
Vincristine-Induced Peripheral Neuropathy (VIPN) in Pediatric Tumors: Mechanisms, Risk Factors, Strategies of Prevention and Treatment


Abstract
:1. Introduction
- − sensory neuropathy: paresthesia, numbness, impaired touch sensitivity/temperature recognition/vibration, neuropathic pain, jaw pain;
- − motor neuropathy: extremity weakness, walking difficulties, deteriorated reflexes and fine motor abilities, impaired balance, muscle cramps;
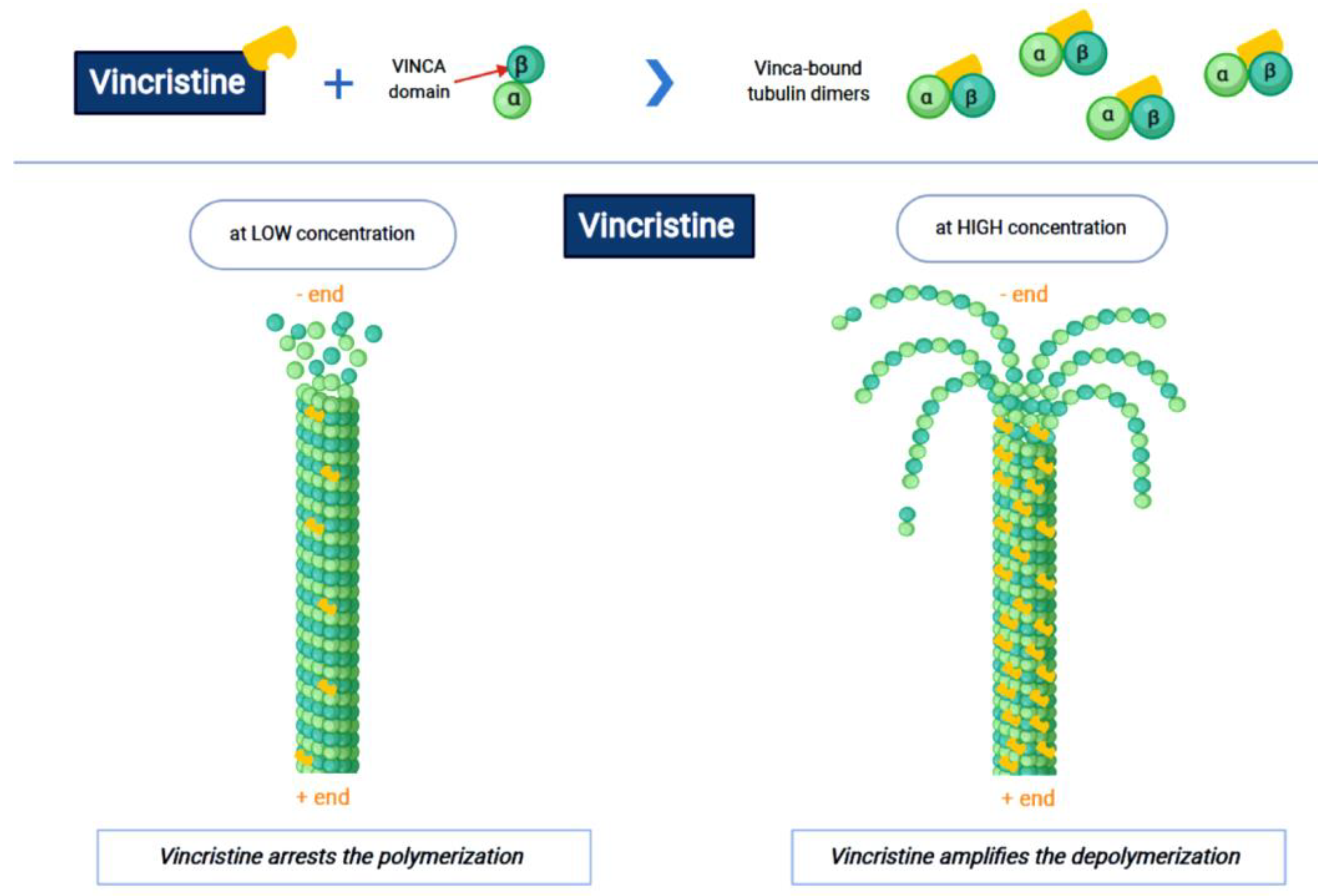
2. Pharmacokinetics and Pharmacodynamics of Vincristine
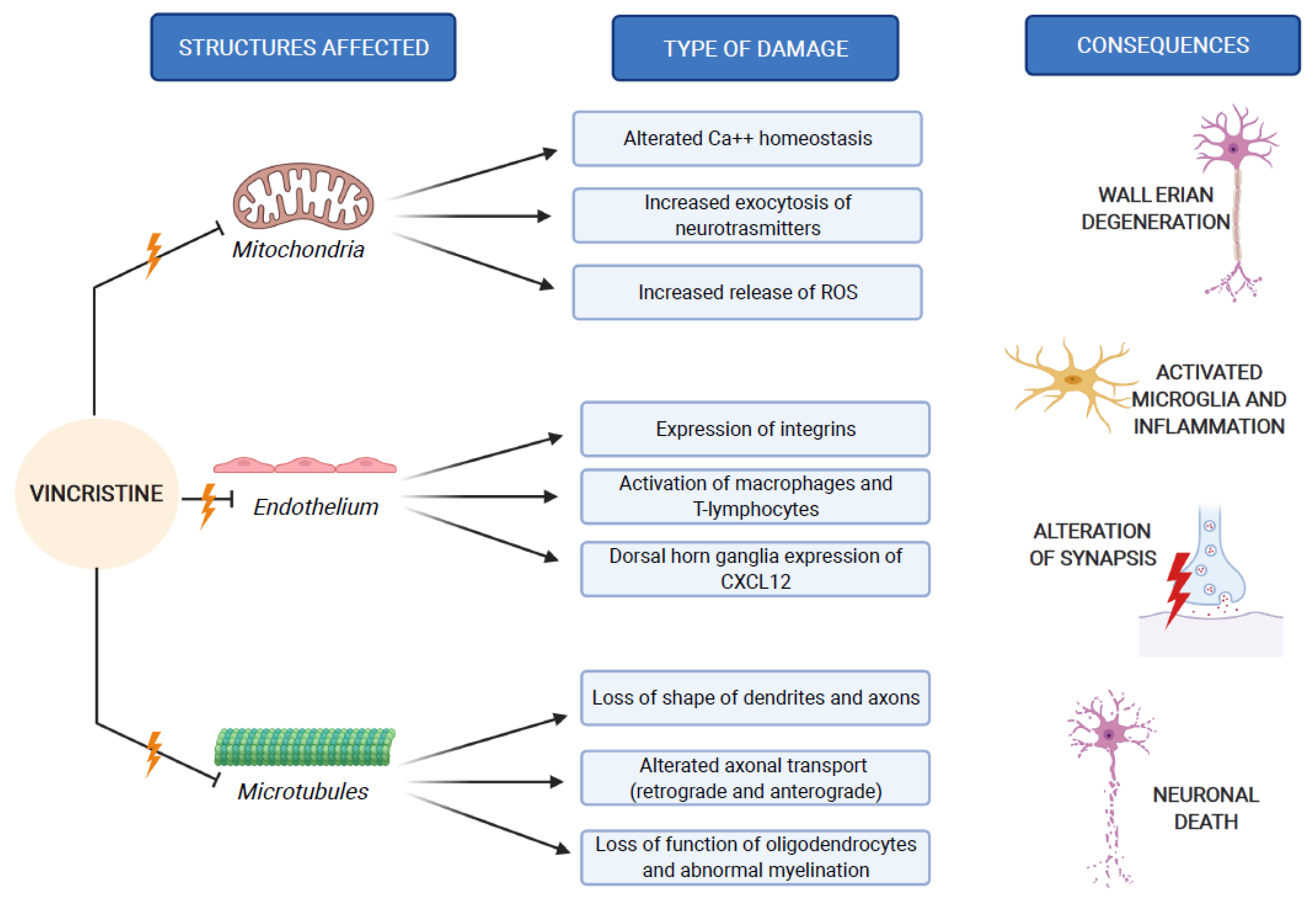
3. Pathogenesis of VIPN
4. Patient-Related Risk Factors for VIPN
5. Treatment-Related Risk Factors for VIPN
6. Strategies for Prevention and Treatment of VIPN
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Martino, E.; Casamassima, G.; Castiglione, S.; Cellupica, E.; Pantalone, S.; Papagni, F.; Rui, M.; Siciliano, A.M.; Collina, S. Vinca alkaloids and analogues as anti-cancer agents: Looking back, peering ahead. Bioorg. Med. Chem. Lett. 2018, 28, 2816–2826. [Google Scholar] [CrossRef] [PubMed]
- Carlson, K.; Ocean, A.J. Peripheral neuropathy with microtubule-targeting agents: Occurrence and management approach. Clin. Breast Cancer 2011, 11, 73–81. [Google Scholar] [CrossRef] [Green Version]
- Tay, C.G.; Lee, V.W.M.; Ong, L.C.; Goh, K.J.; Ariffin, H.; Fong, C.Y. Vincristine-induced peripheral neuropathy in survivors of childhood acute lymphoblastic leukaemia. Pediatr. Blood Cancer 2017, 64. [Google Scholar] [CrossRef] [PubMed]
- Madsen, M.L.; Due, H.; Ejskjær, N.; Jensen, P.; Madsen, J.; Dybkær, K. Aspects of vincristine-induced neuropathy in hematologic malignancies: A systematic review. Cancer Chemother. Pharmacol. 2019, 84, 471–485. [Google Scholar] [CrossRef] [Green Version]
- Triarico, S.; Maurizi, P.; Mastrangelo, S.; Attinà, G.; Capozza, M.A.; Ruggiero, A. Improving the brain delivery of chemotherapeutic drugs in childhood brain tumors. Cancers 2019, 11, 824. [Google Scholar] [CrossRef] [Green Version]
- Nazir, H.F.; AlFutaisi, A.; Zacharia, M.; Elshinawy, M.; Mevada, S.T.; Alrawas, A.; Khater, D.; Jaju, D.; Wali, Y. Vincristine-induced neuropathy in pediatric patients with acute lymphoblastic leukemia in Oman: Frequent autonomic and more severe cranial nerve involvement. Pediatr. Blood Cancer 2017, 64, 12. [Google Scholar] [CrossRef] [PubMed]
- Seetharam, S.; Thankamony, P.; Gopakumar, K.G.; Krishna, K.M.J. Higher incidence of syndrome of inappropriate antidiuretic hormone secretion during induction chemotherapy of acute lymphoblastic leukemia in indian children. Indian J. Cancer 2019, 56, 320–324. [Google Scholar] [CrossRef] [PubMed]
- How, J.; Blattner, M.; Fowler, S.; Wang-Gillam, A.; Schindler, S.E. Chemotherapy-associated posterior reversible encephalopathy syndrome: A case report and review of the literature. Neurologist 2016, 21, 112–117. [Google Scholar] [CrossRef]
- National Institutes of Health NCI. Common Terminology Criteria for Adverse Events (CTCAE). Version 4.03. 2010. Available online: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf (accessed on 28 December 2020).
- Lavoie Smith, E.M.; Li, L.; Hutchinson, R.J.; Ho, R.; Burnette, W.B.; Wells, E.; Bridges, C.; Renbarger, J. Measuring vincristine-induced peripheral neuropathy in children with acute lymphoblastic leukemia. Cancer Nurs. 2013, 36, 49–60. [Google Scholar] [CrossRef] [Green Version]
- Schouten, S.M.; van de Velde, M.E.; Kaspers, G.J.L.; Mokkink, L.B.; van der Sluis, I.M.; van den Bos, C.; Hartman, A.; Abbink, F.C.H.; van den Berg, M.H. Measuring vincristine-induced peripheral neuropathy in children with cancer: Validation of the Dutch pediatric-modified Total Neuropathy Score. Support Care Cancer 2020, 28, 2867–2873. [Google Scholar] [CrossRef] [Green Version]
- Mora, E.; Smith, E.M.; Donohoe, C.; Hertz, D.L. Vincristine-induced peripheral neuropathy in pediatric cancer patients. Am. J. Cancer Res. 2016, 6, 2416–2430. [Google Scholar] [PubMed]
- Ruggiero, A.; Triarico, S.; Trombatore, G.; Battista, A.; Dell’acqua, F.; Rizzari, C.; Riccardi, R. Incidence, clinical features and management of hypersensitivity reactions to chemotherapeutic drugs in children with cancer. Eur. J. Clin. Pharmacol. 2013, 69, 1739–1746. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Lopez, E.; Gutierrez-Camino, A.; Astigarraga, I.; Navajas, A.; Echebarria-Barona, A.; Garcia-Miguel, P.; Garcia de Andoin, N.; Lobo, C.; Guerra-Merino, I.; Martin-Guerrero, I.; et al. Vincristine pharmacokinetics pathway and neurotoxicity during early phases of treatment in pediatric acute lymphoblastic leukemia. Pharmacogenomics 2016, 17, 731–741. [Google Scholar] [CrossRef]
- Zhou, X.J.; Rahmani, R. Preclinical and clinical pharmacology of vinca alkaloids. Drugs 1992, 4, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Goodson, H.V.; Jonasson, E.M. Microtubules and microtubule-associated proteins. Cold Spring Harb. Perspect. Biol. 2018, 1, 10. [Google Scholar] [CrossRef]
- Hara, M.; Fukagawa, T. Where is the right path heading from the centromere to spindle microtubules? Cell Cycle 2019, 18, 1199–1211. [Google Scholar] [CrossRef]
- Liu, Y.M.; Chen, H.L.; Lee, H.Y.; Liou, J.P. Tubulin inhibitors: A patent review. Expert Opin. Ther. Patents 2014, 24, 69–88. [Google Scholar] [CrossRef] [PubMed]
- Cormier, A.; Knossow, M.; Wang, C.; Gigant, B. The binding of vinca domain agents to tubulin: Structural and biochemical studies. Methods Cell Biol. 2010, 95, 373–390. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, F.; Budman, D.R. Review: Tubulin function, actions of antitubulin drugs, and new drug development. Cancer Investig. 2005, 23, 264–273. [Google Scholar] [CrossRef]
- Lobert, S.; Fahy, J.; Hill, B.T.; Duflos, A.; Etievant, C.; Correia, J.J. Vinca alkaloid-induced tubulin spiral formation correlates with cytotoxicity in the leukemic L1210 cell line. Biochemistry 2000, 39, 12053–12062. [Google Scholar] [CrossRef] [PubMed]
- Beck, W.T.; Cass, C.E.; Houghton, P.J. Microtubule-targeting anticancer drugs derived from plants and microbes: Vinca alkaloids, taxanes and epothiolones. In Holland-Frei Cancer Medicine, 5th ed.; Bast, R.C., Kufe, D.W., Pollock, R.E., Eds.; BC Decker Inc.: New York, NY, USA, 2003; pp. 680–698. [Google Scholar]
- Howard, S.M.H.; Theologides, A.; Sheppard, J.R. Comparative effects of vindesine, vinblastine, and vincristine on mitotic arrest and hormone response of L1210 leukemia cells. Cancer Res. 1980, 40, 2695. [Google Scholar]
- Ruggiero, A.; Ferrara, P.; Attinà, G.; Rizzo, D.; Riccardi, R. Renal toxicity and chemotherapy in children with cancer. Br. J. Clin. Pharmacol. 2017, 83, 2605–2614. [Google Scholar] [CrossRef] [PubMed]
- Baas, P.W.; Rao, A.N.; Matamoros, A.J.; Leo, L. Stability properties of neuronal microtubules. Cytoskeleton 2016, 73, 442–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starobova, H.; Vetter, I. Pathophysiology of chemotherapy-induced peripheral neuropathy. Front. Mol. Neurosci. 2017, 10, 174. [Google Scholar] [CrossRef]
- Lee, B.Y.; Hur, E.M. A role of microtubules in oligodendrocyte differentiation. Int. J. Mol. Sci. 2020, 21, 1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Old, E.A.; Nadkarni, S.; Grist, J.; Gentry, C.; Bevan, S.; Kim, K.W.; Mogg, A.J.; Perretti, M.; Malcangio, M. Monocytes expressing CX3CR1 orchestrate the development of vincristineinduced pain. J. Clin. Investig. 2014, 124, 2023–2036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, T.; Zhang, X.L.; Ou-Yang, H.D.; Li, Z.Y.; Liu, C.C.; Huang, Z.Z.; Xu, J.; Wei, J.Y.; Nie, B.L.; Ma, C.; et al. Epigenetic upregulation of CXCL12 expression mediates antitubulin chemotherapeutics-induced neuropathic pain. Pain 2017, 158, 637–648. [Google Scholar] [CrossRef]
- Canta, A.; Pozzi, E.; Carozzi, V.A. Mitochondrial dysfunction in chemotherapy-induced peripheral neuropathy (CIPN). Toxics 2015, 3, 198–223. [Google Scholar] [CrossRef] [Green Version]
- Tari, C.; Fournier, N.; Briand, C. Action of vinca alkaloides on calcium movements through mitochondrial membrane. Pharmacol. Res. Commun. 1986, 18, 519–528. [Google Scholar]
- Islam, B.; Lustberg, M.; Staff, N.P.; Kolb, N.; Alberti, P.; Argyriou, A.A. Vinca alkaloids, thalidomide and eribulin-induced peripheral neurotoxicity: From pathogenesis to treatment. J. Peripher. Nerv. Syst. 2019, 24, 63–73. [Google Scholar] [CrossRef]
- Marchi, S.; Patergnani, S.; Missiroli, S.; Morciano, G.; Rimessi, A.; Wieckowski, M.R.; Giorgi, C.; Pinton, P. Mitochondrial and endoplasmic reticulum calcium homeostasis and cell death. Cell. Calcium. 2018, 69, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Flatters, S.J.L.; Bennett, G.J. Studies of peripheral sensory nerves in paclitaxel-induced painful peripheral neuropathy: Evidence for mitochondrial dysfunction. Pain 2006, 122, 247–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Velde, M.E.; Kaspers, G.L.; Abbink, F.C.H.; Wilhelm, A.J.; Ket, J.C.F.; van den Berg, M.H. Vincristine-induced peripheral neuropathy in children with cancer: A systematic review. Crit. Rev. Oncol. Hematol. 2017, 114, 114–130. [Google Scholar] [CrossRef] [PubMed]
- Stadelmann, C.; Timmler, S.; Barrantes-Freer, A.; Simons, M. Myelin in the central nervous system: Structure, function, and pathology. Physiol. Rev. 2019, 99, 1381–1431. [Google Scholar] [CrossRef] [PubMed]
- De Graaf, S.S.; Bloemhof, H.; Vendrig, D.E.; Uges, D.R. Vincristine disposition in children with acute lymphoblastic leukemia. Med. Pediatr. Oncol. 1995, 24, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Crom, W.R.; De Graaf, S.S.; Synold, T.; Uges, D.R.; Bloemhof, H.; Rivera, G.; Christensen, M.L.; Mahmoud, H.; Evans, W.E. Pharmacokinetics of vincristine in children and adolescents with acute lymphocytic leukemia. J. Pediatr. 1994, 125, 642–649. [Google Scholar] [CrossRef]
- Wright, W.C.; Chenge, J.; Chen, T. Structural perspectives of the CYP3A family and their small molecule modulators in drug metabolism. Liver Res. 2019, 3, 132–142. [Google Scholar] [CrossRef]
- Dennison, J.B.; Kulanthaivel, P.; Barbuch, R.J.; Renbarger, J.L.; Ehlhardt, W.J.; Hall, S.D. Selective metabolism of vincristine in vitro by CYP3A5. Drug Metab. Dispos. 2006, 34, 1317–1327. [Google Scholar] [CrossRef] [Green Version]
- Aplenc, R.; Glatfelter, W.; Han, P.; Rappaport, E.; La, M.; Cnaan, A.; Blackwood, M.A.; Lange, B.; Rebbeck, T. CYP3A genotypes and treatment response in pediatric acute lymphoblastic leukaemia. Br. J. Haematol 2003, 122, 240–244. [Google Scholar] [CrossRef]
- Kishi, S.; Cheng, C.; French, D.; Pei, D.; Das, S.; Cook, E.H.; Hijiya, N.; Rizzari, C.; Rosner, G.L.; Frudakis, T.; et al. Ancestry and pharmacogenetics of antileukemic drug toxicity. Blood 2007, 109, 4151–4157. [Google Scholar] [CrossRef]
- Egbelakin, A.; Ferguson, M.J.; MacGill, E.A.; Lehmann, A.S.; Topletz, A.R.; Quinney, S.K.; Li, L.; McCammack, K.C.; Hall, S.D.; Renbarger, J.L. Increased risk of vincristine neurotoxicity associated with low CYP3A5 expression genotype in children with acute lymphoblastic leukemia. Pediatr. Blood Cancer 2011, 56, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Kayilioglu, H.; Kocak, U.; Kan Karaer, D.; Percin, E.F.; Sal, E.; Tekkesin, F.; Isik, M.; Oner, N.; Belen, F.B.; Yilmaz Keskin, E.; et al. Association of CYP3A5 expression and vincristine neurotoxicity in pediatric malignancies in Turkish population. J. Pediatr. Hematol. Oncol. 2017, 39, 458–462. [Google Scholar] [CrossRef]
- Skiles, J.L.; Chiang, C.; Li, C.H.; Martin, S.; Smith, E.L.; Olbara, G.; Jones, D.R.; Vik, T.A.; Mostert, S.; Abbink, F.; et al. CYP3A5 genotype and its impact on vincristine pharmacokinetics and development of neuropathhy in Kenyan children with cancer. Pediatr. Blood Cancer 2018, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smitherman, A.B.; Faircloth, C.B.; Deal, A.; Troy, M.; Gold, S.H. Vincristine toxicity with co-administration of fluconazole during induction therapy for pediatric acute lymphoblastic leukemia. Pediatr. Blood Cancer 2017, 64. [Google Scholar] [CrossRef] [PubMed]
- Sims, R.P. The effect of race on the CYP3A-mediated metabolism of vincristine in pediatric patients with acute lymphoblastic leukemia. J. Oncol. Pharm. Pract. 2016, 22, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Stock, W.; Diouf, B.; Crews, K.R.; Pei, D.; Cheng, C.; Laumann, K.; Mandrekar, S.J.; Luger, S.; Advani, A.; Stone, R.M.; et al. An inherited genetic variant in CEP72 promoter predisposes to vincristine-induced peripheral neuropathy in adults with acute lymphoblastic leukemia. Clin. Pharmacol. Ther. 2017, 101, 391–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutierrez-Camino, A.; Martin-Guerrero, I.; Lopez-Lopez, E.; Echebarria-Barona, A.; Zabalza, I.; Ruiz, I.; Guerra-Merino, I.; Garcia-Orad, A. Lack of association of the CEP72 RS924607 TT genotype with vincristine-related peripheral neuropathy during the early phase of pediatric acute lymphoblastic leukemia treatment in a Spanish population. Pharmacogenet. Genom. 2016, 26, 100–102. [Google Scholar] [CrossRef] [PubMed]
- Diouf, B.; Evans, W.E. Pharmacogenomics of Vincristine-induced peripheral neuropathy: Progress continues. Clin. Pharmacol. Ther. 2019, 105, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Wright, G.E.B.; Amstutz, U.; Drogemoller, B.I.; Shih, J.; Rassekh, S.R.; Hayden, M.R.; Carleton, B.C.; Ross, C.J.D. Pharmacogenomics of vincr istine-induced peripheral neuropat hyimplicates pharmacokinetic and inherited neuropathy genes. Clin. Pharmacol. Ther. 2018, 105, 402–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Sajdyk, T.; Smith, E.M.L.; Chang, C.W.; Li, C.; Ho, R.H.; Hutchinson, R.; Wells, E.; Skiles, J.L.; Winick, N.; et al. Genetic variants associated with vincristine-induced peripheral neuropathy in two populations of children with acute lymphoblastic leukemia. Clin. Pharmacol. Ther. 2019, 105, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Dudeja, S.; Gupta, S.; Sharma, S.; Jain, A.; Sharma, S.; Jain, P.; Aneja, S.; Chandra, J. Incidence of vincristine induced neurotoxicity in children with acute lymphoblastic leukemia and its correlation with nutritional deficiencies. Pediatr. Hematol. Oncol. 2019, 36, 344–351. [Google Scholar] [CrossRef]
- Sajdyk, T.J.; Boyle, F.A.; Foran, K.S.; Tong, Y.; Pandya, P.; Smith, E.M.L.; Ho, R.H.; Wells, E.; Renbarger, J.L. Obesity as a potential risk factor for Vincristine-induced peripheral neuropathy. J. Pediatr. Hematol. Oncol. 2020, 42, 637–640. [Google Scholar] [CrossRef] [PubMed]
- Kanbayashi, Y.; Hosokawa, T.; Okamoto, K.; Konishi, H.; Otsuji, E.; Yoshikawa, T.; Takagi, T.; Taniwaki, M. Statistical identification of predictors for peripheral neuropathy associated with administration of bortezomib, taxanes, oxaliplatin or vincristine using ordered logistic regression analysis. Anticancer Drugs 2010, 21, 877–881. [Google Scholar] [CrossRef] [PubMed]
- Lavoie Smith, E.M.; Li, L.; Chiang, C.; Thomas, K.; Hutchinson, R.J.; Wells, E.M.; Ho, R.H.; Skiles, J.; Chakraborty, A.; Bridges, C.M.; et al. Patterns and severity of vincristine-induced peripheral neuropathy in children with acute lymphoblastic leukemia. J. Peripher. Nerv. Syst. 2015, 20, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Rosca, L.; Robert-Boire, V.; Delisle, J.F.; Samson, Y.; Perreault, S. Carboplatin and vincristine neurotoxicity in the treatment of pediatric low-grade gliomas. Pediatr. Blood Cancer 2018, 65, 27351. [Google Scholar] [CrossRef]
- Van de Velde, M.E.; Kaspers, G.J.L.; Abbink, F.C.H.; Twisk, J.W.R.; van der Sluis, I.M.; van den Bos, C.; van den Heuvel-Eibrink, M.M.; Segers, H.; Chantrain, C.; van der Werff Ten Bosch, J.; et al. Vincristine-induced peripheral neuropathy in pediatric oncology: A randomized controlled trial comparing push injections with one-hour infusions (The VINCA Trial). Cancers 2020, 12, 3745. [Google Scholar] [CrossRef]
- Nikanjam, M.; Sun, A.; Albers, M.; Mangalindin, K.; Song, E.; Vempaty, H.; Sam, D.; Capparelli, E.V. Vincristine-associated neuropathy with antifungal usage: A Kaiser Northern California experience. J. Pediatr. Hematol. Oncol. 2018, 40, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Arena, R.; Battista, A.; Rizzo, D.; Attinà, G.; Riccardi, R. Azole interactions with multidrug therapy in pediatric oncology. Eur. J. Clin. Pharmacol. 2013, 69, 1–10. [Google Scholar] [CrossRef]
- Moriyama, B.; Henning, S.A.; Leung, J.; Falade-Nwulia, O.; Jarosinski, P.; Penzak, S.R.; Walsh, T.J. Adverse interactions between antifungal azoles and vincristine: Review and analysis of cases. Mycoses 2012, 55, 290–297. [Google Scholar] [CrossRef]
- Thackray, J.; Spatz, K.; Steinherz, P.G. Vincristine toxicity with co-administration of fluconazole: Long-term concerns. Pediatr. Blood Cancer 2017, 64, 12. [Google Scholar] [CrossRef]
- Bellmann, R.; Smuszkiewicz, P. Pharmacokinetics of antifungal drugs: Practical implications for optimized treatment of patients. Infection 2017, 45, 737–779. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.J.; Paul, M.R.; Kuo, D.J. Severe neuropathic pain with concomitant administration of Vincristine and Posaconazole. J. Pediatr. Pharmacol. Ther. 2018, 23, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Jeng, M.R.; Feusner, J. Itraconazole-enhanced vincristine neurotoxicity in a child with acute lymphoblastic leukemia. Pediatr. Hematol. Oncol. 2001, 18, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Bermúdez, M.; Fuster, J.L.; Llinares, E.; Galera, A.; Gonzalez, C. Itraconazole-related increased vincristine neurotoxicity: Case report and review of literature. J. Pediatr. Hematol. Oncol. 2005, 27, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Van Schie, R.M.; Brüggemann, R.J.; Hoogerbrugge, P.M.; te Loo, D.M. Effect of azole antifungal therapy on vincristine toxicity in childhood acute lymphoblastic leukaemia. J. Antimicrob. Chemother. 2011, 66, 1853–1856. [Google Scholar] [CrossRef] [PubMed]
- Pana, Z.D.; Roilides, E. Risk of azole-enhanced vincristine neurotoxicity in pediatric patients with hematological malignancies: Old problem–new dilemma. Pediatr. Blood Cancer 2011, 57, 30–35. [Google Scholar] [CrossRef]
- Ruggiero, A.; Rizzo, D.; Catalano, M.; Coccia, P.; Triarico, S.; Attiná, G. Acute chemotherapy-induced nausea and vomiting in children with cancer: Still waiting for a common consensus on treatment. J. Int. Med. Res. 2018, 46, 2149–2156. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.K.; Bossaer, J.B.; Lewis, P.O.; Sant, A. Peripheral neuropathy in non-Hodgkin’s lymphoma patients receiving vincristine with and without aprepitant/fosaprepitant. J. Oncol. Pharm. Pract. 2020, 26, 809–813. [Google Scholar] [CrossRef]
- Anghelescu, D.L.; Faughnan, L.G.; Jeha, S.; Relling, M.V.; Hinds, P.S.; Sandlund, J.T.; Cheng, C.; Pei, D.; Hankins, G.; Pauley, J.L.; et al. Neuropathic pain during treatment for childhood acute lymphoblastic leukemia. Pediatr. Blood Cancer 2011, 57, 1147–1153. [Google Scholar] [CrossRef] [Green Version]
- Anghelescu, D.L.; Tesney, J.M.; Jeha, S.; Wright, B.B.; Trujillo, L.; Sandlund, J.T.; Pauley, J.; Cheng, C.; Pei, D.; Pui, C.H. Prospective randomized trial of interventions for vincristine-related neuropathic pain. Pediatr. Blood Cancer 2020, 67, 28539. [Google Scholar] [CrossRef]
- Jackson, D.V.; Pope, E.K.; McMahan, R.A.; Cooper, M.R.; Atkins, J.N.; Callahan, R.D.; Paschold, E.H.; Grimm, R.A.; Hopkins, J.O.; Muss, H.B.; et al. Clinical trial of pyridoxine to reduce vincristine neurotoxicity. J. Neurooncol. 1986, 4, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Battle, W.M.; Cohen, J.D.; Snape, W.J. Disorders of colonic motility in patients with diabetes mellitus. Yale J. Biol. Med. 1983, 56, 277–283. [Google Scholar] [PubMed]
- Müller, L.; Kramm, C.M.; Tenenbaum, T.; Wessalowski, R.; Göbel, U. Treatment of vincristine-induced bilateral ptosis with pyridoxine and pyridostigmine. Pediatr. Blood Cancer 2004, 42, 287–288. [Google Scholar] [CrossRef] [PubMed]
- Akbayram, S.; Akgun, C.; Doğan, M.; Sayin, R.; Caksen, H.; Oner, A.F. Use of pyridoxine and pyridostigmine in children with vincristine-induced neuropathy. Indian J. Pediatr. 2010, 77, 681–683. [Google Scholar] [CrossRef] [PubMed]
- Aydin Köker, S.; Gözmen, S.; Demirağ, B.; Ünalp, A.; Karapinar, T.H.; Oymak, Y.; Gürbüz, G.; Öner, E.İ.; Vergin, R.C. Effect of pyridoxine plus pyridostigmine treatment on vincristine-induced peripheral neuropathy in pediatric patients with acute lymphoblastic leukemia: A single-center experience. Neurol. Sci. 2021. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.V.; Wells, H.B.; Atkins, J.N.; Zekan, P.J.; White, D.R.; Richards, F.; Cruz, J.M.; Muss, H.B. Amelioration of vincristine neurotoxicity by glutamic acid. Am. J. Med. 1988, 84, 1016–1022. [Google Scholar] [CrossRef]
- Bradfield, S.M.; Sandler, E.; Geller, T.; Tamura, R.N.; Krischer, J.P. Glutamic acid not beneficial for the prevention of vincristine neurotoxicity in children with cancer. Pediatr. Blood Cancer 2015, 62, 1004–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokhtar, G.M.; Shaaban, S.Y.; Elbarbary, N.S.; Fayed, W.A. A trial to assess the efficacy of glutamic acid in prevention of vincristine-induced neurotoxicity in pediatric malignancies: A pilot study. J. Pediatr. Hematol. Oncol. 2010, 32, 594–600. [Google Scholar] [CrossRef]
- Jackson, D.V.; Rosenbaum, D.L.; Carlisle, L.J.; Long, T.R.; Wells, H.B.; Spurr, C.L. Glutamic acid modification of vincristine toxicity. Cancer Biochem. Biophys. 1984, 7, 245–252. [Google Scholar]
- Boyle, F.M.; Wheeler, H.R.; Shenfield, G.M. Amelioration of experimental cisplatin and paclitaxel neuropathy with glutamate. J. Neurooncol. 1999, 41, 107–116. [Google Scholar] [CrossRef]
- Sands, S.; Ladas, E.J.; Kelly, K.M.; Weiner, M.; Lin, M.; Ndao, D.H.; Dave, A.; Vahdat, L.T.; Bender, J.G. Glutamine for the treatment of vincristine-induced neuropathy in children and adolescents with cancer. Support Care Cancer 2017, 25, 701–708. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Risk Factor | Mechanism | Reference |
|---|---|---|
| Dose | Higher dose of vincristine could facilitate VIPN | [34,55] |
| Administration schedule | Dosing closely may increase the risk of VIPN | [36] |
| Method of administration | Prolonged administration could reduce the risk of VIPN compared to IV bolus administration | [34] |
| Concomitant use of other drugs | Azoles, aprepitant and fosaprepitant inhibit CYP3A4, increasing the risk of VIPN | [59,60,61,62,63,67,68,69] |
| Drug | Dosage | Patients Age (in Years) | Outcome | Reference |
|---|---|---|---|---|
| Gabapentin | 5–10 mg/kg/day (max 50–70 mg/kg/day) | 1–18 | No evidence of superiority over opioids for reducing or preventing VIPN pain | [72] |
| Pyridoxine | 150 mg/sqm/day | 2–13 | Complete resolution of symptoms of VIPN | [76] |
| Pyridostigmine | 3 mg/kg/day | 2–13 | Complete resolution of symptoms of VIPN | [76] |
| Pyridoxine and Pyridostigmine | 150 mg/sqm/day and 3 mg/kg/day | 2–10 | Significantly improvement of symptoms | [77] |
| Glutamic acid | 250 mg daily for BSA * < 1 sqm, 500 mg daily for BSA ≥ 1 sqm | Prevention of VIPN only in patients aged 13 years or more | [79] | |
| 1.5 g daily (on the day before or on the day of the first dose of VCR) | 3–18 | Reduced occurrence of VIPN | [80] | |
| Glutamine | 6 g/sqm twice daily for 21 days | 5–21 | Improvement in sensory function and QoL ** | [83] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Triarico, S.; Romano, A.; Attinà, G.; Capozza, M.A.; Maurizi, P.; Mastrangelo, S.; Ruggiero, A. Vincristine-Induced Peripheral Neuropathy (VIPN) in Pediatric Tumors: Mechanisms, Risk Factors, Strategies of Prevention and Treatment. Int. J. Mol. Sci. 2021, 22, 4112. https://doi.org/10.3390/ijms22084112
Triarico S, Romano A, Attinà G, Capozza MA, Maurizi P, Mastrangelo S, Ruggiero A. Vincristine-Induced Peripheral Neuropathy (VIPN) in Pediatric Tumors: Mechanisms, Risk Factors, Strategies of Prevention and Treatment. International Journal of Molecular Sciences. 2021; 22(8):4112. https://doi.org/10.3390/ijms22084112
Chicago/Turabian StyleTriarico, Silvia, Alberto Romano, Giorgio Attinà, Michele Antonio Capozza, Palma Maurizi, Stefano Mastrangelo, and Antonio Ruggiero. 2021. "Vincristine-Induced Peripheral Neuropathy (VIPN) in Pediatric Tumors: Mechanisms, Risk Factors, Strategies of Prevention and Treatment" International Journal of Molecular Sciences 22, no. 8: 4112. https://doi.org/10.3390/ijms22084112