Safety and Effectiveness of Copaiba Oleoresin (C. reticulata Ducke) on Inflammation and Tissue Repair of Oral Wounds in Rats

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Results
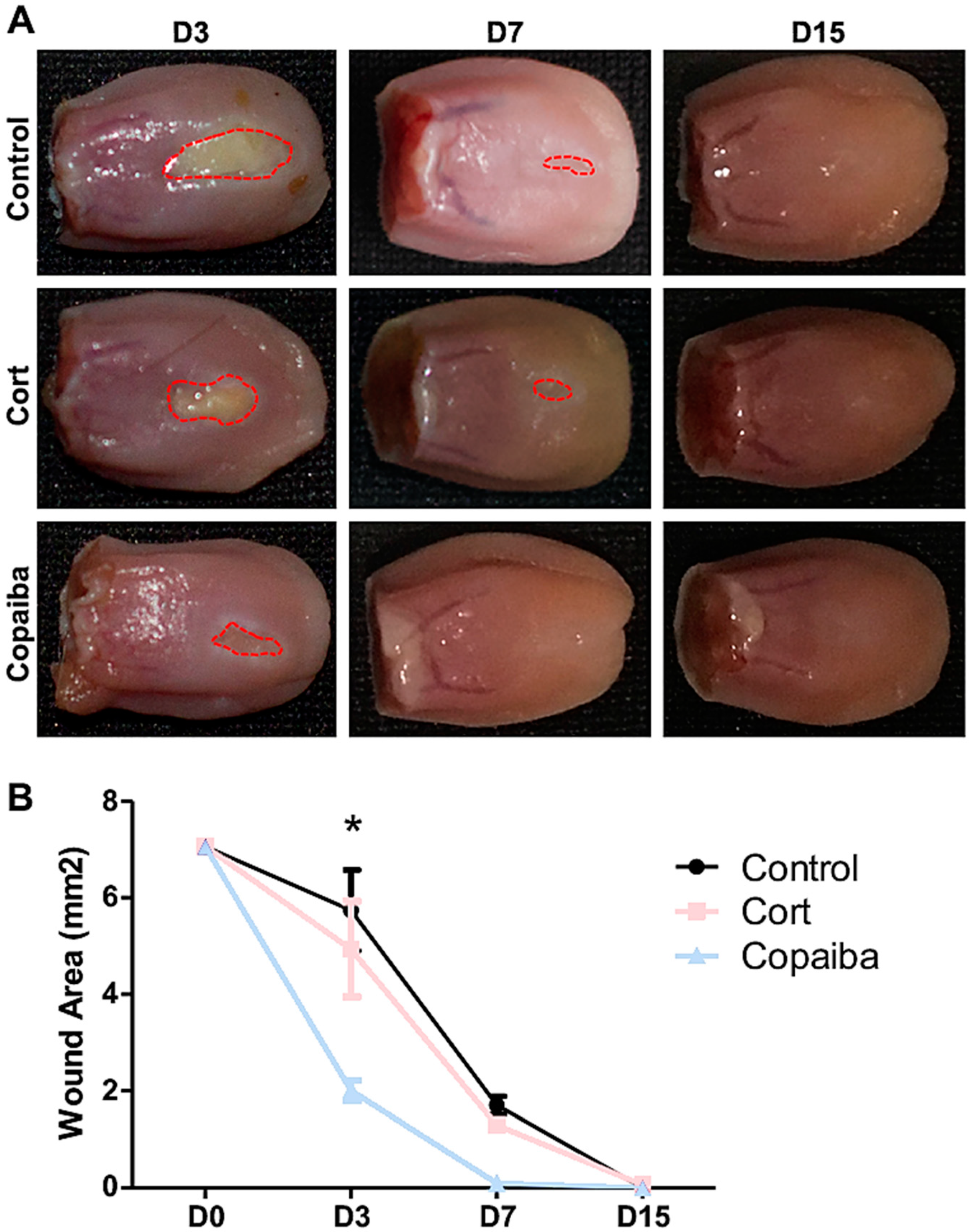
2.1. Copaiba Oleoresin Accelerates the Wound Contraction
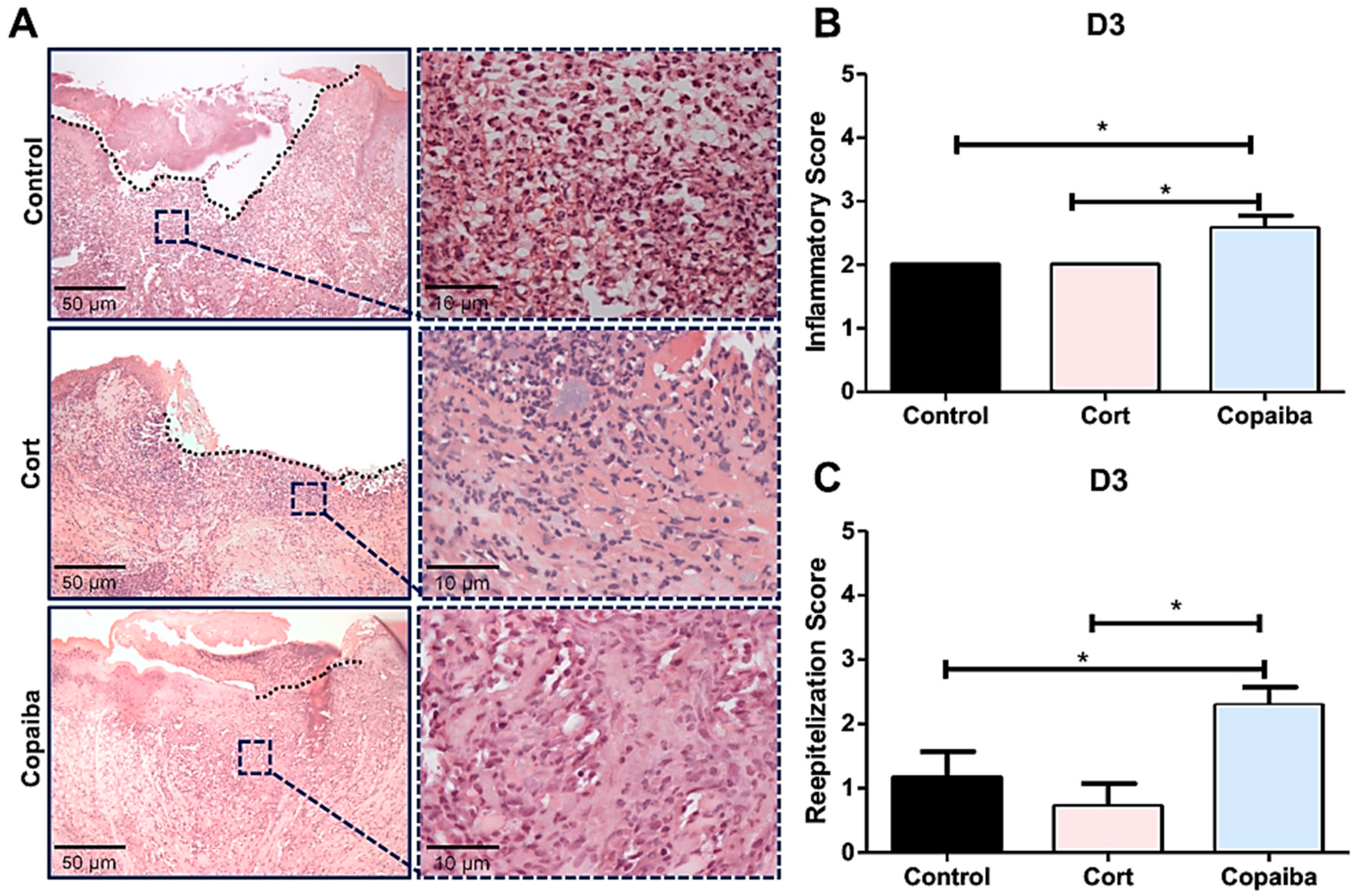
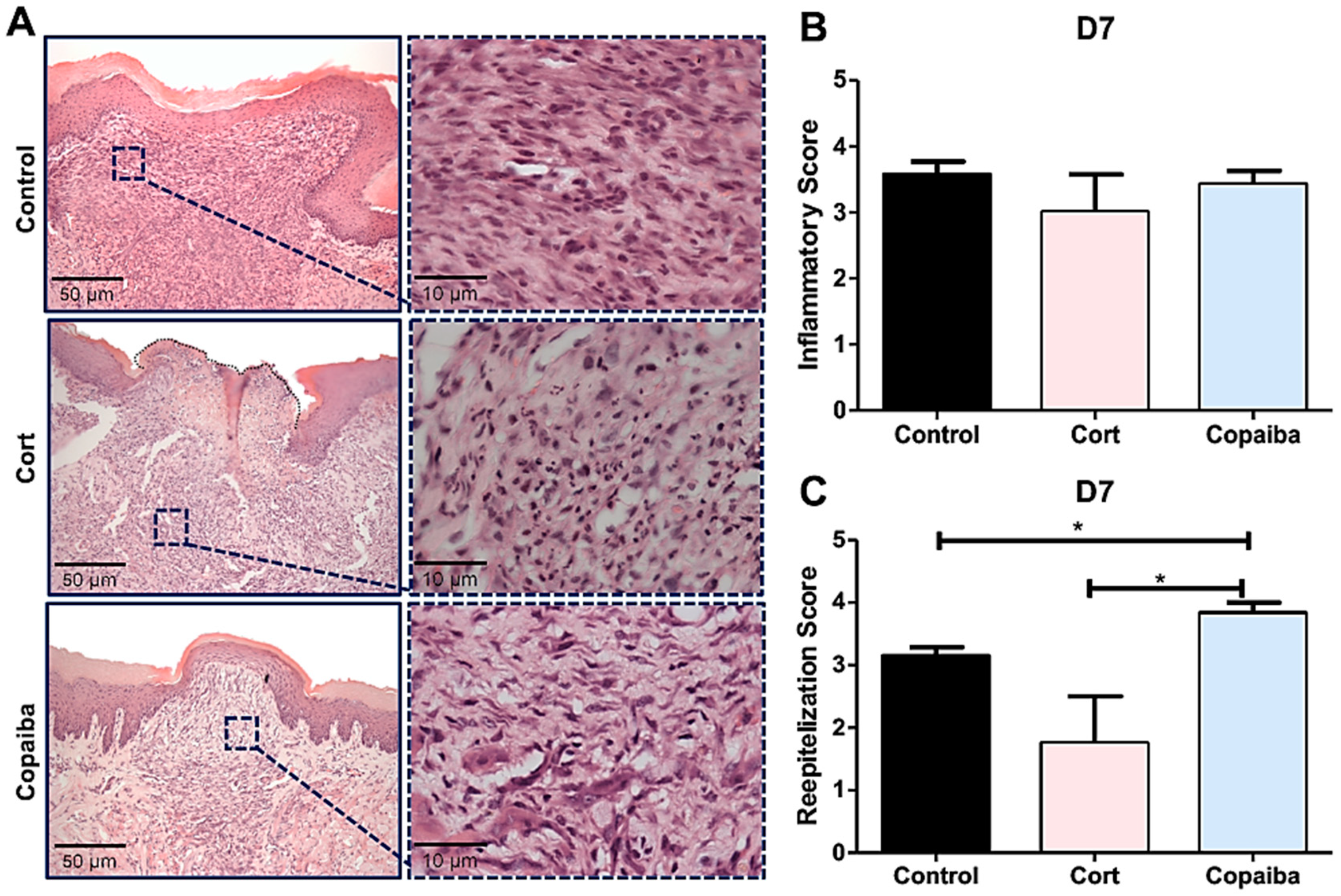
2.2. Copaiba Oleoresin Modulates Inflammatory Process and Accelerates Reepithelization
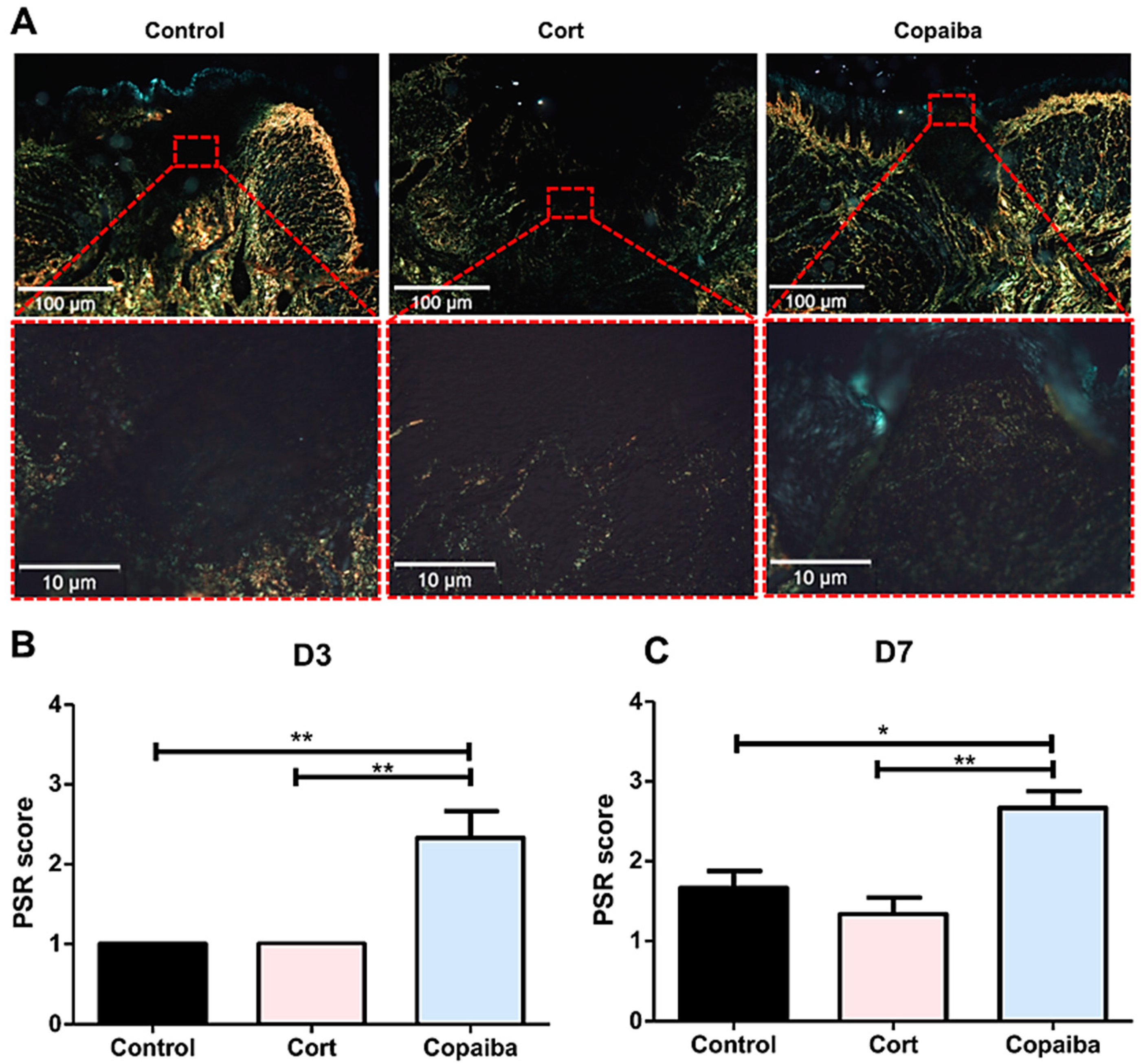
2.3. Copaiba Oleoresin Promoted Collagen Formation
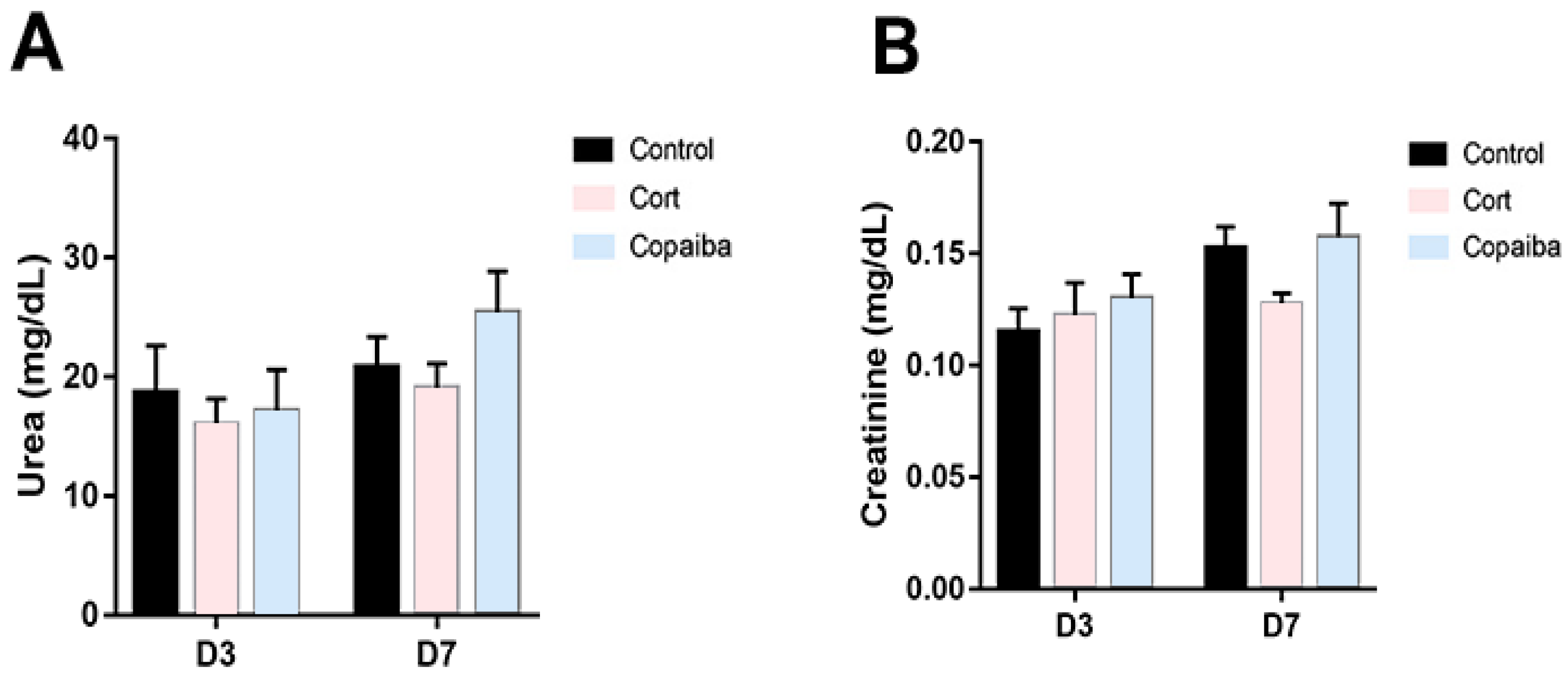
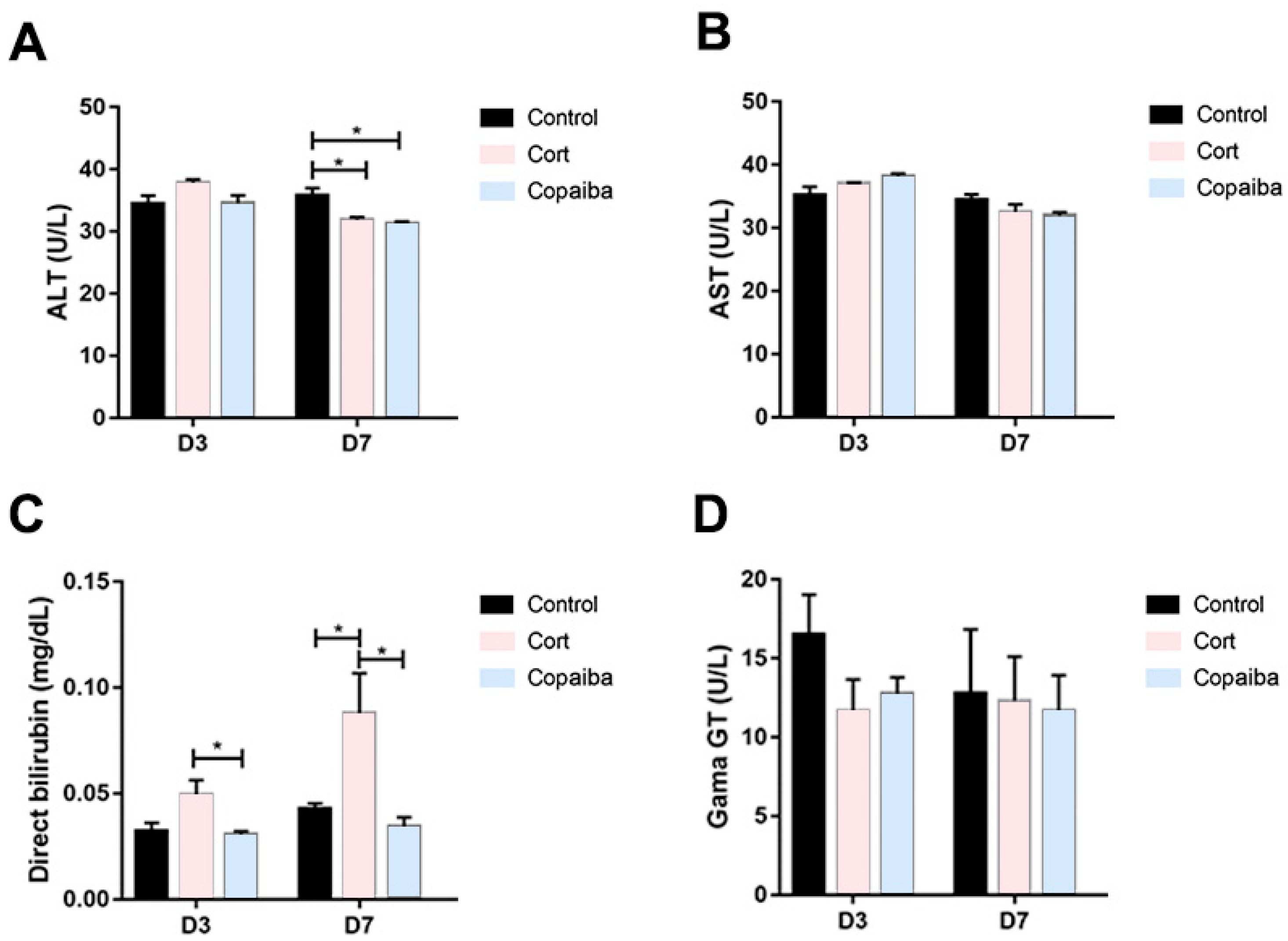
2.4. The Dosage of Copaiba Administered Concluded to Be Safe for Liver and Kidneys
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Plant Material, Characterization and Acute Oral Toxicity Test
4.3. Animals and Experimental Protocol
4.3.1. Animals
4.3.2. Experimental Groups and Wounding Method
4.4. Clinical Analysis
4.5. Histopathological ANALYSES
4.6. PicroSirius Red Staining
4.7. Analysis of Selected Biochemical Parameters of Liver and Kidney Functions
4.8. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| MED | Minimum Effective Dose |
| CTG | Corticoid Group |
| COG | Copaiba Group |
| CG | Control Group |
| D3 | Day 3 |
| D7 | Day 7 |
| D15 | Day 15 |
| HE | Hematoxylin and Eosin |
| DL50 | Median Lethal Dose |
| GC-MS | Gas Chromatography - Mass Spectrometry |
| OECD | Organization for Economic Cooperation and Develpment |
| UFPA | Federal University of Pará |
| CEUA | Ethics Committee on the Use of Animals |
| ARRIVE | Animal Research: Reporting of In Vivo Experiments |
| CONCEA | National Council for Animal Control and Experimentation |
| ALT | Alanine Aminotransferase |
| AST | Aspartate Aminotransferase |
| CAPES | Coordination for Improvement of Higher Education Personnel |
| CNPq | Brazilian National Council for Scientific and Technological Development |
| EMBRAPA | Brazilian Agricultural Research Corporation |
| PROCAD | National Academic Cooperation Program |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Constituents | % |
|---|---|
| δ-Elemene | 0.2 |
| Cyclosativene | 0.9 |
| α-Copaene | 0.5 |
| β-Elemene | 3.3 |
| β-Caryophyllene | 37.6 |
| trans-α-Bergamotene | 9.3 |
| Aromadendrene | 0.9 |
| epi-β-Santalene | 0.1 |
| α-Humulene + (E)-β-farnesene | 5.3 |
| β-Chamigrene | 0.9 |
| γ-Gurjunene | 0.6 |
| γ-Curcumene | 0.6 |
| β-Selinene | 4.9 |
| α-Selinene | 3.1 |
| (Z)-α-Bisabolene | 1.8 |
| α-Bulnesene | 2.1 |
| β-Bisabolene | 13.9 |
| β-Curcumene | 0.4 |
| β-Sesquiphellandrene | 1.1 |
| (E)-γ-Bisabolene | 1.3 |
| Caryophyllene oxide | 0.2 |
| epi-β-Bisabolol | 0.1 |
| β-Bisabolol | 0.2 |
References
- Mortazavi, H.; Safi, Y.; Baharvand, M.; Rahmani, S. Diagnostic Features of Common Oral Ulcerative Lesions: An Updated Decision Tree. Int. J. Dent. 2016, 2016, 7278925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minhas, S.; Sajjad, A.; Kashif, M.; Taj, F.; Al Waddani, H.; Khurshid, Z. Oral Ulcers Presentation in Systemic Diseases: An Update. Open Access Maced. J. Med Sci. 2019, 7, 3341–3347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munoz-Corcuera, M.; Esparza-Gómez, G.; González-Moles, M.; Bascones-Martínez, A. Oral ulcers: Clinical aspects. A tool for dermatologists. Part I. Acute ulcers. Clin. Exp. Dermatol. 2009, 34, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Dhopte, A.; Naidu, G.; Singh-Makkad, R.; Nagi, R.; Bagde, H.; Jain, S. Psychometric analysis of stress, anxiety and depression in patients with recurrent aphthous Stomatitis-A cross-sectional survey based study. J. Clin. Exp. Dent. 2018, 10, e1109–e1114. [Google Scholar] [CrossRef]
- Gutkowski, K.; Chwist, A.; Hartleb, M. Liver injury induced by high-dose methylprednisolone therapy: A case report and brief review of the literature. Hepat. Mon. 2011, 11, 656–661. [Google Scholar] [CrossRef] [Green Version]
- Levin, C.; Maibach, H.I. Topical corticosteroid-induced adrenocortical insufficiency: Clinical implications. Am. J. Clin. Dermatol. 2002, 3, 141–147. [Google Scholar] [CrossRef]
- Petrovska, B.B. Historical review of medicinal plants’ usage. Pharmacogn. Rev. 2012, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- Miranda, L.L.; Guimarães-Lopes, V.D.P.; Altoé, L.S.; Sarandy, M.M.; Melo, F.C.S.A.; Novaes, R.D.; Gonçalves, R.V. Plant Extracts in the Bone Repair Process: A Systematic Review. Mediat. Inflamm. 2019, 2019, 1296153. [Google Scholar] [CrossRef]
- Valli, M.; Russo, H.M.; Bolzani, V.S. The potential contribution of the natural products from Brazilian biodiversity to bioeconomy. Anais da Academia Brasileira de Ciências 2018, 90, 763–778. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, V.P.; Arruda, C.; Abd El-Salam, M.; Bastos, J.K. Brazilian medicinal plants with corroborated anti-inflammatory activities: A review. Pharm. Biol. 2018, 56, 253–268. [Google Scholar] [CrossRef] [Green Version]
- Caesar, L.K.; Cech, N.B. Synergy and antagonism in natural product extracts: When 1 + 1 does not equal 2. Nat. Prod. Rep. 2019, 36, 869–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Junior, V.V.; Rosas, E.C.; Carvalho, M.V.D.; Henriques, M.D.G.M.D.O.; Pinto, A.C. Chemical composition and anti-inflammatory activity of copaiba oils from Copaifera cearensis Huber ex Ducke, Copaifera reticulata Ducke and Copaifera multijuga Hayne—A comparative study. J. Ethnopharmacol. 2007, 112, 248–254. [Google Scholar]
- Da Trindade, R.; da Silva, J.K.; Setzer, W.N. Copaifera of the Neotropics: A Review of the Phytochemistry and Pharmacology. Int. J. Mol. Sci. 2018, 19, 1511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, V.P.; Webber, L.P.; Ortiz, L.; Rados, P.V.; Meurer, L.; Lameira, O.A.; Lima, R.R.; Martins, M.D. Effects of copaiba oil topical administration on oral wound healing. Phytother. Res. 2017, 31, 1283–1288. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, C.; Blanchet, M.R.; Laviolette, M.; Flamand, N. The CB(2) receptor and its role as a regulator of inflammation. Cell. Mol. life Sci. CMLS 2016, 73, 4449–4470. [Google Scholar] [CrossRef] [Green Version]
- Koyama, S.; Purk, A.; Kaur, M.; Soini, H.A.; Novotny, M.V.; Davis, K.; Kao, C.C.; Matsunami, H.; Mescher, A. Beta-caryophyllene enhances wound healing through multiple routes. PLoS ONE 2019, 14, e0216104. [Google Scholar] [CrossRef] [Green Version]
- Satsu, H.; Matsuda, T.; Toshimitsu, T.; Mori, A.; Mae, T.; Tsukagawa, M.; Kitahara, M.; Shimizu, M. Regulation of interleukin-8 secretion in human intestinal epithelial Caco-2 cells by alpha-humulene. Biofactors 2004, 21, 137–139. [Google Scholar] [CrossRef]
- Teixeira, F.B.; de Brito Silva, R.; Lameira, O.A.; Webber, L.P.; Couto, R.S.D.A.; Martins, M.D.; Lima, R.R. Copaiba oil-resin (Copaifera reticulata Ducke) modulates the inflammation in a model of injury to rats’ tongues. BMC Complementary Altern. Med. 2017, 17, 313. [Google Scholar] [CrossRef] [Green Version]
- Koenig, G.; Seneff, S. Gamma-Glutamyltransferase: A Predictive Biomarker of Cellular Antioxidant Inadequacy and Disease Risk. Dis. Markers 2015, 2015, 818570. [Google Scholar] [CrossRef] [Green Version]
- Nisha, R.; Kannan, S.S.; Jagatha, P. Biochemical evaluation of creatinine and urea in patients with renal failure undergoing hemodialysis. J. Clin. Pathol. Lab. Med. 2017, 1, 49732651. [Google Scholar]
- Iglesias-Bartolome, R.; Uchiyama, A.; Molinolo, A.A.; Abusleme, L.; Brooks, S.R.; Callejas-Valera, J.L.; Edwards, D.; Doci, C.; Asselin-Labat, M.L.; Onaitis, M.W.; et al. Transcriptional signature primes human oral mucosa for rapid wound healing. Sci. Transl. Med. 2018, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra, M.B.; Barroso, W.A.; Silva, N.N.D.; Silva, S.D.N.; Borges, A.C.R.; Abreu, I.C.; Borges, M.O.D.R. From Inflammation to Current and Alternative Therapies Involved in Wound Healing. Int. J. Inflamm. 2017, 2017, 3406215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wynn, T.A.; Barron, L. Macrophages: Master regulators of inflammation and fibrosis. Semin. Liver Dis. 2010, 30, 245–257. [Google Scholar] [CrossRef] [Green Version]
- Logie, J.J.; Ali, S.; Marshall, K.M.; Heck, M.M.; Walker, B.R.; Hadoke, P.W. Glucocorticoid-mediated inhibition of angiogenic changes in human endothelial cells is not caused by reductions in cell proliferation or migration. PLoS ONE 2010, 5, e14476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legault, J.; Pichette, A. Potentiating effect of beta-caryophyllene on anticancer activity of alpha-humulene, isocaryophyllene and paclitaxel. J. Pharm. Pharmacol. 2007, 59, 1643–1647. [Google Scholar] [CrossRef]
- Darby, I.A.; Laverdet, B.; Bonté, F.; Desmoulière, A. Fibroblasts and myofibroblasts in wound healing. Clin. Cosmet. Investig. Dermatol. 2014, 7, 301–311. [Google Scholar]
- Paiva, L.A.; Gurgel, L.A.; De Sousa, E.T.; Silveira, E.R.; Silva, R.M.; Santos, F.A.; Rao, V.S.N. Protective effect of Copaifera langsdorffii oleo-resin against acetic acid-induced colitis in rats. J. Ethnopharmacol. 2004, 93, 51–56. [Google Scholar] [CrossRef]
- Guimarães-Santos, A.; Santos, D.S.; Santos, I.R.; Lima, R.R.; Pereira, A.; de Moura, L.S.; Carvalho, R.N.; Lameira, O.; Gomes-Leal, W. Copaiba oil-resin treatment is neuroprotective and reduces neutrophil recruitment and microglia activation after motor cortex excitotoxic injury. Evid.-Based Complementary Altern. Med. eCAM 2012, 2012, 918174. [Google Scholar] [CrossRef] [Green Version]
- Almeida, M.R.; Almeida, M.R.; Darin, J.D.; Hernandes, L.C.; Ramos, M.F.D.S.; Antunes, L.M.G.; Freitas, O.D. Genotoxicity assessment of Copaiba oil and its fractions in Swiss mice. Genet. Mol. Biol. 2012, 35, 664–672. [Google Scholar] [CrossRef]
- Pramick, M.; Whitmore, S.E. Cushing’s syndrome caused by mucosal corticosteroid therapy. Int. J. Dermatol. 2009, 48, 100–101. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Animal research: Reporting in vivo experiments: The ARRIVE guidelines. Br. J. Pharmacol. 2010, 160, 1577–1579. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jornet, P.; Camacho-Alonso, F. Oral and dental complications of intra-oral piercing. J. Adolesc. Health 2006, 39, 767–769. [Google Scholar] [CrossRef] [PubMed]
- Sinha, U.K.; Gallagher, L.A. Effects of steel scalpel, ultrasonic scalpel, CO2 laser, and monopolar and bipolar electrosurgery on wound healing in guinea pig oral mucosa. Laryngoscope 2003, 113, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Melo, V.A.; Anjos, D.C.S.D.; Albuquerque Júnior, R.; Melo, D.B.; Carvalho, F.U.R. Effect of low level laser on sutured wound healing in rats. Acta Cir. Bras. 2011, 26, 129–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]







| Treatment Group (Sample Size) | Doses Administered by Oral Gavage |
|---|---|
| Control (n = 15) | 200 mg/kg/day of saline solution and Tween 20 at 5% |
| Corticoid (n = 15) | 0.5 mg/kg/day of Dexamethasone |
| Copaiba (n = 15) | 200 mg/kg/day of Copaiba oleoresin |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvarenga, M.O.P.; Bittencourt, L.O.; Mendes, P.F.S.; Ribeiro, J.T.; Lameira, O.A.; Monteiro, M.C.; Barboza, C.A.G.; Martins, M.D.; Lima, R.R. Safety and Effectiveness of Copaiba Oleoresin (C. reticulata Ducke) on Inflammation and Tissue Repair of Oral Wounds in Rats. Int. J. Mol. Sci. 2020, 21, 3568. https://doi.org/10.3390/ijms21103568
Alvarenga MOP, Bittencourt LO, Mendes PFS, Ribeiro JT, Lameira OA, Monteiro MC, Barboza CAG, Martins MD, Lima RR. Safety and Effectiveness of Copaiba Oleoresin (C. reticulata Ducke) on Inflammation and Tissue Repair of Oral Wounds in Rats. International Journal of Molecular Sciences. 2020; 21(10):3568. https://doi.org/10.3390/ijms21103568
Chicago/Turabian StyleAlvarenga, María Olimpia Paz, Leonardo Oliveira Bittencourt, Paulo Fernando Santos Mendes, Julia Turra Ribeiro, Osmar Alves Lameira, Marta Chagas Monteiro, Carlos Augusto Galvão Barboza, Manoela Domingues Martins, and Rafael Rodrigues Lima. 2020. "Safety and Effectiveness of Copaiba Oleoresin (C. reticulata Ducke) on Inflammation and Tissue Repair of Oral Wounds in Rats" International Journal of Molecular Sciences 21, no. 10: 3568. https://doi.org/10.3390/ijms21103568