A Novel Way of Preventing Postoperative Pancreatic Fistula by Directly Injecting Profibrogenic Materials into the Pancreatic Parenchyma

 , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
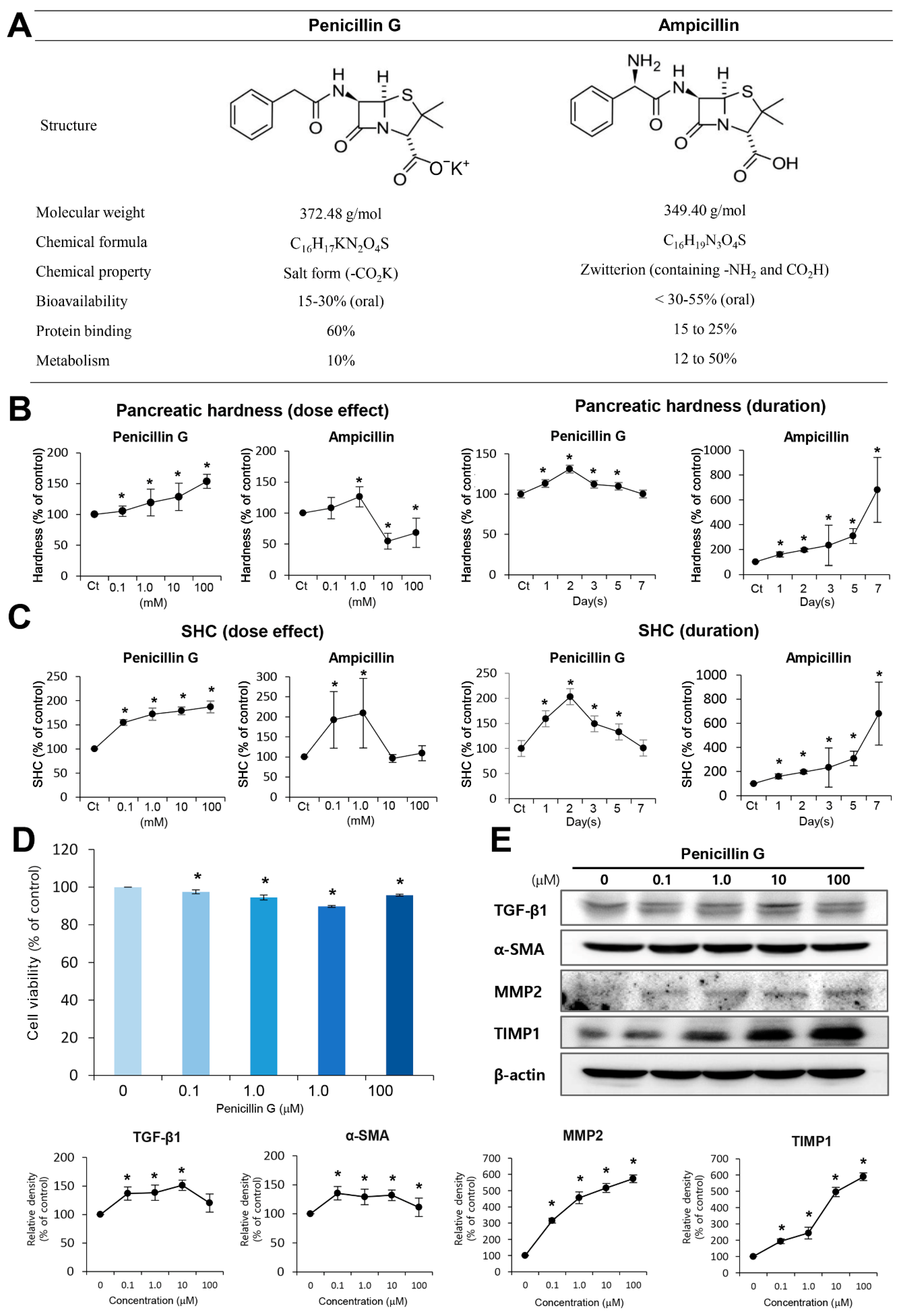
2.1. Selection of Pancreas-Hardening Compounds from Antibiotics Library
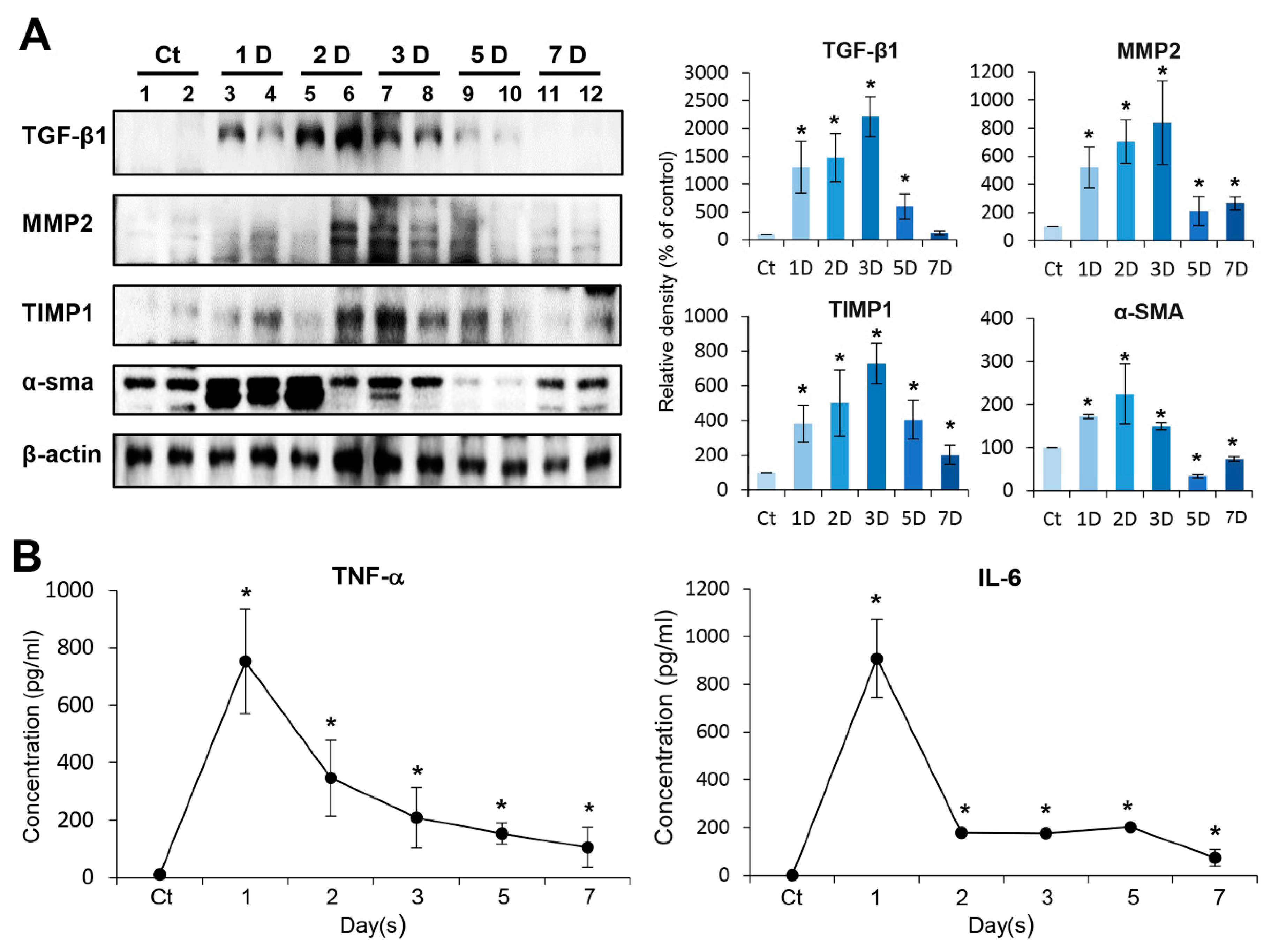
2.2. In Vitro Determination of Profibrotic Property of Penicillin G
2.3. In Vivo Determination of Profibrotic Property of Penicillin G
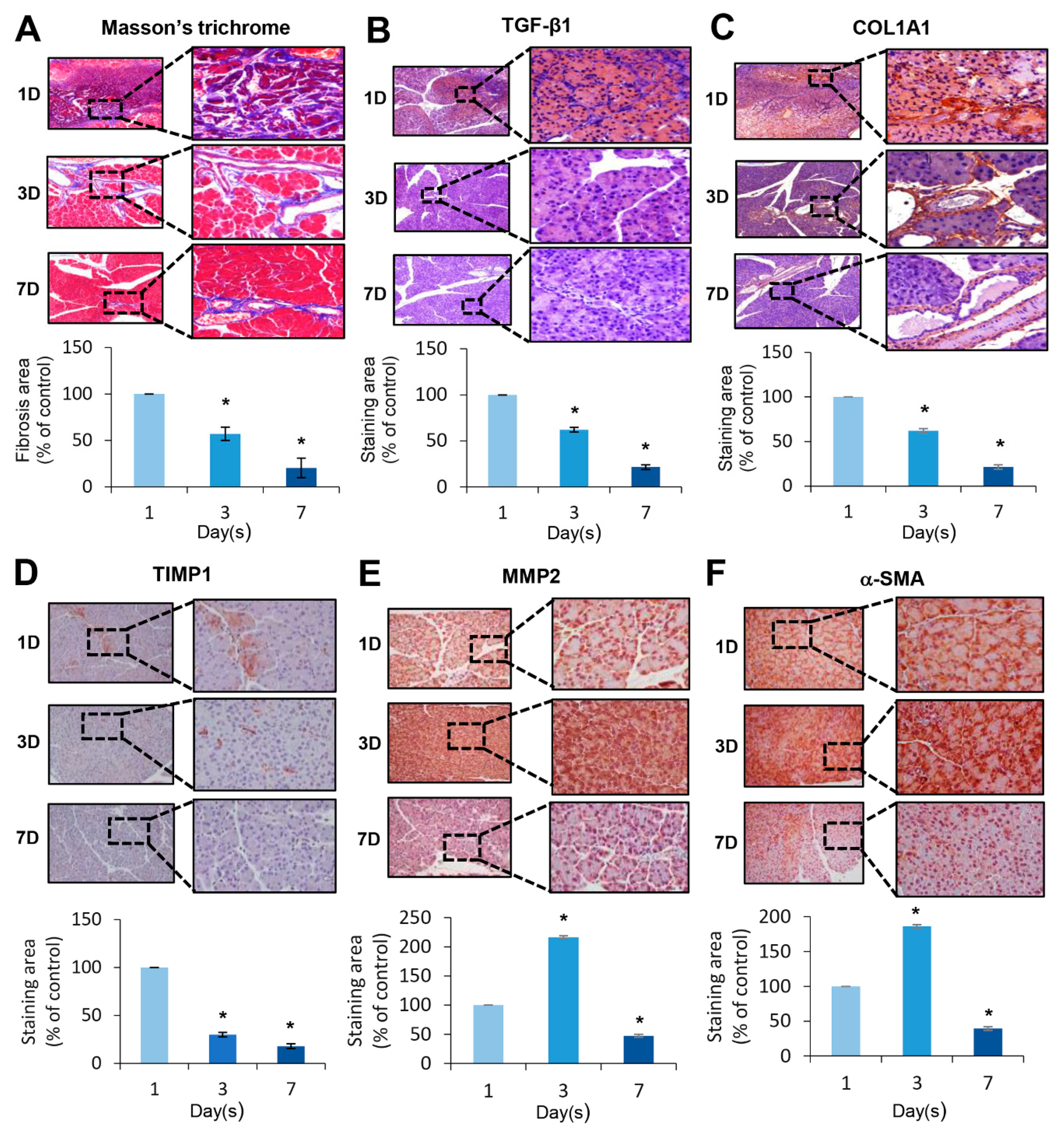
2.4. Histological Changes Induced by the Injection of Penicillin G
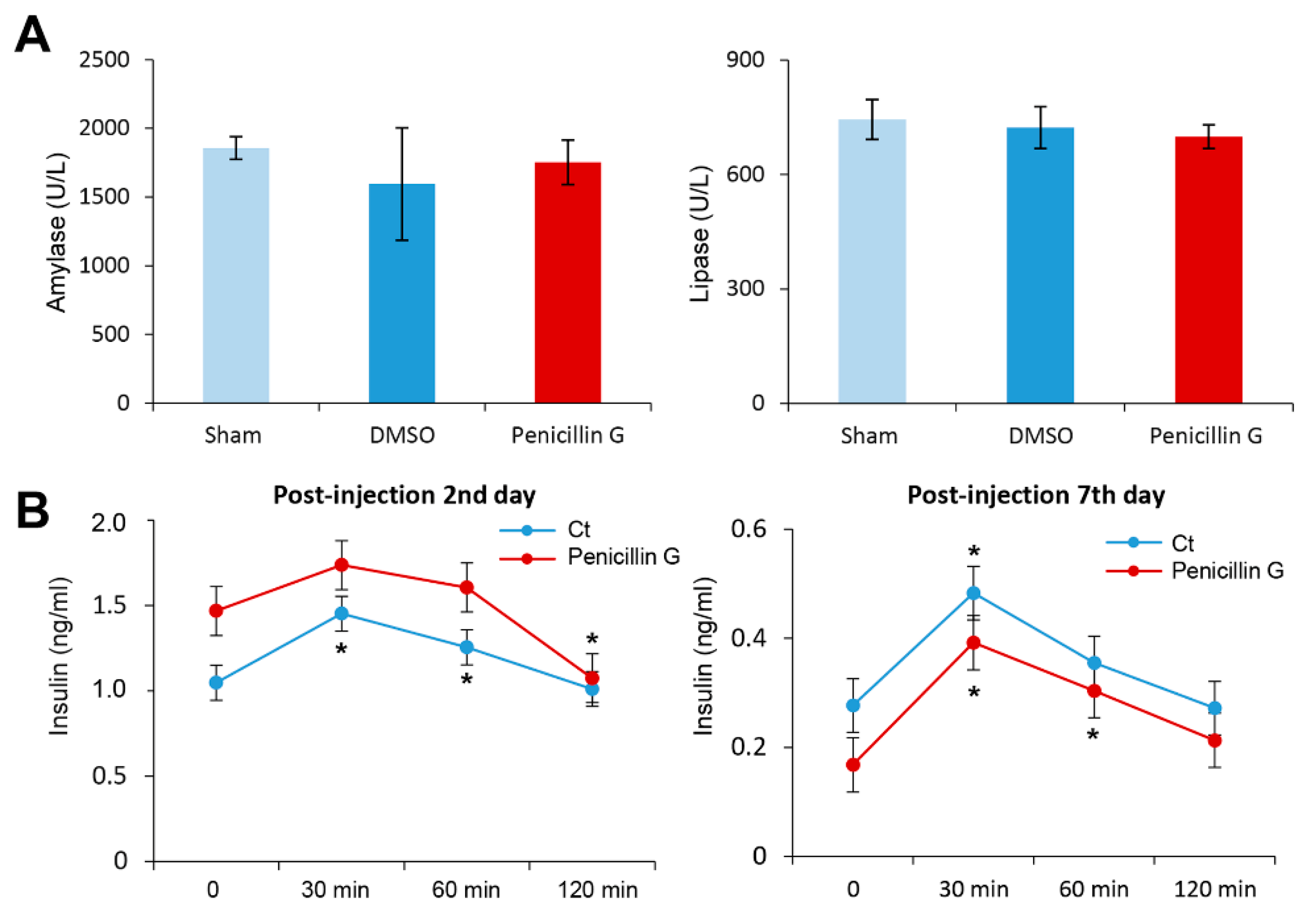
2.5. Effects of Penicillin G on the Pancreatic Function
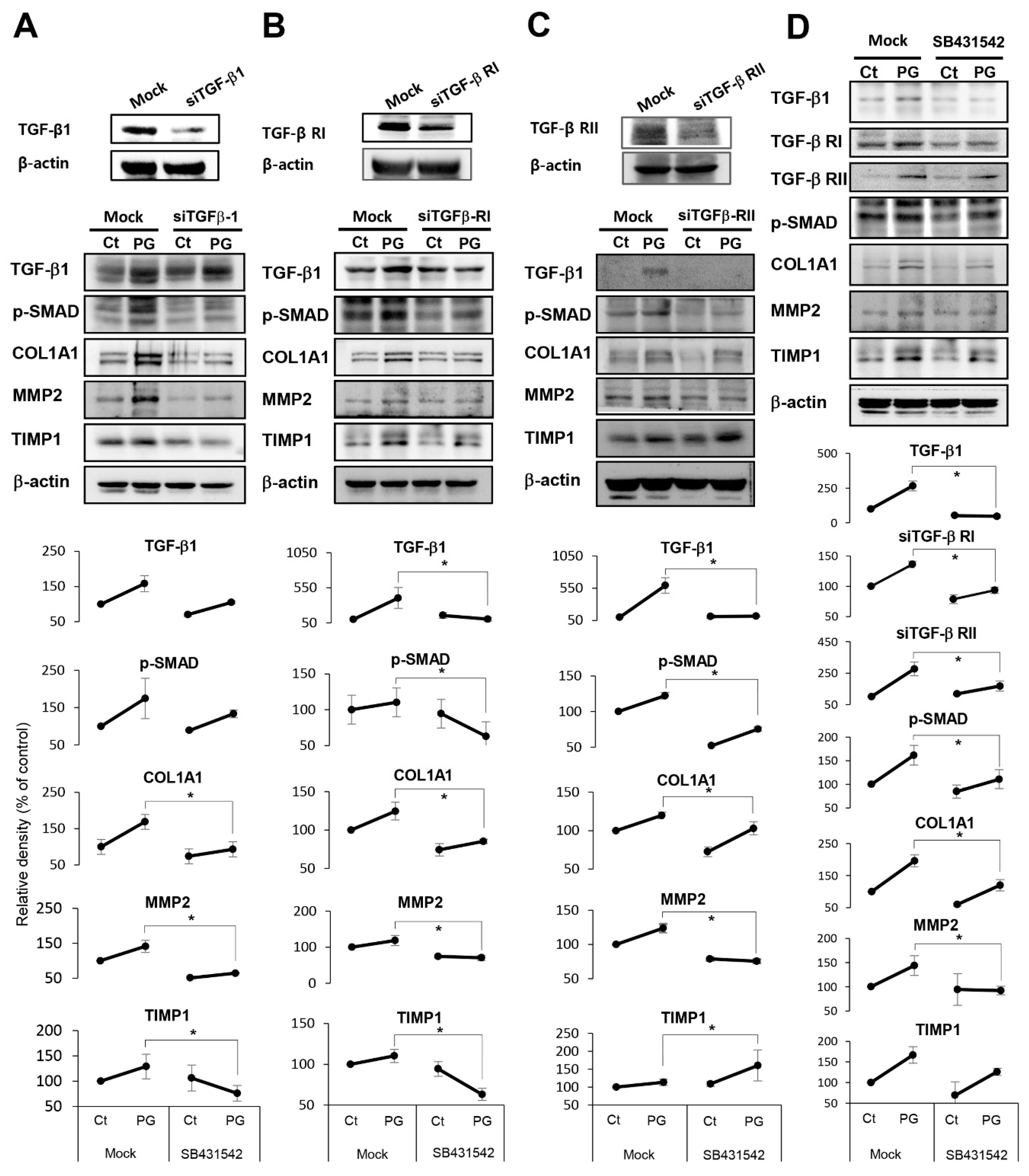
2.6. Investigation of Mechanism Leading to Pancreatic Fibrosis by Penicillin G
3. Discussion
4. Materials and Methods
4.1. Animals Study
4.2. Statistical Analysis
4.3. Additional Materials and Methods
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| α-SMA | alpha smooth muscle actin |
| COL1A1 | collagen type 1 alpha1 |
| DMSO | dimethyl sulfoxide |
| HPSCs | human pancreatic stellate cells |
| IL-6 | interleukin-6 |
| MMP2 | metalloproteinases-2 |
| POD | postoperative day |
| POPF | postoperative pancreatic fistula |
| ELISA | enzyme-linked immunosorbent assay |
| p-SMAD | pospho-SMAD |
| SHC | suture holding capacity |
| TGFβ-1 | transforming growth factor-β1 |
| TIMP1 | tissue inhibitor of metalloproteinases-1 |
| TNF-α | tumor necrosis factor- α |
| Ct | control |
References
- Bassi, C.; Dervenis, C.; Butturini, G.; Fingerhut, A.; Yeo, C.; Izbicki, J.; Neoptolemos, J.; Sarr, M.; Traverso, W.; Buchler, M.; et al. Postoperative pancreatic fistula: An international study group (ISGPF) definition. Surgery 2005, 138, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Schafer, M.; Mullhaupt, B.; Clavien, P.A. Evidence-based pancreatic head resection for pancreatic cancer and chronic pancreatitis. Ann. Surg. 2002, 236, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Buchler, M.W.; Friess, H.; Wagner, M.; Kulli, C.; Wagener, V.; Z’Graggen, K. Pancreatic fistula after pancreatic head resection. Br. J. Surg. 2000, 87, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Cullen, J.J.; Sarr, M.G.; Ilstrup, D.M. Pancreatic anastomotic leak after pancreaticoduodenectomy: Incidence, significance, and management. Am. J. Surg. 1994, 168, 295–298. [Google Scholar] [CrossRef]
- Miedema, B.W.; Sarr, M.G.; van Heerden, J.A.; Nagorney, D.M.; McIlrath, D.C.; Ilstrup, D. Complications following pancreaticoduodenectomy. Current management. Arch. Surg. 1992, 127, 945–949. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Russell, R.C.; Bramhall, S.; Theis, B. Low mortality following resection for pancreatic and periampullary tumours in 1026 patients: UK survey of specialist pancreatic units. UK Pancreatic Cancer Group. Br. J. Surg. 1997, 84, 1370–1376. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, L.; MacNeil, P.; Turcotte, L. Economic evaluation of the use of octreotide for prevention of complications following pancreatic resection. J. Gastrointest. Surg. 1999, 3, 225–232. [Google Scholar] [CrossRef]
- Trede, M.; Schwall, G. The complications of pancreatectomy. Ann. Surg. 1988, 207, 39–47. [Google Scholar] [CrossRef]
- Vallance, A.E.; Young, A.L.; Macutkiewicz, C.; Roberts, K.J.; Smith, A.M. Calculating the risk of a pancreatic fistula after a pancreaticoduodenectomy: A systematic review. Hpb 2015, 17, 1040–1048. [Google Scholar] [CrossRef] [Green Version]
- Yeo, C.J.; Cameron, J.L.; Sohn, T.A.; Lillemoe, K.D.; Pitt, H.A.; Talamini, M.A.; Hruban, R.H.; Ord, S.E.; Sauter, P.K.; Coleman, J.; et al. Six hundred fifty consecutive pancreaticoduodenectomies in the 1990s: Pathology, complications, and outcomes. Ann. Surg. 1997, 226. [Google Scholar] [CrossRef]
- Shrikhande, S.V.; D’Souza, M.A. Pancreatic fistula after pancreatectomy: Evolving definitions, preventive strategies and modern management. World J. Gastroentero 2008, 14, 5789–5796. [Google Scholar] [CrossRef] [PubMed]
- Denbo, J.W.; Orr, W.S.; Zarzaur, B.L.; Behrman, S.W. Toward defining grade C pancreatic fistula following pancreaticoduodenectomy: Incidence, risk factors, management and outcome. Hpb 2012, 14, 589–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.; Briarava, M.; Lai, M.L.; Wang, X.M.; Tu, B.; Cheng, N.S.; Gong, J.P.; Yuan, Y.H.; Pilati, P.; Mocellin, S. Pancreaticojejunostomy versus pancreaticogastrostomy reconstruction for the prevention of postoperative pancreatic fistula following pancreaticoduodenectomy. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Kawai, M.; Hirono, S.; Okada, K.; Sho, M.; Nakajima, Y.; Eguchi, H.; Nagano, H.; Ikoma, H.; Morimura, R.; Takeda, Y.; et al. Randomized Controlled Trial of Pancreaticojejunostomy Versus Stapler Closure of the Pancreatic Stump During Distal Pancreatectomy to Reduce Pancreatic Fistula. Ann. Surg. 2016, 264, 180–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangiafico, S.; Caruso, A.; Manta, R.; Grande, G.; Bertani, H.; Mirante, V.; Pigo, F.; Magnano, L.; Manno, M.; Conigliaro, R. Over-the-scope clip closure for treatment of post-pancreaticogastrostomy pancreatic fistula: A case series. Dig. Endosc. 2017, 29, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Qin, H.; Luo, L.; Zhu, Z.X.; Huang, J.W. Pancreaticogastrostomy has advantages over pancreaticojejunostomy on pancreatic fistula after pancreaticoduodenectomy. A meta-analysis of randomized controlled trials. Int. J. Surg. 2016, 36, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; He, S.; Cheng, Y.; Cheng, N.; Gong, J.; Zeng, Z. Fibrin sealants for the prevention of postoperative pancreatic fistula following pancreatic surgery. Cochrane Database Syst. Rev. 2018, 6, CD009621. [Google Scholar] [CrossRef]
- Sandini, M.; Malleo, G.; Gianotti, L. Scores for Prediction of Fistula after Pancreatoduodenectomy: A Systematic Review. Dig. Surg. 2016, 33, 392–400. [Google Scholar] [CrossRef]
- Gans, S.L.; van Westreenen, H.L.; Kiewiet, J.J.S.; Rauws, E.A.J.; Gouma, D.J.; Boermeester, M.A. Systematic review and meta-analysis of somatostatin analogues for the treatment of pancreatic fistula. Brit. J. Surg. 2012, 99, 754–760. [Google Scholar] [CrossRef]
- Garg, P.K.; Sharma, J.; Jakhetiya, A.; Chishi, N. The Role of Prophylactic Octreotide Following Pancreaticoduodenectomy to Prevent Postoperative Pancreatic Fistula: A Meta-Analysis of the Randomized Controlled Trials. Surg. J. 2018, 4, e182–e187. [Google Scholar] [CrossRef] [Green Version]
- Kurumboor, P.; Palaniswami, K.N.; Pramil, K.; George, D.; Ponnambathayil, S.; Varma, D.; Aikot, S. Octreotide Does Not Prevent Pancreatic Fistula Following Pancreatoduodenectomy in Patients with Soft Pancreas and Non-dilated Duct: A Prospective Randomized Controlled Trial. J. Gastrointest Surg. 2015, 19, 2038–2044. [Google Scholar] [CrossRef] [PubMed]
- Aston, S.J.; Longmire, W.P., Jr. Management of the pancreas after pancreaticoduodenectomy. Ann. Surg. 1974, 179, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Crippa, S.; Cirocchi, R.; Randolph, J.; Partelli, S.; Belfiori, G.; Piccioli, A.; Parisi, A.; Falconi, M. Pancreaticojejunostomy is comparable to pancreaticogastrostomy after pancreaticoduodenectomy: An updated meta-analysis of randomized controlled trials. Langenbeck Arch. Surg. 2016, 401, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.Y.; Xu, J.; Wang, Z.; Petrov, M.S. Stents for the prevention of pancreatic fistula following pancreaticoduodenectomy. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [Green Version]
- Gurusamy, K.S.; Koti, R.; Fusai, G.; Davidson, B.R. Somatostatin analogues for pancreatic surgery. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Huttner, F.J.; Mihaljevic, A.L.; Hackert, T.; Ulrich, A.; Buchler, M.W.; Diener, M.K. Effectiveness of Tachosil((R)) in the prevention of postoperative pancreatic fistula after distal pancreatectomy: A systematic review and meta-analysis. Langenbecks Arch. Surg. 2016, 401, 151–159. [Google Scholar] [CrossRef]
- Klaiber, U.; Probst, P.; Knebel, P.; Contin, P.; Diener, M.K.; Buchler, M.W.; Hackert, T. Meta-analysis of complication rates for single-loop versus dual-loop (Roux-en-Y) with isolated pancreaticojejunostomy reconstruction after pancreaticoduodenectomy. Br. J. Surg. 2015, 102, 331–340. [Google Scholar] [CrossRef]
- Soreide, K.; Labori, K.J. Risk factors and preventive strategies for post-operative pancreatic fistula after pancreatic surgery: A comprehensive review. Scand. J. Gastroenterol. 2016, 51, 1147–1154. [Google Scholar] [CrossRef]
- Machado, N.O. Pancreatic fistula after pancreatectomy: Definitions, risk factors, preventive measures, and management-review. Int. J. Surg. Oncol. 2012, 2012, 602478. [Google Scholar]
- Ramacciato, G.; Mercantini, P.; Petrucciani, N.; Nigri, G.R.; Kazemi, A.; Muroni, M.; Del Gaudio, M.; Balesh, A.; Cescon, M.; Cucchetti, A.; et al. Risk factors of pancreatic fistula after pancreaticoduodenectomy: A collective review. Am. Surg. 2011, 77, 257–269. [Google Scholar]
- Adachi, E.; Harimoto, N.; Yamashita, Y.; Sakaguchi, Y.; Toh, Y.; Okamura, T.; Nishiyama, K.; Saeki, H.; Uchiyama, H.; Morita, M.; et al. Pancreatic leakage test in pancreaticoduodenectomy: Relation to degree of pancreatic fibrosis, pancreatic amylase level and pancreatic fistula. Fukuoka Igaku Zasshi 2013, 104, 490–498. [Google Scholar] [PubMed]
- Peng, Y.P.; Zhu, X.L.; Yin, L.D.; Zhu, Y.; Wei, J.S.; Wu, J.L.; Miao, Y. Risk factors of postoperative pancreatic fistula in patients after distal pancreatectomy: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 185. [Google Scholar] [CrossRef] [Green Version]
- Eshmuminov, D.; Schneider, M.A.; Tschuor, C.; Raptis, D.A.; Kambakamba, P.; Muller, X.; Lesurtel, M.; Clavien, P.A. Systematic review and meta-analysis of postoperative pancreatic fistula rates using the updated 2016 International Study Group Pancreatic Fistula definition in patients undergoing pancreatic resection with soft and hard pancreatic texture. Hpb 2018, 20, 992–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belyaev, O.; Rosenkranz, S.; Munding, J.; Herzog, T.; Chromik, A.M.; Tannapfel, A.; Uhl, W. Quantitative assessment and determinants of suture-holding capacity of human pancreas. J. Surg. Res. 2013, 184, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Balani, S.K.; Miwa, G.T.; Gan, L.S.; Wu, J.T.; Lee, F.W. Strategy of utilizing in vitro and in vivo ADME tools for lead optimization and drug candidate selection. Curr. Top. Med. Chem. 2005, 5, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Zanger, U.M.; Schwab, M. Cytochrome P450 enzymes in drug metabolism: Regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol. Ther. 2013, 138, 103–141. [Google Scholar] [CrossRef]
- Casadei, R.; Ricci, C.; Taffurelli, G.; D’Ambra, M.; Pacilio, C.A.; Ingaldi, C.; Minni, F. Are there preoperative factors related to a “soft pancreas” and are they predictive of pancreatic fistulas after pancreatic resection? Surg. Today 2015, 45, 708–714. [Google Scholar] [CrossRef]
- DeOliveira, M.L.; Winter, J.M.; Schafer, M.; Cunningham, S.C.; Cameron, J.L.; Yeo, C.J.; Clavien, P.A. Assessment of complications after pancreatic surgery: A novel grading system applied to 633 patients undergoing pancreaticoduodenectomy. Ann. Surg. 2006, 244. [Google Scholar] [CrossRef]
- Lin, J.W.; Cameron, J.L.; Yeo, C.J.; Riall, T.S.; Lillemoe, K.D. Risk factors and outcomes in postpancreaticoduodenectomy pancreaticocutaneous fistula. J. Gastrointest Surg. 2004, 8, 951–959. [Google Scholar] [CrossRef]
- Muscari, F.; Suc, B.; Kirzin, S.; Hay, J.M.; Fourtanier, G.; Fingerhut, A.; Sastre, B.; Chipponi, J.; Fagniez, P.L.; Radovanovic, A.; et al. Risk factors for mortality and intra-abdominal complications after pancreatoduodenectomy: Multivariate analysis in 300 patients. Surgery 2006, 139, 591–598. [Google Scholar] [CrossRef]
- Pratt, W.B.; Callery, M.P.; Vollmer, C.M. Risk prediction for development of pancreatic fistula using the ISGPF classification scheme. World J. Surg. 2008, 32, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Jang, J.Y.; Lim, C.S.; Kang, M.J.; Kim, S.H.; Kim, M.A.; Kim, S.W. Measurement of Pancreatic Fat by Magnetic Resonance Imaging Predicting the Occurrence of Pancreatic Fistula After Pancreatoduodenectomy. Ann. Surg. 2010, 251, 932–936. [Google Scholar] [CrossRef]
- Koga, R.; Yamamoto, J.; Saiura, A.; Natori, T.; Katori, M.; Kokudo, N.; Makuuchi, M.; Yamaguchi, T. Clamp-crushing Pancreas Transection in Pancreatoduodenectomy. Hepato-Gastroenterol 2009, 56, 89–93. [Google Scholar]
- Gonzalez, A.C.; Costa, T.F.; Andrade, Z.A.; Medrado, A.R. Wound healing—A literature review. Bras. Derm. 2016, 91, 614–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velnar, T.; Bailey, T.; Smrkolj, V. The wound healing process: An overview of the cellular and molecular mechanisms. J. Int. Med. Res. 2009, 37, 1528–1542. [Google Scholar] [CrossRef]
- Chang, Y.R.; Kang, M.J.; Kim, H.; Jang, J.Y.; Kim, S.W. The natural course of pancreatic fistula and fluid collection after distal pancreatectomy: Is drain insertion needed? Ann. Surg. Treat. Res. 2016, 91, 247–253. [Google Scholar] [CrossRef] [Green Version]
- Hackert, T.; Werner, J.; Buchler, M.W. Postoperative pancreatic fistula. Surg-J. R. Coll. Surg. E. 2011, 9, 211–217. [Google Scholar] [CrossRef]
- Nahm, C.B.; Connor, S.J.; Samra, J.S.; Mittal, A. Postoperative pancreatic fistula: A review of traditional and emerging concepts. Clin. Exp. Gastroenterol. 2018, 11, 105–118. [Google Scholar] [CrossRef] [Green Version]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.C.; Hong, T.H.; Kim, O.-H.; Cho, S.J.; Kim, K.-H.; Song, J.S.; Hwang, K.-S.; Jung, J.-K.; Hong, H.-E.; Seo, H.; et al. A Novel Way of Preventing Postoperative Pancreatic Fistula by Directly Injecting Profibrogenic Materials into the Pancreatic Parenchyma. Int. J. Mol. Sci. 2020, 21, 1759. https://doi.org/10.3390/ijms21051759
Lee SC, Hong TH, Kim O-H, Cho SJ, Kim K-H, Song JS, Hwang K-S, Jung J-K, Hong H-E, Seo H, et al. A Novel Way of Preventing Postoperative Pancreatic Fistula by Directly Injecting Profibrogenic Materials into the Pancreatic Parenchyma. International Journal of Molecular Sciences. 2020; 21(5):1759. https://doi.org/10.3390/ijms21051759
Chicago/Turabian StyleLee, Sang Chul, Tae Ho Hong, Ok-Hee Kim, Suk Joon Cho, Kee-Hwan Kim, Jin Sook Song, Kyu-Seok Hwang, Jae-Kyung Jung, Ha-Eun Hong, Haeyeon Seo, and et al. 2020. "A Novel Way of Preventing Postoperative Pancreatic Fistula by Directly Injecting Profibrogenic Materials into the Pancreatic Parenchyma" International Journal of Molecular Sciences 21, no. 5: 1759. https://doi.org/10.3390/ijms21051759