
Characterization of the MicroRNA Cargo of Extracellular Vesicles Isolated from a Pulmonary Tumor-Draining Vein Identifies miR-203a-3p as a Relapse Biomarker for Resected Non-Small Cell Lung Cancer

 , , , , ,
, , , , , 

Abstract
:1. Introduction
2. Results
2.1. Screening Phase
2.1.1. Patients
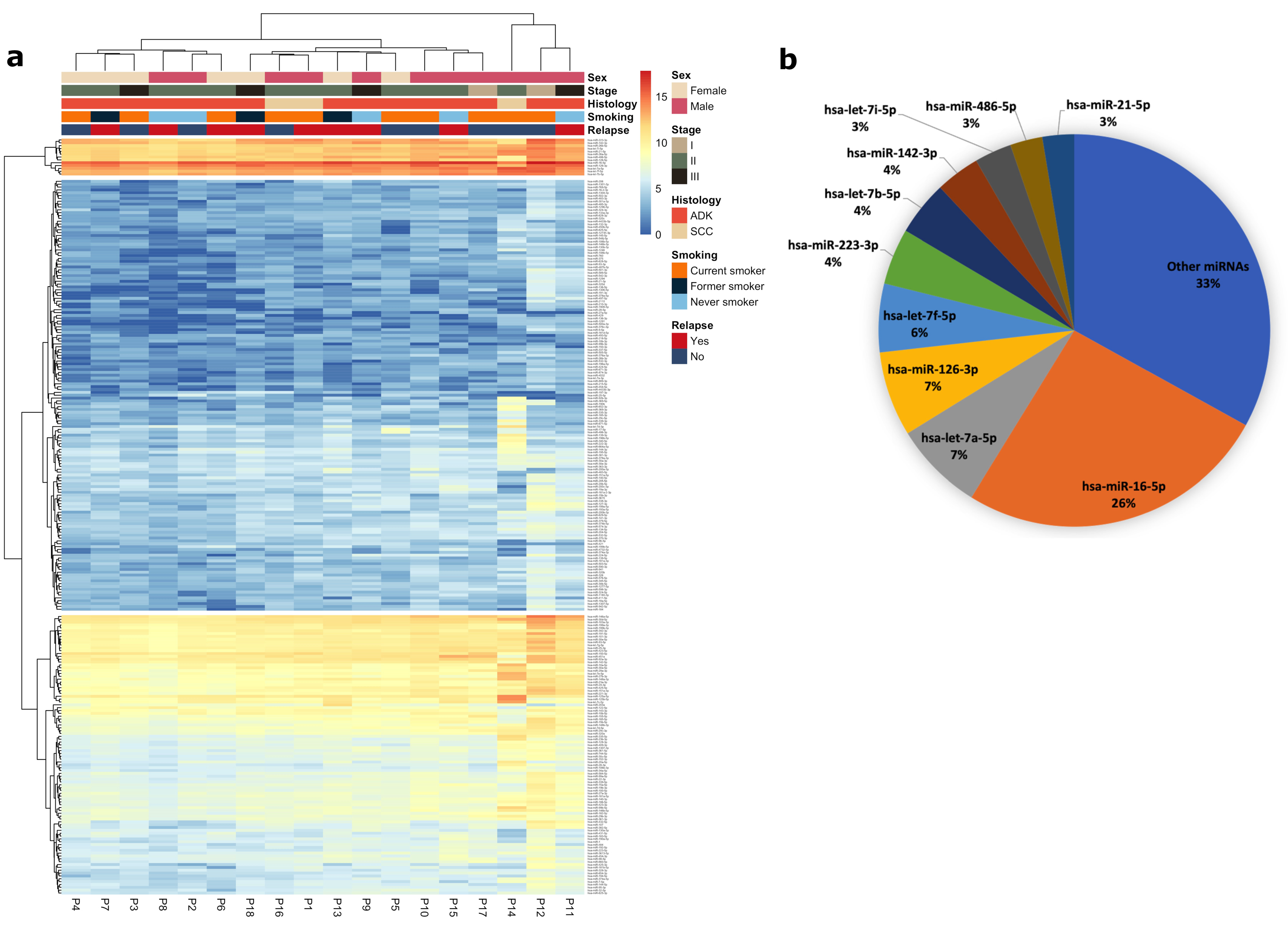
2.1.2. miRNA Profile of EV Purified from Pulmonary TDV
2.1.3. Identification of miRNAs Associated with Relapse
2.1.4. Identification of EV-miR-203a-3p as a Candidate Relapse Biomarker
2.2. Validation Phase
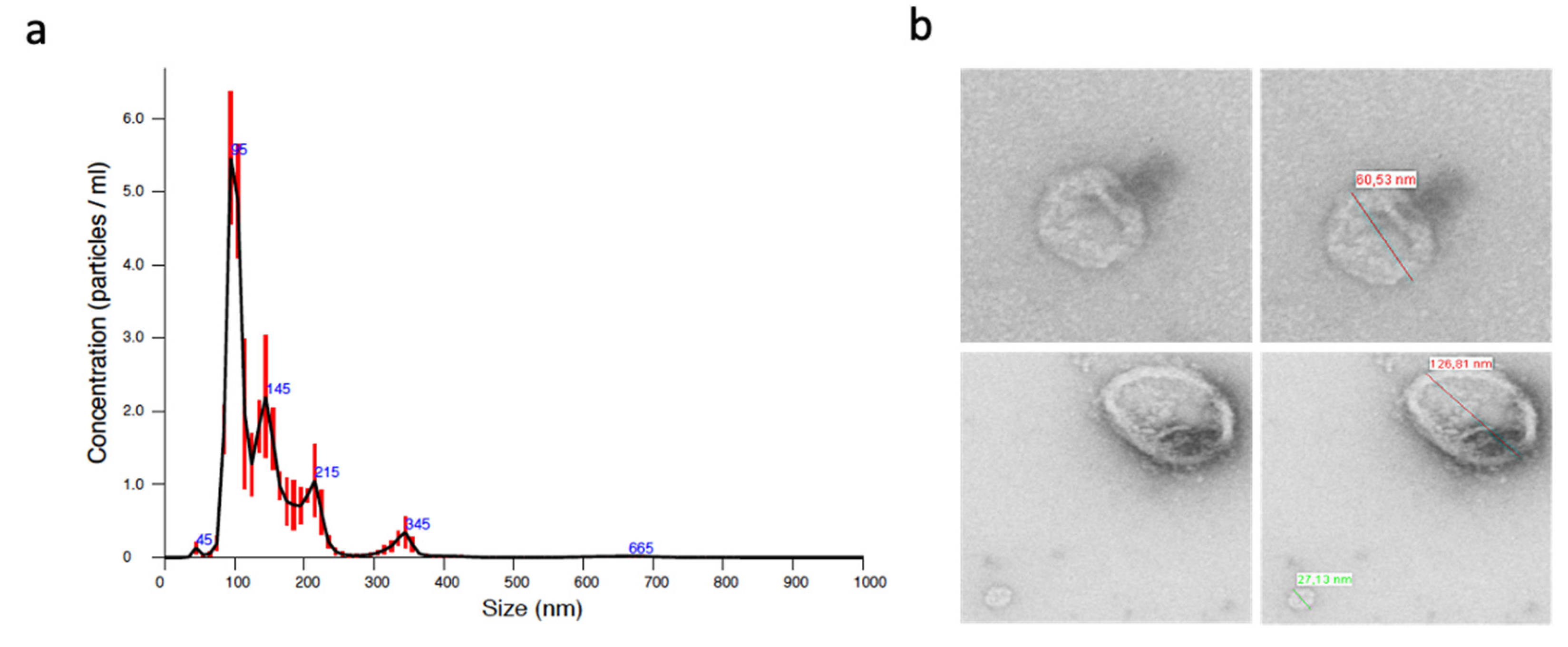
2.2.1. Characterization of Isolated EVs
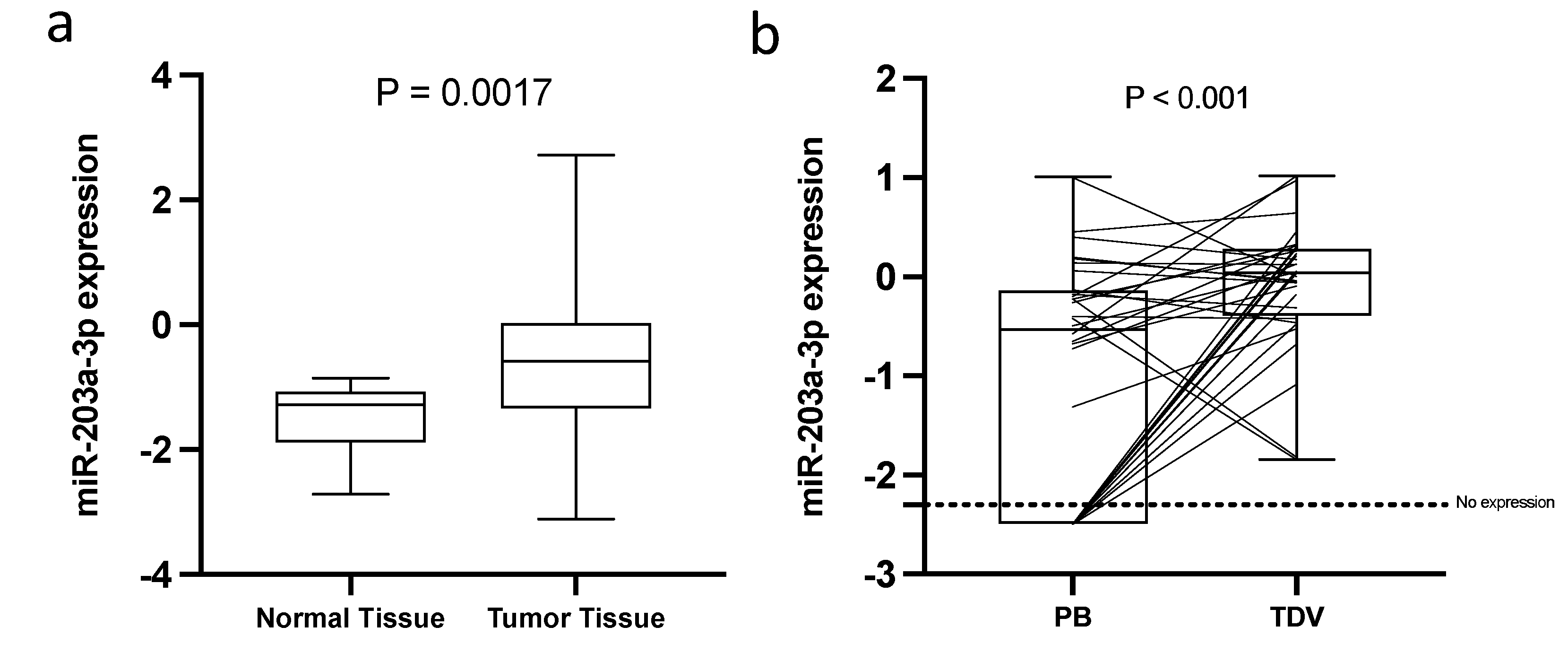
2.2.2. Exploratory Analysis of the Expression of miR-203a-3p in Tissue and Peripheral Blood
2.2.3. Characteristics of the Patients from the Validation Cohort
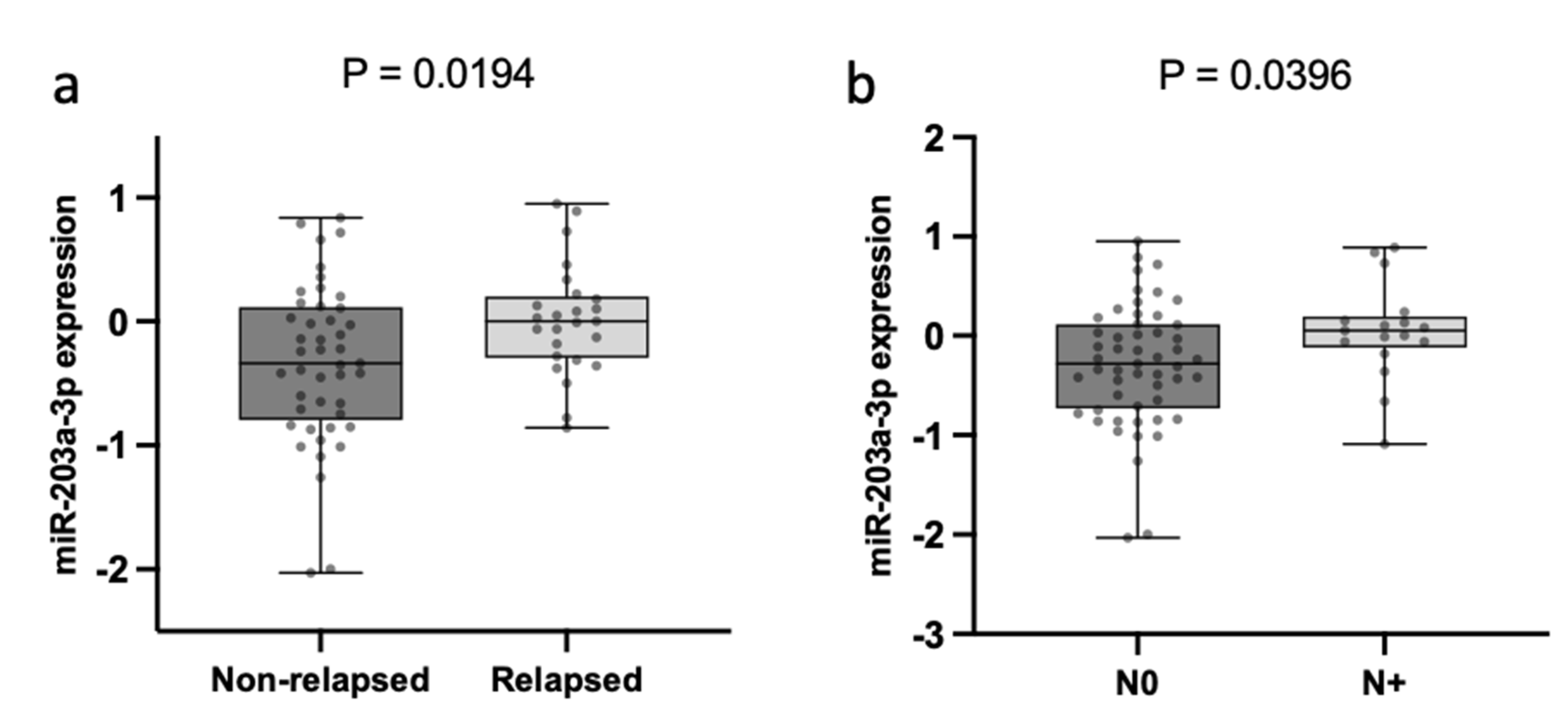
2.2.4. TDV EV-miR-203a-3p Expression Is Associated with N and Relapse
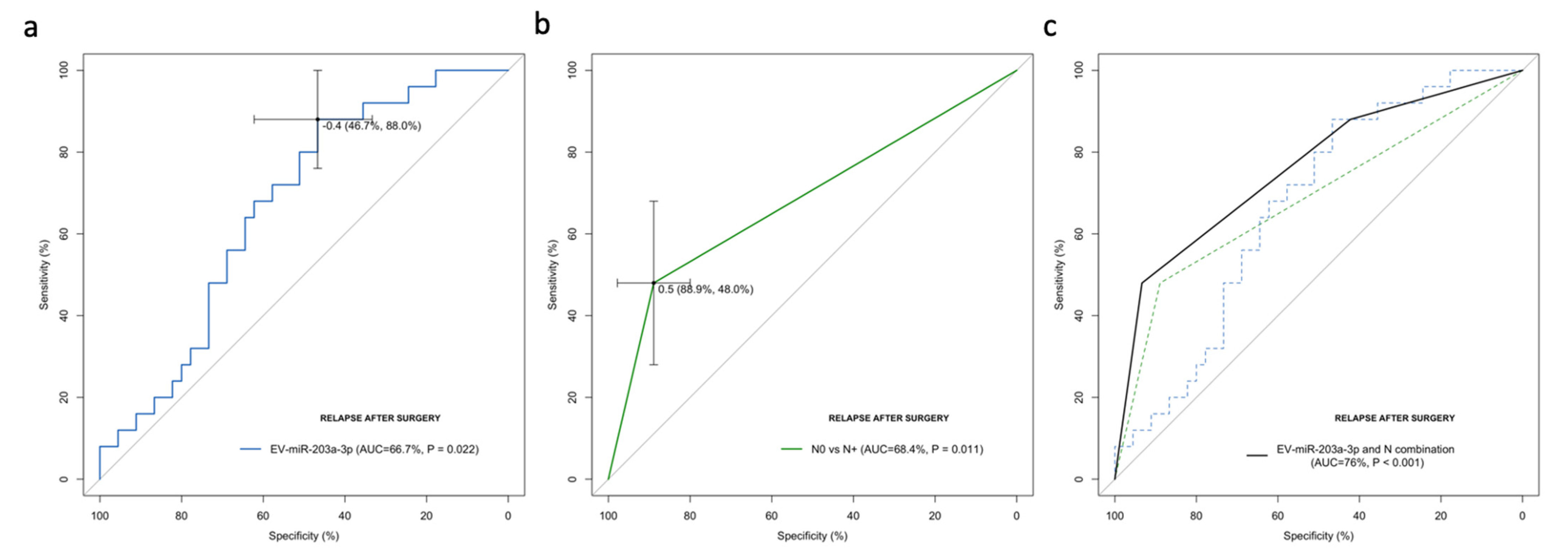
2.2.5. EV-miR-203a-3p Levels Validated as Relapse Biomarkers in the Validation Cohort
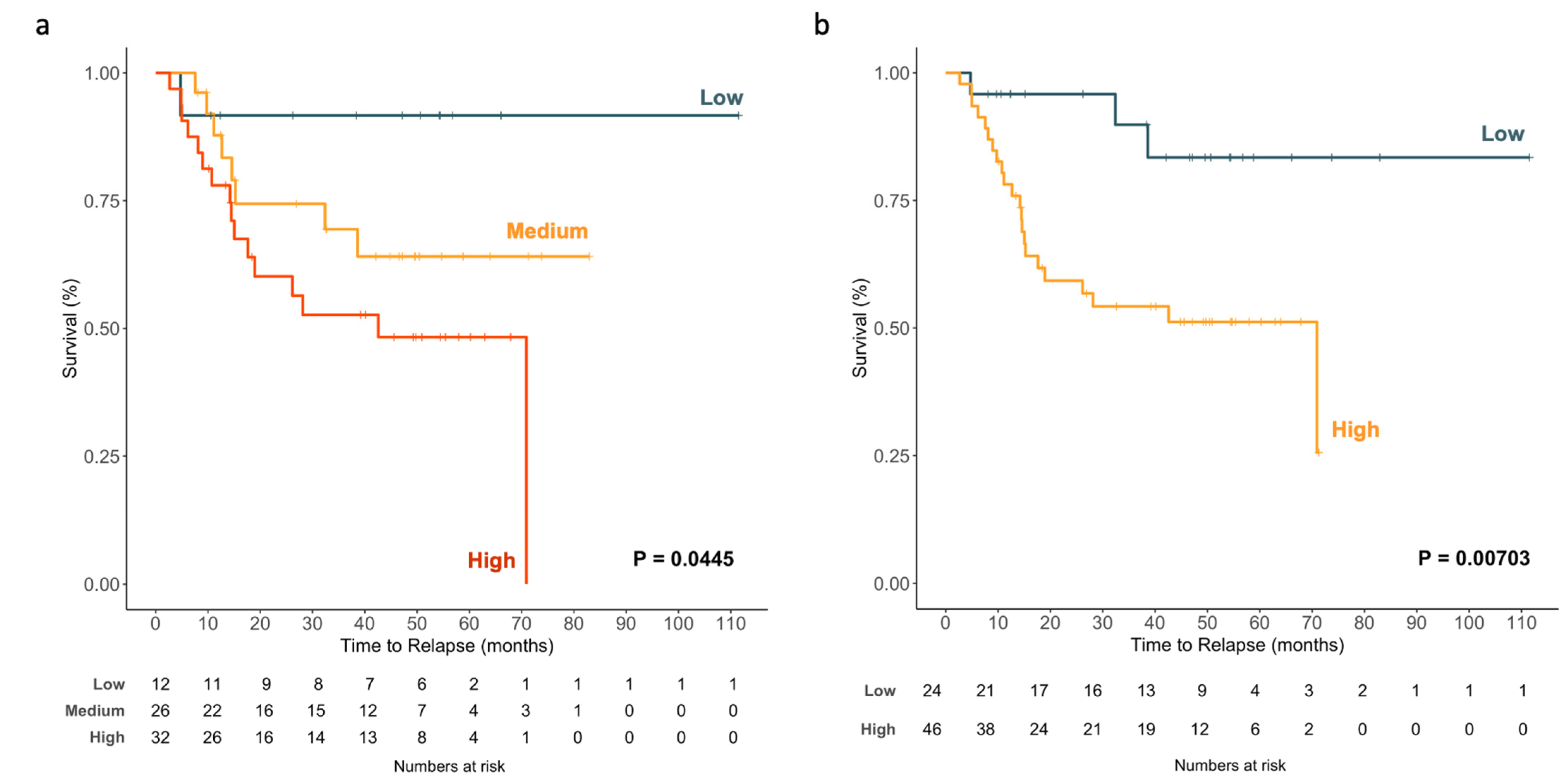
2.2.6. EV-miR-203a-3p Levels Impact TTR
2.2.7. Cox Modeling of Relapse
2.2.8. Impact on the TTR of the Combination of N and EV-miR-203a-3p Levels
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Patient Samples
4.3. EV miRNA Profiling by Small RNAseq in the Screening Phase
4.4. Bioinformatic Analysis of Small RNAseq Data
4.5. EV Purification and Characterization in the Validation Phase
4.6. RNA Extraction and miRNA Expression Analysis in the Validation Phase
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann. Glob. Health 2019, 85, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uramoto, H.; Tanaka, F. Recurrence after surgery in patients with NSCLC. Transl. Lung Cancer Res. 2014, 3, 242. [Google Scholar] [PubMed]
- Liu, C.H.; Peng, Y.J.; Wang, H.H.; Chen, Y.C.; Tsai, C.L.; Chian, C.F.; Huang, T.W. Heterogeneous prognosis and adjuvant chemotherapy in pathological stage I non-small cell lung cancer patients. Thorac. Cancer 2015, 6, 620–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallardo, E.; Navarro, A.; Vinolas, N.; Marrades, R.M.; Diaz, T.; Gel, B.; Quera, A.; Bandres, E.; Garcia-Foncillas, J.; Ramirez, J.; et al. miR-34a as a prognostic marker of relapse in surgically resected non-small-cell lung cancer. Carcinogenesis 2009, 30, 1903–1909. [Google Scholar] [CrossRef] [Green Version]
- Tejero, R.; Navarro, A.; Campayo, M.; Viñolas, N.; Marrades, R.M.; Cordeiro, A.; Ruíz-Martínez, M.; Santasusagna, S.; Molins, L.; Ramirez, J.; et al. miR-141 and miR-200c as markers of overall survival in early stage non-small cell lung cancer adenocarcinoma. PLoS ONE 2014, 9, e101899. [Google Scholar] [CrossRef]
- Duncavage, E.; Goodgame, B.; Sezhiyan, A.; Govindan, R.; Pfeifer, J. Use of microRNA expression levels to predict outcomes in resected stage I non-small cell lung cancer. J. Thorac. Oncol. 2010, 5, 1755–1763. [Google Scholar] [CrossRef] [Green Version]
- Rijavec, E.; Coco, S.; Genova, C.; Rossi, G.; Longo, L.; Grossi, F. Liquid biopsy in non-small cell lung cancer: Highlights and challenges. Cancers 2019, 12, 17. [Google Scholar] [CrossRef] [Green Version]
- Dorsey, J.F.; Kao, G.D.; MacArthur, K.M.; Ju, M.; Steinmetz, D.; Wileyto, E.P.; Simone, C.B.; Hahn, S.M. Tracking viable circulating tumor cells (CTC s) in the peripheral blood of non–small cell lung cancer (NSCLC) patients undergoing definitive radiation therapy: Pilot study results. Cancer 2015, 121, 139–149. [Google Scholar] [CrossRef] [Green Version]
- Muinelo-Romay, L.; Vieito, M.; Abalo, A.; Nocelo, M.A.; Barón, F.; Anido, U.; Brozos, E.; Vázquez, F.; Aguín, S.; Abal, M.; et al. Evaluation of circulating tumor cells and related events as prognostic factors and surrogate biomarkers in advanced NSCLC patients receiving first-line systemic treatment. Cancers 2014, 6, 153–165. [Google Scholar] [CrossRef] [Green Version]
- Wan, L.; Liu, Q.; Liang, D.; Guo, Y.; Liu, G.; Ren, J.; He, Y.; Shan, B. Circulating Tumor Cell and Metabolites as Novel Biomarkers for Early-Stage Lung Cancer Diagnosis. Front. Oncol. 2021, 11, 1465. [Google Scholar] [CrossRef]
- Jamal-Hanjani, M.; Wilson, G.; Horswell, S.; Mitter, R.; Sakarya, O.; Constantin, T.; Salari, R.; Kirkizlar, E.; Sigurjonsson, S.; Pelham, R.; et al. Detection of ubiquitous and heterogeneous mutations in cell-free DNA from patients with early-stage non-small-cell lung cancer. Ann. Oncol. 2016, 27, 862–867. [Google Scholar] [CrossRef]
- Abbosh, C.; Birkbak, N.J.; Wilson, G.A.; Jamal-Hanjani, M.; Constantin, T.; Salari, R.; Le Quesne, J.; Moore, D.A.; Veeriah, S.; Rosenthal, R.; et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature 2017, 545, 446–451. [Google Scholar] [CrossRef]
- Ulivi, P.; Petracci, E.; Marisi, G.; Baglivo, S.; Chiari, R.; Billi, M.; Canale, M.; Pasini, L.; Racanicchi, S.; Vagheggini, A.; et al. Prognostic role of circulating miRNAs in early-stage non-small cell lung cancer. J. Clin. Med. 2019, 8, 131. [Google Scholar] [CrossRef] [Green Version]
- Kaduthanam, S.; Gade, S.; Meister, M.; Brase, J.C.; Johannes, M.; Dienemann, H.; Warth, A.; Schnabel, P.A.; Herth, F.J.; Sültmann, H.; et al. Serum miR-142-3p is associated with early relapse in operable lung adenocarcinoma patients. Lung Cancer 2013, 80, 223–227. [Google Scholar] [CrossRef]
- Wiemer, E.A. Prognostic Circulating MicroRNA Biomarkers in Early-Stage Non-Small Cell Lung Cancer: A Role for miR-150. Clin. Pharmacol. Ther. 2018, 103, 968–970. [Google Scholar] [CrossRef]
- Liu, Q.; Xiang, Y.; Yuan, S.; Xie, W.; Li, C.; Hu, Z.; Wu, N.; Wu, L.; Yu, Z.; Bai, L.; et al. Plasma exosome levels in non-small-cell lung cancer: Correlation with clinicopathological features and prognostic implications. Cancer Biomark. 2018, 22, 267–274. [Google Scholar] [CrossRef]
- Wan, Y.; Liu, B.; Lei, H.; Zhang, B.; Wang, Y.; Huang, H.; Chen, S.; Feng, Y.; Zhu, L.; Gu, Y.; et al. Nanoscale extracellular vesicle-derived DNA is superior to circulating cell-free DNA for mutation detection in early-stage non-small-cell lung cancer. Ann. Oncol. 2018, 29, 2379–2383. [Google Scholar] [CrossRef]
- Dejima, H.; Iinuma, H.; Kanaoka, R.; Matsutani, N.; Kawamura, M. Exosomal microRNA in plasma as a non-invasive biomarker for the recurrence of non-small cell lung cancer. Oncol. Letters 2017, 13, 1256–1263. [Google Scholar] [CrossRef] [Green Version]
- Théry, C.; Witwer, K.W.; Aikawa, E.; Alcaraz, M.J.; Anderson, J.D.; Andriantsitohaina, R.; Antoniou, A.; Arab, T.; Archer, F.; Atkin-Smith, G.K.; et al. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): A position statement of the International Society for Extracellular Vesicles and update of the MISEV2014 guidelines. J. Extracell. Vesicles 2018, 7, 1535750. [Google Scholar] [CrossRef] [Green Version]
- Yáñez-Mó, M.; Siljander, P.R.-M.; Andreu, Z.; Bedina Zavec, A.; Borràs, F.E.; Buzas, E.I.; Buzas, K.; Casal, E.; Cappello, F.; Carvalho, J.; et al. Biological properties of extracellular vesicles and their physiological functions. J. Extracell. Vesicles 2015, 4, 27066. [Google Scholar] [CrossRef] [Green Version]
- Yuan, T.; Huang, X.; Woodcock, M.; Du, M.; Dittmar, R.; Wang, Y.; Tsai, S.; Kohli, M.; Boardman, L.; Patel, T.; et al. Plasma extracellular RNA profiles in healthy and cancer patients. Sci. Rep. 2016, 6, 19413. [Google Scholar] [CrossRef] [Green Version]
- Okumura, Y.; Tanaka, F.; Yoneda, K.; Hashimoto, M.; Takuwa, T.; Kondo, N.; Hasegawa, S. Circulating tumor cells in pulmonary venous blood of primary lung cancer patients. Ann. Thorac. Surg. 2009, 87, 1669–1675. [Google Scholar] [CrossRef]
- Murlidhar, V.; Reddy, R.M.; Fouladdel, S.; Zhao, L.; Ishikawa, M.K.; Grabauskiene, S.; Zhang, Z.; Lin, J.; Chang, A.C.; Carrott, P.; et al. Poor prognosis indicated by venous circulating tumor cell clusters in early-stage lung cancers. Cancer Res. 2017, 77, 5194–5206. [Google Scholar] [CrossRef] [Green Version]
- Navarro, A.; Molins, L.; Marrades, R.M.; Moises, J.; Vinolas, N.; Morales, S.; Canals, J.; Castellano, J.J.; Ramirez, J.; Monzo, M. Exosome Analysis in Tumor-Draining Pulmonary Vein Identifies NSCLC Patients with Higher Risk of Relapse after Curative Surgery. Cancers 2019, 11, 249. [Google Scholar] [CrossRef] [Green Version]
- Crosbie, P.A.; Shah, R.; Krysiak, P.; Zhou, C.; Morris, K.; Tugwood, J.; Booton, R.; Blackhall, F.; Dive, C. Circulating tumor cells detected in the tumor-draining pulmonary vein are associated with disease recurrence after surgical resection of NSCLC. J. Thorac. Oncol. 2016, 11, 1793–1797. [Google Scholar] [CrossRef] [Green Version]
- Castellano, J.J.; Marrades, R.M.; Molins, L.; Viñolas, N.; Moises, J.; Canals, J.; Han, B.; Li, Y.; Martinez, D.; Monzó, M.; et al. Extracellular vesicle lincRNA-p21 expression in tumor-draining pulmonary vein defines prognosis in NSCLC and modulates endothelial cell behavior. Cancers 2020, 12, 734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hattori, M.; Nakanishi, H.; Yoshimura, M.; Iwase, M.; Yoshimura, A.; Adachi, Y.; Gondo, N.; Kotani, H.; Sawaki, M.; Fujita, N.; et al. Circulating tumor cells detection in tumor draining vein of breast cancer patients. Sci. Rep. 2019, 9, 18195. [Google Scholar] [CrossRef] [Green Version]
- Monzo, M.; Santasusagna, S.; Moreno, I.; Martinez, F.; Hernáez, R.; Muñoz, C.; Castellano, J.J.; Moreno, J.; Navarro, A. Exosomal microRNAs isolated from plasma of mesenteric veins linked to liver metastases in resected patients with colon cancer. Oncotarget 2017, 8, 30859. [Google Scholar] [CrossRef] [Green Version]
- Wind, J.; Tuynman, J.; Tibbe, A.; Swennenhuis, J.; Richel, D.; van Berge Henegouwen, M.; Bemelman, W. Circulating tumour cells during laparoscopic and open surgery for primary colonic cancer in portal and peripheral blood. Eur. J. Surg. Oncol. 2009, 35, 942–950. [Google Scholar] [CrossRef]
- Duréndez-Sáez, E.; Torres-Martinez, S.; Calabuig-Fariñas, S.; Meri-Abad, M.; Ferrero-Gimeno, M.; Camps, C. Exosomal microRNAs in non-small cell lung cancer. Transl. Cancer Res. 2021, 10, 3128. [Google Scholar] [CrossRef]
- Zhou, X.; Wen, W.; Shan, X.; Zhu, W.; Xu, J.; Guo, R.; Cheng, W.; Wang, F.; Qi, L.-W.; Chen, Y.; et al. A six-microRNA panel in plasma was identified as a potential biomarker for lung adenocarcinoma diagnosis. Oncotarget 2017, 8, 6513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, X.; Friedman, A. Exosomal miRs in lung cancer: A mathematical model. PLoS ONE 2016, 11, e0167706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabinowits, G.; Gerçel-Taylor, C.; Day, J.M.; Taylor, D.D.; Kloecker, G.H. Exosomal microRNA: A diagnostic marker for lung cancer. Clin. Lung Cancer 2009, 10, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Chen, Y.; Chen, H.; Fei, S.; Chen, D.; Cai, X.; Liu, L.; Lin, B.; Su, H.; Zhao, L.; et al. Evaluation of tumor-derived exosomal miRNA as potential diagnostic biomarkers for early-stage non–small cell lung cancer using next-generation sequencing. Clin. Cancer Res. 2017, 23, 5311–5319. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.; Pochampally, R.; Watabe, K.; Lu, Z.; Mo, Y.-Y. Exosome-mediated transfer of miR-10b promotes cell invasion in breast cancer. Mol. Cancer 2014, 13, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Xue, X.; Wang, C.; Xue, Z.; Wen, J.; Han, J.; Ma, X.; Zang, X.; Deng, H.; Guo, R.; Asuquo, I.P.; et al. Exosomal miRNA profiling before and after surgery revealed potential diagnostic and prognostic markers for lung adenocarcinoma. Acta Biochim. Biophys. Sinica 2020, 52, 281–293. [Google Scholar] [CrossRef]
- Albino, D.; Falcione, M.; Uboldi, V.; Temilola, D.O.; Sandrini, G.; Merulla, J.; Civenni, G.; Kokanovic, A.; Stürchler, A.; Shinde, D.; et al. Circulating extracellular vesicles release oncogenic miR-424 in experimental models and patients with aggressive prostate cancer. Commun. Biol. 2021, 4, 119. [Google Scholar] [CrossRef]
- Shao, H.; Zhang, Y.; Yan, J.; Ban, X.; Fan, X.; Chang, X.; Lu, Z.; Wu, Y.; Zong, L.; Mo, S.; et al. Upregulated microRNA-483-3p is an early event in pancreatic ductal adenocarcinoma (PDAC) and as a powerful liquid biopsy biomarker in PDAC. OncoTargets Ther. 2021, 14, 2163. [Google Scholar] [CrossRef]
- Wang, J.; Liu, Y.; Li, Y.; Zheng, X.; Gan, J.; Wan, Z.; Zhang, J.; Liu, Y.; Wang, Y.; Hu, W.; et al. Exosomal-miR-10a derived from colorectal cancer cells suppresses migration of human lung fibroblasts, and expression of IL-6, IL-8 and IL-1β. Mol. Med. Rep. 2021, 23, 84. [Google Scholar] [CrossRef]
- Zhao, K.; Cheng, J.; Chen, B.; Liu, Q.; Xu, D.; Zhang, Y. Circulating microRNA-34 family low expression correlates with poor prognosis in patients with non-small cell lung cancer. J. Thorac. Dis. 2017, 9, 3735. [Google Scholar] [CrossRef] [Green Version]
- Asakura, K.; Kadota, T.; Matsuzaki, J.; Yoshida, Y.; Yamamoto, Y.; Nakagawa, K.; Takizawa, S.; Aoki, Y.; Nakamura, E.; Miura, J.; et al. A miRNA-based diagnostic model predicts resectable lung cancer in humans with high accuracy. Commun. Biol. 2020, 3, 134. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.-L.; Yao, J.-G.; Huang, X.-Y.; Wang, C.; Wu, X.-M.; Xia, Q.; Long, X.-D. Prognostic significance of miR-1268a expression and its beneficial effects for post-operative adjuvant transarterial chemoembolization in hepatocellular carcinoma. Sci. Rep. 2016, 6, 36104. [Google Scholar] [CrossRef]
- Cavallari, I.; Ciccarese, F.; Sharova, E.; Urso, L.; Raimondi, V.; Silic-Benussi, M.; D’Agostino, D.M.; Ciminale, V. The miR-200 Family of microRNAs: Fine Tuners of Epithelial-Mesenchymal Transition and Circulating Cancer Biomarkers. Cancers 2021, 13, 5874. [Google Scholar] [CrossRef]
- Halvorsen, A.R.; Bjaanæs, M.; LeBlanc, M.; Holm, A.M.; Bolstad, N.; Rubio, L.; Peñalver, J.C.; Cervera, J.; Mojarrieta, J.C.; López-Guerrero, J.A.; et al. A unique set of 6 circulating microRNAs for early detection of non-small cell lung cancer. Oncotarget 2016, 7, 37250. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Todd, N.W.; Xing, L.; Xie, Y.; Zhang, H.; Liu, Z.; Fang, H.; Zhang, J.; Katz, R.L.; Jiang, F. Early detection of lung adenocarcinoma in sputum by a panel of microRNA markers. Int. J. Cancer 2010, 127, 2870–2878. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Wang, Y.; Zou, Y.-Q.; Chen, X.; Huang, B.; Liu, J.; Xu, Y.-M.; Li, J.; Zhang, J.; Yang, W.-M.; et al. Differential miRNA expression in pleural effusions derived from extracellular vesicles of patients with lung cancer, pulmonary tuberculosis, or pneumonia. Tumor Biol. 2016, 37, 15835–15845. [Google Scholar] [CrossRef]
- Zhu, J.; Zeng, Y.; Xu, C.; Qin, H.; Lei, Z.; Shen, D.; Liu, Z.; Huang, J.-A. Expression profile analysis of microRNAs and downregulated miR-486-5p and miR-30a-5p in non-small cell lung cancer. Oncol. Rep. 2015, 34, 1779–1786. [Google Scholar] [CrossRef] [Green Version]
- Du, W.; Tang, H.; Lei, Z.; Zhu, J.; Zeng, Y.; Liu, Z.; Huang, J.-A. miR-335-5p inhibits TGF-β1-induced epithelial–mesenchymal transition in non-small cell lung cancer via ROCK1. Respir. Res. 2019, 20, 225. [Google Scholar] [CrossRef] [Green Version]
- Huo, W.; Zhang, M.; Li, C.; Wang, X.; Zhang, X.; Yang, X.; Fei, H. Correlation of microRNA-335 expression level with clinical significance and prognosis in non-small cell lung cancer. Medicine 2020, 99, e21369. [Google Scholar] [CrossRef]
- Han, Z.; Li, Y.; Zhang, J.; Guo, C.; Li, Q.; Zhang, X.; Lan, Y.; Gu, W.; Xing, Z.; Liang, L.; et al. Tumor-derived circulating exosomal miR-342-5p and miR-574-5p as promising diagnostic biomarkers for early-stage Lung Adenocarcinoma. Int. J. Med. Sci. 2020, 17, 1428. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, J.; Zhu, J.; Zhang, S. Hypoxic non-small-cell lung cancer cell-secreted exosomal microRNA-582-3p drives cancer cell malignant phenotypes by targeting secreted frizzled-related protein 1. Cancer Manag. Res. 2020, 12, 10151. [Google Scholar] [CrossRef]
- Zhou, J.; Wang, H.; Sun, Q.; Liu, X.; Wu, Z.; Wang, X.; Fang, W.; Ma, Z. miR-224-5p-enriched exosomes promote tumorigenesis by directly targeting androgen receptor in non-small cell lung cancer. Mol. Ther.-Nucleic Acids 2021, 23, 1217–1228. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, Y.-M.; Zou, Y.-Q.; Lin, J.; Huang, B.; Liu, J.; Li, J.; Zhang, J.; Yang, W.-M.; Min, Q.-H.; et al. Identification of differential expressed PE exosomal miRNA in lung adenocarcinoma, tuberculosis, and other benign lesions. Medicine. 2017, 96, e8361. [Google Scholar] [CrossRef]
- Poroyko, V.; Mirzapoiazova, T.; Nam, A.; Mambetsariev, I.; Mambetsariev, B.; Wu, X.; Husain, A.; Vokes, E.E.; Wheeler, D.L.; Salgia, R. Exosomal miRNAs species in the blood of small cell and non-small cell lung cancer patients. Oncotarget 2018, 9, 19793. [Google Scholar] [CrossRef] [Green Version]
- Liang, J.; Sun, T.; Wang, G.; Zhang, H. Clinical significance and functions of miR-203a-3p/AVL9 axis in human non-small-cell lung cancer. Pers. Med. 2020, 17, 271–282. [Google Scholar] [CrossRef]
- Takano, Y.; Masuda, T.; Iinuma, H.; Yamaguchi, R.; Sato, K.; Tobo, T.; Hirata, H.; Kuroda, Y.; Nambara, S.; Hayashi, N.; et al. Circulating exosomal microRNA-203 is associated with metastasis possibly via inducing tumor-associated macrophages in colorectal cancer. Oncotarget 2017, 8, 78598. [Google Scholar] [CrossRef] [Green Version]
- Lázaro-Ibáñez, E.; Sanz-Garcia, A.; Visakorpi, T.; Escobedo-Lucea, C.; Siljander, P.; Ayuso-Sacido, Á.; Yliperttula, M. Different gDNA content in the subpopulations of prostate cancer extracellular vesicles: Apoptotic bodies, microvesicles, and exosomes. Prostate 2014, 74, 1379–1390. [Google Scholar] [CrossRef]
- Castellano, J.J.; Canals, J.; Han, B.; Díaz, T.; Monzo, M.; Navarro, A. LncRNA Quantification from Extracellular Vesicles Isolated from Blood Plasma or Conditioned Media. In Long Non-Coding RNAs in Cancer; Springer: New York, NY, USA, 2021; pp. 285–304. [Google Scholar]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-tile: A new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Subtypes | Non-Relapsed Patients n (%) | Relapsed Patients n (%) | p-Value |
|---|---|---|---|---|
| Sex | Male | 6 (66.7) | 5 (55.6) | |
| Female | 3 (33.3) | 4 (44.4) | 1.0 | |
| Age, years | Mean age (range) | 61 (33–79) | 64 (36–80) | 0.287 |
| ≤65 | 7 (77.8) | 4 (44.4) | ||
| >65 | 2 (22.2) | 5 (55.6) | 0.33 | |
| Stage | I | 2 (22.2) | 0 (0) | |
| II | 5 (55.6) | 7 (77.8) | ||
| III | 2 (22.2) | 2 (22.2) | 0.6315 | |
| Histological subtype | Adenocarcinoma | 7 (77.8) | 8 (88.9) | |
| Squamous cell carcinoma | 2 (22.2) | 1 (11.1) | 1.0 | |
| ECOG PS a | 0 | 4 (44.4) | 3 (33.3) | |
| 1 | 5 (55.6) | 6 (66.7) | 1.0 | |
| Adjuvant treatment | Yes | 6 (66.7) | 6 (66.7) | |
| No | 3 (33.3) | 3 (33.3) | 0.6171 | |
| Type of surgery | Lobectomy/bilobectomy | 4 (44.4) | 8 (88.9) | |
| Pneumonectomy | 3 (33.3) | 1 (11.1) | ||
| Segmentectomy | 2 (22.2) | 0 (0) | 0.4543 | |
| Smoking history | Current smoker | 8 (88.9) | 2 (22.2) | |
| Former smoker | 1 (11.1) | 4 (44.4) | ||
| Never a smoker | 0 (0) | 3 (33.3) | 0.1615 |
| miRNA Name | Log Fold Change | p-Value | Average TMM in Relapsed Patients | Average TMM in Non-Relapsed Patients |
|---|---|---|---|---|
| hsa-miR-203a-3p | 1.6505 | 0.0067 | 2575.19 | 822.31 |
| hsa-miR-335-5p | −1.2313 | 0.0245 | 599.65 | 1403.15 |
| hsa-miR-34a-5p | −1.6527 | 0.0259 | 150.19 | 468.98 |
| hsa-miR-141-3p | −1.3132 | 0.0216 | 134.64 | 333.56 |
| hsa-miR-200c-3p | −1.4133 | 0.0141 | 91.94 | 244.24 |
| hsa-miR-200a-3p | −1.6506 | 0.0200 | 66.97 | 207.77 |
| hsa-miR-200b-3p | −1.5803 | 0.0220 | 56.13 | 165.26 |
| hsa-miR-335-3p | −1.9874 | 0.0029 | 34.92 | 134.76 |
| hsa-miR-224-5p | −1.3333 | 0.0285 | 38.74 | 93.53 |
| hsa-miR-424-5p | 1.0711 | 0.0146 | 66.23 | 29.7 |
| hsa-miR-483-3p | 1.5310 | 0.0144 | 52.39 | 19.38 |
| hsa-miR-429 | −2.0576 | 0.0089 | 10.66 | 44.39 |
| hsa-miR-574-5p | −2.0495 | 0.0038 | 8.68 | 35.4 |
| hsa-miR-10b-3p | 1.6994 | 0.0179 | 35.94 | 12.57 |
| hsa-miR-10a-3p | −1.9308 | 0.0069 | 7.83 | 29.45 |
| hsa-miR-1268b | −1.6110 | 0.0228 | 4.29 | 15.36 |
| hsa-miR-582-3p | −1.9282 | 0.0211 | 2.77 | 12.93 |
| Characteristics | Subtypes | n (%) | TTR |
|---|---|---|---|
| Sex | Male | 51 (72.9) | |
| Female | 19 (27.1) | 0.927 | |
| Age, years | Mean age (range) | 64 (32–79) | |
| ≤65 | 36 (51.4) | ||
| >65 | 34 (48.6) | 0.862 | |
| Stage | I | 38 (54.3) | |
| II | 25 (35.7) | ||
| III | 7 (10) | 0.007 | |
| Lymph node involvement | N0 | 53 (75.7) | |
| N+ | 17 (24.3) | 0.001 | |
| Histological subtype | Adenocarcinoma | 49 (70) | |
| Squamous cell carcinoma | 17 (24.3) | ||
| Other | 4 (5.7) | 0.530 | |
| ECOG PS a | 0 | 24 (34.3) | |
| 1 | 44 (62.9) | ||
| 2 | 2 (2.9) | 0.018 | |
| Adjuvant treatment | Yes | 24 (34.3) | |
| No | 46 (65.7) | 0.044 | |
| Relapse | Yes | 25 (35.7) | |
| No | 45 (64.3) | - | |
| Type of surgery | Lobectomy/bilobectomy | 51 (72.9) | |
| Pneumonectomy | 8 (11.4) | ||
| Atypical resection | 6 (8.6) | ||
| Segmentectomy | 5 (7.1) | 0.811 | |
| Smoking history | Current smoker | 34 (48.6) | |
| Former smoker | 31 (44.3) | ||
| Never a smoker | 5 (7.1) | 0.504 |
| Time to Relapse | Hazard Ratio (95%CI) | p |
|---|---|---|
| Stage I assay | 0.174 (0.056–0.543) | 0.003 |
| ECOG PS 0 | 0.360 (0.068–1.912) | 0.230 |
| No adjuvant treatment | 1.375 (0.407–4.646) | 0.609 |
| TDV EV-miR-203a-3p | 2.442 (1.126–5.294) | 0.024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, B.; Molins, L.; He, Y.; Viñolas, N.; Sánchez-Lorente, D.; Boada, M.; Guirao, A.; Díaz, T.; Martinez, D.; Ramirez, J.; et al. Characterization of the MicroRNA Cargo of Extracellular Vesicles Isolated from a Pulmonary Tumor-Draining Vein Identifies miR-203a-3p as a Relapse Biomarker for Resected Non-Small Cell Lung Cancer. Int. J. Mol. Sci. 2022, 23, 7138. https://doi.org/10.3390/ijms23137138
Han B, Molins L, He Y, Viñolas N, Sánchez-Lorente D, Boada M, Guirao A, Díaz T, Martinez D, Ramirez J, et al. Characterization of the MicroRNA Cargo of Extracellular Vesicles Isolated from a Pulmonary Tumor-Draining Vein Identifies miR-203a-3p as a Relapse Biomarker for Resected Non-Small Cell Lung Cancer. International Journal of Molecular Sciences. 2022; 23(13):7138. https://doi.org/10.3390/ijms23137138
Chicago/Turabian StyleHan, Bing, Laureano Molins, Yangyi He, Nuria Viñolas, David Sánchez-Lorente, Marc Boada, Angela Guirao, Tania Díaz, Daniel Martinez, Jose Ramirez, and et al. 2022. "Characterization of the MicroRNA Cargo of Extracellular Vesicles Isolated from a Pulmonary Tumor-Draining Vein Identifies miR-203a-3p as a Relapse Biomarker for Resected Non-Small Cell Lung Cancer" International Journal of Molecular Sciences 23, no. 13: 7138. https://doi.org/10.3390/ijms23137138