1. Introduction
Solitary fibrous tumors (SFTs) are mesenchymal neoplasms that can occur at any location, especially pleural, meningeal or extrapleural sites. Location in limbs is infrequent [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
26,
27,
28,
29,
30,
31,
32,
33,
34,
35,
36,
37,
38,
39,
40].
The evolution of SFTs is often uncertain [
2,
3,
4,
5,
6,
7,
8,
9,
10]. Although most cases evolve favorably, a small group can progress towards dissemination, generally pulmonary, as well as other locations, and will lead to patient death in the absence of effective treatments [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19]. Thus, valid and reproducible tools should be developed in order to design risk-tailored treatment and risk-adjusted follow-up.
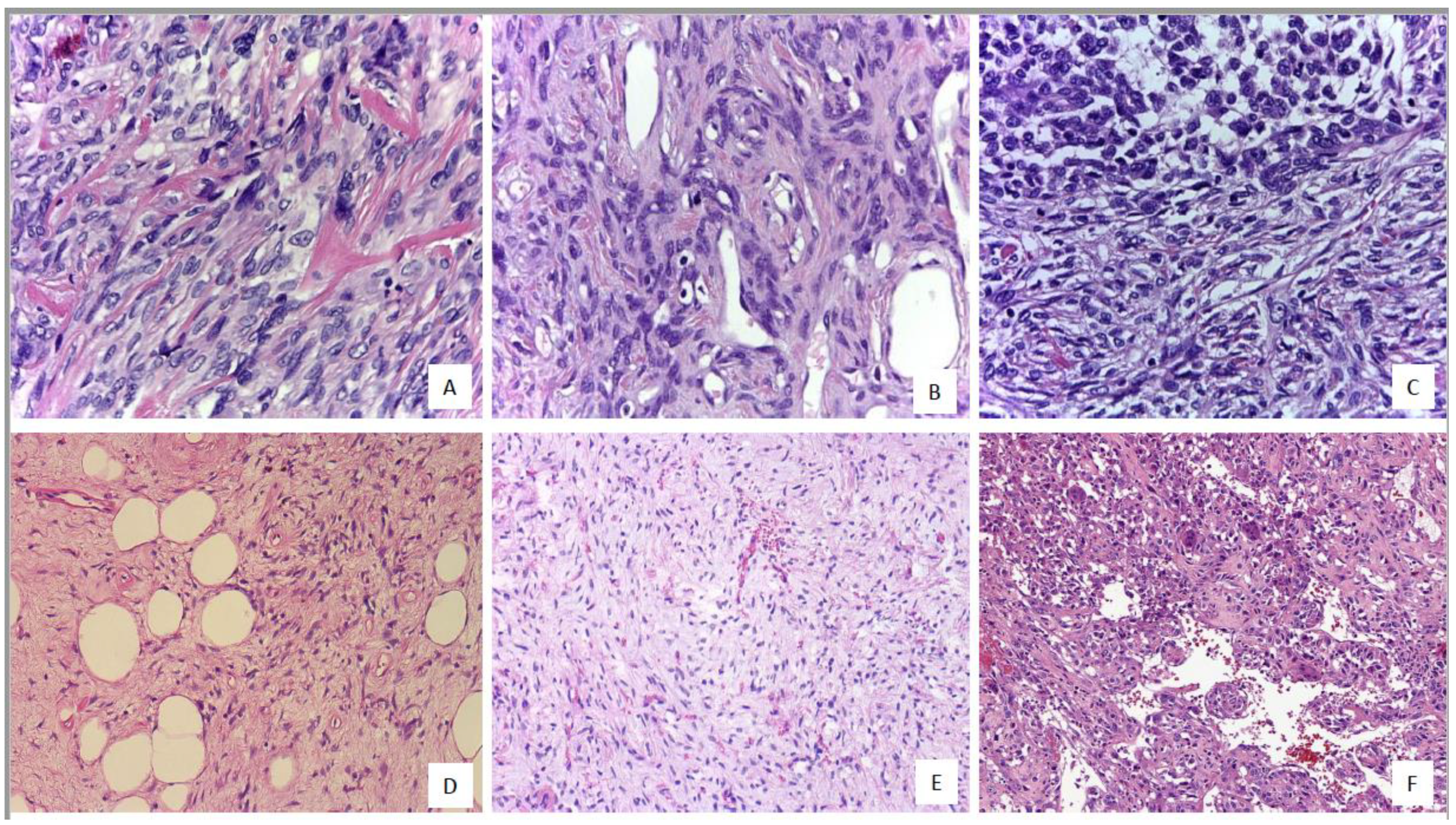
A patternless and hemangiopericytic growth with variably fibrosis and collagenous deposits are characteristic, but SFTs can show many faces, including round cells, giant-cells, myxoid areas, pleomorphic pattern, fat-forming tumors and dedifferentiated forms [
1,
2,
3,
4,
5,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25].
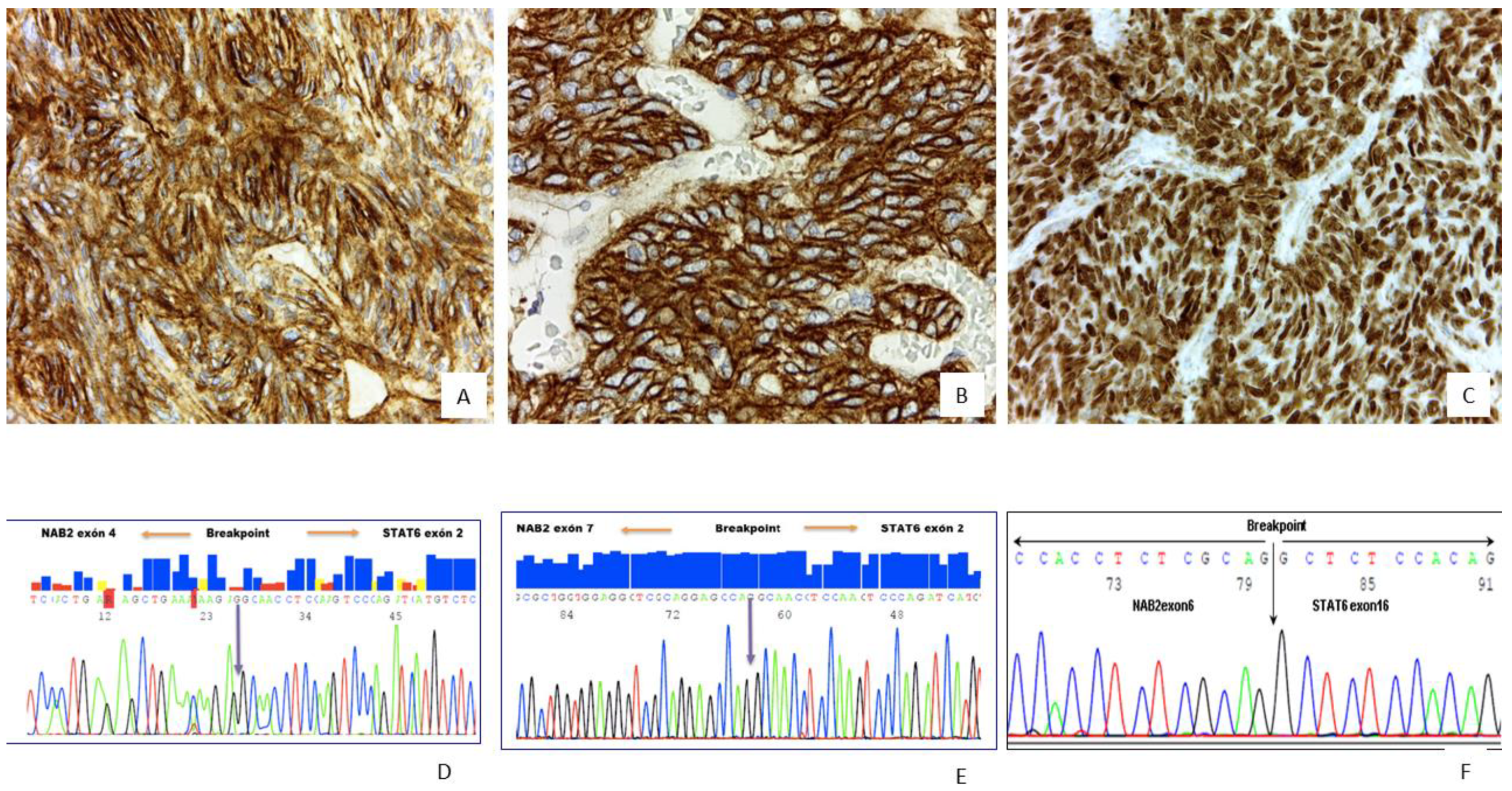
Strong and diffuse nuclear immunoreactivity for Signal transducer and activator of transcription 6 (STAT6) is almost always diagnosed in SFTs, and CD34, Bcl-2 and CD99 immunoexpression is common [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25]. Aberrant epithelial, muscular or neuroendocrine marker expression has been described which may lead to confusion with other tumors that share a similar morphology [
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
36]. The fusion gene
NAB2/STAT6 and its variants confirm a diagnosis of SFT in those cases with unconvincing STAT6 immunoreactivity, and specific gene fusions have been related to prognosis and tumor location [
6,
7,
8,
9,
10,
11,
12,
13,
14,
26,
27,
28,
29,
30,
31,
32,
33,
34,
35,
36,
37,
38,
39,
40]. STAT6 nuclear expression is not exclusive to SFTs and has also been reported in dedifferentiated liposarcoma, glioma-associated oncogene homolog 1 (
GLI1)-amplified tumor, Kaposi sarcoma and Hodgkin as well non-Hodgkin lymphomas [
6,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
36,
37,
38,
39,
40].
Several risk-stratification systems (RSS) have been described [
1,
2,
3,
4,
5], although the Demicco et al. RSS seems to be the most widely implemented [
1,
2,
14]. While most SFTs categorized as low-risk by the Demicco system follow an apparently benign course, some cases may have late relapse or metastases; hence, the RSS is not perfectly specific in predicting the evolution in all cases [
1,
2,
14]. In addition, molecular results have not so far been included in any of the current RSS [
1,
2,
14]. Recently, loss of Apoptotic Protease Activating Factor (APAF-1) expression has been associated with poor prognosis in SFTs, but these findings need to be confirmed in larger series [
41].
We have previously published a small series of SFTs with at least one histological factor associated with aggressive behavior and explored the correlation between the adverse histological findings and molecular profile with tumor behavior [
42]. The main goal of the present study was to confirm our previous results including additional tumors, mainly SFTs categorized as low-risk by Demicco et al. [
1,
2] and correlate the clinical, histological and immunohistochemical findings,
TP53 mutational status and
TERT promotor mutational status with clinical outcome.
3. Discussion
Strong and diffuse nuclear immunoreactivity for STAT6 is a very useful tool for the diagnosis of SFTs, although unexpected epithelial, muscular or neuroendocrine marker expression has also been described in these tumors and may lead to confusion with other neoplasms with hemangiopericytic growth patterns [
2,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
33,
42]. STAT6 expression has also been reported in dedifferentiated liposarcoma and
GLI1-amplified tumors; hence, in cases with overlapping morphology and STAT6 immunoreactivity, additional molecular studies are needed to establish a definitive diagnosis [
2,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
33,
34,
35,
36,
37,
38,
39,
40,
41,
42]. Detection of the specific fusion gene
NAB2/STAT6 and its variants confirm a diagnosis of SFT, especially in rare clinical settings, unusual histological findings or unexpected immunohistochemical results. Moreover, specific gene fusions have been related to prognosis and tumor location [
7,
8,
11,
12,
26,
27,
28,
29,
30,
31,
32,
35,
36,
37,
38,
39,
40,
41,
42]. Various risk-stratification systems (RSS) have been described, with the Demicco et al. system being the most widely implemented, as recommended in the World Health Organization (WHO) blue book [
1,
2,
3,
4,
5,
14].
Most low risk SFTs categorized by Demicco et al. and other RSS follow an apparently indolent course. However, some of these cases may have late recurrence/relapse and/or metastases leading to uncertainty and skepticism among oncologists regarding the specificity of RSS in correctly predicting evolution in all cases [
1,
2,
3,
4,
5,
14]. Furthermore, molecular results have not been included in any of the present RSS so far [
1,
2,
3,
4,
5,
6,
7,
8,
42].
Regarding histological predictive factors of aggressiveness, high mitotic counts with a general agreement of ≥4/10HPFs represent the strongest predictor of malignant behavior, as confirmed in the present series where all tumors categorized as high-risk and many of the tumors classified as intermediate-risk revealed ≥4/10HPFs [
1,
2,
3,
4,
5,
6,
7,
8,
42]. Likewise, necrosis was present in the same group of tumors (all high-risk and many intermediate-risk).
Of all the immunohistochemical markers applied in this series, only Ki-67 ≥ 10 was associated with poor evolution. Similar to mitosis and necrosis, this finding was also found in all SFTs categorized as high-risk. Ki-67 has only been included in the Diebold et al. RSS [
3], and although further confirmation is needed, this factor may represent an additional variable that could provide valuable predictive information on tumor evolution. In the present series, half the tumors categorized as low-risk by the Demicco et al. system but with worse evolution (late recurrences or metastasis) showed Ki-67 ≥ 10.
Recently, loss of APAF-1 immunoexpression has been associated with the progression and poor prognosis in SFTs [
41]. APAF-1 inactivation may lead to impaired apoptotic function, and eventually may contribute toward malignant SFT transformation [
41]. Nevertheless, this finding needs to be confirmed in larger series. We failed to find this association in the present study, despite some SFTs with aggressive evolution (dedifferentiated tumors) showing loss of APAF-1 expression by immunohistochemistry.
Molecular studies in SFTs have been progressively implemented in many centers for diagnosis and prognosis. SFTs with the most common canonical
NAB2 exon 4-STAT6 exon 2 fusion variant are often located in the thorax and are less cellular with abundant fibrosis [
8,
9,
10,
11,
12,
28,
29,
30,
31,
32,
37,
38,
39,
40]. These tumors have a higher tumor age, larger tumor size, lower mitotic activity and lower recurrence rate [
28,
29,
30,
31,
32,
37,
38,
39,
40]. However, those tumors with
NAB2 exon 6-STAT6 exon 16/17 fusion variants typically show a more cellular round to ovoid cell morphology and are often located in the deep soft tissue of the intra-abdominal/retroperitoneal/pelvic region or in central nervous system [
28,
29,
30,
31,
32,
37,
38,
39,
40]. SFTs with
NAB2 exon 6-STAT6 exon 16/17 fusion occur in a significantly younger age group, showing higher mitotic activity and a higher recurrence rate [
39].
Recently, a new study reported that SFTs with the
NAB2 exon 4-STAT6 exon 2 fusion variant show a transcriptional signature enriched for genes involved in DNA binding, gene transcription and nuclear localization, whereas SFTs with the
NAB2 exon 6-STAT6 exon 16/17 fusion variants were enriched for genes involved in tyrosine kinase signaling, cell proliferation and cytoplasmic localization [
40]. In addition, Georgies T et al. have reported prognostic significance in SFTs depending on
STAT6 domain composition [
40]. They categorized SFTs as either
STAT6-TAD (contained only the transactivation domain of STAT6) or
STAT-Full (fusions with most of the STAT6 domain intact). Tumors with
STAT6-TAD fusions had a higher mitotic count (
p = 0.016) and were associated with poor prognosis [
40].
We did not observe any direct association of gene fusion variants with aggressiveness or location of any histologic or phenotypic profile in the present series.
A limitation of the present study was the fact that 48.5% of the samples (47/97) showed non-informative RNA results for the detection of the
NAB2/STAT6 fusion gene. Nevertheless, all cases in the present series showed strong and diffuse STAT6 nuclear expression by immunohistochemistry. This finding of strong and diffuse nuclear STAT6 immunoreactivity has previously been implemented in many laboratories as a surrogate for the molecular analysis in solitary fibrous tumors considering the good correlation between the nuclear STAT6 overexpression and the presence of the
NAB2/STAT6 fusion gene [
1,
2,
3,
4,
5,
6,
7,
8,
42]. Furthermore, since the
NAB2/STAT6 fusion gene represents an intrachromosomal inversion, a non-informative or negative result is not exceptional in gene fusion molecular studies.
Reverse transcription-polymerase chain reaction (RT-PCR) may not be the most suitable method to detect fusion genes in SFTs, and more sensitive techniques such as next generation sequencing (NGS) or RNAseq may have improved the quality of the results. However, these very advanced molecular ancillary tests are also more expensive and not widely available in all pathology labs. RNA analysis failure using RT-PCR could be explained by limited material in the case of a core biopsy or by fixation issues or tissue conservation [
1,
2,
3,
4,
5,
6,
7,
8,
42]. Furthermore, although the present study used the most frequent primers for RT-PCR, they would not necessarily cover the full spectrum of possible gene fusion types in solitary fibrous tumors. Indeed, RNA analysis failure may be considered multifactorial.
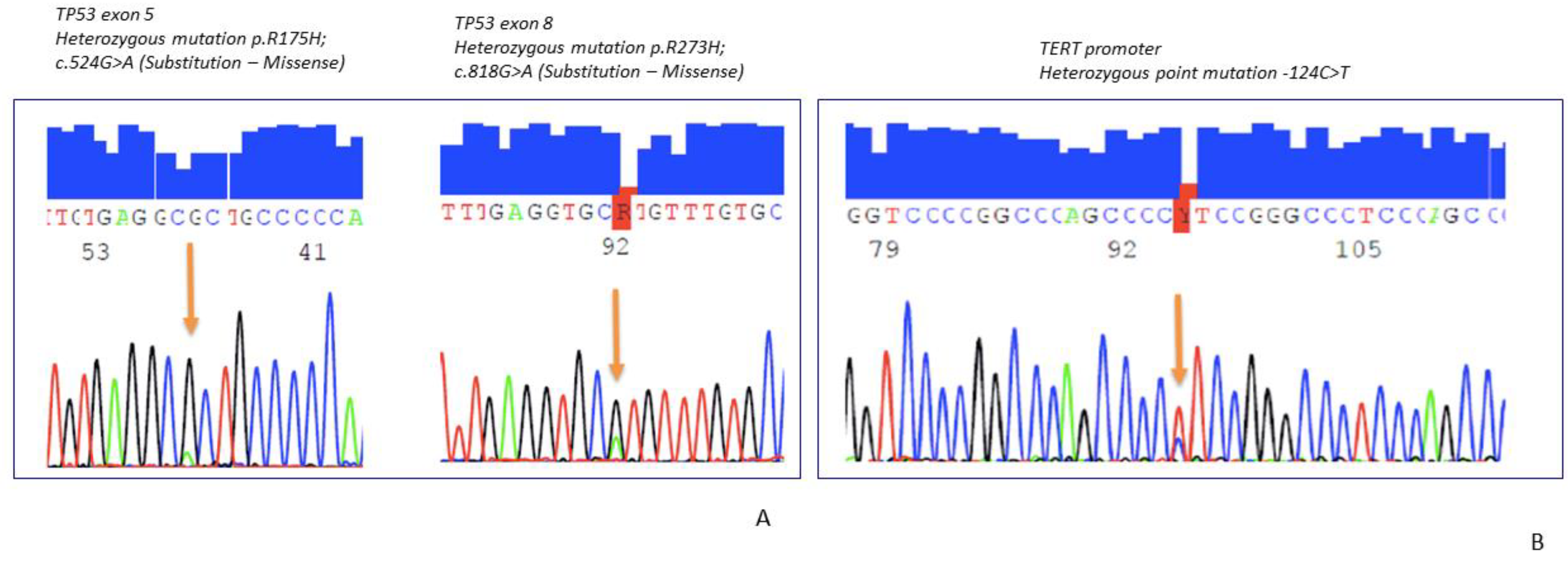
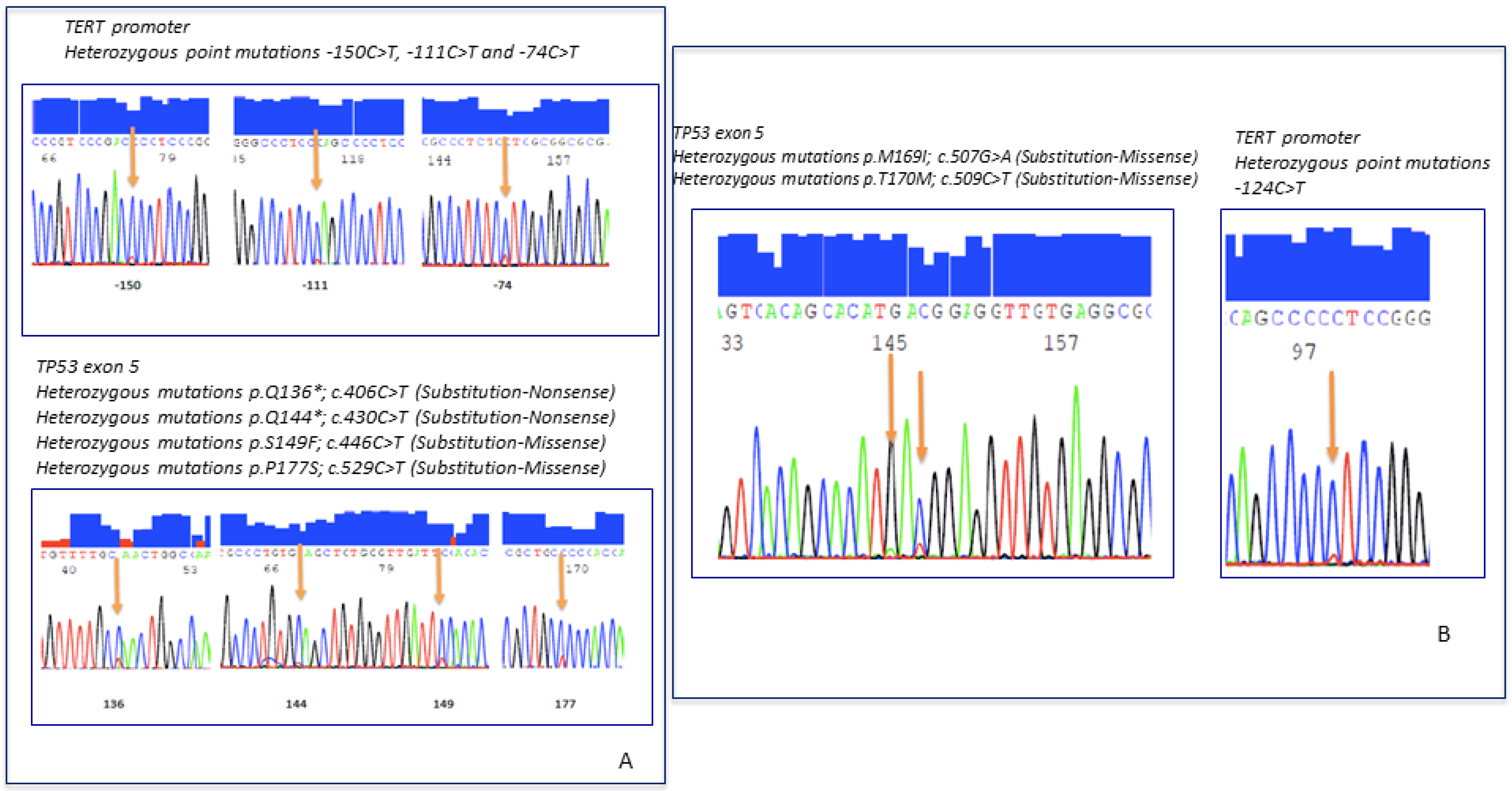
TERT promoter mutations and the
TP53 mutation have been associated with malignant behavior in SFTs [
7,
8,
12,
35,
36,
37,
38,
39,
40,
41,
42]. The overall prevalence of the
TP53 mutation in the current series was low, in contrast to the
TERT mutation that was found in almost half the tumors. Many of the high-risk tumors had
TP53 mutations,
HTER mutations or both [
7,
8,
12,
35,
36,
37,
38,
39,
40,
41,
42]. Likewise, intermediate-risk SFTs with the
HTER mutation in the present series showed poor evolution, in line with the previous observation of Demicco et al. where the
TERT mutation probably provides no additional prognostic information on tumors already classified as low or high risk [
7]. At present, despite the various studies confirming that the
HTER promotor and/or
TP53 alterations in SFTs are associated with prognosis, no risk stratification system has so far incorporated these molecular factors [
1,
2,
3,
4,
5,
6,
7,
8]. In the present series, there were only 11 cases with non-informative results for
HTER and
p53 molecular status, all of which were classified as low-risk of metastasis.
Four RSS have been proposed in the literature that classify SFTs into three (low, intermediate, high-risk) or two categories (low vs. high-risk) depending on the system [
1,
2,
3,
4,
5,
14]. The most commonly implemented is the Demicco et al. RSS which includes both clinical and histological variables [
1,
2,
14]. The Diebold et al. system includes the Ki-67 index, which is not included in the other RSS [
3]. Although presumably all dedifferentiated SFTs show other adverse clinical or histological factors, this histological characteristic has not been included in any of the RSS [
1,
2,
3,
4,
5,
14].
In the present series, all SFTs classified as high-risk by Demicco et al. had Ki-67 ≥ 10. We had four cases categorized as low-risk by Demicco et al. but with a worse clinical evolution. Two out these four cases had a Ki-67 index higher than 10 and when applying the Diebold et al. RSS [
3], those cases were classified as high-risk tumors; hence, when the systems disagree on risk stratification, the clinical evolution becomes more difficult to predict, which may suggest an imperfect specificity in predicting accurate evolution in some RSS. Incorporating the Ki-67 index might provide prognostic information in some cases independently of the histologic appearance of the tumor. However, Ki-67 results in the present series need to be validated in independent SFT series.
The identification of dedifferentiation in SFTs is very important because new evidence has revealed that antiangiogenics are effective, and their use as a first line of treatment should be considered in SFTs, but not in dedifferentiated SFTs for which chemotherapy is more effective [
8].
It would be interesting in the future to study the tumor/stromal tissue interaction, and whether the amount of collagen and/or the type of collagen fibers could have any prognostic significance in these tumors. At present, hypercellularity in solitary fibrous tumors, which usually correlates with a lower amount of collagen, has been correlated in some studies with a somewhat more aggressive evolution in SFTs, although hypercellularity is not necessarily always associated with aggressive evolution [
1,
2,
3,
4,
5,
14].
In conclusion, risk assessment still remains a challenging issue in SFT classification and the final outcome. However, the integration of clinical, morphologic, immunohistochemical and molecular findings may improve risk stratification and classification of SFTs and could guide the clinician when designing risk-adjusted treatment and follow-up. Regardless of the assigned risk stratification score, SFTs may require long-term follow-up considering that low-risk tumors may occasionally show a non-indolent evolution. The inclusion of molecular findings in RSS could improve precision in the classification of SFTs, especially those of intermediate risk. Nevertheless, future studies are required to determine the most effective way to incorporate molecular analyses into RSS on SFTs. The coexistence of several adverse factors such as ≥4 mitoses/10HPF, necrosis, Ki-67 ≥ 10%, mutations in HTER and/or p53 may suggest the need for a closer clinical follow-up regardless of the histological appearance of the tumor.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}