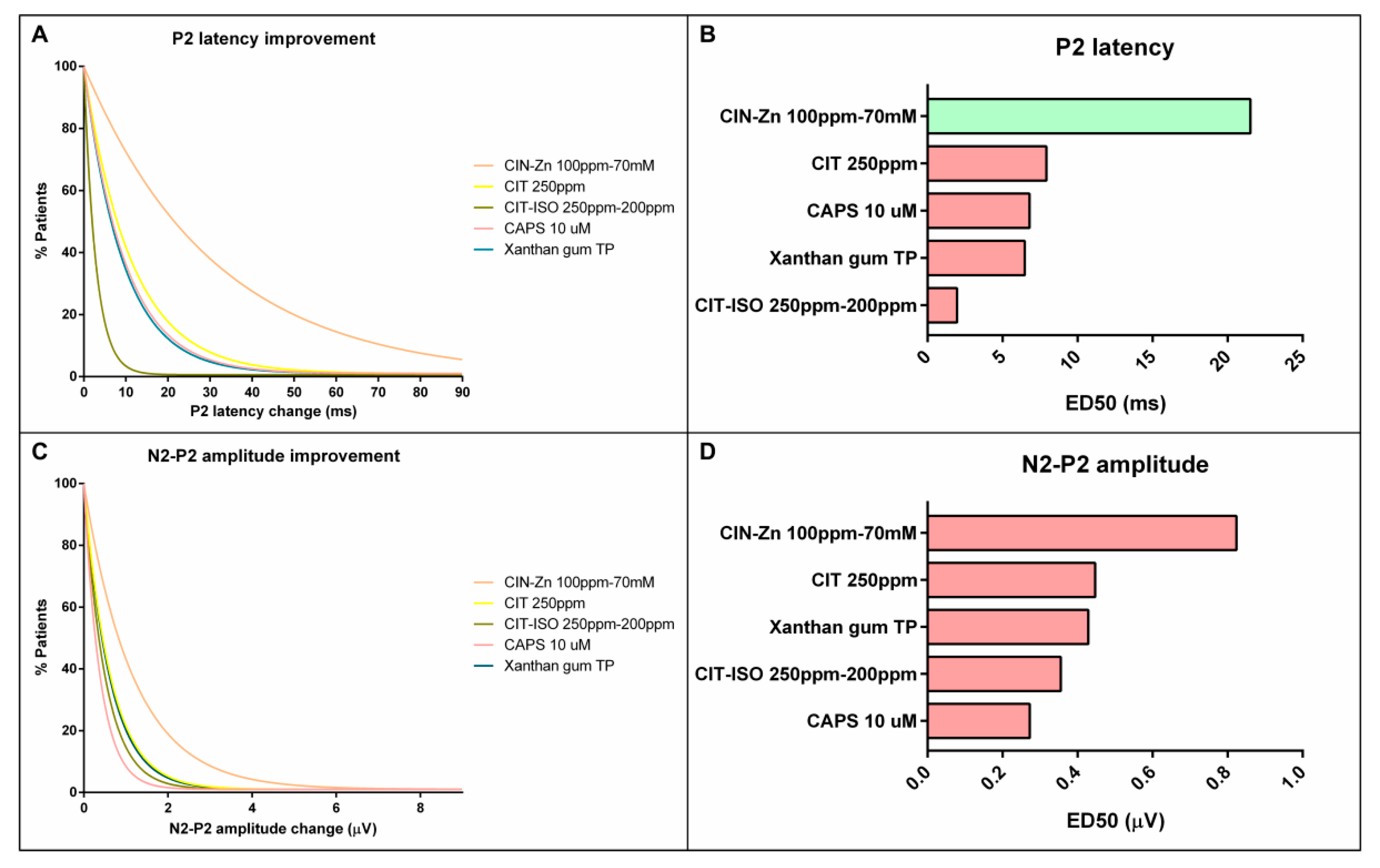
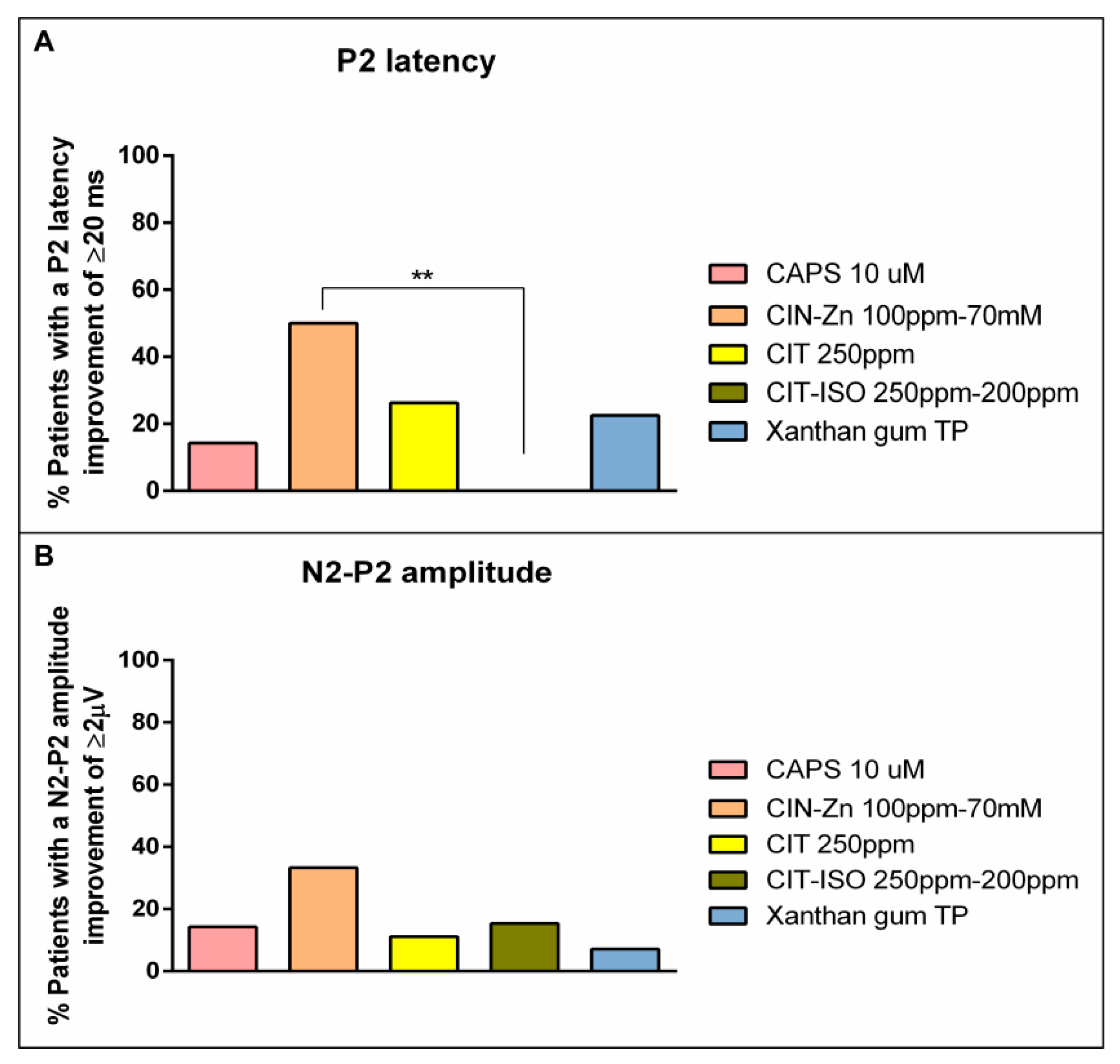
2.5.2. Effect on Neurophysiology
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Biomechanical Assessment
4.2.1. VFS Procedure
4.2.2. Experimental Design for VFS Studies
- (a)
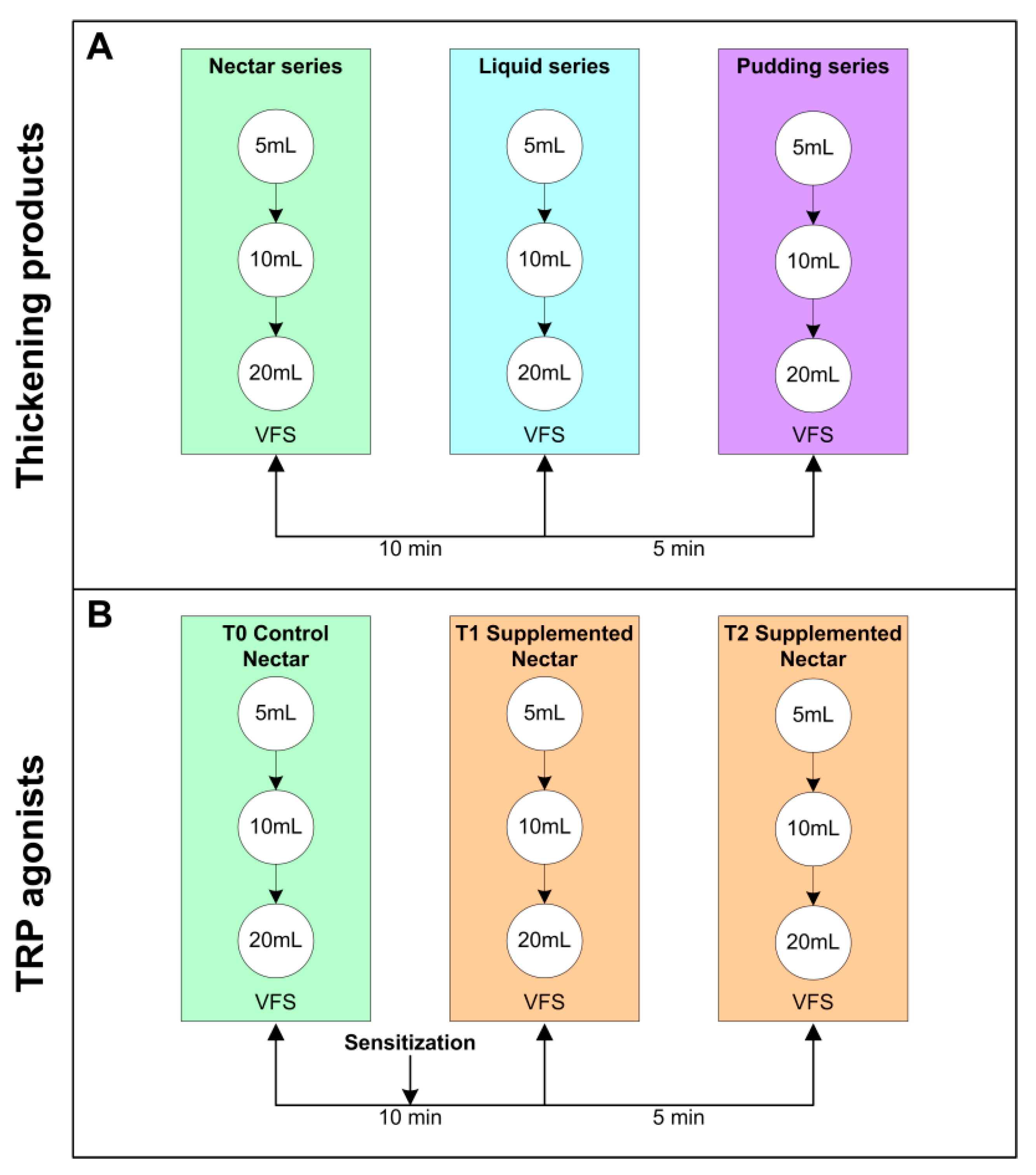
- Effect of increasing shear viscosity while swallowing 5, 10 and 20 mL of liquid, nectar (238–295 mPa·s) or pudding (1840–3682 mPa·s) viscosity series. Nectar viscosities were obtained by adding 4.5 g (295 mPa·s) of Resource ThickenUp (TU) or 1.2 g (238 mPa·s) of Resource ThickenUp Clear (TUC) to 100 mL of water. Pudding viscosities were obtained by adding 9 g (3682 mPa·s) of TU or 6 g (1840 mPa·s) of TUC to 100 mL of liquid. The liquid used was a 1:1 mixture of water and hydrosoluble radiopaque contrast (Gastrografin—Bayer Hispania SL, Barcelona, Spain for the MS thickener—or Omnipaque—GE Healthcare, Chicago, Illinois, USA- for XG). The protocol has been previously described [23,28] (Figure 8a).
- (b)
- Effect of TRP agonists. In the acute stimulation with TRP agonists protocol, VFS consisted of a first control series (T0) of 5, 10 and 20 mL of “nectar” (238 mPas·s) boluses without supplementation followed by two 5, 10 and 20 mL nectar series (T1 and T2) supplemented with a TRP agonist. Between T0 and T1, there was a sensitization period that consisted of two 5 mL nectar boluses containing the same agonist (Figure 8b). The TRP agonists studied were: capsaicinoids (TRPV1 agonist) at 150 µM [23] and 10 µM [26], piperine (TRPV1/A1 agonist) at 1 mM and 150 µM [24], menthol (TRPM8 agonist) at 10 mM and 1 mM [25], cinnamaldehyde-zinc (CIN-Zn) at 100 ppm–70 mM (TRPA1 agonists), citral (CIT) at 250 ppm (TRPA1 agonist), and citral-isopulegol (CIT-ISO) at 250 ppm–200 ppm (TRPA1-TRPM8 agonists) [27] (Table 4).
4.3. Neurophysiological Assessment
4.3.1. pSEPs Procedure
4.3.2. Experimental Design for pSEPs
- (a)
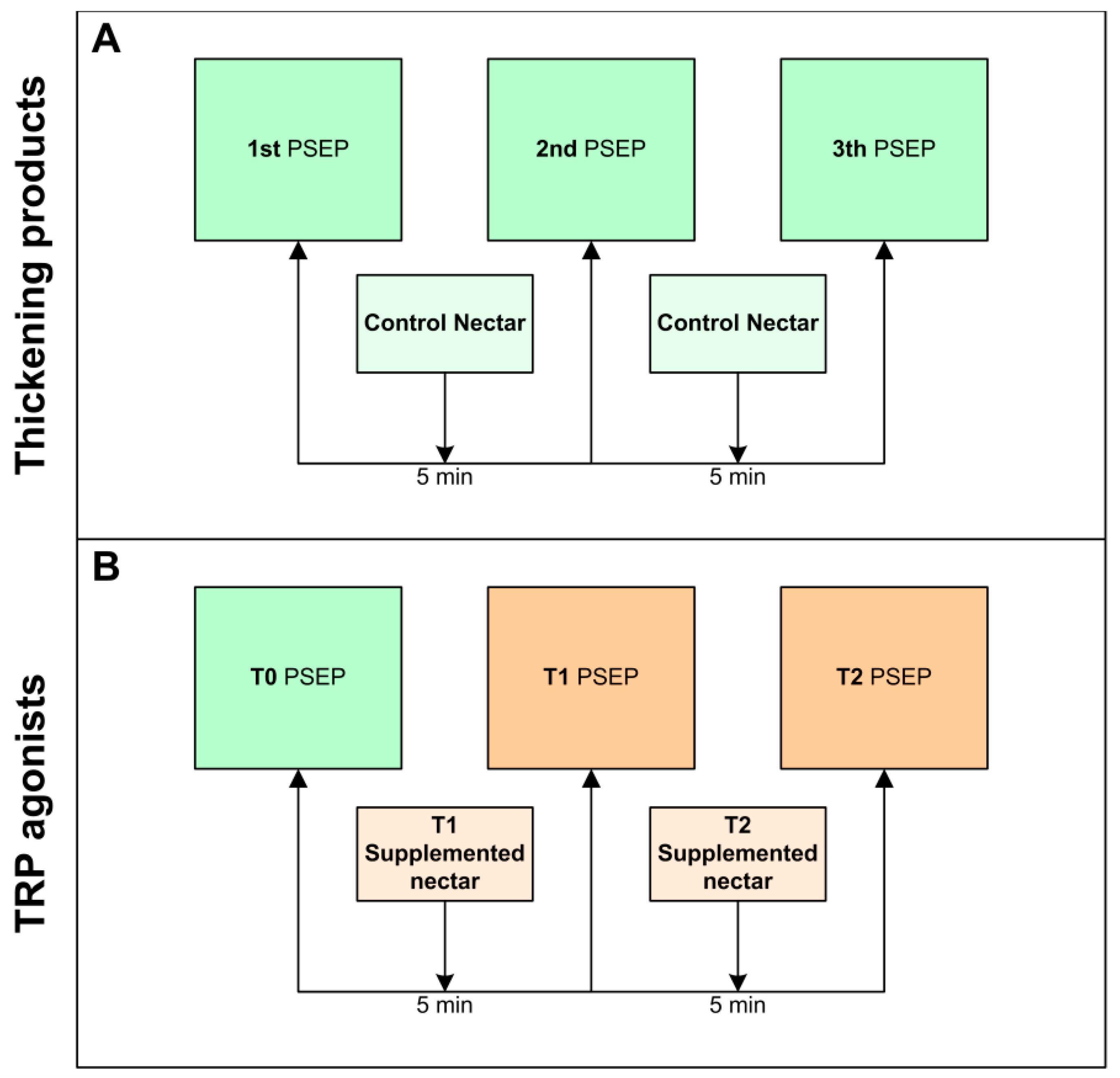
- Effect of thickeners on the neurophysiology of swallowing. A total of 3 sets of stimuli were recorded: T0 (control), T1 (first time point post-stimulation) and T2 (second time point post-stimulation). Each set was characterized by having a duration of 4:15 min in which the patient received an electrical stimulus every 5 s. There was a rest interval of 1 min between the stimulation sets, during which a single bolus of 35 mL of nectar (238 mPa·s) was taken (Figure 9a). Only the effect of XG-TP was studied as a control [27].
- (b)
- Effect of acute stimulation with TRP agonists on the neurophysiology of swallow. The same protocol as described above was followed at T0 but with the difference that the nectar bolus taken between stimulation sets was supplemented with TRP agonists at T1 and T2. In this case, T0 was the basal situation, and T1 and T2 were used to determine the effect of TRP stimulation (Figure 9b). To avoid the effect of multiple administrations, a period of 5 days was left between the VFS and the pSEPs recording. TRP agonists studied were: capsaicinoids (TRPV1 agonist) at 10 µM [26], CIN-Zn at 100 ppm–70 mM (TRPA1 agonists), CIT at 250 ppm (TRPA1 agonist), and CIT-ISO at 250 ppm–200 ppm (TRPA1-TRPM8 agonists) [27] (Table 4).
4.4. Data Analysis
- Intragroup differences (effect of TRP stimulants and fluid thickening, each person acting as his own control). (a) VFS signs: the differences within the same treatment group on VFS signs of safety or efficacy of swallow were analyzed by comparing the prevalence of unsafe swallows (number of unsafe swallows/total number of swallows) or efficacy impairment signs (number of ineffective swallows/total number of swallows) of nectar series (5, 10, and 20 mL) with that of pudding for the groups treated with the thickeners, and the control nectar series T0 with T1 or T2 for the groups treated with a TRP agonist; (b) Biomechanics: the effect of increasing viscosity or TRP stimulation on the biomechanics of swallow response was assessed by comparing the time to LVC (ms) and UESO (ms) while swallowing 5 mL nectar vs. 5 mL pudding (increasing viscosity effect) and while swallowing 5 mL of control nectar (T0) vs. 5 mL nectar supplemented with a TPR agonist (T1 and T2); (c) Neurophysiology: the effect of TP and TRP stimulation on the neurophysiology of swallowing was assessed by comparing the P2 peak latency and N2-P2 amplitude of pSEPs between the control recording set (T0) vs. the first (T1) or second (T2) post-stimulation sets.
- Intergroup differences (comparison of the therapeutic effect between all treatments, including TRP stimulation vs. fluid thickening) were assessed as follows: (a) Therapeutic effect of TP: percentage change of pudding minus nectar for each VFS sign, biomechanical and neurophysiological parameter; (b) Therapeutic effect of TRP agonists between each other: percentage change for each VFS sign, or biomechanical and neurophysiological parameter between T0 and T1 or T2; (c) Therapeutic effect of TRP agonists with TP: percentage change for each VFS sign, or biomechanical and neurophysiological parameter between T0 and T1 or T2 vs. percentage of change between nectar and pudding.
- Pharmacodynamic effect. To normalize and facilitate the comparisons on the potency of the therapeutic effect of each compound (both TP and TRP), the acute pharmacodynamic effect of the TRP agonists and thickeners on the prevalence of safety impairments and the time to LVC and to UESO were analyzed using a one-phase decay curve (ref). These curves were constructed for each agonist and thickener with the proportion of patients whose prevalence of safety impairments improved by at least 30% and time to LVC and UESO improved at least 100 ms with the model Y = [Y0-Plateau]·e(−K·X)+Plateau. The same curve model was obtained for P2 latency (minimum shortening of 20 ms) and N2-P2 amplitude (increased by at least 2 µV) in order to know the effect on the neurophysiological response. In addition, we compared the proportion of patients in whom these variables improved. The curves enabled the results to be differentiated into three groups according to their pharmacological effect, taking into account the ED50 value: high, intermediate and low therapeutic effect (Table 5).
4.5. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clavé, P.; Shaker, R. Dysphagia: Current reality and scope of the problem. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Baijens, L.W.J.; Clavé, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.-C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European society for swallowing disorders—European union geriatric medicine society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403. [Google Scholar] [CrossRef] [PubMed]
- Newman, R.; Vilardell, N.; Clavé, P.; Speyer, R. Effect of Bolus Viscosity on the Safety and Efficacy of Swallowing and the Kinematics of the Swallow Response in Patients with Oropharyngeal Dysphagia: White Paper by the European Society for Swallowing Disorders (ESSD). Dysphagia 2016, 31, 719. [Google Scholar] [CrossRef] [PubMed]
- Bolivar-Prados, M.; Rofes, L.; Arreola, V.; Guida, S.; Nascimento, W.; Martín, A.; Vilardell, N.; Ortega, O.; Ripken, D.; Lansik, M.; et al. Effect of a gum-based thickener on the safety of swallowing in patients with post-stroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2019, 31, e13695. [Google Scholar] [CrossRef] [PubMed]
- Ortega, O.; Bolívar-Prados, M.; Arreola, V.; Nascimento, W.; Tomsen, N.; Gallegos, C.; Brito-de La Fuente, E.; Clavé, P. Therapeutic Effect, Rheological Properties and Xanthan Gum Thickener on Four Different. Nutrients 2020, 12, 1873. [Google Scholar] [CrossRef]
- Rosenvinge, S.K.; Starke, I.D. Improving care for patients with dysphagia. Age Ageing 2005, 34, 587–593. [Google Scholar] [CrossRef]
- Shim, J.S.; Oh, B.M.; Han, T.R. Factors Associated With Compliance With Viscosity-Modified Diet Among Dysphagic Patients. Ann. Rehabil. Med. 2013, 37, 628–632. [Google Scholar] [CrossRef]
- Loeb, M.B.; Becker, M.; Eady, A.; Walker-Dilks, C. Interventions to Prevent Aspiration Pneumonia in Older Adults: A Systematic Review. J. Am. Geriatr. Soc. 2003, 51, 1018–1022. [Google Scholar] [CrossRef]
- El Solh, A.A.; Saliba, R. Pharmacologic prevention of aspiration pneumonia: A systematic review. Am. J. Geriatr. Pharmacother. 2007, 5, 352–362. [Google Scholar] [CrossRef]
- Cheng, I.; Sasegbon, A.; Hamdy, S. Effects of pharmacological agents for neurogenic oropharyngeal dysphagia: A systematic review and meta-analysis. Neurogastroenterol. Motil. 2022, 34, e14220. [Google Scholar] [CrossRef]
- Rofes, L.; Arreola, V.; Romea, M.; Palomeras, E.; Almirall, J.; Cabré, M.; Serra-Prat, M.; Clavé, P.; Palomera, E.; Almirall, J.; et al. Pathophysiology of oropharyngeal dysphagia in the frail elderly. Neurogastroenterol. Motil. 2010, 22, 851.e230. [Google Scholar] [CrossRef] [PubMed]
- Rofes, L.; Ortega, O.; Vilardell, N.; Mundet, L.; Clavé, P. Spatiotemporal characteristics of the pharyngeal event-related potential in healthy subjects and older patients with oropharyngeal dysfunction. Neurogastroenterol. Motil. 2017, 29, 1–11. [Google Scholar] [CrossRef]
- Cabib, C.; Ortega, O.; Vilardell, N.; Mundet, L.; Clavé, P.; Rofes, L. Chronic post-stroke oropharyngeal dysphagia is associated with impaired cortical activation to pharyngeal sensory inputs. Eur. J. Neurol. 2017, 24, 1355–1362. [Google Scholar] [CrossRef] [PubMed]
- Cabib, C.; Nascimento, W.; Rofes, L.; Arreola, V.; Tomsen, N.; Mundet, L.; Muriana, D.; Palomeras, E.; Michou, E.; Clavé, P.; et al. Neurophysiological and Biomechanical Evaluation of the Mechanisms Which Impair Safety of Swallow in Chronic Post-stroke Patients. Transl. Stroke Res. 2019, 11, 16–28. [Google Scholar] [CrossRef]
- Tomsen, N.; Ortega, O.; Nascimento, W.; Carrión, S.; Clavé, P. Oropharyngeal Dysphagia in Older People is Associated with Reduced Pharyngeal Sensitivity and Low Substance P and CGRP Concentration in Saliva. Dysphagia 2021, 37, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Vilardell, N.; Arreola, L.R.V.; Muriana, A.M.D.; Clavé, P. Videofluoroscopic assessment of the pathophysiology of chronic poststroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2017, 29, e13111. [Google Scholar] [CrossRef]
- Miarons, M.; Clavé, P.; Wijngaard, R.; Ortega, O.; Arreola, V.; Nascimento, W.; Rofes, L. Pathophysiology of Oropharyngeal Dysphagia Assessed by Videofluoroscopy in Patients with Dementia Taking Antipsychotics. J. Am. Med. Dir. Assoc. 2018, 19, 812.e1–812.e10. [Google Scholar] [CrossRef]
- Espinosa-Val, C.; Martín-Martínez, A.; Graupera, M.; Arias, O.; Elvira, A.; Cabré, M.; Palomera, E.; Bolívar-Prados, M.; Clavé, P.; Ortega, O. Prevalence, risk factors, and complications of oropharyngeal dysphagia in older patients with dementia. Nutrients 2020, 12, 863. [Google Scholar] [CrossRef]
- Caterina, M.J.; Schumacher, M.A.; Tominaga, M.; Rosen, T.A.; Levine, J.D.; Julius, D. The capsaicin receptor: A heat-activated ion channel in the pain pathway. Nature 1997, 389, 816–824. [Google Scholar] [CrossRef]
- Alvarez-Berdugo, D.; Rofes, L.; Farré, R.; Casamitjana, J.F.; Enrique, A.; Chamizo, J.; Padrón, A.; Navarro, X.; Clavé, P.; Farré, R.; et al. Localization and expression of TRPV1 and TRPA1 in the human oropharynx and larynx. Neurogastroenterol. Motil. 2016, 28, 91–100. [Google Scholar] [CrossRef]
- Alvarez-Berdugo, D.; Rofes, L.; Casamitjana, J.F.; Enrique, A.; Chamizo, J.; Viña, C.; Pollán, C.M.; Clavé, P. TRPM8, ASIC1, and ASIC3 localization and expression in the human oropharynx. Neurogastroenterol. Motil. 2018, 30, 5–7. [Google Scholar] [CrossRef]
- Meotti, F.C.; De Andrade, E.L.; Calixto, J.B. TRP modulation by natural compounds. Handb. Exp. Pharmacol. 2014, 223, 1177–1238. [Google Scholar] [CrossRef]
- Rofes, L.; Arreola, V.; Martin, A.; Clave, P. Natural capsaicinoids improve swallow response in older patients with oropharyngeal dysphagia. Gut 2013, 62, 1280–1287. [Google Scholar] [CrossRef]
- Rofes, L.; Arreola, V.; Martin, A.; Clavé, P. Effect of oral piperine on the swallow response of patients with oropharyngeal dysphagia. J. Gastroenterol. 2014, 49, 1517–1523. [Google Scholar] [CrossRef]
- Alvarez-Berdugo, D.; Rofes, L.; Arreola, V.; Martin, A.; Molina, L.; Clavé, P. A comparative study on the therapeutic effect of TRPV1, TRPA1, and TRPM8 agonists on swallowing dysfunction associated with aging and neurological diseases. Neurogastroenterol. Motil. 2017, 30, 1–9. [Google Scholar] [CrossRef]
- Tomsen, N.; Ortega, O.; Rofes, L.; Arreola, V.; Martin, A.; Mundet, L.; Clavé, P. Acute and subacute effects of oropharyngeal sensory stimulation with TRPV1 agonists in older patients with oropharyngeal dysphagia: A biomechanical and neurophysiological randomized pilot study. Therap. Adv. Gastroenterol. 2019, 12, 1–13. [Google Scholar] [CrossRef]
- Tomsen, N.; Alvarez-Berdugo, D.; Rofes, L.; Ortega, O.; Arreola, V.; Nascimento, W.; Martin, A.; Cabib, C.; Bolivar-Prados, M.; Mundet, L.; et al. A randomized clinical trial on the acute therapeutic effect of TRPA1 and TRPM8 agonists in patients with oropharyngeal dysphagia. Neurogastroenterol. Motil. 2020, 32, e13821. [Google Scholar] [CrossRef]
- Rofes, L.; Arreola, V.; Mukherjee, R.; Swanson, J.; Clavé, P. The effects of a xanthan gum-based thickener on the swallowing function of patients with dysphagia. Aliment. Pharmacol. Ther. 2014, 39, 1169–1179. [Google Scholar] [CrossRef]
- Vilardell, N.; Rofes, L.; Arreola, V.; Speyer, R.; Clavé, P. A Comparative Study Between Modified Starch and Xanthan Gum Thickeners in Post-Stroke Oropharyngeal Dysphagia. Dysphagia 2016, 31, 169–179. [Google Scholar] [CrossRef]
- Bolivar-Prados, M.; Tomsen, N.; Arenas, C.; Ibáñez, L.; Clave, P. A bit thick: Hidden risks in thickening products’ labelling for dysphagia treatment. Food Hydrocoll. 2021, 123, 106960. [Google Scholar] [CrossRef]
- Matta, Z.; Chambers, E.; Mertz-Garcia, J.; McGowan-Helverson, J.M. Sensory characteristics of beverages prepared with commercial thickeners used for dysphagia diets. J. Am. Diet. Assoc. 2006, 106, 1049–1054. [Google Scholar] [CrossRef] [PubMed]
- Nakato, R.; Manabe, N.; Shimizu, S.; Hanayama, K.; Shiotani, A.; Hata, J.; Haruma, K. Effects of Capsaicin on Older Patients with Oropharyngeal Dysphagia: A Double-Blind, Placebo-Controlled, Crossover Study. Digestion 2017, 95, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.Z.; Ando, H.; Unno, S.; Masuda, Y.; Kitagawa, J. Activation of TRPV1 and TRPM8 Channels in the Larynx and Associated Laryngopharyngeal Regions Facilitates the Swallowing Reflex. Int. J. Mol. Sci. 2018, 19, 4113. [Google Scholar] [CrossRef]
- Alvarez-Berdugo, D.; Jiménez, M.; Clavé, P.; Rofes, L. Pharmacodynamics of TRPV1 agonists in a bioassay using human PC-3 cells. Sci. World J. 2014, 2014, 184526. [Google Scholar] [CrossRef] [PubMed]
- Zanotto, K.L.; Iodi Carstens, M.; Carstens, E. Cross-desensitization of responses of rat trigeminal subnucleus caudalis neurons to cinnamaldehyde and menthol. Neurosci. Lett. 2008, 430, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Cabib, C.; Nascimento, W.; Rofes, L.; Arreola, V.; Tomsen, N.; Mundet, L.; Palomeras, E.; Michou, E.; Clavé, P.; Ortega, O. Short-term neurophysiological effects of sensory pathway neurorehabilitation strategies on chronic poststroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2020, 32, 1–14. [Google Scholar] [CrossRef]
- Clavé, P.; De Kraa, M.; Arreola, V.; Girvent, M.; Farré, R.; Palomera, E.; Serra-Prat, M. The effect of bolus viscosity on swallowing function in neurogenic dysphagia. Aliment. Pharmacol. Ther. 2006, 24, 1385–1394. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | CAPS 150 µM | CAPS 10 µM | PIPE 1 MM | PIPE 150 µM | MENT 10 mM | MENT 1 mM | CIN-ZN | CIT | CIT-ISO | MS-TP | XG-TP | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 329 | 33 | 7 | 20 | 20 | 20 | 20 | 21 | 21 | 16 | 33 | 118 | |
| Age (years) | 78.2 ± 6.5 | 75.9 ± 1.9 | 83.5 ± 6.3 | 75.1 ± 3.3 | 76.6 ± 2.4 | 78.2 ± 8.2 | 77.6 ± 8.4 | 81.6 ± 7.6 | 78.0 ± 7.5 | 79.8 ± 7.9 | 73.9 ± 2.2 | 74.4 ± 12.4 | >0.999 |
| Sex (% men) | 47.8 | 60.6 | 57.1 | 40 | 45 | 40 | 55 | 38.1 | 42.9 | 56.4 | 48.5 | 54.2 | 0.708 |
| Barthel Index | 71.9 ± 26.4 | n/a | 70 ± 33.7 | 74.2 ± 7.9 | 78.0 ± 6.9 | 75 ± 33.9 | 80.3 ± 28.5 | 75.8 ± 33.8 | 58.5 ± 30.7 | 63.2 ± 35.6 | n/a | n/a | 0.999 |
| MNA-sf | 11.6 ± 3.9 | n/a | 9.5 ± 2.9 | n/a | n/a | 18.0 ± 7.3 | 9.5 ± 2.63 | n/a | n/a | n/a | n/a | 9.7 ± 2.8 | 0.823 |
| OD Etiology (%) | |||||||||||||
| Aging | 41.6 | 30.3 | 57.1 | 60 | 55 | n/a | n/a | 62 | 57.1 | 50 | 30.3 | 34.17 | 0.035 |
| Stroke | 42.5 | 45.5 | 28.6 | 40 | 25 | n/a | n/a | 19.0 | 23.8 | 25 | 45.5 | 55 | 0.004 |
| ND | 15.8 | 24.3 | 14.3 | 0 | 20 | n/a | n/a | 19.0 | 19.0 | 25 | 24.2 | 10.83 | 0.018 |
| CAPS 150 µM | CAPS 10 µM | PIPE 1 mM | PIPE 150 µM | MENT 10 mM | MENT 1 mM | CIN-Zn | CIT | CIT-ISO | MS TP | XG TP | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Safe swallow | K | 4.73 | 14.75 | 2.80 | 4.21 | 11.53 | 4.74 | 4.34 | 9.68 | 3.74 | 2.75 | 3.34 |
| Tau | 0.21 | 0.07 | 0.36 | 0.24 | 0.09 | 0.21 | 0.23 | 0.10 | 0.27 | 0.36 | 0.30 | |
| R2 | 0.78 | 0.46 | 0.91 | 0.85 | 0.53 | 0.72 | 0.76 | 0.55 | 0.84 | 0.89 | 0.27 | |
| ED50 | 0.15 | 0.05 | 0.25 | 0.16 | 0.06 | 0.15 | 0.16 | 0.07 | 0.19 | 0.25 | 0.21 | |
| LVC | K | 0.01 | 0.03 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | 0.03 | 0.04 |
| Tau | 144.8 | 73.67 | 110.7 | 72.00 | 102.2 | 93.41 | 71.71 | 46.17 | 37.61 | 39.50 | 24.51 | |
| R2 | 0.98 | 0.88 | 0.91 | 0.96 | 0.96 | 0.80 | 0.95 | 0.85 | 0.92 | 0.17 | 0.84 | |
| ED50 | 100.4 | 26.07 | 76.73 | 51.83 | 70.83 | 50.63 | 65.37 | 49.72 | 32.00 | 27.78 | 23.58 | |
| UESO | K | 0.01 | 0.03 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.02 | 0.03 | 0.08 |
| Tau | 92.34 | 36.92 | 98.33 | 140.6 | 137.8 | 98.23 | 127.8 | 97.57 | 47.41 | 32.67 | 12.20 | |
| R2 | 0.89 | 0.35 | 0.54 | 0.85 | 0.74 | 0.43 | 0.68 | 0.39 | 0.34 | 0.12 | 0.73 | |
| ED50 | 64.58 | 25.96 | 69.15 | 97.48 | 96.89 | 69.09 | 89.89 | 68.61 | 33.35 | 22.98 | 31.88 |
| CAPS 10 µM | CIN-Zn | CIT | CIT-ISO | XG TP | ||
|---|---|---|---|---|---|---|
| P2 latency | K | 0.104 | 0.032 | 0.089 | 0.356 | 0.109 |
| Tau | 9.662 | 31.05 | 11.26 | 2.81 | 9.211 | |
| R2 | −0.062 | 0.893 | 0.356 | 0.764 | 0.062 | |
| ED50 | 6.79 | 21.52 | 7.92 | 1.96 | 6.48 | |
| N2-P2 amplitude | K | 2.582 | 0.8537 | 1.574 | 1.98 | 1.641 |
| Tau | 0.387 | 1.171 | 0.635 | 0.505 | 0.609 | |
| R2 | 0.467 | 0.710 | 0.679 | 0.801 | 0.856 | |
| ED50 | 0.27 | 0.82 | 0.45 | 0.36 | 0.43 |
| Study | Trial Registration Code | Thickening Product | TRP Receptor | Agonist (Concentration) | VFS | pSEP |
|---|---|---|---|---|---|---|
| Compensatory treatment | ||||||
| Rofes et al. 2013 [23] | ISRCTN31088564 | Modified starch | n/a | n/a | + | − |
| Rofes et al. 2014 [28] | NCT01158313 | Xanthan gum | n/a | n/a | + | − |
| Active treatment | ||||||
| Rofes et al. 2013 [23] | ISRCTN31088564 | Modified starch | TRPV1 | Capsaicinoids (150 µM) | + | − |
| Rofes et al. 2014 [24] | NCT01383694 | Modified starch | TRPV1/A1 | Piperine (1 mM and 150 µM) | + | − |
| Alvarez-Berdugo et al. 2017 [25] | NCT03050957 | Modified starch | TRM8 | Methol (10 mM and 1 mM) | + | − |
| Tomsen et al. 2019 [26] | NCT01762228 | Modified starch | TRPV1 | Capsaicinoids (10 µM) | + | + |
| Tomsen et al. 2020 [27] | NCT02422576 | Xanthan Gum | TRPA1 | Cinnamaldehyde-Zinc (100 ppm–70 mM) | + | + |
| Xanthan Gum | TRPA1 | Citral (250 ppm) | + | + | ||
| Xanthan Gum | TRPA1-TRPM8 | Citral-Isopulegol (250 ppm–200 ppm) | + | + | ||
| Variable | Therapeutic Effect |
|---|---|
| Signs of safety impairment | High: >30% Improvement Intermediate: 10–29% Low: <10% |
| Time to LVC and UESO | High: >100 ms Improvement Intermediate: 50–99 ms Low: <50 ms |
| P2 peak latency | High: >20 ms Improvement Intermediate: 19–10 ms Low: <10 ms |
| N2-P2 amplitude | High: >2 µV Improvement Intermediate: 1–2 µV Low: <1 µV |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomsen, N.; Ortega, O.; Alvarez-Berdugo, D.; Rofes, L.; Clavé, P. A Comparative Study on the Effect of Acute Pharyngeal Stimulation with TRP Agonists on the Biomechanics and Neurophysiology of Swallow Response in Patients with Oropharyngeal Dysphagia. Int. J. Mol. Sci. 2022, 23, 10773. https://doi.org/10.3390/ijms231810773
Tomsen N, Ortega O, Alvarez-Berdugo D, Rofes L, Clavé P. A Comparative Study on the Effect of Acute Pharyngeal Stimulation with TRP Agonists on the Biomechanics and Neurophysiology of Swallow Response in Patients with Oropharyngeal Dysphagia. International Journal of Molecular Sciences. 2022; 23(18):10773. https://doi.org/10.3390/ijms231810773
Chicago/Turabian StyleTomsen, Noemí, Omar Ortega, Daniel Alvarez-Berdugo, Laia Rofes, and Pere Clavé. 2022. "A Comparative Study on the Effect of Acute Pharyngeal Stimulation with TRP Agonists on the Biomechanics and Neurophysiology of Swallow Response in Patients with Oropharyngeal Dysphagia" International Journal of Molecular Sciences 23, no. 18: 10773. https://doi.org/10.3390/ijms231810773