
Increased LRG1 Levels in Overweight and Obese Adolescents and Its Association with Obesity Markers, Including Leptin, Chemerin, and High Sensitivity C-Reactive Protein


 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Description of the Study Group and Obesity in School Adolescents
2.2. Plasma LRG1 Levels Are Significantly Elevated in Overweight and Obese Children
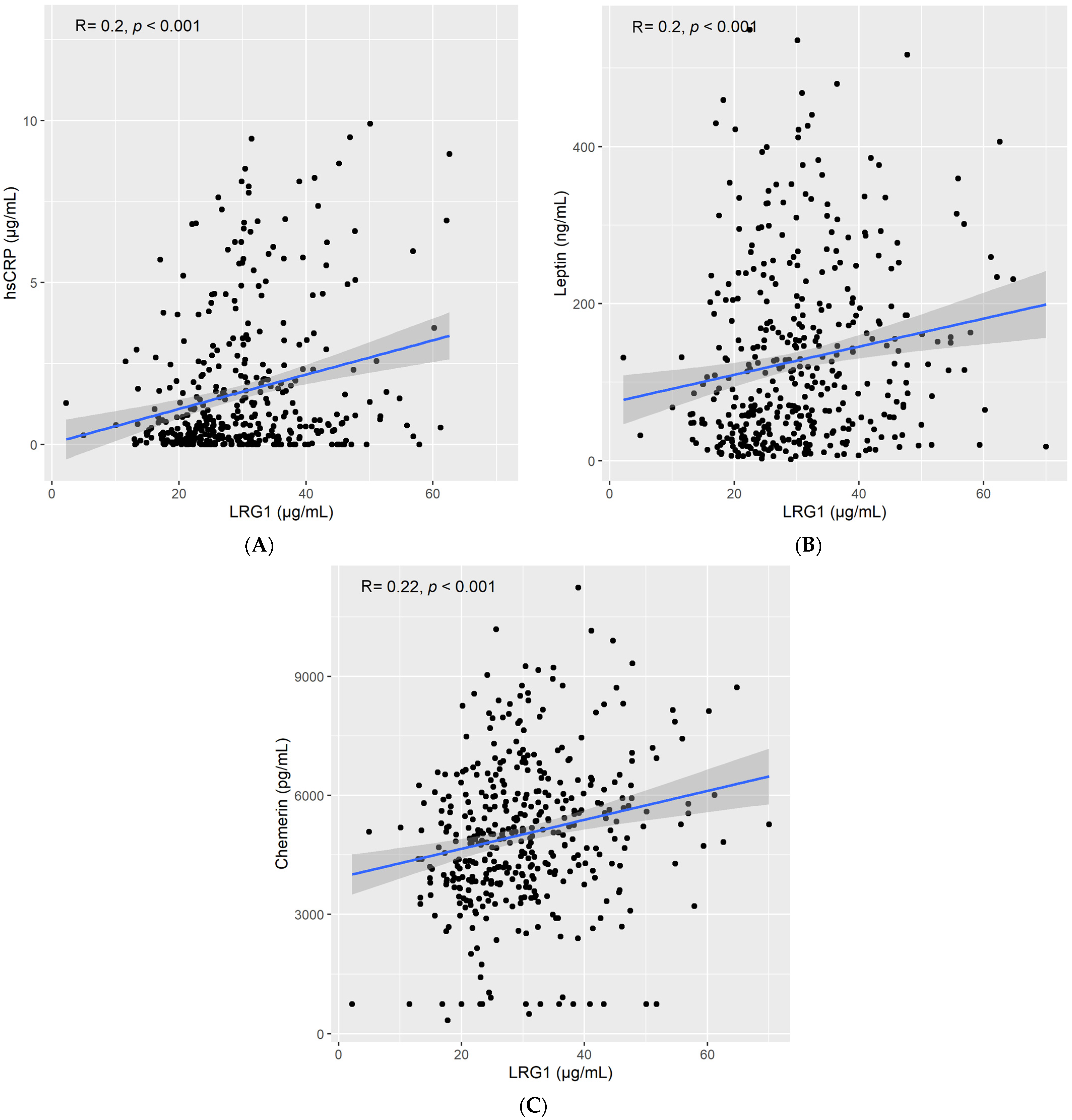
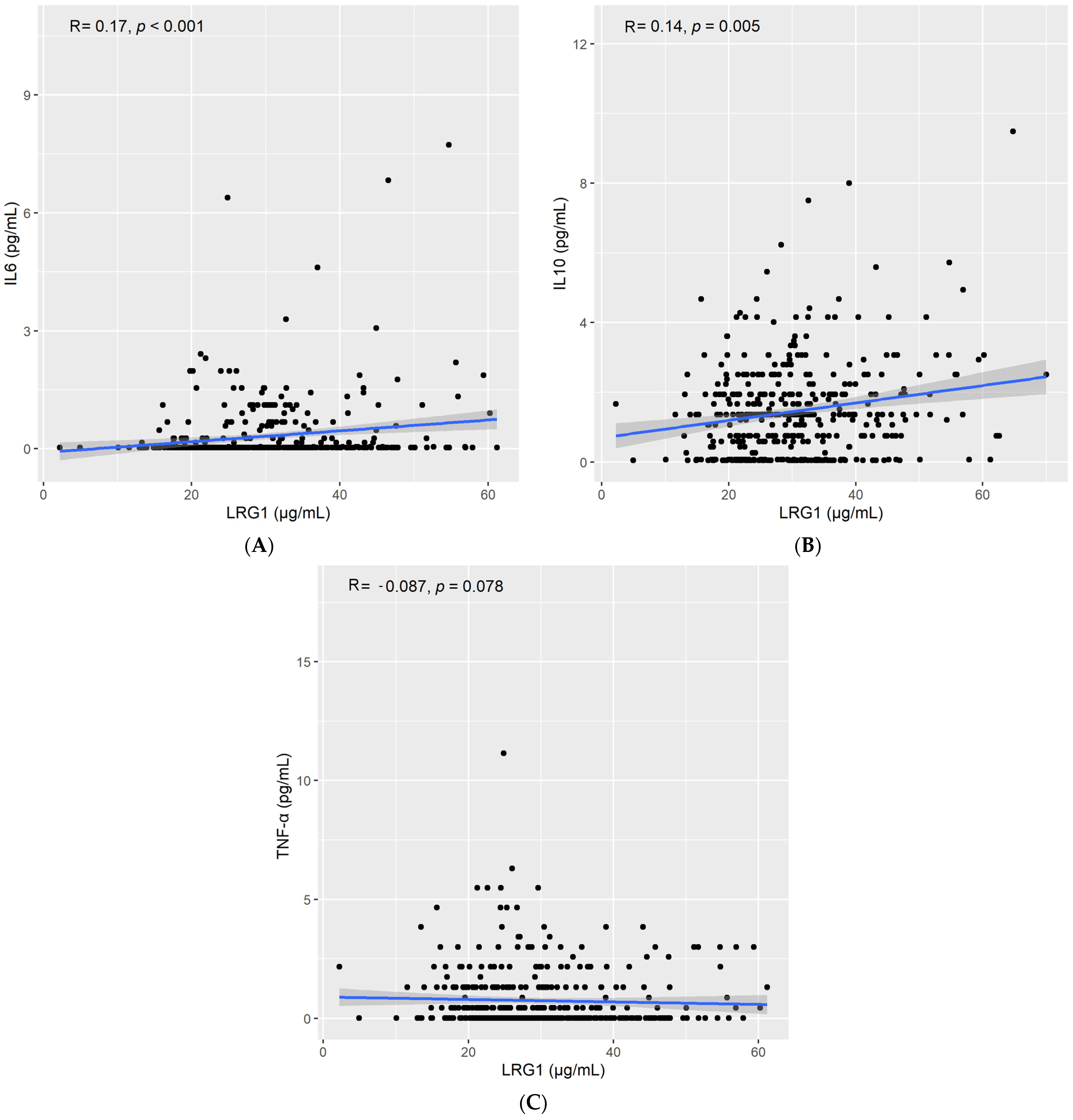
2.3. LRG1 Correlates with Obesity and Inflammatory Markers
3. Discussion
4. Materials and Methods
4.1. Study Participants, Ethics, Consent, and Permissions
4.2. Blood Collection and Biochemical Analyses
4.3. ELISA Assays for LRG1 and HsCRP
4.4. Multiplexing Assays
4.5. Anthropometric Measurements
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al Hammadi, H.; Reilly, J. Prevalence of obesity among school-age children and adolescents in the Gulf cooperation council (GCC) states: A systematic review. BMC Obes. 2019, 6, 3. [Google Scholar] [CrossRef] [Green Version]
- Elkum, N.; Alarouj, M.; Bennakhi, A.; Shaltout, A. The complex etiology of childhood obesity in arabs is highlighted by a combination of biological and socio-economic factors. Front. Public Health 2019, 7, 72. [Google Scholar] [CrossRef]
- Elkum, N.; Al-Arouj, M.; Sharifi, M.; Shaltout, A.; Bennakhi, A. Prevalence of childhood obesity in the state of Kuwait. Pediatr. Obes. 2016, 11, e30–e34. [Google Scholar] [CrossRef]
- Valente, A.M.; Strong, W.; Sinaiko, A.R. Obesity and insulin resistance in young people. Am. Heart J. 2001, 142, 440–444. [Google Scholar] [CrossRef]
- Sinaiko, A.R.; Jacobs, D.R.; Steinberger, J.; Moran, A.; Luepker, R.; Rocchini, A.P.; Prineas, R.J. Insulin resistance syndrome in childhood: Associations of the euglycemic insulin clamp and fasting insulin with fatness and other risk factors. J. Pediatr. 2001, 139, 700–707. [Google Scholar] [CrossRef]
- Kobe, B.; Kajava, A.V. The leucine-rich repeat as a protein recognition motif. Curr. Opin. Struct. Biol. 2001, 11, 725–732. [Google Scholar] [CrossRef]
- Jemmerson, R. Paradoxical Roles of Leucine-Rich α2-Glycoprotein-1 in Cell Death and Survival Modulated by Transforming Growth Factor-Beta 1 and Cytochrome c. Front. Cell Dev. Biol. 2021, 9, 744908. [Google Scholar] [CrossRef]
- Saito, K.; Tanaka, T.; Kanda, H.; Ebisuno, Y.; Izawa, D.; Kawamoto, S.; Okubo, K.; Miyasaka, M. Gene Expression Profiling of Mucosal Addressin Cell Adhesion Molecule-1+ High Endothelial Venule Cells (HEV) and Identification of a Leucine-Rich HEV Glycoprotein as a HEV Marker. J. Immunol. 2002, 168, 1050–1059. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Zhu, L.; Fang, J.; Ge, Z.; Li, X. LRG1 modulates epithelial-mesenchymal transition and angiogenesis in colorectal cancer via HIF-1α activation. J. Exp. Clin. Cancer Res. 2016, 35, 29. [Google Scholar] [CrossRef] [Green Version]
- Hong, Q.; Zhang, L.; Fu, J.; Verghese, D.A.; Chauhan, K.; Nadkarni, G.N.; Li, Z.; Ju, W.; Kretzler, M.; Cai, G.-Y.; et al. LRG1 promotes diabetic kidney disease progression by enhancing TGF-β–induced angiogenesis. J. Am. Soc. Nephrol. 2019, 30, 546–562. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Teo, M.H.Y.; Pek, S.L.T.; Wu, X.; Leong, M.L.; Tay, H.M.; Hou, H.W.; Ruedl, C.; Moss, S.E.; Greenwood, J.; et al. A multifunctional role of leucine-rich α-2-Glycoprotein 1 in cutaneous wound healing under normal and diabetic conditions. Diabetes 2020, 69, 2467–2480. [Google Scholar] [CrossRef] [PubMed]
- Lapeire, L.; Hendrix, A.; Lambein, K.; Van Bockstal, M.; Braems, G.; Broecke, R.V.D.; Limame, R.; Mestdagh, P.; Vandesompele, J.; Vanhove, C.; et al. Cancer-Associated adipose tissue promotes breast cancer progression by paracrine oncostatin M and Jak/STAT3 signaling. Cancer Res. 2014, 74, 6806–6819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Chen, X.; Huang, H.; Han, C.; Qu, Y.; Jin, H.; Niu, T.; Zhang, Y.; Liu, K.; Xu, X. Elevated plasma and vitreous levels of leucine-rich-α2-glycoprotein are associated with diabetic retinopathy progression. Acta Ophthalmol. 2019, 97, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Yu, Y.; Suh, M.-J.; Torralba, M.G.; Stenzel, R.D.; Tovchigrechko, A.; Thovarai, V.; Harkins, D.M.; Rajagopala, S.V.; Osborne, W.; et al. Type 1 diabetes: Urinary proteomics and protein network analysis support perturbation of lysosomal function. Theranostics 2017, 7, 2704–2717. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Ryu, J.; Liu, J.; Luo, H.; Lv, Y.; Langlais, P.R.; Wen, J.; Dong, F.; Sun, Z.; Xia, W.; et al. LRG1 is an adipokine that mediates obesity-induced hepatosteatosis and insulin resistance. J. Clin. Investig. 2021, 131, e148545. [Google Scholar] [CrossRef]
- Pek, S.L.T.; Tavintharan, S.; Wang, X.; Lim, S.C.; Woon, K.; Yeoh, L.Y.; Ng, X.; Liu, J.; Sum, C.F. Elevation of a novel angiogenic factor, leucine-rich-α2-glycoprotein (LRG1), is associated with arterial stiffness, endothelial dysfunction, and peripheral arterial disease in patients with type 2 diabetes. J. Clin. Endocrinol. Metab. 2015, 100, 1586–1593. [Google Scholar] [CrossRef] [Green Version]
- Muramoto, A.; Tsushita, K.; Kato, A.; Ozaki, N.; Tabata, M.; Endo, M.; Oike, Y.; Oiso, Y. Angiopoietin-like protein 2 sensitively responds to weight reduction induced by lifestyle intervention on overweight Japanese men. Nutr. Diabetes 2011, 1, e20. [Google Scholar] [CrossRef] [Green Version]
- Abu-Farha, M.; Abubaker, J.; Al-Khairi, I.; Cherian, P.; Noronha, F.; Hu, F.B.; Behbehani, K.; Elkum, N. Higher plasma betatrophin/ANGPTL8 level in Type 2 Diabetes subjects does not correlate with blood glucose or insulin resistance. Sci. Rep. 2015, 5, 10949. [Google Scholar] [CrossRef]
- Hammad, M.M.; Abu-Farha, M.; Al-Taiar, A.; Alam-Eldin, N.; Al-Sabah, R.; Shaban, L.; Al-Mulla, F.; Abubaker, J.; Rahman, A. Correlation of circulating ANGPTL5 levels with obesity, high sensitivity C-reactive protein and oxidized low-density lipoprotein in adolescents. Sci. Rep. 2020, 10, 6330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kravitz, M.S.; Pitashny, M.; Shoenfeld, Y. Protective molecules–C-Reactive Protein (CRP), Serum Amyloid P (SAP), Pentraxin3 (PTX3), Mannose-Binding Lectin (MBL), and Apolipoprotein A1 (Apo A1), and Their Autoantibodies: Prevalence and Clinical Significance in Autoimmunity. J. Clin. Immunol. 2005, 25, 582–591. [Google Scholar] [CrossRef]
- Abu-Farha, M.; Al-Khairi, I.; Cherian, P.; Chandy, B.; Sriraman, D.; Alhubail, A.; Al-Refaei, F.; AlTerki, A.; Abubaker, J. Increased ANGPTL3, 4 and ANGPTL8/betatrophin expression levels in obesity and T2D. Lipids Health Dis. 2016, 15, 181. [Google Scholar] [CrossRef] [Green Version]
- Al-Terki, A.; Abu-Farha, M.; Alkhairi, I.; Cherian, P.T.; Sriraman, D.; Shyamsundar, A.; Ali, S.; Almulla, F.; Tuomilehto, J.; Abubaker, J.A. Increased Level of Angiopoietin Like Proteins 4 and 8 in People With Sleep Apnea. Front. Endocrinol. 2018, 9, 651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artemniak-Wojtowicz, D.; Kucharska, A.; Pyrżak, B. Obesity and chronic inflammation crosslinking. Central Eur. J. Immunol. 2020, 45, 461–468. [Google Scholar] [CrossRef]
- Galcheva, S.V.; Iotova, V.M.; Yotov, Y.T.; Bernasconi, S.; Street, M.E. Circulating proinflammatory peptides related to abdominal adiposity and cardiometabolic risk factors in healthy prepubertal children. Eur. J. Endocrinol. 2011, 164, 553–558. [Google Scholar] [CrossRef] [Green Version]
- Takumansang, R.; Warouw, S.M.; Lestari, H. Interleukin-6 and insulin resistance in obese adolescents. Paediatr. Indones. 2016, 53, 268–272. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Lim, J.; Nam, G.E.; Park, H.S. Correlation between Serum Lipid Parameters and Interleukin-10 Concentration in Obese Individuals. J. Obes. Metab. Syndr. 2021, 30, 173–177. [Google Scholar] [CrossRef]
- Kondo, H.; Abe, I.; Gotoh, K.; Fukui, A.; Takanari, H.; Ishii, Y.; Ikebe, Y.; Kira, S.; Oniki, T.; Saito, S.; et al. Interleukin 10 Treatment Ameliorates High-Fat Diet–Induced Inflammatory Atrial Remodeling and Fibrillation. Circ. Arrhythmia Electrophysiol. 2018, 11, e006040. [Google Scholar] [CrossRef]
- Chang, J.-S.; Chang, C.-C.; Chien, E.-Y.; Lin, S.-H.; Cheng-Shiuan, T.; Bai, C.-H.; Chao, K.-C. Association between interleukin 1β and interleukin 10 concentrations: A cross-sectional study in young adolescents in Taiwan. BMC Pediatr. 2013, 13, 123. [Google Scholar] [CrossRef] [Green Version]
- Tam, C.S.; Garnett, S.P.; Cowell, C.T.; Heilbronn, L.K.; Lee, J.W.; Wong, M.; Baur, L.A. IL-6, IL-8 and IL-10 Levels in Healthy Weight and Overweight Children. Horm. Res. Paediatr. 2010, 73, 128–134. [Google Scholar] [CrossRef]
- Esposito, K.; Pontillo, A.; Giugliano, F.; Giugliano, G.; Marfella, R.; Nicoletti, G.; Giugliano, D. Association of Low Interleukin-10 Levels with the Metabolic Syndrome in Obese Women. J. Clin. Endocrinol. Metab. 2003, 88, 1055–1058. [Google Scholar] [CrossRef]
- Dritsoula, A.; Dowsett, L.; Pilotti, C.; O’Connor, M.N.; Moss, S.E.; Greenwood, J. Angiopathic activity of LRG1 is induced by the IL-6/STAT3 pathway. Sci. Rep. 2022, 12, 4867. [Google Scholar] [CrossRef]
- Cevey, C.; Penas, F.N.; Soto, C.D.A.; Mirkin, G.A.; Goren, N.B. IL-10/STAT3/SOCS3 Axis Is Involved in the Anti-inflammatory Effect of Benznidazole. Front. Immunol. 2019, 10, 1267. [Google Scholar] [CrossRef]
- Matarese, G.; Moschos, S.; Mantzoros, C.S. Leptin in Immunology. J. Immunol. 2005, 174, 3137–3142. [Google Scholar] [CrossRef] [Green Version]
- La Cava, A. Leptin in inflammation and autoimmunity. Cytokine 2017, 98, 51–58. [Google Scholar] [CrossRef]
- Yang, J.; Liu, Z.; Liu, H.; He, J.; Yang, J.; Lin, P.; Wang, Q.; Du, J.; Ma, W.; Yin, Z.; et al. C-reactive protein promotes bone destruction in human myeloma through the CD32–p38 MAPK–Twist axis. Sci. Signal. 2017, 10, eaan6282. [Google Scholar] [CrossRef] [Green Version]
- Krautbauer, S.; Wanninger, J.; Eisinger, K.; Hader, Y.; Beck, M.; Kopp, A.; Schmid, A.; Weiss, T.S.; Dorn, C.; Buechler, C. Chemerin is highly expressed in hepatocytes and is induced in non-alcoholic steatohepatitis liver. Exp. Mol. Pathol. 2013, 95, 199–205. [Google Scholar] [CrossRef]
- Wittamer, V.; Franssen, J.D.; Vulcano, M.; Mirjolet, J.F.; Le Poul, E.; Migeotte, I.; Brézillon, S.; Tyldesley, R.; Blanpain, C.; Detheux, M.; et al. Specific recruitment of antigen-presenting cells by chemerin, a novel processed ligand from human inflammatory fluids. J. Exp. Med. 2003, 198, 977–985. [Google Scholar] [CrossRef]
- Goralski, K.B.; McCarthy, T.C.; Hanniman, E.A.; Zabel, B.A.; Butcher, E.C.; Parlee, S.D.; Muruganandan, S.; Sinal, C.J. Chemerin, a Novel Adipokine That Regulates Adipogenesis and Adipocyte Metabolism. J. Biol. Chem. 2007, 282, 28175–28188. [Google Scholar] [CrossRef] [Green Version]
- Bozaoglu, K.; Bolton, K.; McMillan, J.; Zimmet, P.; Jowett, J.; Collier, G.; Walder, K.; Segal, D. Chemerin Is a Novel Adipokine Associated with Obesity and Metabolic Syndrome. Endocrinology 2007, 148, 4687–4694. [Google Scholar] [CrossRef]
- Bozaoglu, K.; Segal, D.; Shields, K.A.; Cummings, N.; Curran, J.E.; Comuzzie, A.G.; Mahaney, M.C.; Rainwater, D.L.; VandeBerg, J.L.; Maccluer, J.W.; et al. Chemerin Is Associated with Metabolic Syndrome Phenotypes in a Mexican-American Population. J. Clin. Endocrinol. Metab. 2009, 94, 3085–3088. [Google Scholar] [CrossRef]
- Chakaroun, R.; Raschpichler, M.; Klöting, N.; Oberbach, A.; Flehmig, G.; Kern, M.; Schön, M.R.; Shang, E.; Lohmann, T.; Dreßler, M.; et al. Effects of weight loss and exercise on chemerin serum concentrations and adipose tissue expression in human obesity. Metabolism 2012, 61, 706–714. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Mu, J.; Du, J.; Feng, Y.; Xu, W.; Bai, M.; Zhang, H. Alpha-lipoic acid could attenuate the effect of chemerin-induced diabetic nephropathy progression. Iran. J. Basic Med. Sci. 2021, 24, 1107. [Google Scholar] [CrossRef]
- Xie, Z.-B.; Zhang, Y.-F.; Jin, C.; Mao, Y.-S.; Fu, D.-L. LRG-1 promotes pancreatic cancer growth and metastasis via modulation of the EGFR/p38 signaling. J. Exp. Clin. Cancer Res. 2019, 38, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ban, Z.; He, J.; Tang, Z.; Zhang, L.; Xu, Z. LRG-1 enhances the migration of thyroid carcinoma cells through promotion of the epithelial-mesenchymal transition by activating MAPK/p38 signaling. Oncol. Rep. 2019, 41, 3270–3280. [Google Scholar] [CrossRef] [PubMed]
- Lim, A.K.H.; Nikolic-Paterson, D.J.; Ma, F.Y.; Ozols, E.; Thomas, M.C.; Flavell, R.A.; Davis, R.J.; Tesch, G.H. Role of MKK3–p38 MAPK signalling in the development of type 2 diabetes and renal injury in obese db/db mice. Diabetologia 2009, 52, 347–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donohoe, F.; Wilkinson, M.; Baxter, E.; Brennan, D.J. Mitogen-Activated Protein Kinase (MAPK) and Obesity-Related Cancer. Int. J. Mol. Sci. 2020, 21, 1241. [Google Scholar] [CrossRef] [Green Version]
- Pickert, G.; Neufert, C.; Leppkes, M.; Zheng, Y.; Wittkopf, N.; Warntjen, M.; Lehr, H.-A.; Hirth, S.; Weigmann, B.; Wirtz, S.; et al. STAT3 links IL-22 signaling in intestinal epithelial cells to mucosal wound healing. J. Exp. Med. 2009, 206, 1465–1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naka, T.; Fujimoto, M. LRG is a novel inflammatory marker clinically useful for the evaluation of disease activity in rheumatoid arthritis and inflammatory bowel disease. Immunol. Med. 2018, 41, 62–67. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, J.; Zhang, X.; Wang, C.; Huang, Y.; Dai, K.; Zhang, X. TNF-α-induced LRG1 promotes angiogenesis and mesenchymal stem cell migration in the subchondral bone during osteoarthritis. Cell Death Dis. 2017, 8, e2715. [Google Scholar] [CrossRef]
- Makita, N.; Hizukuri, Y.; Yamashiro, K.; Murakawa, M.; Hayashi, Y. IL-10 enhances the phenotype of M2 macrophages induced by IL-4 and confers the ability to increase eosinophil migration. Int. Immunol. 2015, 27, 131–141. [Google Scholar] [CrossRef] [Green Version]
- Al-Taiar, A.; Rahman, A.; Al-Sabah, R.; Shaban, L.; Al-Harbi, A. Vitamin D status among adolescents in Kuwait: A cross-sectional study. BMJ Open 2018, 8, e021401. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Al-Taiar, A.; Shaban, L.; Al-Sabah, R.; Al-Harbi, A.; Mojiminiyi, O. Plasma 25-Hydroxy Vitamin D Is Not Associated with Either Cognitive Function or Academic Performance in Adolescents. Nutrients 2018, 10, 1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Normal-Weight N = 193 1 | Overweight N = 89 1 | Obesity N = 143 1 | p-Value 2 |
|---|---|---|---|---|
| Sex | >0.9 | |||
| Female | 107 (55%) | 49 (55%) | 76 (53%) | |
| Male | 86 (45%) | 40 (45%) | 67 (47%) | |
| Age Group | 0.8 | |||
| 10–<12 years | 82 (42%) | 37 (42%) | 62 (43%) | |
| 12–<13 years | 67 (35%) | 28 (31%) | 52 (36%) | |
| 13+ years | 44 (23%) | 24 (27%) | 29 (20%) | |
| Glucose (mmol/L) | 4.87 (0.72) | 4.87 (0.74) | 5.22 (1.76) | 0.11 |
| WBC (×109 cells/L) | 6.32 (1.61) | 6.95 (2.03) | 7.72 (1.90) | <0.001 |
| RBC (×1012 cells/L) | 4.99 (0.43) | 5.04 (0.37) | 5.11 (0.41) | 0.011 |
| Folate | 1491 (282) | 1449 (292) | 1529 (319) | 0.3 |
| Vitamin D (nmol/L) | 36 (23) | 34 (20) | 33 (19) | 0.8 |
| Odds Ratio (OR) 1 | Adjusted Odds Ratio (AOR) 3 | |||||||
|---|---|---|---|---|---|---|---|---|
| Overweight | Obese | Overweight | Obese | |||||
| OR 1 [95% CI] 2 | p-Value | OR 1 [95% CI] 2 | p-Value | AOR 3 [95% CI] 2 | p-Value | AOR 3 [95% CI] 2 | p-Value | |
| LRG1 (univariable) | 1.03 [1.00, 1.05] | 0.055 | 1.03 [1.01, 1.06] | 0.005 | 1.03 [1.00, 1.06] | 0.043 | 1.04 [1.01, 1.06] | 0.004 |
| LRG1 (categories) | ||||||||
| Lower tertile (<24.8 µg/mL) | 1 [Ref.] | - | 1 [Ref.] | - | 1 [Ref.] | - | 1 [Ref.] | - |
| Middle tertile (>24.8 and <32.5 µg/mL) | 1.22 [0.64, 2.32] | 0.6 | 2.42 [1.38, 4.25] | 0.002 | 1.20 [0.63, 2.30] | 0.6 | 2.39 [1.36, 4.20] | 0.002 |
| Upper tertile (>35.5 µg/mL) | 1.93 [1.04, 3.57] | 0.037 | 2.55 [1.44, 4.53] | 0.001 | 2.04 [1.08, 3.83] | 0.027 | 2.64 [1.47, 4.74] | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhammad, R.; Abu-Farha, M.; Hammad, M.M.; Thanaraj, T.A.; Channanath, A.; Alam-Eldin, N.; Al-Sabah, R.; Shaban, L.; Alduraywish, A.; Al-Mulla, F.; et al. Increased LRG1 Levels in Overweight and Obese Adolescents and Its Association with Obesity Markers, Including Leptin, Chemerin, and High Sensitivity C-Reactive Protein. Int. J. Mol. Sci. 2022, 23, 8564. https://doi.org/10.3390/ijms23158564
Alhammad R, Abu-Farha M, Hammad MM, Thanaraj TA, Channanath A, Alam-Eldin N, Al-Sabah R, Shaban L, Alduraywish A, Al-Mulla F, et al. Increased LRG1 Levels in Overweight and Obese Adolescents and Its Association with Obesity Markers, Including Leptin, Chemerin, and High Sensitivity C-Reactive Protein. International Journal of Molecular Sciences. 2022; 23(15):8564. https://doi.org/10.3390/ijms23158564
Chicago/Turabian StyleAlhammad, Rashed, Mohamed Abu-Farha, Maha M. Hammad, Thangavel Alphonse Thanaraj, Arshad Channanath, Nada Alam-Eldin, Reem Al-Sabah, Lemia Shaban, Abdulrahman Alduraywish, Fahd Al-Mulla, and et al. 2022. "Increased LRG1 Levels in Overweight and Obese Adolescents and Its Association with Obesity Markers, Including Leptin, Chemerin, and High Sensitivity C-Reactive Protein" International Journal of Molecular Sciences 23, no. 15: 8564. https://doi.org/10.3390/ijms23158564