Immunotherapy for Uterine Cervical Cancer Using Checkpoint Inhibitors: Future Directions

 , and
, and
Abstract
:1. Introduction
2. Cervical Cancer Immunopathogenesis Associated with Effects of ICIs
3. Evidence from Clinical Research for Cervical Cancer with ICIs
4. Future Directions of Immunotherapy for Cervical Cancer
4.1. Chemotherapy with ICIs for Cervical Cancer
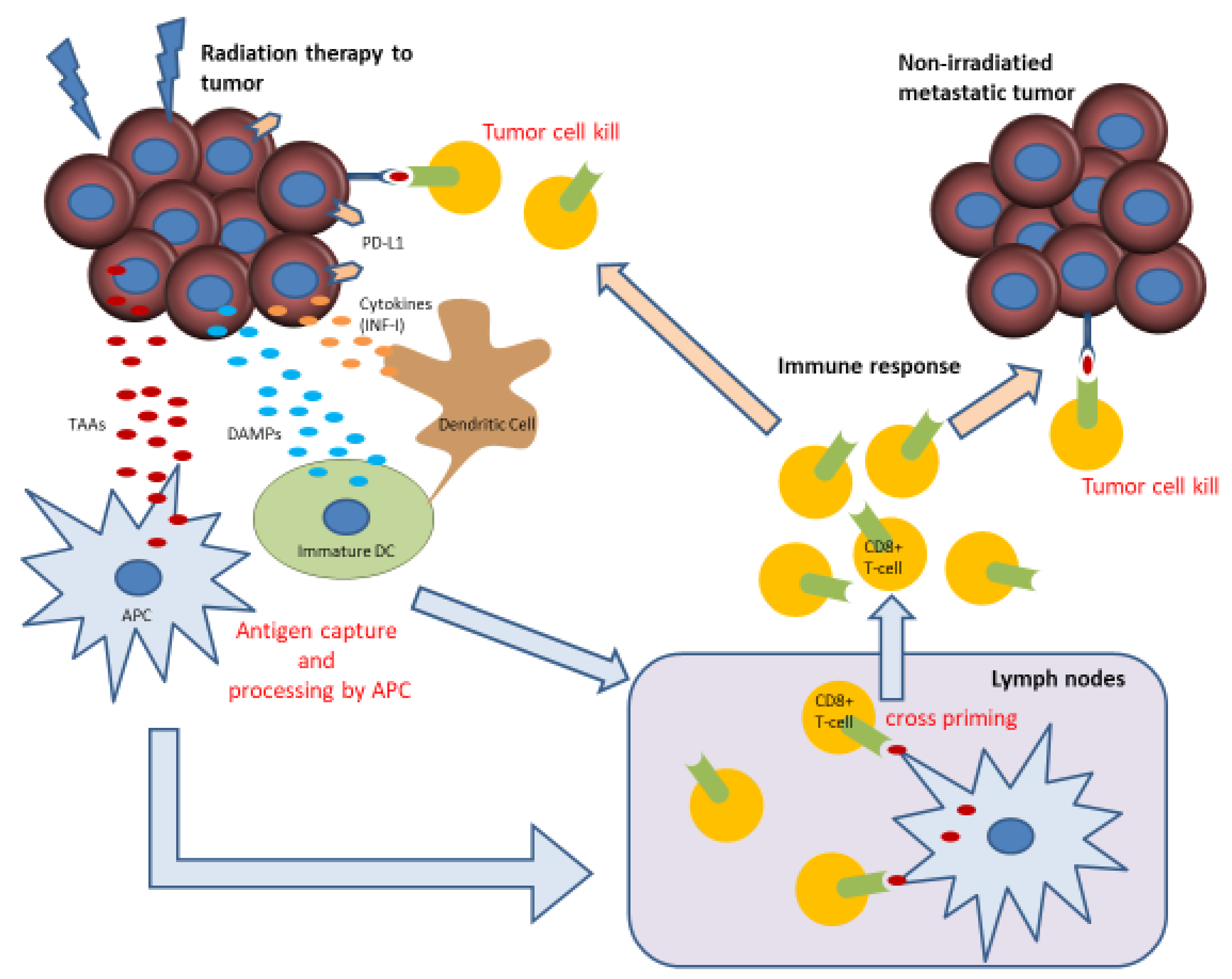
4.2. Concurrent Chemoradiation Therapy (CCRT) with ICIs for Cervical Cancer
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef] [Green Version]
- Hamanishi, J.; Mandai, M.; Konishi, I. Immune checkpoint inhibition in ovarian cancer. Int. Immunol. 2016, 28, 339–348. [Google Scholar] [CrossRef] [Green Version]
- Iwai, Y.; Hamanishi, J.; Chamoto, K.; Honjo, T. Cancer immunotherapies targeting the PD-1 signaling pathway. J. Biomed. Sci. 2017, 24, 26. [Google Scholar] [CrossRef] [Green Version]
- Cancer; IAfRo. Cancer Fact Sheets: Cervical Cancer. Available online: http://gco.iarc.fr/today/data/pdf/factsheets/cancers/cancer-fact-sheets-16.pdf (accessed on 20 July 2019).
- Koh, W.J.; Abu-Rustum, N.R.; Bean, S.; Bradley, K.; Campos, S.M.; Cho, K.R.; Chon, H.S.; Chu, C.; Clark, R.; Cohn, D.; et al. NCCN Guidelines Panel Disclosures EmilyWyse Patient Advocate NCCN Guidelines Version 2.2018 Cervical Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf (accessed on 20 July 2019).
- Tewari, K.S.; Sill, M.W.; Long, H.J., 3rd; Penson, R.T.; Huang, H.; Ramondetta, L.M.; Landrum, L.M.; Oaknin, A.; Reid, T.J.; Leitao, M.M.; et al. Improved survival with bevacizumab in advanced cervical cancer. N. Engl. J. Med. 2014, 370, 734–743. [Google Scholar] [CrossRef] [Green Version]
- Kagabu, M.; Nagasawa, T.; Fukagawa, D.; Tomabechi, H.; Sato, S.; Shoji, T.; Baba, T. Immunotherapy for Uterine Cervical Cancer. Healthcare (Basel) 2019, 7, 108. [Google Scholar] [CrossRef] [Green Version]
- Chung, H.C.; Ros, W.; Delord, J.P.; Perets, R.; Italiano, A.; Shapira-Frommer, R.; Manzuk, L.; Piha-Paul, S.A.; Xu, L.; Zeigenfuss, S.; et al. Efficacy and Safety of Pembrolizumab in Previously Treated Advanced Cervical Cancer: Results From the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2019, 37, 1470–1478. [Google Scholar] [CrossRef]
- Trujillo, J.A.; Sweis, R.F.; Bao, R.; Luke, J.J. T Cell-Inflamed versus Non-T Cell-Inflamed Tumors: A Conceptual Framework for Cancer Immunotherapy Drug Development and Combination Therapy Selection. Cancer Immunol. Res. 2018, 6, 990–1000. [Google Scholar] [CrossRef] [Green Version]
- Balermpas, P.; Martin, D.; Wieland, U.; Rave-Frank, M.; Strebhardt, K.; Rodel, C.; Fokas, E.; Rodel, F. Human papilloma virus load and PD-1/PD-L1, CD8(+) and FOXP3 in anal cancer patients treated with chemoradiotherapy: Rationale for immunotherapy. Oncoimmunology 2017, 6, e1288331. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Lu, J.; Tian, H.; Du, W.; Zhao, L.; Feng, J.; Yuan, D.; Li, Z. Increased expression of PDL1 by the human papillomavirus 16 E7 oncoprotein inhibits anticancer immunity. Mol. Med. Rep. 2017, 15, 1063–1070. [Google Scholar] [CrossRef] [Green Version]
- Mezache, L.; Paniccia, B.; Nyinawabera, A.; Nuovo, G.J. Enhanced expression of PD L1 in cervical intraepithelial neoplasia and cervical cancers. Mod. Pathol. 2015, 28, 1594–1602. [Google Scholar] [CrossRef]
- Meng, Y.; Liang, H.; Hu, J.; Liu, S.; Hao, X.; Wong, M.S.K.; Li, X.; Hu, L. PD-L1 Expression Correlates With Tumor Infiltrating Lymphocytes And Response To Neoadjuvant Chemotherapy In Cervical Cancer. J. Cancer 2018, 9, 2938–2945. [Google Scholar] [CrossRef]
- Feng, Y.C.; Ji, W.L.; Yue, N.; Huang, Y.C.; Ma, X.M. The relationship between the PD-1/PD-L1 pathway and DNA mismatch repair in cervical cancer and its clinical significance. Cancer Manag. Res. 2018, 10, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Enwere, E.K.; Kornaga, E.N.; Dean, M.; Koulis, T.A.; Phan, T.; Kalantarian, M.; Kobel, M.; Ghatage, P.; Magliocco, A.M.; Lees-Miller, S.P.; et al. Expression of PD-L1 and presence of CD8-positive T cells in pre-treatment specimens of locally advanced cervical cancer. Mod. Pathol. 2017, 30, 577–586. [Google Scholar] [CrossRef] [Green Version]
- Reddy, O.L.; Shintaku, P.I.; Moatamed, N.A. Programmed death-ligand 1 (PD-L1) is expressed in a significant number of the uterine cervical carcinomas. Diagn. Pathol. 2017, 12, 45. [Google Scholar] [CrossRef]
- Dijkstra, K.K.; Voabil, P.; Schumacher, T.N.; Voest, E.E. Genomics- and Transcriptomics-Based Patient Selection for Cancer Treatment With Immune Checkpoint Inhibitors: A Review. JAMA Oncol. 2016, 2, 1490–1495. [Google Scholar] [CrossRef]
- Yaguchi, T.; Kawakami, Y. Cancer-induced heterogeneous immunosuppressive tumor microenvironments and their personalized modulation. Int. Immunol. 2016, 28, 393–399. [Google Scholar] [CrossRef] [Green Version]
- Frenel, J.S.; Le Tourneau, C.; O’Neil, B.; Ott, P.A.; Piha-Paul, S.A.; Gomez-Roca, C.; Van Brummelen, E.M.J.; Rugo, H.S.; Thomas, S.; Saraf, S.; et al. Safety and Efficacy of Pembrolizumab in Advanced, Programmed Death Ligand 1-Positive Cervical Cancer: Results From the Phase Ib KEYNOTE-028 Trial. J. Clin. Oncol. 2017, 35, 4035–4041. [Google Scholar] [CrossRef]
- Naumann, R.W.; Hollebecque, A.; Meyer, T.; Devlin, M.J.; Oaknin, A.; Kerger, J.; Lopez-Picazo, J.M.; Machiels, J.P.; Delord, J.P.; Evans, T.R.J.; et al. Safety and Efficacy of Nivolumab Monotherapy in Recurrent or Metastatic Cervical, Vaginal, or Vulvar Carcinoma: Results From the Phase I/II CheckMate 358 Trial. J. Clin. Oncol. 2019, 37, 2825–2834. [Google Scholar] [CrossRef]
- Golden, E.B.; Frances, D.; Pellicciotta, I.; Demaria, S.; Helen Barcellos-Hoff, M.; Formenti, S.C. Radiation fosters dose-dependent and chemotherapy-induced immunogenic cell death. Oncoimmunology 2014, 3, e28518. [Google Scholar] [CrossRef] [Green Version]
- Chouaib, S.; Messai, Y.; Couve, S.; Escudier, B.; Hasmim, M.; Noman, M.Z. Hypoxia promotes tumor growth in linking angiogenesis to immune escape. Front. Immunol. 2012, 3, 21. [Google Scholar] [CrossRef] [Green Version]
- Khan, K.A.; Kerbel, R.S. Improving immunotherapy outcomes with anti-angiogenic treatments and vice versa. Nat. Rev. Clin. Oncol. 2018, 15, 310–324. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Powles, T.; Atkins, M.B.; Escudier, B.; McDermott, D.F.; Suarez, C.; Bracarda, S.; Stadler, W.M.; Donskov, F.; Lee, J.L.; et al. Atezolizumab plus bevacizumab versus sunitinib in patients with previously untreated metastatic renal cell carcinoma (IMmotion151): A multicentre, open-label, phase 3, randomised controlled trial. Lancet 2019, 393, 2404–2415. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodriguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- Efficacy and Safety of BCD-100 (Anti-PD-1) in Combination With Platinum-Based Chemotherapy With and Without Bevacizumab as First-Line Treatment of Subjects With Advanced Cervical Cancer (FERMATA). Available online: https://clinicaltrials.gov/ct2/show/NCT03912415 (accessed on 20 July 2019).
- Efficacy and Safety Study of First-line Treatment With Pembrolizumab (MK-3475) Plus Chemotherapy Versus Placebo Plus Chemotherapy in Women With Persistent, Recurrent, or Metastatic Cervical Cancer (MK-3475-826/KEYNOTE-826). Available online: https://clinicaltrials.gov/ct2/show/NCT03635567 (accessed on 20 July 2019).
- Platinum Chemotherapy Plus Paclitaxel With Bevacizumab and Atezolizumab in Metastatic Carcinoma of the Cervix. Available online: https://clinicaltrials.gov/ct2/show/NCT03556839 (accessed on 20 July 2019).
- Lee, L.; Matulonis, U. Immunotherapy and radiation combinatorial trials in gynecologic cancer: A potential synergy? Gynecol. Oncol. 2019, 154, 236–245. [Google Scholar] [CrossRef]
- Mole, R.H. Whole body irradiation; radiobiology or medicine? Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef]
- Abuodeh, Y.; Venkat, P.; Kim, S. Systematic review of case reports on the abscopal effect. Curr. Probl. Cancer 2016, 40, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Takaya, M.; Niibe, Y.; Tsunoda, S.; Jobo, T.; Imai, M.; Kotani, S.; Unno, N.; Hayakawa, K. Abscopal effect of radiation on toruliform para-aortic lymph node metastases of advanced uterine cervical carcinoma—A case report. Anticancer Res. 2007, 27, 499–503. [Google Scholar]
- Rodriguez-Ruiz, M.E.; Vanpouille-Box, C.; Melero, I.; Formenti, S.C.; Demaria, S. Immunological Mechanisms Responsible for Radiation-Induced Abscopal Effect. Trends Immunol. 2018, 39, 644–655. [Google Scholar] [CrossRef]
- McCall, N.S.; Dicker, A.P.; Lu, B. Beyond Concurrent Chemoradiation: The Emerging Role of PD-1/PD-L1 Inhibitors in Stage III Lung Cancer. Clin. Cancer Res. 2018, 24, 1271–1276. [Google Scholar] [CrossRef] [Green Version]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef]
- TSR-042 as Maintenance Therapy for Patients With High-Risk Locally Advanced Cervical Cancer After Chemo-Radiation (ATOMICC). Available online: https://clinicaltrials.gov/ct2/show/NCT03833479 (accessed on 20 July 2019).
- Pembrolizumab and Chemoradiation Treatment for Advanced Cervical Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02635360 (accessed on 20 July 2019).
- Trial Assessing the Inhibitor of Programmed Cell Death Ligand 1 (PD-L1) Immune Checkpoint Atezolizumab (ATEZOLACC). Available online: https://clinicaltrials.gov/ct2/show/NCT03612791 (accessed on 20 July 2019).


{kind=link}
| / | KEYNOTE-158 [8] | CheckMate 358 [20] |
|---|---|---|
| Treatment | pembrolizumab | nivolumab |
| Phase | II | I/II |
| n | 98 | 19 |
| Stage | ||
| II | 1 (1.0%) | 1 (5.3%) |
| III | 4 (4.1%) | 2 (10.5%) |
| IV | 93 (94.9%) | 16 (84.2%) |
| PD-L1 expression | ||
| Positive | 82 (83.7%) | 10 (62.5%) |
| Negative | 15 (15.3%) | 6 (37.5%) |
| Unknown | 1 (1%) | 3 (15.8%) |
| Previous radiotherapy | 85 (86.7%) | 17 (89.5%) |
| Previous line of systemic therapy | ||
| 0 | 0 (0%) | 0 (0%) |
| 1 | 30 (30.6%) | 8 (42.1%) |
| 2 | 34 (34.7%) | 8 (42.1%) |
| 3 | 16 (16.3%) | 3 (15.8%) |
| Previous antineoplastic agents | ||
| Cisplatin | 79 (80.6%) | 15 (78.9%) |
| Carboplatin | 66 (67.3%) | 11 (57.9%) |
| Paclitaxel | 85 (86.7%) | 12 (63.2%) |
| Bevacizumab | 41 (41.8%) | 6 (31.6%) |
| Topotecan | 17 (17.3%) | 5 (26.3%) |
| / | KEYNOTE-158 [8] | CheckMate 358 [20] |
|---|---|---|
| Treatment | pembrolizumab | nivolumab |
| n | 98 | 19 |
| ORR (95% CI) | 12.2% (6.5 to 20.4) | 26.3% (9.1 to 51.2) |
| DCR (95% CI) | 30.6% (21.7 to 40.7) | 68.4% (43.4 to 87.4) |
| Best overall response | ||
| CR | 3 (3.1%) | 3 (15.8%) |
| PR | 9 (9.2%) | 2 (10.5%) |
| SD | 18 (18.4%) | 8 (42.1%) |
| PD | 55 (56.1%) | 6 (31.6%) |
| Not able to be evaluated* | 5 (5.1%) | 0 (0%) |
| Not able to be assessed# | 8 (8.2%) | 0 (0%) |
| Title | Study Population | n | Phase | Treatment | Primary Outcomes | Secondary Outcomes | Clinical Trial Code |
|---|---|---|---|---|---|---|---|
| Efficacy and Safety of BCD-100 (Anti-PD-1) in Combination with Platinum-Based Chemotherapy with and Without Bevacizumab as First-Line Treatment of Subjects with Advanced Cervical Cancer (FERMATA) [26] | Advanced cervical cancer | 316 | III | Paclitaxel + cisplatin (or carboplatin) Bevacizumab BCD-100 (anti-PD-1) | OS | PFS, ORR, DOR | NCT03912415 |
| Efficacy and Safety Study of First-Line Treatment with Pembrolizumab (MK-3475) Plus Chemotherapy Versus Placebo Plus Chemotherapy in Women with Persistent, Recurrent, or Metastatic Cervical Cancer (MK-3475-826/KEYNOTE-826) [27] | Recurrent or metastatic cervical cancer | 600 | III | Paclitaxel + cisplatin (or carboplatin) Bevacizumab Pembrolizumab | PFS, OS | ORR, DCR, DOR | NCT03635567 |
| Platinum Chemotherapy Plus Paclitaxel with Bevacizumab and Atezolizumab in Metastatic Carcinoma of the Cervix [28] | Recurrent or metastatic cervical cancer | 404 | III | Paclitaxel + cisplatin Bevacizumab Atezolizumab | OS | PFS, ORR, DOR, AE | NCT03556839 |
| Title | Study Population | n | Phase | Treatment | Primary Outcomes | Secondary Outcomes | Clinical Trial Code |
|---|---|---|---|---|---|---|---|
| TSR-042 as Maintenance Therapy for Patients with High-risk Locally Advanced Cervical Cancer After Chemo-radiation (ATOMICC) [36] | Stage IB/IIA/IIB/III/IVA cervical cancer with pelvic or PALN | 132 | II | CRT Maintenance TSR-042 (anti-PD-1 antibody) | PFS | AE, OS | NCT03833479 |
| Pembrolizumab and Chemoradiation Treatment for Advanced Cervical Cancer [37] | Locally advanced cervical cancer | 88 | II | Pembrolizumab with CRT | Change in immunologic markers following combination of study drug with chemoradiation, DLT | Metabolic Response Rate on PET/CT imaging, incidence of distant metastases, PFS, OS | NCT02635360 |
| Trial Assessing the Inhibitor of Programmed Cell Death Ligand 1 (PD-L1) Immune Checkpoint Atezolizumab (ATEZOLACC) [38] | Locally advanced cervical cancer | 190 | II | Atezolizumab with CRT and adjuvant atezolizumab | PFS | NCT03612791 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kagabu, M.; Nagasawa, T.; Sato, C.; Fukagawa, Y.; Kawamura, H.; Tomabechi, H.; Takemoto, S.; Shoji, T.; Baba, T. Immunotherapy for Uterine Cervical Cancer Using Checkpoint Inhibitors: Future Directions. Int. J. Mol. Sci. 2020, 21, 2335. https://doi.org/10.3390/ijms21072335
Kagabu M, Nagasawa T, Sato C, Fukagawa Y, Kawamura H, Tomabechi H, Takemoto S, Shoji T, Baba T. Immunotherapy for Uterine Cervical Cancer Using Checkpoint Inhibitors: Future Directions. International Journal of Molecular Sciences. 2020; 21(7):2335. https://doi.org/10.3390/ijms21072335
Chicago/Turabian StyleKagabu, Masahiro, Takayuki Nagasawa, Chie Sato, Yasuko Fukagawa, Hanae Kawamura, Hidetoshi Tomabechi, Shuji Takemoto, Tadahiro Shoji, and Tsukasa Baba. 2020. "Immunotherapy for Uterine Cervical Cancer Using Checkpoint Inhibitors: Future Directions" International Journal of Molecular Sciences 21, no. 7: 2335. https://doi.org/10.3390/ijms21072335