
Janus Kinase Inhibitors Improve Disease Activity and Patient-Reported Outcomes in Rheumatoid Arthritis: A Systematic Review and Meta-Analysis of 24,135 Patients

 , ,
, ,
Abstract
:1. Introduction
2. Results
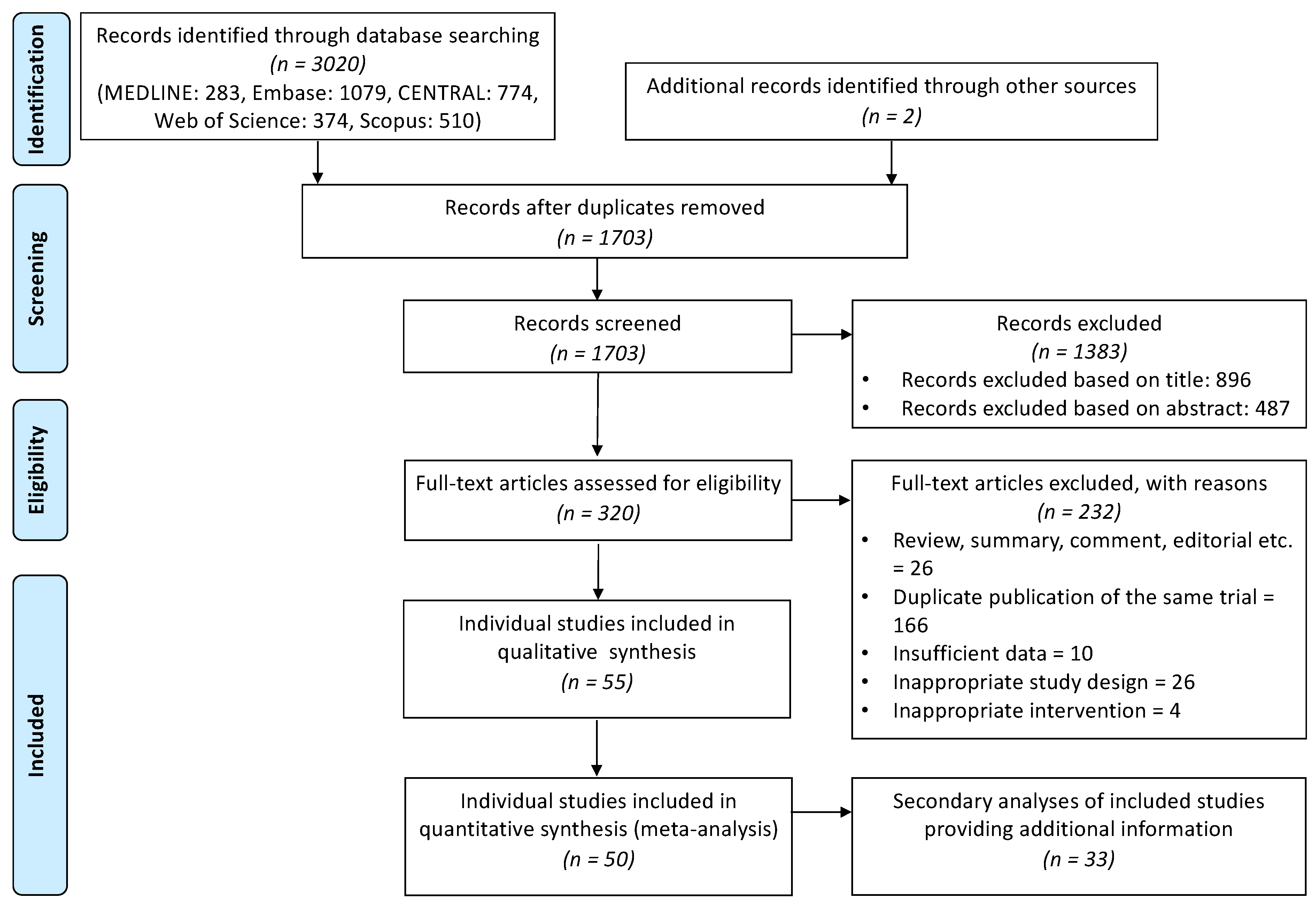
2.1. Description of the Studies
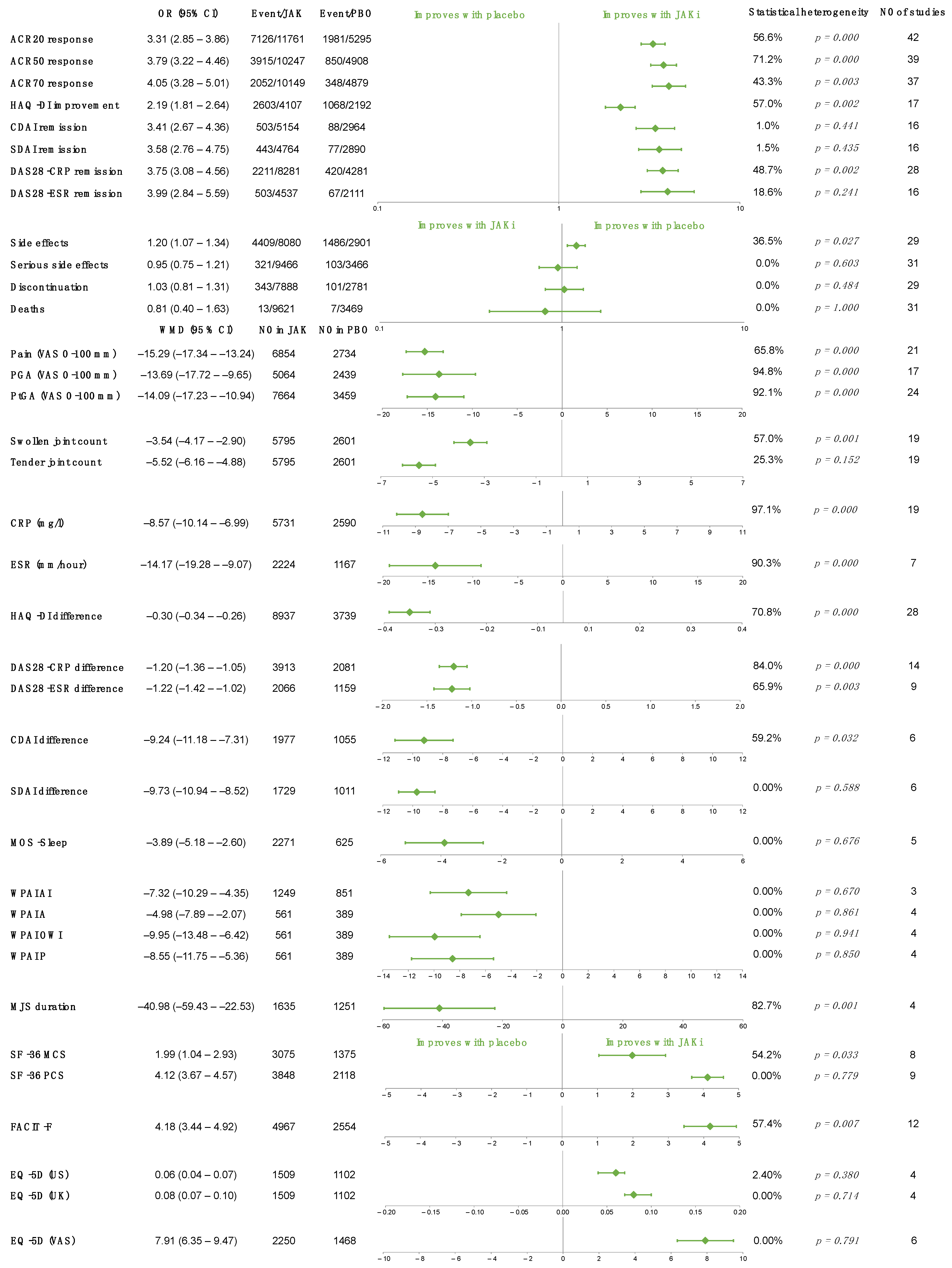
2.2. JAK Inhibitors vs. Placebo
2.3. JAK Inhibitors vs. MTX
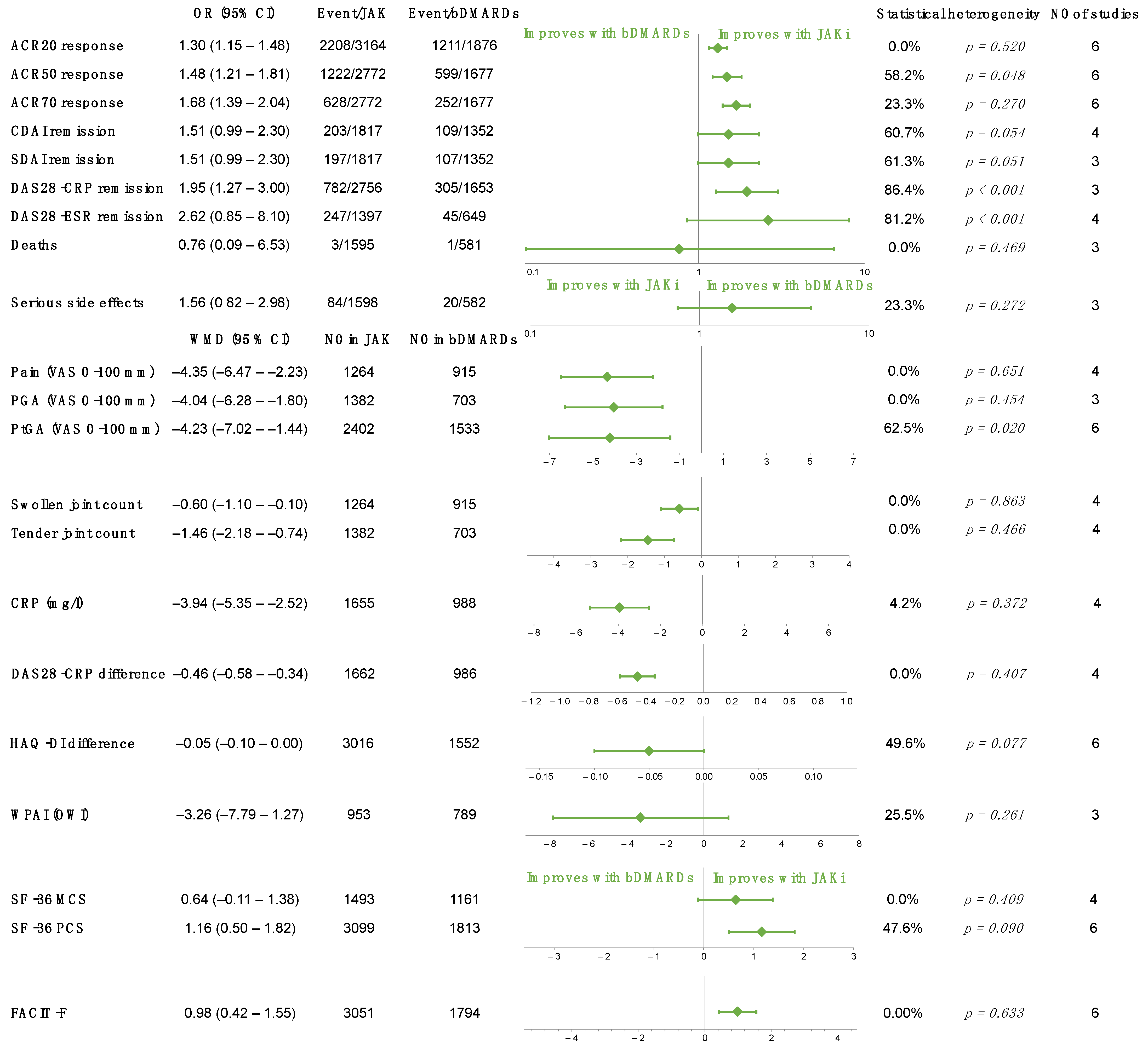
2.4. JAK Inhibitors vs. bDMARDs
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.2. Selection Criteria
4.3. Selection Process and Data Extraction
4.4. Statistical Analysis
4.5. Assessment of Risk of Bias and the Quality/Certainty of Evidence
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; Barton, A.; Burmester, G.R.; Emery, P.; Firestein, G.S.; Kavanaugh, A.; McInnes, I.B.; Solomon, D.H.; Strand, V.; et al. Rheumatoid arthritis. Nat. Rev. Dis. Primers 2018, 4, 18001. [Google Scholar] [CrossRef]
- Smolen, J.S.; Breedveld, F.C.; Burmester, G.R.; Bykerk, V.; Dougados, M.; Emery, P.; Kvien, T.K.; Navarro-Compán, M.V.; Oliver, S.; Schoels, M.; et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann. Rheum. Dis. 2016, 75, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Landewé, R.B.M.; Bijlsma, J.W.J.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; McInnes, I.B.; Sepriano, A.; van Vollenhoven, R.F.; de Wit, M.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann. Rheum. Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef] [Green Version]
- Nagy, G.; Roodenrijs, N.M.T.; Welsing, P.M.; Kedves, M.; Hamar, A.; van der Goes, M.C.; Kent, A.; Bakkers, M.; Blaas, E.; Senolt, L.; et al. EULAR definition of difficult-to-treat rheumatoid arthritis. Ann. Rheum. Dis. 2021, 80, 31–35. [Google Scholar] [CrossRef]
- Buch, M.H.; Eyre, S.; McGonagle, D. Persistent inflammatory and non-inflammatory mechanisms in refractory rheumatoid arthritis. Nat. Rev. Rheumatol. 2021, 17, 17–33. [Google Scholar] [CrossRef]
- Hu, X.; Li, J.; Fu, M.; Zhao, X.; Wang, W. The JAK/STAT signaling pathway: From bench to clinic. Signal Transduct. Target. Ther. 2021, 6, 402. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.M.; Kanno, Y.; Villarino, A.; Ward, M.; Gadina, M.; O’Shea, J.J. JAK inhibition as a therapeutic strategy for immune and inflammatory diseases. Nat. Rev. Drug Discov. 2017, 16, 843–862. [Google Scholar] [CrossRef]
- Simon, L.S.; Taylor, P.C.; Choy, E.H.; Sebba, A.; Quebe, A.; Knopp, K.L.; Porreca, F. The Jak/STAT pathway: A focus on pain in rheumatoid arthritis. Semin. Arthritis Rheum. 2021, 51, 278–284. [Google Scholar] [CrossRef]
- Fraenkel, L.; Bathon, J.M.; England, B.R.; St. Clair, E.W.; Arayssi, T.; Carandang, K.; Deane, K.D.; Genovese, M.; Huston, K.K.; Kerr, G.; et al. 2021 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Care Res. 2021, 73, 924–939. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Saag, K.G.; Bridges, S.L., Jr.; Akl, E.A.; Bannuru, R.R.; Sullivan, M.C.; Vaysbrot, E.; McNaughton, C.; Osani, M.; Shmerling, R.H.; et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Care Res. 2016, 68, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Heijde, D.; Tanaka, Y.; Fleischmann, R.; Keystone, E.; Kremer, J.; Zerbini, C.; Cardiel, M.H.; Cohen, S.; Nash, P.; Song, Y.W.; et al. Tofacitinib (CP-690,550) in patients with rheumatoid arthritis receiving methotrexate: Twelve-month data from a twenty-four-month phase III randomized radiographic study. Arthritis Rheum. 2013, 65, 559–570. [Google Scholar] [CrossRef]
- van Vollenhoven, R.F.; Fleischmann, R.; Cohen, S.; Lee, E.B.; García Meijide, J.A.; Wagner, S.; Forejtova, S.; Zwillich, S.H.; Gruben, D.; Koncz, T.; et al. Tofacitinib or adalimumab versus placebo in rheumatoid arthritis. N. Engl. J. Med. 2012, 367, 508–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kremer, J.; Li, Z.G.; Hall, S.; Fleischmann, R.; Genovese, M.; Martin-Mola, E.; Isaacs, J.D.; Gruben, D.; Wallenstein, G.; Krishnaswami, S.; et al. Tofacitinib in combination with nonbiologic disease-modifying antirheumatic drugs in patients with active rheumatoid arthritis: A randomized trial. Ann. Intern. Med. 2013, 159, 253–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burmester, G.R.; Blanco, R.; Charles-Schoeman, C.; Wollenhaupt, J.; Zerbini, C.; Benda, B.; Gruben, D.; Wallenstein, G.; Krishnaswami, S.; Zwillich, S.H.; et al. Tofacitinib (CP-690,550) in combination with methotrexate in patients with active rheumatoid arthritis with an inadequate response to tumour necrosis factor inhibitors: A randomised phase 3 trial. Lancet 2013, 381, 451–460. [Google Scholar] [CrossRef]
- Fleischmann, R.; Kremer, J.; Cush, J.; Schulze-Koops, H.; Connell, C.A.; Bradley, J.D.; Gruben, D.; Wallenstein, G.V.; Zwillich, S.H.; Kanik, K.S. Placebo-controlled trial of tofacitinib monotherapy in rheumatoid arthritis. N. Engl. J. Med. 2012, 367, 495–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleischmann, R.; Mysler, E.; Hall, S.; Kivitz, A.J.; Moots, R.J.; Luo, Z.; DeMasi, R.; Soma, K.; Zhang, R.; Takiya, L.; et al. Efficacy and safety of tofacitinib monotherapy, tofacitinib with methotrexate, and adalimumab with methotrexate in patients with rheumatoid arthritis (ORAL Strategy): A phase 3b/4, double-blind, head-to-head, randomised controlled trial. Lancet 2017, 390, 457–468. [Google Scholar] [CrossRef]
- Fleischmann, R.; Cutolo, M.; Genovese, M.C.; Lee, E.B.; Kanik, K.S.; Sadis, S.; Connell, C.A.; Gruben, D.; Krishnaswami, S.; Wallenstein, G.; et al. Phase IIb dose-ranging study of the oral JAK inhibitor tofacitinib (CP-690,550) or adalimumab monotherapy versus placebo in patients with active rheumatoid arthritis with an inadequate response to disease-modifying antirheumatic drugs. Arthritis Rheum. 2012, 64, 617–629. [Google Scholar] [CrossRef]
- Nakamura, Y.; Suzuki, T.; Yamazaki, H.; Kato, H. Tofacitinib Versus Non-Tumor Necrosis Factor Biologics for Patients With Active Rheumatoid Arthritis. Arch. Rheumatol. 2018, 33, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Boyle, D.L.; Soma, K.; Hodge, J.; Kavanaugh, A.; Mandel, D.; Mease, P.; Shurmur, R.; Singhal, A.K.; Wei, N.; Rosengren, S.; et al. The JAK inhibitor tofacitinib suppresses synovial JAK1-STAT signalling in rheumatoid arthritis. Ann. Rheum. Dis. 2015, 74, 1311–1316. [Google Scholar] [CrossRef] [Green Version]
- Kremer, J.M.; Bloom, B.J.; Breedveld, F.C.; Coombs, J.H.; Fletcher, M.P.; Gruben, D.; Krishnaswami, S.; Burgos-Vargas, R.; Wilkinson, B.; Zerbini, C.A.; et al. The safety and efficacy of a JAK inhibitor in patients with active rheumatoid arthritis: Results of a double-blind, placebo-controlled phase IIa trial of three dosage levels of CP-690,550 versus placebo. Arthritis Rheum. 2009, 60, 1895–1905. [Google Scholar] [CrossRef]
- Kremer, J.M.; Cohen, S.; Wilkinson, B.E.; Connell, C.A.; French, J.L.; Gomez-Reino, J.; Gruben, D.; Kanik, K.S.; Krishnaswami, S.; Pascual-Ramos, V.; et al. A phase IIb dose-ranging study of the oral JAK inhibitor tofacitinib (CP-690,550) versus placebo in combination with background methotrexate in patients with active rheumatoid arthritis and an inadequate response to methotrexate alone. Arthritis Rheum. 2012, 64, 970–981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, Y.; Suzuki, M.; Nakamura, H.; Toyoizumi, S.; Zwillich, S.H. Phase II study of tofacitinib (CP-690,550) combined with methotrexate in patients with rheumatoid arthritis and an inadequate response to methotrexate. Arthritis Care Res. 2011, 63, 1150–1158. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Takeuchi, T.; Yamanaka, H.; Nakamura, H.; Toyoizumi, S.; Zwillich, S. Efficacy and safety of tofacitinib as monotherapy in Japanese patients with active rheumatoid arthritis: A 12-week, randomized, phase 2 study. Mod. Rheumatol. 2015, 25, 514–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, P.C.; Keystone, E.C.; van der Heijde, D.; Weinblatt, M.E.; Del Carmen Morales, L.; Reyes Gonzaga, J.; Yakushin, S.; Ishii, T.; Emoto, K.; Beattie, S.; et al. Baricitinib versus Placebo or Adalimumab in Rheumatoid Arthritis. N. Engl. J. Med. 2017, 376, 652–662. [Google Scholar] [CrossRef]
- Genovese, M.C.; Kremer, J.; Zamani, O.; Ludivico, C.; Krogulec, M.; Xie, L.; Beattie, S.D.; Koch, A.E.; Cardillo, T.E.; Rooney, T.P.; et al. Baricitinib in Patients with Refractory Rheumatoid Arthritis. N. Engl. J. Med. 2016, 374, 1243–1252. [Google Scholar] [CrossRef]
- Dougados, M.; Van Der Heijde, D.; Chen, Y.C.; Greenwald, M.; Drescher, E.; Liu, J.; Beattie, S.; De La Torre, I.; Rooney, T.; Schlichting, D.; et al. Baricitinib, an oral janus kinase (jak)1/jak2 inhibitor, in patients with active rheumatoid arthritis (RA) and an inadequate response to cDMARD therapy: Results of the phase 3 Ra-build study. Ann. Rheum. Dis. 2015, 74, 79–80. [Google Scholar] [CrossRef]
- Li, Z.; Hu, J.; Bao, C.; Li, X.; Li, X.; Xu, J.; Spindler, A.J.; Zhang, X.; Xu, J.; He, D.; et al. Baricitinib in patients with rheumatoid arthritis with inadequate response to methotrexate: Results from a phase 3 study. Clin. Exp. Rheumatol. 2020, 38, 732–741. [Google Scholar] [PubMed]
- Keystone, E.C.; Taylor, P.C.; Drescher, E.; Schlichting, D.E.; Beattie, S.D.; Berclaz, P.Y.; Lee, C.H.; Fidelus-Gort, R.K.; Luchi, M.E.; Rooney, T.P.; et al. Safety and efficacy of baricitinib at 24 weeks in patients with rheumatoid arthritis who have had an inadequate response to methotrexate. Ann. Rheum. Dis. 2015, 74, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Emoto, K.; Cai, Z.; Aoki, T.; Schlichting, D.; Rooney, T.; Macias, W. Efficacy and Safety of Baricitinib in Japanese Patients with Active Rheumatoid Arthritis Receiving Background Methotrexate Therapy: A 12-week, Double-blind, Randomized Placebo-controlled Study. J. Rheumatol. 2016, 43, 504–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenwald, M.W.; Fidelus-Gort, R.; Levy, R.; Liang, J.; Vaddi, K.; Williams, W.V.; Newton, R. A randomized dose-ranging, placebo-controlled study of INCB028050, a selective JAK1 and JAK2 inhibitor in subjects with active rheumatoid arthritis. Arthritis Rheum. 2010, 62, 2172. [Google Scholar] [CrossRef]
- Smolen, J.S.; Pangan, A.L.; Emery, P.; Rigby, W.; Tanaka, Y.; Vargas, J.I.; Zhang, Y.; Damjanov, N.; Friedman, A.; Othman, A.A.; et al. Upadacitinib as monotherapy in patients with active rheumatoid arthritis and inadequate response to methotrexate (SELECT-MONOTHERAPY): A randomised, placebo-controlled, double-blind phase 3 study. Lancet 2019, 393, 2303–2311. [Google Scholar] [CrossRef]
- Fleischmann, R.; Pangan, A.L.; Song, I.H.; Mysler, E.; Bessette, L.; Peterfy, C.; Durez, P.; Ostor, A.J.; Li, Y.; Zhou, Y.; et al. Upadacitinib Versus Placebo or Adalimumab in Patients With Rheumatoid Arthritis and an Inadequate Response to Methotrexate: Results of a Phase III, Double-Blind, Randomized Controlled Trial. Arthritis Rheumatol. 2019, 71, 1788–1800. [Google Scholar] [CrossRef] [PubMed]
- Burmester, G.R.; Kremer, J.M.; Van den Bosch, F.; Kivitz, A.; Bessette, L.; Li, Y.; Zhou, Y.; Othman, A.A.; Pangan, A.L.; Camp, H.S. Safety and efficacy of upadacitinib in patients with rheumatoid arthritis and inadequate response to conventional synthetic disease-modifying anti-rheumatic drugs (SELECT-NEXT): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2018, 391, 2503–2512. [Google Scholar] [CrossRef]
- Genovese, M.C.; Smolen, J.S.; Weinblatt, M.E.; Burmester, G.R.; Meerwein, S.; Camp, H.S.; Wang, L.; Othman, A.A.; Khan, N.; Pangan, A.L.; et al. Efficacy and Safety of ABT-494, a Selective JAK-1 Inhibitor, in a Phase IIb Study in Patients With Rheumatoid Arthritis and an Inadequate Response to Methotrexate. Arthritis Rheumatol. 2016, 68, 2857–2866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kremer, J.M.; Emery, P.; Camp, H.S.; Friedman, A.; Wang, L.; Othman, A.A.; Khan, N.; Pangan, A.L.; Jungerwirth, S.; Keystone, E.C. A Phase IIb Study of ABT-494, a Selective JAK-1 Inhibitor, in Patients With Rheumatoid Arthritis and an Inadequate Response to Anti-Tumor Necrosis Factor Therapy. Arthritis Rheumatol. 2016, 68, 2867–2877. [Google Scholar] [CrossRef] [PubMed]
- Genovese, M.C.; Fleischmann, R.; Combe, B.; Hall, S.; Rubbert-Roth, A.; Zhang, Y.; Zhou, Y.; Mohamed, M.F.; Meerwein, S.; Pangan, A.L. Safety and efficacy of upadacitinib in patients with active rheumatoid arthritis refractory to biologic disease-modifying anti-rheumatic drugs (SELECT-BEYOND): A double-blind, randomised controlled phase 3 trial. Lancet 2018, 391, 2513–2524. [Google Scholar] [CrossRef]
- Rubbert-Roth, A.; Enejosa, J.; Pangan, A.L.; Haraoui, B.; Rischmueller, M.; Khan, N.; Zhang, Y.; Martin, N.; Xavier, R.M. Trial of Upadacitinib or Abatacept in Rheumatoid Arthritis. N. Engl. J. Med. 2020, 383, 1511–1521. [Google Scholar] [CrossRef]
- Kameda, H.; Takeuchi, T.; Yamaoka, K.; Oribe, M.; Kawano, M.; Zhou, Y.; Othman, A.A.; Pangan, A.L.; Kitamura, S.; Meerwein, S.; et al. Efficacy and safety of upadacitinib in Japanese patients with rheumatoid arthritis (SELECT-SUNRISE): A placebo-controlled phase IIb/III study. Rheumatology 2020, 59, 3303–3313. [Google Scholar] [CrossRef] [PubMed]
- Combe, B.; Kivitz, A.; Tanaka, Y.; Van Der Heijde, D.; Matzkies, F.; Bartok, B.; Ye, L.; Guo, Y.; Tasset, C.; Sundy, J.; et al. Efficacy and safety of filgotinib for patients with rheumatoid arthritis with inadequate response to methotrexate: FINCH1 primary outcome results. Arthritis Rheumatol. 2019, 71, 849–851. [Google Scholar] [CrossRef]
- Genovese, M.C.; Kalunian, K.; Gottenberg, J.-E.; Mozaffarian, N.; Bartok, B.; Matzkies, F.; Gao, J.; Guo, Y.; Tasset, C.; Sundy, J.S.; et al. Effect of Filgotinib vs Placebo on Clinical Response in Patients With Moderate to Severe Rheumatoid Arthritis Refractory to Disease-Modifying Antirheumatic Drug Therapy: The FINCH 2 Randomized Clinical Trial. JAMA 2019, 322, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, A.; Kremer, J.; Ponce, L.; Cseuz, R.; Reshetko, O.V.; Stanislavchuk, M.; Greenwald, M.; Van der Aa, A.; Vanhoutte, F.; Tasset, C.; et al. Filgotinib (GLPG0634/GS-6034), an oral selective JAK1 inhibitor, is effective as monotherapy in patients with active rheumatoid arthritis: Results from a randomised, dose-finding study (DARWIN 2). Ann. Rheum. Dis. 2017, 76, 1009–1019. [Google Scholar] [CrossRef] [PubMed]
- Westhovens, R.; Taylor, P.C.; Alten, R.; Pavlova, D.; Enríquez-Sosa, F.; Mazur, M.; Greenwald, M.; Van der Aa, A.; Vanhoutte, F.; Tasset, C.; et al. Filgotinib (GLPG0634/GS-6034), an oral JAK1 selective inhibitor, is effective in combination with methotrexate (MTX) in patients with active rheumatoid arthritis and insufficient response to MTX: Results from a randomised, dose-finding study (DARWIN 1). Ann. Rheum. Dis. 2017, 76, 998–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genovese, M.C.; Greenwald, M.; Codding, C.; Zubrzycka-Sienkiewicz, A.; Kivitz, A.J.; Wang, A.; Shay, K.; Wang, X.; Garg, J.P.; Cardiel, M.H. Peficitinib, a JAK Inhibitor, in Combination With Limited Conventional Synthetic Disease-Modifying Antirheumatic Drugs in the Treatment of Moderate-to-Severe Rheumatoid Arthritis. Arthritis Rheumatol. 2017, 69, 932–942. [Google Scholar] [CrossRef] [PubMed]
- Kivitz, A.J.; Gutierrez-Ureña, S.R.; Poiley, J.; Genovese, M.C.; Kristy, R.; Shay, K.; Wang, X.; Garg, J.P.; Zubrzycka-Sienkiewicz, A. Peficitinib, a JAK Inhibitor, in the Treatment of Moderate-to-Severe Rheumatoid Arthritis in Patients With an Inadequate Response to Methotrexate. Arthritis Rheumatol. 2017, 69, 709–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeuchi, T.; Tanaka, Y.; Tanaka, S.; Kawakami, A.; Iwasaki, M.; Katayama, K.; Rokuda, M.; Izutsu, H.; Ushijima, S.; Kaneko, Y.; et al. Efficacy and safety of peficitinib (ASP015K) in patients with rheumatoid arthritis and an inadequate response to methotrexate: Results of a phase III randomised, double-blind, placebo-controlled trial (RAJ4) in Japan. Ann. Rheum. Dis. 2019, 78, 1305–1319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, Y.; Takeuchi, T.; Tanaka, S.; Kawakami, A.; Iwasaki, M.; Song, Y.W.; Chen, Y.H.; Wei, J.C.; Lee, S.H.; Rokuda, M.; et al. Efficacy and safety of peficitinib (ASP015K) in patients with rheumatoid arthritis and an inadequate response to conventional DMARDs: A randomised, double-blind, placebo-controlled phase III trial (RAJ3). Ann. Rheum. Dis. 2019, 78, 1320–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genovese, M.C.; van Vollenhoven, R.F.; Pacheco-Tena, C.; Zhang, Y.; Kinnman, N. VX-509 (Decernotinib), an Oral Selective JAK-3 Inhibitor, in Combination With Methotrexate in Patients With Rheumatoid Arthritis. Arthritis Rheumatol. 2016, 68, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Genovese, M.C.; Yang, F.; Østergaard, M.; Kinnman, N. Efficacy of VX-509 (decernotinib) in combination with a disease-modifying antirheumatic drug in patients with rheumatoid arthritis: Clinical and MRI findings. Ann. Rheum. Dis. 2016, 75, 1979–1983. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, R.M.; Damjanov, N.S.; Kivitz, A.J.; Legedza, A.; Hoock, T.; Kinnman, N. A randomized, double-blind, placebo-controlled, twelve-week, dose-ranging study of decernotinib, an oral selective JAK-3 inhibitor, as monotherapy in patients with active rheumatoid arthritis. Arthritis Rheumatol. 2015, 67, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.F.; Damjanov, N.; Stamenkovic, B.; Radunovic, G.; Kivitz, A.; Cox, L.; Manukyan, Z.; Banfield, C.; Saunders, M.; Chandra, D.; et al. Efficacy and Safety of PF-06651600 (Ritlecitinib), a Novel JAK3/TEC Inhibitor, in Patients With Moderate-to-Severe Rheumatoid Arthritis and an Inadequate Response to Methotrexate. Arthritis Rheumatol. 2020, 72, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Conaghan, P.G.; Østergaard, M.; Bowes, M.A.; Wu, C.; Fuerst, T.; van der Heijde, D.; Irazoque-Palazuelos, F.; Soto-Raices, O.; Hrycaj, P.; Xie, Z.; et al. Comparing the effects of tofacitinib, methotrexate and the combination, on bone marrow oedema, synovitis and bone erosion in methotrexate-naive, early active rheumatoid arthritis: Results of an exploratory randomised MRI study incorporating semiquantitative and quantitative techniques. Ann. Rheum. Dis. 2016, 75, 1024–1033. [Google Scholar] [CrossRef] [PubMed]
- van Vollenhoven, R.; Takeuchi, T.; Pangan, A.L.; Friedman, A.; Mohamed, M.E.F.; Chen, S.; Rischmueller, M.; Blanco, R.; Xavier, R.M.; Strand, V. Efficacy and Safety of Upadacitinib Monotherapy in Methotrexate-Naive Patients With Moderately-to-Severely Active Rheumatoid Arthritis (SELECT-EARLY): A Multicenter, Multi-Country, Randomized, Double-Blind, Active Comparator–Controlled Trial. Arthritis Rheumatol. 2020, 72, 1607–1620. [Google Scholar] [CrossRef] [PubMed]
- Westhovens, R.; Rigby, W.F.C.; Van Der Heijde, D.; Ching, D.W.T.; Bartok, B.; Matzkies, F.; Yin, Z.; Guo, Y.; Tasset, C.; Sundy, J.; et al. Efficacy and safety of filgotinib for patients with rheumatoid arthritis naïve to methotrexate therapy: FINCH3 primary outcome results. Arthritis Rheumatol. 2019, 71, 1606–1608. [Google Scholar] [CrossRef]
- Lee, E.B.; Fleischmann, R.; Hall, S.; Wilkinson, B.; Bradley, J.D.; Gruben, D.; Koncz, T.; Krishnaswami, S.; Wallenstein, G.V.; Zang, C.; et al. Tofacitinib versus methotrexate in rheumatoid arthritis. N. Engl. J. Med. 2014, 370, 2377–2386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleischmann, R.; Schiff, M.; van der Heijde, D.; Ramos-Remus, C.; Spindler, A.; Stanislav, M.; Zerbini, C.A.; Gurbuz, S.; Dickson, C.; de Bono, S.; et al. Baricitinib, Methotrexate, or Combination in Patients With Rheumatoid Arthritis and No or Limited Prior Disease-Modifying Antirheumatic Drug Treatment. Arthritis Rheumatol. 2017, 69, 506–517. [Google Scholar] [CrossRef]
- Takeuchi, T.; Tanaka, Y.; Iwasaki, M.; Ishikura, H.; Saeki, S.; Kaneko, Y. Efficacy and safety of the oral Janus kinase inhibitor peficitinib (ASP015K) monotherapy in patients with moderate to severe rheumatoid arthritis in Japan: A 12-week, randomised, double-blind, placebo-controlled phase IIb study. Ann. Rheum. Dis. 2016, 75, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Menshikova, I.; Dzhenzhera, N.; Pak, Y.; Kolosova, I. Comparison of efficacy of tofacitinib vs. etanercept treatment in rheumatoid arthtritis patients with high activity disease by ultrasound evaluation with power doppler (1 year treatment period). Ann. Rheum. Dis. 2018, 77, 976. [Google Scholar] [CrossRef]
- Vanhoutte, F.; Mazur, M.; Voloshyn, O.; Stanislavchuk, M.; Van der Aa, A.; Namour, F.; Galien, R.; Meuleners, L.; van’t Klooster, G. Efficacy, Safety, Pharmacokinetics, and Pharmacodynamics of Filgotinib, a Selective JAK-1 Inhibitor, After Short-Term Treatment of Rheumatoid Arthritis: Results of Two Randomized Phase IIa Trials. Arthritis Rheumatol. 2017, 69, 1949–1959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luchi, M.; Fidelus-Gort, R.; Douglas, D.; Zhang, H.; Flores, R.; Newton, R.; Scherle, P.; Yeleswaram, S.; Chen, X.; Sandor, V. A randomized, dose-ranging, placebo-controlled, 84-day study of INCB039110, a selective janus kinase-1 inhibitor, in patients with active rheumatoid arthritis. Arthritis Rheum. 2013, 65, S765–S766. [Google Scholar] [CrossRef]
- Dougados, M.; van der Heijde, D.; Chen, Y.C.; Greenwald, M.; Drescher, E.; Liu, J.; Beattie, S.; Witt, S.; de la Torre, I.; Gaich, C.; et al. Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: Results from the RA-BUILD study. Ann. Rheum. Dis. 2017, 76, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.; Genovese, M.; Keystone, E.C.; Drescher, E.; Berclaz, P.Y.; Lee, C.; Fidelus-Gort, R.; Schlichting, D.; Beattie, S.; Luchi, M.; et al. 24-Week results of a blinded phase IIB dose-ranging study of baricitinib, an oral JAK1/JAK2 inhibitor, in combination with traditional dmards in patients with rheumatoid arthritis. Rheumatology 2013, 52, i44–i45. [Google Scholar] [CrossRef] [Green Version]
- Smolen, J.S.; Schlichting, D.E.; Sterling, K.L.; Keystone, E.; Taylor, P.; Genovese, M.C.; Johnson, L.; Rizo Rodriguez, J.C.; Lee, C.H.; Gaich, C.L. 12-and 24-week patient-reported outcomes from a phase 2B dose-ranging study of baricitinib, an oral janus kinase 1/janus kinase 2 inhibitor, in combination with traditional disease-modifying antirheumatic drugs in patients with rheumatoid arthritis. Arthritis Rheum. 2012, 64, S214. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Hu, J.; Bao, C.; Li, X.; Li, X.; Xu, J.; Spindler, A.; Zhang, X.; Xu, J.; Li, Z.; et al. Efficacy and safety of baricitinib in MTX-IR patients with rheumatoid arthritis: 52 week results from a phase 3 study (RA-balance). Ann. Rheum. Dis. 2018, 77, 969–970. [Google Scholar] [CrossRef]
- Smolen, J.S.; Kremer, J.M.; Gaich, C.L.; DeLozier, A.M.; Schlichting, D.E.; Xie, L.; Stoykov, I.; Rooney, T.; Bird, P.; Sánchez Bursón, J.M.; et al. Patient-reported outcomes from a randomised phase III study of baricitinib in patients with rheumatoid arthritis and an inadequate response to biological agents (RA-BEACON). Ann. Rheum. Dis. 2017, 76, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Keystone, E.C.; Taylor, P.C.; Tanaka, Y.; Gaich, C.; DeLozier, A.M.; Dudek, A.; Zamora, J.V.; Cobos, J.A.C.; Rooney, T.; Bono, S.; et al. Patient-reported outcomes from a phase 3 study of baricitinib versus placebo or adalimumab in rheumatoid arthritis: Secondary analyses from the RA-BEAM study. Ann. Rheum. Dis. 2017, 76, 1853–1861. [Google Scholar] [CrossRef]
- Schiff, M.; Takeuchi, T.; Fleischmann, R.; Gaich, C.L.; DeLozier, A.M.; Schlichting, D.; Kuo, W.L.; Won, J.E.; Carmack, T.; Rooney, T.; et al. Patient-reported outcomes of baricitinib in patients with rheumatoid arthritis and no or limited prior disease-modifying antirheumatic drug treatment. Arthritis Res. Ther. 2017, 19, 208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiff, M.; Takeuchi, T.; Gaich, C.; DeLozier, A.M.; Schlichting, D.; Kuo, W.L.; Durez, P.; Carmack, T.; Won, J.E.; Fleischmann, R. Patient-reported outcomes from a phase 3 study of baricitinib in patients with early rheumatoid arthritis who had received limited or no treatment with disease-modifying anti-rheumatic drugs. Ann. Rheum. Dis. 2016, 75, 419. [Google Scholar] [CrossRef]
- Emery, P.; Blanco, R.; Maldonado Cocco, J.; Chen, Y.C.; Gaich, C.L.; DeLozier, A.M.; de Bono, S.; Liu, J.; Rooney, T.; Chang, C.H.; et al. Patient-reported outcomes from a phase III study of baricitinib in patients with conventional synthetic DMARD-refractory rheumatoid arthritis. RMD Open 2017, 3, e000410. [Google Scholar] [CrossRef] [PubMed]
- Strand, V.; Suthoff, E.; Fleischmann, R.M.; Vera-Llonch, M.; Jiang, J.; Zhang, Y.; Kinnman, N. Effects of VX-509, an investigational oral selective janus kinase 3 (JAK3) inhibitor, on patient-reported outcomes in a phase 2A study of patients with active rheumatoid arthritis. Arthritis Rheum. 2013, 65, S1004–S1005. [Google Scholar] [CrossRef] [Green Version]
- Genovese, M.C.; Van Vollenhoven, R.; Bloom, B.J.; Jiang, J.G.; Kinnman, N. A phase 2B, 12-week study of VX-509, an oral selective janus kinase 3 inhibitor, in combination with background methotrexate in rheumatoid arthritis. Arthritis Rheum. 2013, 65, 3320. [Google Scholar] [CrossRef]
- Genovese, M.C.; Greenwald, M.; Codding, C.; Cardiel, M.H.; Zubrzycka-Sienkiewicz, A.; Kivitz, A.J.; Wisseh, S.; Shay, K.; Garg, J.P. A phase 2b, randomized, double-blind, parallel-group, placebo-controlled, dose-finding, multi-center study to evaluate the safety and efficacy of asp015k in moderate to severe rheumatoid arthritis subjects not on concomitant methotrexate. Arthritis Rheumatol. 2014, 66, S1234–S1235. [Google Scholar] [CrossRef]
- Kivitz, A.J.; Zubrzycka-Sienkiewicz, A.; Gutierrez-Ureña, S.R.; Poiley, J.; Kristy, R.; Shay, K.; Garg, J.P. A phase 2b, randomized, double-blind, parallel-group, placebo-controlled, dose-finding, multi-center study to evaluate the safety and efficacy of ASP015K in moderate to severe rheumatoid arthritis subjects who have had an inadequate response to methotrexate. Arthritis Rheumatol. 2014, 66, S421–S422. [Google Scholar] [CrossRef]
- Coombs, J.H.; Bloom, B.J.; Breedveld, F.C.; Fletcher, M.P.; Gruben, D.; Kremer, J.M.; Burgos-Vargas, R.; Wilkinson, B.; Zerbini, C.A.; Zwillich, S.H. Improved pain, physical functioning and health status in patients with rheumatoid arthritis treated with CP-690,550, an orally active Janus kinase (JAK) inhibitor: Results from a randomised, double-blind, placebo-controlled trial. Ann. Rheum. Dis. 2010, 69, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Strand, V.; van der Heijde, D.; Tanaka, Y.; Keystone, E.; Kremer, J.; Zerbini, C.A.F.; Cardiel, M.H.; Cohen, S.; Nash, P.; Song, Y.W.; et al. Tofacitinib in combination with methotrexate in patients with rheumatoid arthritis: Patient-reported outcomes from the 24-month Phase 3 ORAL Scan study. Clin. Exp. Rheumatol. 2020, 38, 848–857. [Google Scholar]
- Strand, V.; Kremer, J.; Wallenstein, G.; Kanik, K.S.; Connell, C.; Gruben, D.; Zwillich, S.H.; Fleischmann, R. Effects of tofacitinib monotherapy on patient-reported outcomes in a randomized phase 3 study of patients with active rheumatoid arthritis and inadequate responses to DMARDs. Arthritis Res. Ther. 2015, 17, 307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strand, V.; van Vollenhoven, R.F.; Lee, E.B.; Fleischmann, R.; Zwillich, S.H.; Gruben, D.; Koncz, T.; Wilkinson, B.; Wallenstein, G. Tofacitinib or adalimumab versus placebo: Patient-reported outcomes from a phase 3 study of active rheumatoid arthritis. Rheumatology (Oxford) 2016, 55, 1031–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Vollenhoven, R.; Cohen, S.; Mendelsohn, A.; Bananis, E.; Fan, H.; Takiya, L.; Fleischmann, R. Efficacy of adalimumab and tofacitinib in rheumatoid arthritis: Post-HOC analyses from a phase 3 study. Ann. Rheum. Dis. 2016, 75, 1042. [Google Scholar] [CrossRef]
- Strand, V.; Lee, E.B.; Fleischmann, R.; Alten, R.E.; Koncz, T.; Zwillich, S.H.; Gruben, D.; Wilkinson, B.; Krishnaswami, S.; Wallenstein, G. Tofacitinib versus methotrexate in rheumatoid arthritis: Patient-reported outcomes from the randomised phase III ORAL Start trial. RMD Open 2016, 2, e000308. [Google Scholar] [CrossRef] [Green Version]
- Fleischmann, R.; Strand, V.; Wilkinson, B.; Kwok, K.; Bananis, E. Relationship between clinical and patient-reported outcomes in a phase 3 trial of tofacitinib or MTX in MTX-naïve patients with rheumatoid arthritis. RMD Open 2016, 2, e000232. [Google Scholar] [CrossRef] [Green Version]
- Strand, V.; Burmester, G.R.; Zerbini, C.A.; Mebus, C.A.; Zwillich, S.H.; Gruben, D.; Wallenstein, G.V. Tofacitinib with methotrexate in third-line treatment of patients with active rheumatoid arthritis: Patient-reported outcomes from a phase III trial. Arthritis Care Res. 2015, 67, 475–483. [Google Scholar] [CrossRef]
- Strand, V.; Mysler, E.; Moots, R.J.; Wallenstein, G.; DeMasi, R.; Luo, Z.; Soma, K.; Iikuni, N.; Fleischmann, R. Tofacitinib with and without methotrexate versus adalimumab with methotrexate for the treatment of rheumatoid arthritis: Patient-reported outcomes from a phase 3b/4 randomized trial. Arthritis Rheumatol. 2017, 69 (Suppl. 10), 2716–2717. [Google Scholar]
- Strand, V.; Mysler, E.; Moots, R.J.; Wallenstein, G.V.; DeMasi, R.; Gruben, D.; Soma, K.; Iikuni, N.; Smolen, J.S.; Fleischmann, R. Patient-reported outcomes for tofacitinib with and without methotrexate, or adalimumab with methotrexate, in rheumatoid arthritis: A phase IIIB/IV trial. RMD Open 2019, 5, e001040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strand, V.; Kremer, J.M.; Gruben, D.; Krishnaswami, S.; Zwillich, S.H.; Wallenstein, G.V. Tofacitinib in Combination with Conventional Disease-Modifying Antirheumatic Drugs in Patients with Active Rheumatoid Arthritis: Patient-Reported Outcomes from a Phase III Randomized Controlled Trial. Arthritis Care Res. 2017, 69, 592–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genovese, M.C.; Fleischmann, R.; Combe, B.; Hall, S.; Zhang, Y.; Zhou, Y.; Mohamed, M.F.; Meerwein, S.; Pangan, A.L. Upadacitinib in patients with active rheumatoid arthritis and inadequate response or intolerance to biological dMARDS: A phase 3 randomized, placebocontrolled, double-blind study of a selective JAK1 inhibitor. Ann. Rheum. Dis. 2018, 77, 970. [Google Scholar] [CrossRef]
- Strand, V.; Schiff, M.; Tundia, N.; Friedman, A.; Meerwein, S.; Pangan, A.; Ganguli, A.; Fuldeore, M.; Song, Y.; Pope, J. Effects of upadacitinib on patient-reported outcomes: Results from SELECT-BEYOND, a phase 3 randomized trial in patients with rheumatoid arthritis and inadequate responses to biologic disease-modifying antirheumatic drugs. Arthritis Res. Ther. 2019, 21, 263. [Google Scholar] [CrossRef] [Green Version]
- Strand, V.; Bergman, M.; Tundia, N.; Ostor, A.; Durez, P.; Song, I.H.; Enejosa, J.J.; Schlacher, C.; Song, Y.; Fleischmann, R. Upadacitinib improves patient-reported outcomes in patients with rheumatoid arthritis and inadequate response to methotrexate: Results from select-compare. Ann. Rheum. Dis. 2019, 78, 738–739. [Google Scholar] [CrossRef] [Green Version]
- Strand, V.; Tundia, N.; Radominski, S.; Friedman, A.; Dunlap, K.; Goldschmidt, D.; Bergman, M. Upadacitinib monotherapy improves patientreported outcomes in methotrexate-naïve patients with moderately to severely active rheumatoid arthritis: Results from selectearly. Ann. Rheum. Dis. 2019, 78, 372–373. [Google Scholar] [CrossRef] [Green Version]
- Van Vollenhoven, R.; Takeuchi, T.; Pangan, A.L.; Friedman, A.; Mohamed, M.F.; Chen, S.; Rischmueller, M.; Blanco, R.; Xavier, R.M.; Strand, V. A phase 3, randomized controlled trial comparing upadacitinib monotherapy to MTX monotherapy in MTX-naïve patients with active rheumatoid arthritis. Int. J. Rheum. Dis. 2019, 22, 173–174. [Google Scholar] [CrossRef] [Green Version]
- Strand, V.; Buch, M.; Tundia, N.; Camp, H.S.; Suboticki, J.; Goldschmidt, D.; Wells, A.F. Upadacitinib monotherapy improves patient-reported outcomes in patients with rheumatoid arthritis and inadequate response to methotrexate. Arthritis Rheumatol. 2018, 70, 2833–2834. [Google Scholar] [CrossRef] [Green Version]
- Strand, V.; Pope, J.; Tundia, N.; Friedman, A.; Camp, H.S.; Pangan, A.; Ganguli, A.; Fuldeore, M.; Goldschmidt, D.; Schiff, M. Upadacitinib improves patient-reported outcomes in patients with rheumatoid arthritis and inadequate response to conventional synthetic disease-modifying antirheumatic drugs: Results from SELECT-NEXT. Arthritis Res. Ther. 2019, 21, 272. [Google Scholar] [CrossRef] [Green Version]
- Heiberg, T.; Kvien, T.K. Preferences for improved health examined in 1024 patients with rheumatoid arthritis: Pain has highest priority. Arthritis Care Res. 2002, 47, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Walsh, D.A.; McWilliams, D.F. Mechanisms, impact and management of pain in rheumatoid arthritis. Nat. Rev. Rheumatol. 2014, 10, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves dos Santos, G.; Delay, L.; Yaksh, T.L.; Corr, M. Neuraxial Cytokines in Pain States. Front. Immunol. 2020, 10, 3061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaible, H.-G. Nociceptive neurons detect cytokines in arthritis. Arthritis Res. Ther. 2014, 16, 470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawasaki, Y.; Zhang, L.; Cheng, J.-K.; Ji, R.-R. Cytokine Mechanisms of Central Sensitization: Distinct and Overlapping Role of Interleukin-1β, Interleukin-6, and Tumor Necrosis Factor-α in Regulating Synaptic and Neuronal Activity in the Superficial Spinal Cord. J. Neurosci. 2008, 28, 5189–5194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popiolek-Barczyk, K.; Mika, J. Targeting the Microglial Signaling Pathways: New Insights in the Modulation of Neuropathic Pain. Curr. Med. Chem. 2016, 23, 2908–2928. [Google Scholar] [CrossRef] [Green Version]
- Ren, K.; Dubner, R. Interactions between the immune and nervous systems in pain. Nat. Med. 2010, 16, 1267–1276. [Google Scholar] [CrossRef]
- Haroon, E.; Raison, C.L.; Miller, A.H. Psychoneuroimmunology Meets Neuropsychopharmacology: Translational Implications of the Impact of Inflammation on Behavior. Neuropsychopharmacology 2012, 37, 137–162. [Google Scholar] [CrossRef] [PubMed]
- Crispino, N.; Ciccia, F. JAK/STAT pathway and nociceptive cytokine signalling in rheumatoid arthritis and psoriatic arthritis. Clin. Exp. Rheumatol. 2021, 39, 668–675. [Google Scholar] [PubMed]
- Weng, C.; Xue, L.; Wang, Q.; Lu, W.; Xu, J.; Liu, Z. Comparative efficacy and safety of Janus kinase inhibitors and biological disease-modifying antirheumatic drugs in rheumatoid arthritis: A systematic review and network meta-analysis. Ther. Adv. Musculoskelet Dis. 2021, 13, 1–13. [Google Scholar] [CrossRef]
- Shamail, G.M.H.; Haridoss, M.; Natarajan, M.; Joshua, V.; Bagepally, B.S. Association Between Janus Kinase Inhibitors Therapy and Mental Health Outcome in Rheumatoid Arthritis: A Systematic Review and Meta-analysis. Rheumatol. Ther. 2021. [Google Scholar] [CrossRef] [PubMed]
- Matcham, F.; Galloway, J.; Hotopf, M.; Roberts, E.; Scott, I.C.; Steer, S.; Norton, S. The Impact of Targeted Rheumatoid Arthritis Pharmacologic Treatment on Mental Health: A Systematic Review and Network Meta-Analysis. Arthritis Rheumatol. 2018, 70, 1377–1391. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, R.M.; van der Heijde, D.; Gardiner, P.V.; Szumski, A.; Marshall, L.; Bananis, E. DAS28-CRP and DAS28-ESR cut-offs for high disease activity in rheumatoid arthritis are not interchangeable. RMD Open 2017, 3, e000382. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.C.; Lee, Y.H. Comparison of the efficacy and safety of tofacitinib and baricitinib in patients with active rheumatoid arthritis: A Bayesian network meta-analysis of randomized controlled trials. Z. Rheumatol. 2019, 78, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Bae, S.-C.; Song, G.G. Comparative efficacy and safety of tofacitinib, with or without methotrexate, in patients with active rheumatoid arthritis: A Bayesian network meta-analysis of randomized controlled trials. Rheumatol. Int. 2015, 35, 1965–1974. [Google Scholar] [CrossRef] [PubMed]
- Kawalec, P.; Mikrut, A.; Wiśniewska, N.; Pilc, A. The effectiveness of tofacitinib, a novel Janus kinase inhibitor, in the treatment of rheumatoid arthritis: A systematic review and meta-analysis. Clin. Rheumatol. 2013, 32, 1415–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, K.J.; Sanchez, H.N.; Schoenbrunner, N. Defining response to TNF-inhibitors in rheumatoid arthritis: The negative impact of anti-TNF cycling and the need for a personalized medicine approach to identify primary non-responders. Clin. Rheumatol. 2019, 38, 2967–2976. [Google Scholar] [CrossRef] [Green Version]
- Chatzidionysiou, K.; Sfikakis, P.P. Low rates of remission with methotrexate monotherapy in rheumatoid arthritis: Review of randomised controlled trials could point towards a paradigm shift. RMD Open 2019, 5, e000993. [Google Scholar] [CrossRef] [PubMed]
- Sung, Y.K.; Lee, Y.H. Comparative study of the efficacy and safety of tofacitinib, baricitinib, upadacitinib, and filgotinib versus methotrexate for disease-modifying antirheumatic drug-naïve patients with rheumatoid arthritis. Z. Rheumatol. 2021, 80, 889–898. [Google Scholar] [CrossRef]
- Inui, K.; Koike, T. Combination therapy with biologic agents in rheumatic diseases: Current and future prospects. Ther. Adv. Musculoskelet. Dis. 2016, 8, 192–202. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Wiley: Hoboken, NJ, USA, 2021; Available online: www.training.cochrane.org/handbook (accessed on 22 December 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claire, R.; Gluud, C.; Berlin, I.; Coleman, T.; Leonardi-Bee, J. Using Trial Sequential Analysis for estimating the sample sizes of further trials: Example using smoking cessation intervention. BMC Med. Res. Methodol. 2020, 20, 284. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Murad, M.H.; Montori, V.M.; Ioannidis, J.P.; Jaeschke, R.; Devereaux, P.J.; Prasad, K.; Neumann, I.; Carrasco-Labra, A.; Agoritsas, T.; Hatala, R.; et al. How to read a systematic review and meta-analysis and apply the results to patient care: Users’ guides to the medical literature. JAMA 2014, 312, 171–179. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Population | Total No of Patients | Intervention | Comparator | Concomitant Medication | |
|---|---|---|---|---|---|---|---|
| PBO | Active Comparator | ||||||
| NCT00902486 [30] | 2010 | inadequate response to DMARDs | 124 | baricitinib | + | – | csDMARD |
| NCT01185353 [28,61,62] | 2015 | inadequate response to MTX | 301 | baricitinib | + | – | MTX |
| NCT02265705 [27,63] | 2020 | inadequate response to MTX | 290 | baricitinib | + | – | MTX |
| NCT01721044 [25,64] | 2016 | inadequate response to TNFi | 527 | baricitinib | + | – | csDMARD |
| NCT01710358 [24,65] | 2017 | inadequate response to MTX | 1305 | baricitinib | + | adalimumab | csDMARD |
| NCT01711359 [55,66,67] | 2017 | csDMARD naive | 584 | baricitinib | + | MTX | – |
| NCT01721057 [26,60,68] | 2017 | inadequate response to csDMARDs | 684 | baricitinib | + | – | csDMARDs |
| NCT01469013 [29] | 2016 | inadequate response to MTX | 145 | baricitinib | + | – | MTX |
| NCT01052194 [49,69] | 2015 | inadequate response to MTX | 204 | decernotinib | + | – | – |
| NCT2011–004419–22 [47,70] | 2016 | inadequate response to MTX | 358 | decernotinib | + | – | MTX |
| NCT01754935 [48] | 2016 | inadequate response to DMARDs | 43 | decernotinib | + | – | DMARDs |
| NCT01888874 [42] | 2016 | inadequate response to MTX | 594 | filgotinib | + | – | MTX |
| NCT01894516 [41] | 2017 | inadequate response to MTX | 283 | filgotinib | + | – | – |
| NCT02889796 [39] | 2019 | inadequate response to MTX | 1755 | filgotinib | + | adalimumab | MTX |
| NCT02873936 [40] | 2019 | inadequate response or intolerance to bDMARDs | 448 | filgotinib | + | – | csDMARD |
| NCT02886728 [53] | 2019 | MTX naive | 1249 | filgotinib | + | MTX | – |
| NCT01384422 [58] | 2017 | n.a. | 36 | filgotinib | + | – | MTX |
| NCT01668641 [58] | 2017 | n.a. | 91 | filgotinib | + | – | MTX |
| NCT01626573 [59] | 2013 | n.a. | 60 | itacitinib | + | – | csDMARDs |
| NCT01565655 [43,71] | 2017 | inadequate response to csDMARDs | 289 | peficitinib | + | – | – |
| NCT01554696 [44,72] | 2017 | inadequate response to MTX | 379 | peficitinib | + | – | MTX |
| NCT02308163 [46] | 2019 | inadequate response to csDMARDs | 507 | peficitinib | + | etanercept | MTX |
| NCT02305849 [45] | 2019 | inadequate response to MTX | 519 | peficitinib | + | – | MTX |
| NCT01649999 [56] | 2016 | no restrictions | 281 | peficitinib | + | – | – |
| NCT02969044 [50] | 2020 | inadequate response to MTX | 70 | ritlecitinib | + | – | MTX |
| NCT00976599 [19] | 2015 | inadequate response to MTX | 29 | tofacitinib | + | – | MTX |
| NCT01164579 [51] | 2016 | MTX naive | 109 | tofacitinib | + | MTX | – |
| NCT00550446 [17] | 2012 | inadequate response to DMARDs | 384 | tofacitinib | + | adalimumab | – |
| NCT00147498 [20,73] | 2009 | inadequate response to DMARDs | 264 | tofacitinib | + | – | – |
| NCT00413660 [21] | 2012 | inadequate response to DMARDs | 507 | tofacitinib | + | – | MTX |
| Menshikova 2018, [57] | 2018 | n.a. | 30 | tofacitinib | – | etanercept | n.a. |
| NCT02157012 [18] | 2018 | inadequate response to DMARDs | 50 | tofacitinib | – | tocilizumab, abatacept | MTX |
| NCT00847613 [11,74] | 2013 | inadequate response to MTX | 797 | tofacitinib | + | – | MTX |
| NCT00814307 [17,75] | 2012 | inadequate response to DMARDs | 610 | tofacitinib | + | – | – |
| NCT00853385 [12,76,77] | 2012 | inadequate response to MTX | 717 | tofacitinib | + | adalimumab | MTX |
| NCT01039688 [54,78,79] | 2014 | MTX naive | 956 | tofacitinib | – | MTX | – |
| NCT00960440 [14,80] | 2013 | inadequate response to TNFi | 399 | tofacitinib | + | – | MTX |
| NCT02187055 [16,81,82] | 2017 | inadequate response to MTX | 1146 | tofacitinib | – | adalimumab | MTX |
| NCT00856544 [13,83] | 2013 | inadequate response to DMARDs | 792 | tofacitinib | + | – | nonbiologic DMARDs |
| NCT00603512 [22] | 2011 | inadequate response to MTX | 136 | tofacitinib | + | – | MTX |
| NCT00687193 [23] | 2015 | inadequate response to at least one synthetic or bDMARD | 317 | tofacitinib | + | – | – |
| NCT01960855 [35] | 2016 | inadequate response to TNFi | 276 | upadacitinib | + | – | MTX |
| NCT02066389 [34] | 2016 | inadequate response to MTX | 299 | upadacitinib | + | – | MTX |
| NCT02706847 [36,84,85] | 2018 | inadequate response to bDMARDs | 499 | upadacitinib | + | – | csDMARD |
| NCT03086343 [37] | 2020 | inadequate response to bDMARDs | 612 | upadacitinib | – | abatacept | csDMARD |
| NCT02629159 [32,86] | 2019 | inadequate response to MTX | 1629 | upadacitinib | + | adalimumab | MTX |
| NCT02706873 [52,87,88] | 2020 | MTX naive | 945 | upadacitinib | – | MTX | – |
| NCT02706951 [31,89] | 2019 | inadequate response to MTX | 648 | upadacitinib | – | MTX | – |
| NCT02675426 [33,90] | 2018 | inadequate response to csDMARDs | 661 | upadacitinib | + | – | csDMARD |
| NCT02720523 [38] | 2020 | inadequate response to csDMARDs | 197 | upadacitinib | + | – | csDMARD |
| Outcomes | No. of Participants (Studies) Follow Up | Certainty of the Evidence (GRADE) | Relative Effect (95% CI) | Anticipated Absolute Effects | |
|---|---|---|---|---|---|
| Risk with Placebo | Risk Difference with JAK Inihbitors | ||||
| JAK inhibitors compared to placebo (<6 months) | |||||
| Pain assessed on VAS Scale from: 0 to 100 | 9588 (21 RCTs) | ⊕⊕⊕◯ MODERATE a,b | – | The mean pain was 0 mm | MD 15.29 mm lower (17.34 lower to 13.24 lower) |
| Number of patients reaching remission according to DAS28–ESR | 6648 (16 RCTs) | ⊕⊕⊕⊕ HIGH b | OR 3.99 (2.84 to 5.59) | 32 per 1000 | 84 more per 1000 (53 more to 123 more) |
| Number of patients reaching remission according to DAS28–CRP | 12,562 (28 RCTs) | ⊕⊕⊕◯ MODERATE a,b | OR 3.75 (3.08 to 4.56) | 98 per 1000 | 192 more per 1000 (153 more to 233 more) |
| Number of patients reaching 20% improvement according to ACR criteria (ACR20) | 17,056 (42 RCTs) | ⊕⊕⊕◯ MODERATE a,b | OR 3.31 (2.85 to 3.86) | 374 per 1000 | 290 more per 1000 (256 more to 324 more) |
| Mortality | 13,090 (31 RCTs) | ⊕⊕◯◯ LOW b | OR 0.81 (0.40 to 1.63) | 2 per 1000 | 0 fewer per 1000 (1 fewer to 1 more) |
| Number of patients with serious side effects | 12,932 (31 RCTs) | ⊕⊕⊕◯ MODERATE a | OR 0.95 (0.75 to 1.21) | 30 per 1000 | 1 fewer per 1000 (7 fewer to 6 more) |
| Change in CRP assessed with: mg/L | 8321 (19 RCTs) | ⊕⊕◯◯ LOW a,b | – | The mean change in C–reactive protein was 0 mg/L | MD 8.57 mg/L lower (10.14 lower to 6.99 lower) |
| JAK inhibitors compared to bDMARDs (<6 months) | |||||
| Pain assessed on VAS Scale from: 0 to 100 | 2179 (4 RCTs) | ⊕⊕⊕◯ MODERATE a | – | The mean pain was 0 mm | MD 4.35 mm lower (6.47 lower to 2.23 lower) |
| Number of patients reaching remission according to DAS28–ESR | 2046 (4 RCTs) | ⊕◯◯◯ VERY LOW a,b | OR 2.62 (0.85 to 8.10) | 69 per 1000 | 94 more per 1000 (10 fewer to 307 more) |
| Number of patients reaching remission according to DAS28–CRP | 4409 (3 RCTs) | ⊕⊕◯◯ LOW a,b | OR 1.95 (1.27 to 3.00) | 185 per 1000 | 122 more per 1000 (39 more to 220 more) |
| Number of patients reaching 20% improvement according to ACR criteria (ACR20) | 5040 (6 RCTs) | ⊕⊕⊕◯ MODERATE a | OR 1.30 (1.15 to 1.48) | 646 per 1000 | 58 more per 1000 (31 more to 84 more) |
| Mortality | 2176 (3 RCTs) | ⊕⊕◯◯ LOW a | OR 0.76 (0.09 to 6.53) | 2 per 1000 | 0 fewer per 1000 (2 fewer to 9 more) |
| Number of patients with serious side effects | 2180 (3 RCTs) | ⊕⊕◯◯ LOW a | RR 1.56 (0.82 to 2.98) | 34 per 1000 | 19 more per 1000 (6 fewer to 68 more) |
| Change in CRP assessed with: mg/L | 2643 (4 RCTs) | ⊕⊕◯◯ LOW a | – | The mean change in C–reactive proteint was 0 mg/L | MD 3.94 mg/: lower (5.35 lower to 2.52 lower) |
| JAK inhibitors compared to MTX (<6 months) | |||||
| Pain—not measured | – | – | – | – | – |
| Number of patients reaching remission according to DAS28–ESR | 2028 (4 RCTs) | ⊕◯◯◯ VERY LOW a,b | OR 2.62 (0.85 to 8.10) | 69 per 1000 | 94 more per 1000 (10 fewer to 307 more) |
| Number of patients reaching remission according to DAS28–CRP | 2519 (4 RCTs) | ⊕⊕◯◯ LOW a,b | OR 3.05 (1.79 to 5.18) | 202 per 1000 | 234 more per 1000 (110 more to 365 more) |
| Number of patients reaching 20% improvement according to ACR criteria (ACR20) | 3617 (6 RCTs) | ⊕⊕⊕◯ MODERATE a,b | OR 2.33 (1.80 to 3.03) | 581 per 1000 | 183 more per 1000 (133 more to 227 more) |
| Mortality—not measured | – | – | – | – | – |
| Number of patients with serious side effects | 1643 (3 RCTs) | ⊕⊕◯◯ LOW b | OR 1.30 (0.75 to 2.25) | 32 per 1000 | 9 more per 1000 (8 fewer to 37 more) |
| Change in CRP assessed with: mg/L—not measured | – | – | – | – | – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tóth, L.; Juhász, M.F.; Szabó, L.; Abada, A.; Kiss, F.; Hegyi, P.; Farkas, N.; Nagy, G.; Helyes, Z. Janus Kinase Inhibitors Improve Disease Activity and Patient-Reported Outcomes in Rheumatoid Arthritis: A Systematic Review and Meta-Analysis of 24,135 Patients. Int. J. Mol. Sci. 2022, 23, 1246. https://doi.org/10.3390/ijms23031246
Tóth L, Juhász MF, Szabó L, Abada A, Kiss F, Hegyi P, Farkas N, Nagy G, Helyes Z. Janus Kinase Inhibitors Improve Disease Activity and Patient-Reported Outcomes in Rheumatoid Arthritis: A Systematic Review and Meta-Analysis of 24,135 Patients. International Journal of Molecular Sciences. 2022; 23(3):1246. https://doi.org/10.3390/ijms23031246
Chicago/Turabian StyleTóth, Lilla, Márk F. Juhász, László Szabó, Alan Abada, Fruzsina Kiss, Péter Hegyi, Nelli Farkas, György Nagy, and Zsuzsanna Helyes. 2022. "Janus Kinase Inhibitors Improve Disease Activity and Patient-Reported Outcomes in Rheumatoid Arthritis: A Systematic Review and Meta-Analysis of 24,135 Patients" International Journal of Molecular Sciences 23, no. 3: 1246. https://doi.org/10.3390/ijms23031246