Alterations in the Nervous System and Gut Microbiota after β-Hemolytic Streptococcus Group A Infection—Characteristics and Diagnostic Criteria of PANDAS Recognition

 ,
,  , ,
, ,
Abstract
:1. From Acute Pharyngitis to Rheumatic Fever
2. Rheumatic Fever and OCD
3. PANDAS and OCD—Where Is the Line?
PANDAS Symptoms
4. PANDAS Diagnostic Guidelines
- Presence of OCD and/or tics, mainly multiple ones, complex or not observable in other disorders
- Specific period of childhood and age (symptoms of PANDAS are more common between the age of 3 years old and period of puberty)
- Acute onset and episodic changes in behavior
- Association with infection of Streptococci group A
4.1. The Presence of OCD and/or Tics
4.2. Specific Period of Childhood and Age
4.3. Acute Onset and Episodic Changes in Behavior
4.4. Association with Infection of Streptococci Group A
- Titers of either ASO or anti-DNase B can remain at a high level even for many months after GAS infection, which might present as a false positive result.
- Approximately 40% of children with GAS infection do not present the increased levels of ASO or anti-DNase B which is a false negative result.
- Time constitutes an essential critical factor in the determination of the increased levels (approximately 2–4 times higher) of ASO, and anti-DNase B after one-four and six-eight weeks correspondingly.
- When a child with specific symptoms presents negative results from a throat swab, the levels of basic anti-streptococcal antibodies should be provided.
4.5. Coexisting Neurological Impairments
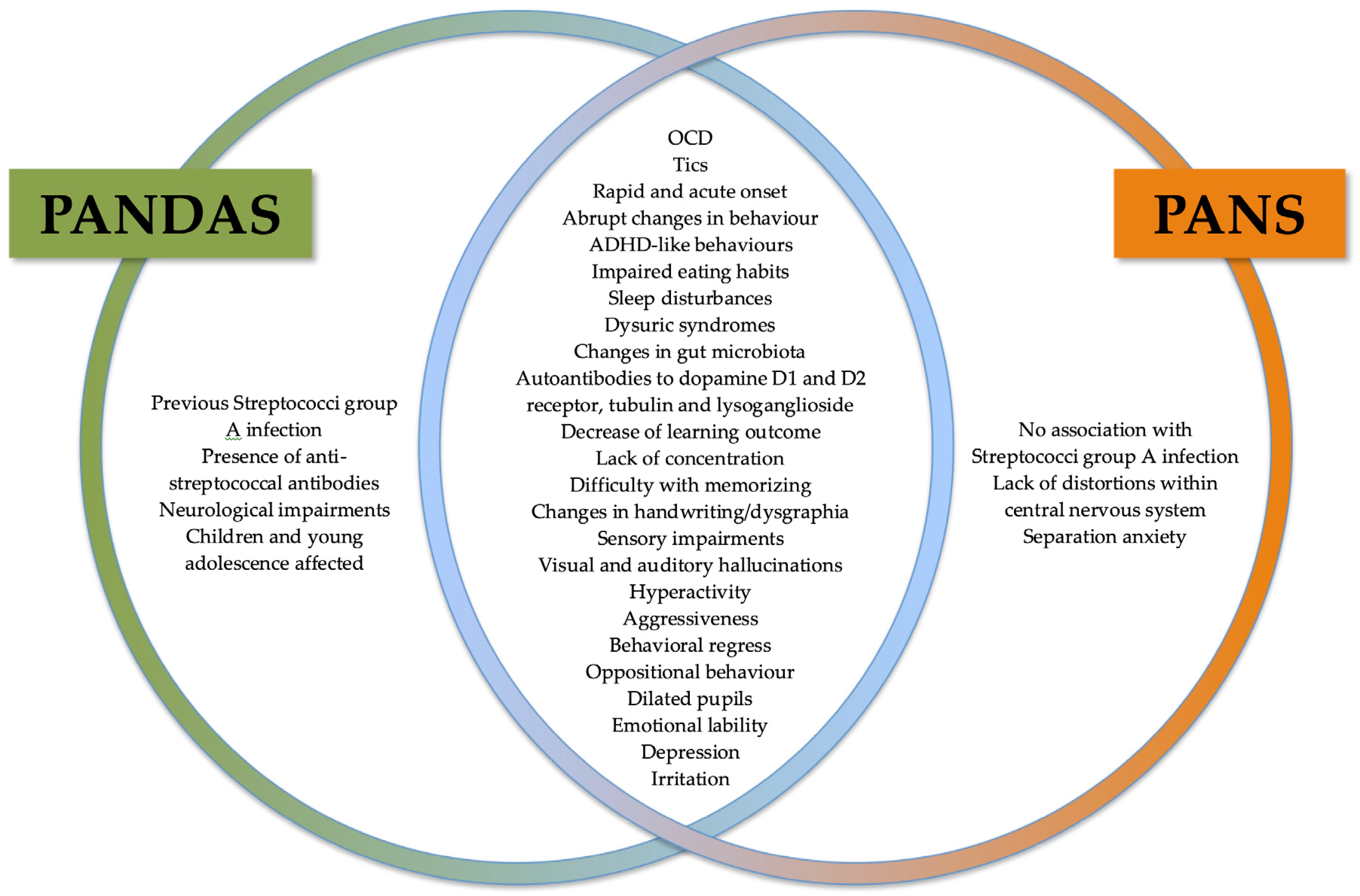
5. PANDAS vs. PANS
- Rapid onset or recurrence of OCD or abnormalities associated with food intake.
- Rapid onset of coexisting neuropsychiatric disorders (at least two of them):
- Increased anxiety levels and/or fear associated with the separation from parents
- Increased motility or motor dysfunctions (including tics and dysgraphia)
- Behavioral regress
- Rapid decline of grades among children in school
- Emotional lability (irritability, aggression and/or oppositional behaviours)
- Dysuric symptoms
- Somatic signs (including insomnia)
- Present symptoms were not explained and associated with the known neurological or medical conditions [98].
The Pathophysiology of GAS Infection and PANDAS
6. PANDAS and Alterations in the Nervous System
6.1. Striatum and Striatal Interneurons
6.2. Microglia
6.3. Basal Ganglia and Antibodies
6.4. Other Structures in CNS
7. The Characterization of Gut Microbiota
7.1. The Impact of Gut Microbiota on the CNS
7.2. Alterations in Gut Microbiota in PANDAS
8. Genetic Approach to OCD, Including PANDAS
9. Treatment of PANDAS
9.1. Antibiotic Therapy
9.2. Psychoactive Drugs
9.3. Nonsteroidal Anti-Inflammatory Drugs
9.4. Tonsillectomy
9.5. Other Treatment Strategies
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| PANDAS | Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections |
| PANS | Pediatric Acute-Onset Neuropsychiatric Syndrome |
| MBL | Mannose-binding lectin |
| TNF-α | Tumor necrosis factor alpha |
| OCD | Obsessive-compulsive disorders |
| ADHD | Attention-Deficit/Hyperactivity Disorder |
| GAS | Group A Streptococci |
| CaM kinase II | Calmodulin-dependent protein kinase II |
| IgM | Immunoglobulin M |
| TRAPS | Tumor Necrosis Factor Receptor Associated Periodic Syndrome |
| ASO | Antistreptolysin-O |
| SLITRK1 | Slit and Trk-like family member 1 |
| CELSR3 | Cadherin EGF LAG Seven-Pass G-Type Receptor 3 |
| FLT3 | FMS-like receptor tyrosine kinase-3 |
| COL27A1 | Collagen type XXVII alpha 1 chain |
| SLITRK5 | SLIT and NTRK-like protein 5 |
| HDC | Histidine decarboxylase |
| NRXN1 | Neurexin 1 |
| CNTN6 | Contactin 6 |
| DRD3 | Dopamine Receptor D3 |
| GDNF | Glial cell-derived neurotrophic factor |
| KCNJ5 | Potassium Voltage-Gated Channel Subfamily J Member 5 |
| AADAC | Arylacetamide Deacetylase |
| HCN4 | Potassium/sodium hyperpolarization-activated cyclic nucleotide-gated channel 4 |
| SSRI | Selective Serotonin Reuptake Inhibitor |
| MRI | Magnetic Resonance Imaging |
| PET | Positron Emission Tomography |
| IVIG | Intravenous immunoglobulin therapy |
| NSAID | Nonsteroidal anti-inflammatory drug |
| LPS | Lipopolysaccharide |
| NOX2 | NADPH oxidase 2 |
| ND | No data |
References
- Anjos, L.M.M.; Marcondes, M.B.; Lima, M.F.; Mondelli, A.L.; Okoshi, M.P. Streptococcal acute pharyngitis. Rev. Soc. Bras. Med. Trop. 2014, 47, 409–413. [Google Scholar] [CrossRef]
- Ivaska, L.; Niemela, J.; Lempainen, J.; Osterback, R.; Waris, M.; Vuorinen, T.; Hytonen, J.; Rantakokko-Jalava, K.; Peltola, V. Aetiology of febrile pharyngitis in children: Potential of myxovirus resistance protein A (MxA) as a biomarker of viral infection. J. Infect. 2017, 74, 385–392. [Google Scholar] [CrossRef]
- Bisno, A.L. Acute Pharyngitis. N. Engl. J. Med. 2001, 344, 205–211. [Google Scholar] [CrossRef]
- Soderholm, A.T.; Barnett, T.C.; Sweet, M.J.; Walker, M.J. Group a streptococcal pharyngitis: Immune responses involved in bacterial clearance and GAS-associated immunopathologies. J. Leukoc. Biol. 2017, 103, 193–213. [Google Scholar] [CrossRef]
- Shaikh, N.; Swaminathan, N.; Hooper, E.G. Accuracy and precision of the signs and symptoms of streptococcal pharyngitis in children: A systematic review. J. Pediatr. 2012, 160, 487–493. [Google Scholar] [CrossRef]
- Shulman, S.T.; Tanz, R.R. Group a streptococcal pharyngitis and immune-mediated complications: From diagnosis to management. Expert Rev. Anti Infect. Ther. 2010, 8, 137–150. [Google Scholar] [CrossRef]
- Walker, M.J.; Barnett, T.C.; McArthur, J.D.; Cole, J.N.; Gillen, C.M.; Henningham, A.; Sriprakash, K.S.; Sanderson-Smith, M.L.; Nizet, V. Disease manifestations and pathogenic mechanisms of group A Streptococcus. Clin. Microbiol. Rev. 2014, 27, 264–301. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, D.E.; Zhang, Y.; Bode, L.; Munte, T.F.; Hauser, U.; Schmorl, P.; Richter-Witte, C.; Godecke-Koch, T.; Feutl, S.; Schramm, J.; et al. Brain potential amplitude varies as a function of Borna disease virus-specific immune complexes in obsessive-compulsive disorder. Mol. Psychiatry 2005, 10, 519–520. [Google Scholar] [CrossRef]
- Muller, N.; Riedel, M.; Blendinger, C.; Oberle, K.; Jacobs, E.; Abele-Horn, M. Mycoplasma pneumoniae infection and Tourette’s syndrome. Psychiatry Res. 2004, 129, 119–125. [Google Scholar] [CrossRef]
- Matsuo, M.; Tsuchiya, K.; Hamasaki, Y.; Singer, H.S. Restless legs syndrome: Association with streptococcal or Mycoplasma infection. Pediatr. Neurol. 2004, 31, 119–121. [Google Scholar] [CrossRef]
- Leon, J.; Hommer, R.; Grant, P.; Farmer, C.; D’Souza, P.; Kessler, R.; Williams, K.; Leckman, J.F.; Swedo, S. Longitudinal outcomes of children with pediatric autoimmune neuropsychiatric disorder associated with streptococcal infections (PANDAS). Eur. Child Adolesc. Psychiatry 2018, 27, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Carapetis, J.R.; Beaton, A.; Cunningham, M.W.; Guilherme, L.; Karthikeyan, G.; Mayosi, B.M.; Sable, C.; Steer, A.; Wilson, N.; Wyber, R.; et al. Acute rheumatic fever and rheumatic heart disease. Nat. Rev. Dis. Primers 2016, 2, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coffey, P.M.; Ralph, A.P.; Krause, V.L. The role of social determinants of health in the risk and prevention of group a streptococcal infection, acute rheumatic fever and rheumatic heart disease: A systematic review. PLoS Negl. Trop. Dis. 2018, 12, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gewitz, M.H.; Baltimore, R.S.; Tani, L.Y.; Sable, C.A.; Shulman, S.T.; Carapetis, J.; Remenyi, B.; Taubert, K.A.; Bolger, A.F.; Beerman, L.; et al. Revision of the Jones Criteria for the Diagnosis of Acute Rheumatic Fever in the Era of Doppler Echocardiography. Circulation 2015, 131, 1806–1818. [Google Scholar] [CrossRef] [Green Version]
- Karthikeyan, G.; Guilherme, L. Acute rheumatic fever. Lancet 2018, 392, 161–174. [Google Scholar] [CrossRef]
- Webb, R.H.; Grant, C.; Harnden, A. Acute rheumatic fever. BMJ 2015, 351, h3443. [Google Scholar] [CrossRef] [Green Version]
- Carapetis, J.R.; Currie, B.J.; Mathews, J.D. Cumulative incidence of rheumatic fever in an endemic region: A guide to the susceptibility of the population? Epidemiol. Infect. 2000, 124, 239–244. [Google Scholar] [CrossRef]
- Guilherme, L.; Kalil, J. Rheumatic fever and rheumatic heart disease: Cellular mechanisms leading autoimmune reactivity and disease. J. Clin. Immunol. 2010, 30, 17–23. [Google Scholar] [CrossRef]
- Garcia, A.F.; Yamaga, K.M.; Shafer, L.A.; Bollt, O.; Tam, E.K.; Cunningham, M.W.; Kurahara, D.K. Cardiac myosin epitopes recognized by autoantibody in acute and convalescent rheumatic fever. Pediatr. Infect. Dis. J. 2016, 35, 1021–1026. [Google Scholar] [CrossRef] [Green Version]
- Perez-Vigil, A.; Cruz, L.F.D.L.; Brander, G.; Isomura, K.; Gromark, C.; Mataix-Cols, D. The link between autoimmune diseases and obsessive-compulsive and tic disorders: A systematic review. Neurosci. Biobehav. Rev. 2016, 71, 542–562. [Google Scholar] [CrossRef]
- Asbahr, F.R.; Negrao, A.B.; Gentil, V.; Zanetta, D.M.; Paz, J.A.D.; Marques-Dias, M.J.; Kiss, M.H. Obsessive-Compulsive and Related Symptoms in Children and Adolescents with Rheumatic Fever With and Without Chorea: A Prospective 6-Month Study. Am. J. Psychiatry 1998, 155, 1122–1124. [Google Scholar] [CrossRef] [PubMed]
- Grzanka, K.; Pieczyrak, R.; Kotulska, A.; Kucharz, E. Zmiany dotyczace ukladu nerwowego u chorych na goraczke reumatyczna Neurological involvement in patients with rheumatic fever. Reumatologia/Rheumatology 2005, 43, 211–215. [Google Scholar]
- Punukollu, M.; Mushet, N.; Linney, M.; Hennessy, C.; Morton, M. Neuropsychiatric manifestations of Sydenham’s chorea: A systematic review. Dev. Med. Child Neurol. 2016, 58, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Galvin, J.E.; Hemric, M.E.; Ward, K.; Cunningham, M.W. Cytotoxic mAb from rheumatic carditis recognizes heart valves and laminin. J. Clin. Investig. 2000, 106, 217–224. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, M.W. Rheumatic Fever, Autoimmunity, and Molecular Mimicry: The Streptococcal Connection. Int. Rev. Immunol. 2014, 33, 314–329. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, M.W. Streptococcus and rheumatic fever. Curr. Opin. Rheumatol. 2012, 24, 408–416. [Google Scholar] [CrossRef]
- Swedo, S.E.; Leonard, H.L.; Garvey, M.; Mittleman, B.; Allen, A.J.; Perlmutter, S.; Lougee, L.; Dow, S.; Zamkoff, J.; Dubbert, B.K. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: Clinical description of the first 50 cases. Am. J. Psychiatry 1998, 155, 264–271. [Google Scholar] [CrossRef]
- Murphy, T.K.; Gerardi, D.M.; Parker-Athill, E.C. The PANDAS Controversy: Why (and How) Is It Still Unsettled? Curr. Dev. Disord. Rep. 2014, 1, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Swedo, S.E.; Leonard, H.L.; Rapoport, J.L. The pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS) subgroup: Separating fact from fiction. Pediatrics 2004, 113, 907–911. [Google Scholar] [CrossRef]
- Chiarello, F.; Spitoni, S.; Hollander, E.; Matucci Cerinic, M.; Pallanti, S. An expert opinion on PANDAS/PANS: Highlights and controversies. Int. J. Psychiatry Clin. Pract. 2017, 21, 91–98. [Google Scholar] [CrossRef]
- Snider, L.A.; Swedo, S.E. PANDAS: Current status and directions for research. Mol. Psychiatry 2004, 9, 900–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodner, S.M.; Morshed, S.A.; Peterson, B.S. The question of PANDAS in adults. Biol. Psychiatry 2001, 49, 807–810. [Google Scholar] [CrossRef]
- Carelli, R.; Pallanti, S. Streptococcal infections of skin and PANDAS. Dermatol. Ther. 2014, 27, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Jaspers-Fayer, F.; Han, S.H.J.; Chan, E.; McKenney, K.; Simpson, A.; Boyle, A.; Ellwyn, R.; Stewart, S.E. Prevalence of Acute-Onset Subtypes in Pediatric Obsessive-Compulsive Disorder. J. Child Adolesc. Psychopharmacol. 2017, 27, 332–341. [Google Scholar] [CrossRef]
- Swedo, S.E.; Rapoport, J.L.; Cheslow, D.L.; Leonard, H.L.; Ayoub, E.M.; Hosier, D.M.; Wald, E.R. High prevalence of obsessive-compulsive symptoms in patients with Sydenham’s chorea. Am. J. Psychiatry 1989, 146, 246–249. [Google Scholar]
- Swedo, S.E. Sydenham’s chorea: A model for childhood autoimmune neuropsychiatric disorders. JAMA 1994, 272, 1788–1791. [Google Scholar] [CrossRef]
- Gilbert, D.L.; Kurlan, R. PANDAS: Horse or zebra? Neurology 2009, 73, 1252–1253. [Google Scholar] [CrossRef]
- De Oliveira, S.K.; Pelajo, C.F. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infection (PANDAS): A Controversial Diagnosis. Curr. Infect. Dis. Rep. 2010, 12, 103–109. [Google Scholar] [CrossRef]
- Swedo, S.E.; Leckman, J.F.; Rose, N.R. From research subgroup to clinical syndrome: Modifying the PANDAS criteria to describe PANS (pediatric acute-onset neuropsychiatric syndrome). Pediatr. Ther. 2012, 2, 113. [Google Scholar] [CrossRef]
- Murphy, T.K.; Parker-Athill, E.C.; Lewin, A.B.; Storch, E.A.; Mutch, P.J. Cefdinir for recent-onset pediatric neuropsychiatric disorders: A pilot randomized trial. J. Child Adolesc. Psychopharmacol. 2015, 25, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Jadah, R.H.S.; Mujeeb, A.A. Neuropsychiatric symptoms following sore throat in a young boy. BMJ Case Rep. 2019, 12, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, P.J.; Minderaa, R.B. Tic disorders and obsessive-compulsive disorder: Is autoimmunity involved? Int. Rev. Psychiatry 2005, 17, 497–502. [Google Scholar] [CrossRef]
- Bernstein, G.A.; Victor, A.M.; Pipal, A.J.; Williams, K.A. Comparison of clinical characteristics of pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections and childhood obsessive-compulsive disorder. J. Child Adolesc. Psychopharmacol. 2010, 20, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calkin, C.V.; Carandang, C.G. Certain eating disorders may be a neuropsychiatric manifestation of PANDAS: Case report. J. Can. Acad. Child Adolesc. Psychiatry 2007, 16, 132–135. [Google Scholar] [PubMed]
- Murphy, T.K.; Kurlan, R.; Leckman, J. The immunobiology of Tourette’s disorder, pediatric autoimmune neuropsychiatric disorders associated with streptococcus, and related disorders: A way forward. J. Child Adolesc. Psychopharmacol. 2010, 20, 317–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calaprice, D.; Tona, J.; Parker-Athill, E.C.; Murphy, T.K. A Survey of Pediatric Acute-Onset Neuropsychiatric Syndrome Characteristics and Course. J. Child Adolesc. Psychopharmacol. 2017, 27, 607–618. [Google Scholar] [CrossRef] [Green Version]
- Giulino, L.; Gammon, P.; Sullivan, K.; Franklin, M.; Foa, E.; Maid, R.; March, J.S. Is parental report of upper respiratory infection at the onset of obsessive-compulsive disorder suggestive of pediatric autoimmune neuropsychiatric disorder associated with streptococcal infection? J. Child Adolesc. Psychopharmacol. 2002, 12, 157–164. [Google Scholar] [CrossRef]
- Lin, H.; Williams, K.A.; Katsovich, L.; Findley, D.B.; Grantz, H.; Lombroso, P.J.; Kingb, R.A.; Bessenc, D.E.; Johnsond, D.; Kaplan, E.L.; et al. Streptococcal Upper Respiratory Tract Infections and Psychosocial Stress Predict Future Tic and Obsessive-Compulsive Symptom Severity in Children and Adolescents with Tourette Syndrome and Obsessive-Compulsive Disorder. Biol. Psychiatry 2010, 67, 684–691. [Google Scholar] [CrossRef] [Green Version]
- Orlovska, S.; Vestergaard, C.H.; Bech, B.H.; Nordentoft, M.; Vestergaard, M.; Benros, M.E. Association of Streptococcal Throat Infection with Mental Disorders: Testing Key Aspects of the PANDAS Hypothesis in a Nationwide Study. JAMA Psychiatry 2017, 74, 740–746. [Google Scholar] [CrossRef]
- Williams, K.A.; Swedo, S.E. Post-infectious autoimmune disorders: Sydenham’s chorea, PANDAS and beyond. Brain Res. 2015, 1617, 144–154. [Google Scholar] [CrossRef]
- Perrin, E.M.; Murphy, M.L.; Casey, J.R.; Pichichero, M.E.; Runyan, D.K.; Miller, W.C.; Snider, L.A.; Swedo, S.E. Does group a beta-hemolytic streptococcal infection increase risk for behavioral and neuropsychiatric symptoms in children? Arch. Pediatr. Adolesc. Med. 2004, 158, 848–856. [Google Scholar] [CrossRef] [Green Version]
- Murphy, T.K.; Snider, L.A.; Mutch, P.J.; Harden, E.; Zaytoun, A.; Edge, P.J.; Storch, E.A.; Yang, M.C.; Mann, G.; Goodman, W.K.; et al. Relationship of Movements and Behaviors to Group A Streptococcus Infections in Elementary School Children. Biol. Psychiatry 2007, 61, 279–284. [Google Scholar] [CrossRef]
- Garcia-Delgar, B.; Morer, A.; Luber, M.J.; Coffey, B.J. Obsessive-compulsive disorder, tics, and autoinflammatory diseases: Beyond PANDAS. J. Child Adolesc. Psychopharmacol. 2016, 26, 847–850. [Google Scholar]
- Thienemann, M.; Murphy, T.; Leckman, J.; Shaw, R.; Williams, K.; Kapphahn, C.; Frankovich, J.; Geller, D.; Bernstein, G.; Chang, K.; et al. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part I—Psychiatric and Behavioral Interventions. J. Child Adolesc. Psychopharmacol. 2017, 27, 566–573. [Google Scholar] [CrossRef]
- Chang, K.; Frankovich, J.; Cooperstock, M.; Cunningham, M.W.; Latimer, M.E.; Murphy, T.K.; Pasternack, M.; Thienemann, M.; Williams, K.; Walter, J.; et al. Clinical Evaluation of Youth with Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS): Recommendations from the 2013 PANS Consensus Conference. J. Child Adolesc. Psychopharmacol. 2015, 25, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Sen, E.S.; Ramanan, A.V. How to use antistreptolysin O titre. Arch. Dis. Child Educ. Pract. Ed. 2014, 99, 231–238. [Google Scholar] [CrossRef]
- Delice, S. Detection of anti- DNase B antibody upper normal values in children’s age groups who were admitted to hospital with noninfectious reasons. North Clin. Istanbul. 2015, 2, 136–141. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.F.; Bertille, N.; Cohen, R.; Chalumeau, M. Rapid antigen detection test for group A streptococcus in children with pharyngitis (Review). Cochrane Database Syst. Rev. 2016, 7, CD010502. [Google Scholar]
- Katz, B.Z. Streptococcal Infections and Exacerbations in Pediatric Autoimmune Neuropsychiatric Disorder Associated With Streptococcal Infection: A Systematic Review and Meta-Analysis. Pediatr. Infect. Dis. J. 2019, 38, e190–e191. [Google Scholar] [CrossRef]
- Frick, L.; Pittenger, C. Microglial Dysregulation in OCD, Tourette Syndrome, and PANDAS. J. Immunol. Res. 2016, 2016, 1–8. [Google Scholar] [CrossRef]
- Zibordi, F.; Zorzi, G.; Carecchio, M.; Nardocci, N. CANS: Childhood acute neuropsychiatric syndromes. Eur. J. Paediatr. Neurol. 2018, 22, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Giedd, J.N.; Rapoport, J.L.; Garvey, M.A.; Perlmutter, S.; Swedo, S.E. MRI assessment of children with obsessive-compulsive disorder or tics associated with streptococcal infection. Am. J. Psychiatry 2000, 157, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Giedd, J.N.; Rapoport, J.L.; Kruesi, M.J.; Parker, C.; Schapiro, M.B.; Allen, A.J.; Leonard, H.L.; Kaysen, D.; Dickstein, D.P.; Marsch, W.L.; et al. Sydenham’s chorea: Magnetic resonance imaging of the basal ganglia. Neurology 1996, 45, 2199–2202. [Google Scholar] [CrossRef] [PubMed]
- Frick, L.R.; Rapanelli, M.; Jindachomthong, K.; Grant, P.; Leckman, J.F.; Swedo, S.; Williams, K.; Pittenger, C. Differential binding of antibodies in PANDAS patients to cholinergic interneurons in the striatum. Brain Behav. Immun. 2018, 69, 304–311. [Google Scholar] [CrossRef]
- Tay, T.L.; Bechade, C.; D’Andrea, I.; St-Pierre, M.K.; Henry, M.S.; Roumier, A.; Tremblay, M.E. Microglia Gone Rogue: Impacts on Psychiatric Disorders across the Lifespan. Front. Mol. Neurosci. 2018, 4, 421. [Google Scholar] [CrossRef] [Green Version]
- Quagliariello, A.; Del Chierico, F.; Russo, A.; Reddel, S.; Conte, G.; Lopetuso, L.R.; Ianiro, G.; Dallapiccola, B.; Cardona, F.; Gasbarrini, A.; et al. Gut microbiota profiling and gut-brain crosstalk in children affected by pediatric acute-onset neuropsychiatric syndrome and pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. Front. Microbiol. 2018, 9, 1–15. [Google Scholar] [CrossRef]
- Celik, G.G.; Tas, D.A.; Tahiroglu, A.Y.; Erken, E.; Seydaoglu, G.; Ray, P.C.; Avci, A. Mannose-Binding Lectin2 gene polymorphism in PANDAS patients. Noro Psikiyatri Arsivi 2018, 56, 99–105. [Google Scholar]
- Luleyap, H.; Onatoglu, D.; Yilmaz, M.; Alptekin, D.; Tahiroglu, A.; Cetiner, S.; Pazarbasi, A.; Unal, I.; Avci, A.; Comertpay, G. Association between pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections disease and tumor necrosis factor- gene-308 g/a, -850 c/t polymorphisms in 4-12-year-old children in Adana/Turkey. Indian J. Hum. Genet. 2013, 19, 196. [Google Scholar] [CrossRef] [Green Version]
- Morris-Berry, C.M.; Pollard, M.; Gao, S.; Thompson, C.; Singer, H.S. Anti-streptococcal, tubulin, and dopamine receptor 2 antibodies in children with PANDAS and Tourette syndrome: Single-point and longitudinal assessments. J. Neuroimmunol. 2013, 264, 106–113. [Google Scholar] [CrossRef]
- Macerollo, A.; Martino, D. Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS): An Evolving Concept. Tremor Other Hyperkinetic Mov. 2013, 3. [Google Scholar] [CrossRef]
- Hesselmark, E.; Bejerot, S. Biomarkers for diagnosis of Pediatric Acute Neuropsychiatric Syndrome (PANS)-Sensitivity and specificity of the Cunningham Panel. J. Neuroimmunol. 2017, 312, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Snider, L.A.; Lougee, L.; Slattery, M.; Grant, P.; Swedo, S.E. Antibiotic prophylaxis with azithromycin or penicillin for childhood-onset neuropsychiatric disorders. Biol. Psychiatry 2005, 57, 788–792. [Google Scholar] [CrossRef]
- Murphy, T.K.; Brennan, E.M.; Johnco, C.; Parker-Athill, E.C.; Miladinovic, B.; Storch, E.A.; Lewin, A.B. A Double-Blind Randomized Placebo-Controlled Pilot Study of Azithromycin in Youth with Acute-Onset Obsessive-Compulsive Disorder. J. Child Adolesc. Psychopharmacol. 2017, 27, 640–651. [Google Scholar] [CrossRef]
- Aman, M.; Rettiganti, M.; Nagaraja, H.N.; Hollway, J.A.; Mccracken, J.; Mcdougle, C.J.; Tierney, E.; Scahill, L.; Arnold, L.E.; Hellings, J.; et al. Tolerability, safety, and benefits of risperidone in children and adolescents with autism: 21-month follow-up after 8-week placebo-controlled trial. J. Child Adolesc. Psychopharmacol. 2015, 25, 482–493. [Google Scholar] [CrossRef]
- Elia, J.; Dell, M.L.; Friedman, D.F.; Zimmerman, R.A.; Balamuth, N.; Ahmed, A.A.; Pati, S. PANDAS with catatonia: A case report. Therapeutic response to lorazepam and plasmapheresis. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 1145–1150. [Google Scholar] [CrossRef]
- Kovacevic, M.; Grant, P.; Swedo, S.E. Use of Intravenous Immunoglobulin in the Treatment of Twelve Youths with Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections. J. Child Adolesc. Psychopharmacol. 2015, 25, 65–69. [Google Scholar] [CrossRef] [Green Version]
- Storch, E.A.; Murphy, T.K.; Geffken, G.R.; Mann, G.; Adkins, J.J.; Merlo, L.; Duke, D.; Munson, M.; Swaine, Z.; Goodman, W.K. Cognitive-behavioral therapy for PANDAS-related obsessive-compulsive disorder: Findings from a preliminary waitlist controlled open trial. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1171–1178. [Google Scholar] [CrossRef] [Green Version]
- Celik, G.; Taa, D.; Tahiroglu, A.; Avci, A.; Yuksel, B.; Cam, P. Vitamin D deficiency in obsessive-compulsive disorder patients with pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: A case control study. Noro Psikiyatri Arsivi 2016, 53, 31–34. [Google Scholar] [CrossRef]
- Sigra, S.; Hesselmark, E.; Bejerot, S. Treatment of PANDAS and PANS: A systematic review. Neurosci. Biobehav. Rev. 2018, 86, 51–65. [Google Scholar] [CrossRef]
- Cooperstock, M.S.; Swedo, S.E.; Pasternack, M.S.; Murphy, T.K.; Consortium, F.T.P. Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Part III-Treatment and Prevention of Infections. J. Child Adolesc. Psychopharmacol. 2017, 27, 594–606. [Google Scholar] [CrossRef]
- Moore, D.P. Neuropsychiatric aspects of Sydenham’s chorea: A comprehensive review. J. Clin. Psychiatry 1996, 57, 407–414. [Google Scholar]
- Winter, G.; Hart, R.A.; Charlesworth, R.P.G.; Sharpley, C.F. Gut microbiome and depression: What we know and what we need to know. Rev. Neurosci. 2018, 29, 629–643. [Google Scholar] [CrossRef]
- Hermann, A.; Walker, R.H. Diagnosis and Treatment of Chorea Syndromes. Curr. Neurol. Neurosci. Rep. 2015, 15, 514. [Google Scholar] [CrossRef]
- Stern, J.S. Tourette’s syndrome and its borderland. Pract. Neurol. 2018, 18, 262–270. [Google Scholar] [CrossRef]
- Martino, D.; Ganos, C.; Pringsheim, T.M. Tourette Syndrome and Chronic Tic Disorders: The Clinical Spectrum Beyond Tics. Int. Rev. Neurobiol. 2017, 134, 1461–1490. [Google Scholar]
- Hallett, M. Tourette Syndrome: Update. Brain Dev. 2015, 37, 651–655. [Google Scholar] [CrossRef] [Green Version]
- Cavanna, A.E.; Black, K.J.; Hallett, M.; Voon, V. Neurobiology of the Premonitory Urge in Tourette’s Syndrome: Pathophysiology and Treatment Implications. J. Neuropsychiatry Clin. Neurosci. 2017, 29, 95–104. [Google Scholar] [CrossRef] [Green Version]
- Scharf, J.; Yu, D.; Huang, A.; Tsetsos, F.; Paschou, P.; Coppola, G.; Mathews, C. Collaborative Genome-Wide Association and Copy Number Variation Analysis of Tourette Syndrome. Eur. Neuropsychopharmacol. 2019, 29, S736–S737. [Google Scholar] [CrossRef]
- Hirschtritt, M.E.; Darrow, S.M.; Illmann, C.; Osiecki, L.; Grados, M.; Sandor, P.; Dion, Y.; King, R.A.; Pauls, D.; Budman, C.L.; et al. Genetic and phenotypic overlap of specific obsessive-compulsive and attention-deficit/hyperactive subtypes with Tourette syndrome. Psychol. Med. 2017, 48, 279–293. [Google Scholar] [CrossRef] [Green Version]
- Church, A.J. Tourettes syndrome: A cross sectional study to examine the PANDAS hypothesis. J. Neurol. Neurosurg. Psychiatry 2003, 74, 602–607. [Google Scholar] [CrossRef] [Green Version]
- Spinello, C.; Laviola, G.; Macri, S. Pediatric Autoimmune Disorders Associated with Streptococcal Infections and Tourettes Syndrome in Preclinical Studies. Front. Neurosci. 2016, 10, 310. [Google Scholar] [CrossRef]
- Suhs, K.-W.; Skripuletz, T.; Pul, R.; Alvermann, S.; Schwenkenbecher, P.; Stangel, M.; Muller-Vahl, K. Gilles de la Tourette syndrome is not linked to contactin-associated protein receptor 2 antibodies. Mol. Brain 2015, 8, 62. [Google Scholar] [CrossRef] [Green Version]
- Oosterveer, D.M.; Overweg-Plandsoen, W.C.; Roos, R.A. Sydenhams Chorea: A Practical Overview of the Current Literature. Pediatr. Neurol. 2010, 43, 1–6. [Google Scholar] [CrossRef]
- Crealey, M.; Allen, N.M.; Webb, D.; Bouldin, A.; Sweeney, N.M.; Peake, D.; Tirupathi, S.; Butler, K.; King, M.D. Sydenhams chorea: Not gone but perhaps forgotten. Arch. Dis. Child. 2015, 100, 1160–1162. [Google Scholar] [CrossRef]
- Murphy, T.K.; Goodman, W.K.; Ayoub, E.M.; Voeller, K.K. On defining Sydenham’s chorea: Where do we draw the line? Biol. Psychiatry 2000, 47, 851–857. [Google Scholar] [CrossRef]
- Walker, K.G.; De Vries, P.J.; Stein, D.J.; Wilmshurst, J.M. Sydenham chorea and PANDAS in South Africa: Review of evidence and recommendations for management in resource-poor countries. J. Child Neurol. 2015, 30, 850–859. [Google Scholar] [CrossRef]
- Morris, C.M.; Pardo-Villamizar, C.; Gause, C.D.; Singer, H.S. Serum autoantibodies measured by immunofluorescence confirm a failure to differentiate PANDAS and Tourette syndrome from controls. J. Neurol. Sci. 2009, 276, 45–48. [Google Scholar] [CrossRef]
- Gamucci, A.; Uccella, S.; Sciarretta, L.; D’Apruzzo, M.; Calevo, M.G.; Mancardi, M.M.; Veneselli, E.; De Grandis, E. PANDAS and PANS: Clinical, Neuropsychological, and Biological Characterization of a Monocentric Series of Patients and Proposal for a Diagnostic Protocol. J. Child Adolesc. Psychopharmacol. 2019, 29, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Lehman, M.; Navarro, V.; Suchecki, D.; Handa, R. Introduction to the PANS special issue. J. Neuroendocrinol. 2018, 30, 12612. [Google Scholar] [CrossRef]
- Frankovich, J.; Thienemann, M.; Rana, S.; Chang, K. Five Youth with Pediatric Acute-Onset Neuropsychiatric Syndrome of Differing Etiologies. J. Child Adolesc. Psychopharmacol. 2015, 25, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Muller, N.; Schwarz, M.J. Neuroimmune-endocrine crosstalk in schizophrenia and mood disorders. Expert Rev. Neurother. 2006, 6, 1017–1038. [Google Scholar] [CrossRef]
- Hornig, M. The role of microbes and autoimmunity in the pathogenesis of neuropsychiatric illness. Curr. Opin. Rheumatol. 2013, 25, 488–495. [Google Scholar] [CrossRef]
- Morer, A.; Viñas, O.; Lázaro, L.; Bosch, J.; Toro, J.; Castro, J. D8/17 Monoclonal Antibody: An Unclear Neuropsychiatric Marker. Behav. Neurol. 2005, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Sokol, M.S.; Ward, P.E.; Tamiya, H.; Kondo, D.G.; Houston, D.; Zabriskie, J.B. D8/17 Expression on B Lymphocytes in Anorexia Nervosa. Am. J. Psychiatry 2002, 159, 1430–1432. [Google Scholar] [CrossRef]
- Bronze, M.S.; Dale, J.B. Epitopes of streptococcal M proteins that evoke antibodies that cross-react with human brain. J. Immunol. 1993, 151, 2820–2828. [Google Scholar]
- Kim, S.W.; Grant, J.E.; Kim, S.I.; Swanson, T.A.; Bernstein, G.A.; Jaszcz, W.B.; Williams, K.A.; Schlievert, P.M. A Possible Association of Recurrent Streptococcal Infections and Acute Onset of Obsessive-Compulsive Disorder. J. Neuropsychiatry Clin. Neurosci. 2004, 16, 252–260. [Google Scholar] [CrossRef]
- Marazziti, D.; Albert, U.; Mucci, F.; Piccinni, A. The Glutamate and the Immune Systems: New Targets for the Pharmacological Treatment of OCD. Curr. Med. Chem. 2018, 25, 5731–5738. [Google Scholar] [CrossRef]
- Macri, S.; Spinello, C.; Widomska, J.; Magliozzi, R.; Poelmans, G.; Invernizzi, R.W.; Creti, R.; Roessner, V.; Bartolini, E.; Margarit, I.; et al. Neonatal corticosterone mitigates autoimmune neuropsychiatric disorders associated with streptococcus in mice. Sci. Rep. 2018, 8, 1–12. [Google Scholar] [CrossRef]
- Kipnis, J.; Cardon, M.; Avidan, H.; Lewitus, G.M.; Mordechay, S.; Rolls, A.; Shani, Y.; Schwartz, M. Dopamine, through the extracellular signal-regulated kinase pathway, downregulates CD4+CD25+ regulatory T-cell activity: Implications for neurodegeneration. J. Neurosci. 2004, 24, 6133–6143. [Google Scholar] [CrossRef] [Green Version]
- Besser, M.J.; Ganor, Y.; Levite, M. Dopamine by itself activates either D2, D3 or D1/D5 dopaminergic receptors in normal human T-cells and triggers the selective secretion of either IL-10, TNFalpha or both. J. Neuroimmunol. 2005, 169, 161–171. [Google Scholar] [CrossRef]
- Ben-Pazi, H.; Stoner, J.A.; Cunningham, M.W. Dopamine Receptor Autoantibodies Correlate with Symptoms in Sydenham’s Chorea. PLoS ONE 2013, 8, e73516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravindran, A.V.; Griffiths, J.; Merali, Z.; Anisman, H. Circulating lymphocyte subsets in obsessive compulsive disorder, major depression and normal controls. J. Affect. Disord. 1999, 52, 1–10. [Google Scholar] [CrossRef]
- Lamothe, H.; Baleyte, J.-M.; Smith, P.; Pelissolo, A.; Mallet, L. Individualized Immunological Data for Precise Classification of OCD Patients. Brain Sci. 2018, 8, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, T.K.; Storch, E.A.; Lewin, A.B.; Edge, P.J.; Goodman, W.K. Clinical factors associated with pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. J. Pediatr. 2012, 160, 314–319. [Google Scholar] [CrossRef] [Green Version]
- Levite, M. Dopamine and T Cells: Dopamine Receptors and Potent Effects on T Cells, Dopamine Production in T Cells, and Abnormalities in the Dopaminergic System in T Cells in Autoimmune, Neurological and Psychiatric Diseases. Acta Physiol. 2016, 216, 42–89. [Google Scholar] [CrossRef]
- Gruner, P.; Pittenger, C. Cognitive inflexibility in Obsessive-Compulsive Disorder. Neuroscience 2017, 345, 243–255. [Google Scholar] [CrossRef] [Green Version]
- Kirvan, C.A.; Swedo, S.E.; Snider, L.A.; Cunningham, M.W. Antibody-mediated neuronal cell signaling in behavior and movement disorders. J. Neuroimmunol. 2006, 179, 173–179. [Google Scholar] [CrossRef]
- Cunningham, M.W. Rheumatic fever revisited. Nat. Rev. Cardiol. 2014, 11, 123. [Google Scholar] [CrossRef] [Green Version]
- Hughes, R.; MedSci, F.; Bensa, S.; Willison, H.; Van Den Bergh, P.; Comi, G.; IIIa, I.; Nobile-Orazio, E.; van Doorn, P.; Dalakas, M.; et al. Randomized controlled trial of intravenous immunoglobulin versus oral prednisolone in chronic inflammatory demyelinating polyradiculoneuropathy. Ann. Neurol. 2001, 50, 195–201. [Google Scholar] [CrossRef]
- Kataoka, Y.; Kalanithi, P.S.A.; Grantz, H.; Schwartz, M.L.; Saper, C.; Leckman, J.F.; Vaccarino, F.M. Decreased number of parvalbumin and cholinergic interneurons in the striatum of individuals with Tourette syndrome. J. Comp. Neurol. 2010, 518, 277–291. [Google Scholar] [CrossRef]
- Bonsi, P.; Cuomo, D.; Martella, G.; Madeo, G.; Schirinzi, T.; Puglisi, F.; Ponterio, G.; Pisani, A. Centrality of Striatal Cholinergic Transmission in Basal Ganglia Function. Front. Neuroanat. 2011, 5, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swedo, S.; Williams, K. PANDAS as a post-Streptococcal autoimmune neuropsychiatric form of OCD. In Obsessive-Compulsive Disorder: Phenomenology, Pathophysiology, and Treatment; Pittenger, C., Ed.; Oxford University Press: New York, NY, USA, 2017; pp. 311–321. [Google Scholar]
- Cox, C.J.; Sharma, M.; Leckman, J.F.; Zuccolo, J.; Zuccolo, A.; Kovoor, A.; Swedo, S.E.; Cunningham, M.W. Brain Human Monoclonal Autoantibody from Sydenham Chorea Targets Dopaminergic Neurons in Transgenic Mice and Signals Dopamine D2 Receptor: Implications in Human Disease. J. Immunol. 2013, 191, 5524–5541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sciamanna, G.; Napolitano, F.; Pelosi, B.; Bonsi, P.; Vitucci, D.; Nuzzo, T.; Punzo, D.; Ghiglieri, V.; Ponterio, G.; Pasqualetti, M.; et al. Rhes regulates dopamine D2 receptor transmission in striatal cholinergic interneurons. Neurobiol. Dis. 2015, 78, 146–161. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.; Stevens, B.; Sierra, A.; Wake, H.; Bessis, A.; Nimmerjahn, A. The role of microglia in the healthy brain. J. Neurosci. 2011, 31, 16064–16069. [Google Scholar] [CrossRef]
- Du, L.; Zhang, Y.; Chen, Y.; Zhu, J.; Yang, Y.; Zhang, H.L. Role of Microglia in Neurological Disorders and Their Potentials as a Therapeutic Target. Mol. Neurobiol. 2017, 54, 7567–7584. [Google Scholar] [CrossRef]
- Dileepan, T.; Smith, E.D.; Knowland, D.; Hsu, M.; Platt, M.; Bittner-Eddy, P.; Cohen, B.; Southern, P.; Latimer, E.; Harley, E.; et al. Group A Streptococcus intranasal infection promotes CNS infiltration by streptococcal-specific Th17 cells. J. Clin. Investig. 2016, 126, 303–317. [Google Scholar] [CrossRef] [Green Version]
- Husby, G.; Rijn, I.D.; Zabriskie, J.; Abdin, Z.; Williams, R. Anti-Neuronal Antibody in Sydenhams Chorea. Lancet 1977, 309, 1208. [Google Scholar] [CrossRef]
- Kirvan, C.A.; Swedo, S.E.; Heuser, J.S.; Cunningham, M.W. Mimicry and autoantibody-mediated neuronal cell signaling in Sydenham chorea. Nat. Med. 2003, 9, 914–920. [Google Scholar] [CrossRef]
- Kirvan, C.A.; Cox, C.J.; Swedo, S.E.; Cunningham, M.W. Tubulin Is a Neuronal Target of Autoantibodies in Sydenham’s Chorea. J. Immunol. 2007, 178, 7412–7421. [Google Scholar] [CrossRef]
- Kirvan, C.A.; Swedo, S.E.; Kurahara, D.; Cunningham, M.W. Streptococcal mimicry and antibody-mediated cell signaling in the pathogenesis of Sydenhams chorea. Autoimmunity 2006, 39, 21–29. [Google Scholar] [CrossRef]
- Hoffman, K.L. A Murine Model for Neuropsychiatric Disorders Associated with Group A -Hemolytic Streptococcal Infection. J. Neurosci. 2004, 24, 1780–1791. [Google Scholar] [CrossRef] [PubMed]
- Brimberg, L.; Benhar, I.; Mascaro-Blanco, A.; Alvarez, K.; Lotan, D.; Winter, C.; Klein, J.; Moses, A.E.; Somnier, F.E.; Leckman, J.F. Behavioral, Pharmacological, and Immunological Abnormalities after Streptococcal Exposure: A Novel Rat Model of Sydenham Chorea and Related Neuropsychiatric Disorders. Neuropsychopharmacology 2012, 37, 2076–2087. [Google Scholar] [CrossRef] [PubMed]
- Yaddanapudi, K.; Hornig, M.; Serge, R.; Miranda, J.D.; Baghban, A.; Villar, G.; Lipkin, W.I. Passive transfer of streptococcus-induced antibodies reproduces behavioral disturbances in a mouse model of pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection. Mol. Psychiatry 2009, 15, 712–726. [Google Scholar] [CrossRef] [PubMed]
- Church, A.J.; Dale, R.C.; Giovannoni, G. Anti-basal ganglia antibodies: A possible diagnostic utility in idiopathic movement disorders? Arch. Dis. Child 2004, 89, 611–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlmutter, S.J.; Leitman, S.F.; Garvey, M.A.; Hamburger, S.; Feldman, E.; Leonard, H.L.; Swedo, S.E. Therapeutic plasma exchange and intravenous immunoglobulin for obsessive-compulsive disorder and tic disorders in childhood. Lancet 1999, 354, 1153–1158. [Google Scholar] [CrossRef]
- Ben-Pazi, H.; Sadan, O.; Offen, D. Striatal Microinjection of Sydenham Chorea Antibodies: Using a Rat Model to Examine the Dopamine Hypothesis. J. Mol. Neurosci. 2012, 46, 162–166. [Google Scholar] [CrossRef]
- Lotan, D.; Benhar, I.; Alvarez, K.; Mascaro-Blanco, A.; Brimberg, L.; Frenkel, D.; Cunningham, M.W.; Joel, D. Behavioral and neural effects of intra-striatal infusion of anti-streptococcal antibodies in rats. Brain Behav. Immun. 2014, 38, 249–262. [Google Scholar] [CrossRef] [Green Version]
- Pavone, P.; Bianchini, R.; Parano, E.; Incorpora, G.; Rizzo, R.; Mazzone, L.; Trifiletti, R.R. Anti-brain antibodies in PANDAS versus uncomplicated streptococcal infection. Pediatr. Neurol. 2004, 30, 107–110. [Google Scholar] [CrossRef] [Green Version]
- da Rocha, F.F.; Correa, H.; Teixeira, A.L. Obsessive-compulsive disorder and immunology: A review. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2008, 32, 1139–1146. [Google Scholar] [CrossRef]
- Peterson, B.S.; Leckman, J.F.; Tucker, D.; Scahill, L.; Staib, L.; Zhang, H.; King, R.; Cohen, D.J.; Gore, J.C.; Lombroso, P. Preliminary findings of antistreptococcal antibody titers and basal ganglia volumes in tic, obsessive-compulsive, and attention- deficit/hyperactivity disorders. Arch. Gen. Psychiatry 2000, 57, 364–372. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, R.; Gulisano, M.; Pavone, P.; Fogliano, F.; Robertson, M.M. Increased antistreptococcal antibody titers and anti-basal ganglia antibodies in patients with Tourette syndrome: Controlled cross-sectional study. J. Child Neurol. 2006, 21, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, B.; Romero-Rebollar, C.; Jimenez-Angeles, L.; Genis-Mendoza, A.D.; Flores, J.; Lanzagorta, N.; Arroyo, M.; de la Fuente-Sandoval, C.; Santana, D.; Medina-Banuelos, V.; et al. Neuroanatomical features and its usefulness in classification of patients with PANDAS. CNS Spectr. 2018, 24, 533–543. [Google Scholar] [CrossRef]
- Snider, L.A.; Swedo, S.E. Post-streptococcal Autoimmune Disorders of the Central Nervous System. Curr. Opin. Neurol. 2003, 16, 359–365. [Google Scholar] [PubMed]
- Bellini, S.; Fleming, K.E.; De, M.; McCauley, J.P.; Petroccione, M.A.; D’Brant, L.Y.; Tkachenko, A.; Kwon, S.; Jones, L.A.; Scimemi, A. Neuronal Glutamate Transporters Control Dopaminergic Signaling and Compulsive Behaviors. J. Neurosci. 2018, 38, 937–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stollerman, G.H. Rheumatic Fever in the 21st Century. Clin. Infect. Dis. 2001, 33, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, M.W. Molecular Mimicry, Autoimmunity, and Infection: The Cross-Reactive Antigens of Group A Streptococci and their Sequelae. Gram Posit. Pathog. 2019, 7, 86–107. [Google Scholar]
- Kumar, A.; Williams, M.T.; Chugani, H.T. Evaluation of Basal Ganglia and Thalamic Inflammation in Children with Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infection and Tourette Syndrome: A Positron Emission Tomographic (PET) Study Using 11C-[R]-PK11. J. Child Neurol. 2015, 30, 749–756. [Google Scholar] [CrossRef]
- Malan-Muller, S.; Valles-Colomer, M.; Raes, J.; Lowry, C.A.; Seedat, S.; Hemmings, S.M.J. The gut microbiome and mental health: Implications for anxiety- and trauma-related disorders. Omics J. Integr. Biol. 2018, 22, 90–107. [Google Scholar] [CrossRef]
- Lach, G.; Schellekens, H.; Dinan, T.G.; Cryan, J.F. Anxiety, Depression, and the Microbiome: A Role for Gut Peptides. Neurotherapeutics 2018, 15, 36–59. [Google Scholar] [CrossRef] [Green Version]
- Gulas, E.; Wysiadecki, G.; Strzelecki, D.; Gawlik-Kotelnicka, O.; Polguj, M. Can microbiology affect psychiatry? A link between gut microbiota and psychiatric disorders. Psychiatr. Pol. 2018, 52, 1023–1039. [Google Scholar]
- Foster, J.A.; McVey Neufeld, K.A. Gut-brain axis: How the microbiome influences anxiety and depression. Trends Neurosci. 2013, 36, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Fowlie, G.; Cohen, N.; Ming, X. The perturbance of microbiome and gut-brain axis in autism spectrum disorders. Int. J. Mol. Sci. 2018, 19, 2251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seitz, J.; Trinh, S.; Herpertz-Dahlmann, B. The Microbiome and Eating Disorders. Psychiatr. Clin. N. Am. 2019, 42, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Caputi, V.; Giron, M.C. Microbiome-gut-brain axis and toll-like receptors in parkinson’s disease. Int. J. Mol. Sci. 2018, 19, 1689. [Google Scholar] [CrossRef] [Green Version]
- Sochocka, M.; Donskow-Lysoniewska, K.; Diniz, B.S.; Kurpas, D.; Brzozowska, E.; Leszek, J. The Gut Microbiome Alterations and Inflammation-Driven Pathogenesis of Alzheimer’s Disease—A Critical Review. Mol. Neurobiol. 2019, 56, 1841–1851. [Google Scholar] [CrossRef] [Green Version]
- Aarts, E.; Ederveen, T.H.A.; Naaijen, J.; Zwiers, M.P.; Boekhorst, J.; Timmerman, H.M.; Smeekens, S.P.; Netea, M.G.; Buitelaar, J.K.; Franke, B.; et al. Gut microbiome in ADHD and its relation to neural reward anticipation. PLoS ONE 2017, 12, 1–17. [Google Scholar]
- Kanji, S.; Fonseka, T.M.; Marshe, V.S.; Sriretnakumar, V.; Hahn, M.K.; Muller, D.J. The microbiome-gut-brain axis: Implications for schizophrenia and antipsychotic induced weight gain. Eur. Arch. Psychiatry Clin. Neurosci. 2018, 268, 3–15. [Google Scholar] [CrossRef]
- Leclercq, S.; Matamoros, S.; Cani, P.D.; Neyrinck, A.M.; Jamar, F.; Starkel, P.; Windey, K.; Trematoli, V.; Backhed, F.; Verbeke, K.; et al. Intestinal permeability, gut-bacterial dysbiosis, and behavioral markers of alcohol-dependence severity. Proc. Natl. Acad. Sci. USA 2014, 111, E4485–E4493. [Google Scholar] [CrossRef] [Green Version]
- Gondalia, S.; Parkinson, L.; Stough, C.; Scholey, A. Gut microbiota and bipolar disorder: A review of mechanisms and potential targets for adjunctive therapy. Psychopharmacology 2019, 236, 1433–1443. [Google Scholar] [CrossRef]
- Tang, Y.; Liu, S.; Shu, H.; Yanagisawa, L.; Tao, F. Gut Microbiota Dysbiosis Enhances Migraine-Like Pain Via TNF Upregulation. Mol. Neurobiol. 2019, 57, 461–468. [Google Scholar] [CrossRef]
- Milliken, S.; Allen, R.M.; Lamont, R.F. The role of antimicrobial treatment during pregnancy on the neonatal gut microbiome and the development of atopy, asthma, allergy and obesity in childhood. Expert Opin. Drug Saf. 2019, 18, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Jasarevic, E.; Howard, C.D.; Misic, A.M.; Beiting, D.P.; Bale, T.L. Stress during pregnancy alters temporal and spatial dynamics of the maternal and offspring microbiome in a sex-specific manner. Sci. Rep. 2017, 7, 44182. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.R.; Clarke, G.; Cryan, J.F.; Dinan, T.G. Brain-gut-microbiota axis: Challenges for translation in psychiatry. Ann. Epidemiol. 2016, 26, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Rudzki, L.; Szulc, A. Immune Gate of Psychopathology-The Role of Gut Derived Immune Activation in Major Psychiatric Disorders. Front. Psychiatry 2018, 9, 205. [Google Scholar] [CrossRef] [Green Version]
- Lener, M.S.; Niciu, M.J.; Ballard, E.D.; Park, M.; Park, L.T.; Nugent, A.C.; Zarate, C.A., Jr. Glutamate and Gamma-Aminobutyric Acid Systems in the Pathophysiology of Major Depression and Antidepressant Response to Ketamine. Biol. Psychiatry 2017, 81, 886–897. [Google Scholar] [CrossRef] [Green Version]
- Lydiard, R.B. The role of GABA in anxiety disorders. J. Clin. Psychiatry 2003, 64 (Suppl. 3), 21–27. [Google Scholar]
- Romeo, B.; Choucha, W.; Fossati, P.; Rotge, J.-Y. Meta-analysis of central and peripheral Y-aminobutyric acid levels in patients with unipolar and bipolar depression. J. Psychiatry Neurosci. 2018, 43, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Freed, R.D.; Coffey, B.J.; Mao, X.; Weiduschat, N.; Kang, G.; Shungu, D.C.; Gabbay, V. Decreased Anterior Cingulate Cortex Y-Aminobutyric Acid in Youth with Tourettes Disorder. Pediatr. Neurol. 2016, 65, 64–70. [Google Scholar] [CrossRef]
- Gabbay, V.; Bradley, K.A.; Mao, X.; Ostrover, R.; Kang, G.; Shungu, D.C. Anterior cingulate cortex Y-aminobutyric acid deficits in youth with depression. Transl. Psychiatry 2017, 7, e1216. [Google Scholar] [CrossRef]
- Chiu, P.; Lui, S.S.; Hung, K.S.; Chan, R.C.; Chan, Q.; Sham, P.; Cheung, E.F.C.; Mak, H.K.F. In vivo gamma-aminobutyric acid and glutamate levels in people with first-episode schizophrenia: A proton magnetic resonance spectroscopy study. Schizophr. Res. 2018, 193, 295–303. [Google Scholar] [CrossRef]
- Gubellini, P.; Pisani, A.; Centonze, D.; Bernardi, G.; Calabresi, P. Metabotropic glutamate receptors and striatal synaptic plasticity: Implications for neurological diseases. Prog. Neurobiol. 2004, 74, 271–300. [Google Scholar] [CrossRef] [PubMed]
- Sherwin, E.; Sandhu, K.V.; Dinan, T.G.; Cryan, J.F. May the Force Be with You: The Light and Dark Sides of the Microbiota-Gut-Brain Axis in Neuropsychiatry. CNS Drugs 2016, 30, 1019–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, J.M.; Murphy, K.; Stanton, C.; Ross, R.P.; Kober, O.I.; Juge, N.; Avershina, E.; Rudi, K.; Narbad, A.; Jenmalm, M.C.; et al. The composition of the gut microbiota throughout life, with an emphasis on early life. Microb. Ecol. Health Dis. 2015, 26, 26050. [Google Scholar] [CrossRef]
- Otoole, P.W.; Claesson, M.J. Gut microbiota: Changes throughout the lifespan from infancy to elderly. Int. Dairy J. 2010, 20, 281–291. [Google Scholar] [CrossRef]
- Aleman, F.D.D.; Valenzano, D.R. Microbiome evolution during host aging. PLoS Pathog. 2019, 15, e1007727. [Google Scholar] [CrossRef] [PubMed]
- Derrien, M.; Alvarez, A.-S.; Vos, W.M.D. The Gut Microbiota in the First Decade of Life. Trends Microbiol. 2019, 27, 997–1010. [Google Scholar] [CrossRef] [Green Version]
- Becattini, S.; Taur, Y.; Pamer, E.G. Antibiotic-induced changes in the intestinal microbiota and disease. Trends Mol. Med. 2016, 22, 458–478. [Google Scholar] [CrossRef] [Green Version]
- Murphy, T.K.; Storch, E.A.; Turner, A.; Reid, J.M.; Tan, J.; Lewin, A.B. Maternal history of autoimmune disease in children presenting with tics and/or obsessive-compulsive disorder. J. Neuroimmunol. 2010, 229, 243–247. [Google Scholar] [CrossRef] [Green Version]
- O’Roak, B.J.; Morgan, T.M.; Fishman, D.O.; Saus, E.; Alonso, P.; Gratacos, M.; Estivill, X.; Teltsh, O.; Kohn, Y.; Kidd, K.K.; et al. Additional support for the association of SLITRK1 var321 and Tourette syndrome. Mol. Psychiatry 2010, 15, 447–450. [Google Scholar] [CrossRef]
- Tian, Y.; Gunther, J.R.; Liao, I.H.; Liu, D.; Ander, B.P.; Stamova, B.S.; Lit, L.; Jickling, G.C.; Xu, H.; Zhan, X.; et al. GABA- and acetylcholine-related gene expression in blood correlate with tic severity and microarray evidence for alternative splicing in Tourette syndrome: A pilot study. Brain Res. 2011, 1381, 228–236. [Google Scholar] [CrossRef]
- Neth, O.; Jack, D.L.; Dodds, A.W.; Holzel, H.; Klein, N.J.; Turner, M.W. Mannose-binding lectin binds to a range of clinically relevant microorganisms and promotes complement deposition. Infect. Immun. 2000, 68, 688–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Xu, Z.; Ou, X.; Wang, M.; Yang, X.; Li, Q. Mannose-binding lectin polymorphisms and recurrent respiratory tract infection in Chinese children. Eur. J. Pediatr. 2009, 168, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Gomaa, M.H.; Ali, S.S.; Fattouh, A.M.; Hamza, H.S.; Badr, M.M. MBL2 gene polymorphism rs1800450 and rheumatic fever with and without rheumatic heart disease: An Egyptian pilot study. Pediatr. Rheumatol. 2018, 16, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, J.S. Tic Disorders and PANDAS. Semin. Pediatr. Neurol. 2018, 25, 25–33. [Google Scholar] [CrossRef]
- Farhood, Z.; Ong, A.A.; Discolo, C.M. PANDAS: A systematic review of treatment options. Int. J. Pediatr. Otorhinolaryngol. 2016, 89, 149–153. [Google Scholar] [CrossRef]
- Frankovich, J. 23.3 Clinical Management of Pediatric Acute-Onset Neuropsychiatric Syndrome: Use of Immunomodulatory Therapies. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, S339. [Google Scholar] [CrossRef]
- Brown, K.D.; Farmer, C.; Freeman, G.M.; Spartz, E.J.; Farhadian, B.; Thienemann, M.; Frankovich, J. Effect of Early and Prophylactic Nonsteroidal Anti-Inflammatory Drugs on Flare Duration in Pediatric Acute-Onset Neuropsychiatric Syndrome: An Observational Study of Patients Followed by an Academic Community-Based Pediatric Acute-Onset Neuropsychiatric Syndrome Clinic. J. Child Adolesc. Psychopharmacol. 2017, 27, 619–628. [Google Scholar]
- Hesselmark, E.; Bejerot, S. Patient Satisfaction and Treatments Offered to Swedish Patients with Suspected Pediatric Acute-Onset Neuropsychiatric Syndrome and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections. J. Child Adolesc. Psychopharmacol. 2019, 29, 634–641. [Google Scholar] [CrossRef] [Green Version]
- Mahapatra, A.; Panda, P.K.; Sagar, R. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection treated successfully with a course of oral antibiotics. Asian J. Psychiatr. 2017, 25, 256–257. [Google Scholar] [CrossRef]
- Swedo, S.E.; Frankovich, J.; Murphy, T.K. Overview of Treatment of Pediatric Acute-Onset Neuropsychiatric Syndrome. J. Child Adolesc. Psychopharmacol. 2017, 27, 562–565. [Google Scholar] [CrossRef] [Green Version]
- Hirschtritt, M.E.; Bloch, M.H.; Mathews, C.A. Obsessive-Compulsive Disorder. JAMA 2017, 317, 1358. [Google Scholar] [CrossRef] [PubMed]
- Cognitive-Behavior Therapy, Sertraline, and Their Combination for Children and Adolescents with Obsessive-Compulsive Disorder. JAMA 2004, 292, 1969. [CrossRef] [PubMed] [Green Version]
- Ost, L.-G.; Riise, E.N.; Wergeland, G.J.; Hansen, B.; Kvale, G. Cognitive behavioral and pharmacological treatments of OCD in children: A systematic review and meta-analysis. J. Anxiety Disord. 2016, 43, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Demirkaya, S.K.; Demirkaya, M.; Yusufo_lu, C.; Akln, E. Atomoxetine Use in Attention-Deficit/Hyperactivity Disorder and Comorbid Tic Disorder in Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections. J. Child Adolesc. Psychopharmacol. 2017, 27, 104–105. [Google Scholar] [CrossRef] [Green Version]
- Spartz, E.J.; Freeman, G.M., Jr.; Brown, K.; Farhadian, B.; Thienemann, M.; Frankovich, J. Course of Neuropsychiatric Symptoms After Introduction and Removal of Nonsteroidal Anti-Inflammatory Drugs: A Pediatric Observational Study. J. Child Adolesc. Psychopharmacol. 2017, 27, 652–659. [Google Scholar] [CrossRef]
- Alexander, A.A.Z.; Patel, N.J.; Southammakosane, C.A.; Mortensen, M.M. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS): An indication for tonsillectomy. Int. J. Pediatr. Otorhinolaryngol. 2011, 75, 872–873. [Google Scholar] [CrossRef]
- Windfuhr, J.P.; Hilf, K.M. Tonsillectomy remains a questionable option for pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS). GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 2016, 15, 110–115. [Google Scholar]
- Demesh, D.; Virbalas, J.M.; Bent, J.P. The role of tonsillectomy in the treatment of Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS). JAMA Otolaryngol. Head Neck Surg. 2015, 141, 272–275. [Google Scholar] [CrossRef] [Green Version]
- Wilbur, C.; Bitnun, A.; Kronenberg, S.; Laxer, R.M.; Levy, D.M.; Logan, W.J.; Shouldice, M.; Yeh, E.A. PANDAS/PANS in childhood: Controversies and evidence. Paediatr. Child Health 2019, 24, 85–91. [Google Scholar] [CrossRef]
- Pavone, P.; Falsaperla, R.; Nicita, F.; Zecchini, A.; Battaglia, C.; Spalice, A.; Iozzi, L.; Parano, E.; Vitaliti, G.; Verrotti, A.; et al. Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infection (PANDAS): Clinical Manifestations, IVIG Treatment Outcomes, Results from a Cohort of Italian Patients. Neuropsychiatry 2018, 8, 854–860. [Google Scholar] [CrossRef]
- Latimer, M.E.; L’Etoile, N.; Seidlitz, J.; Swedo, S.E. Therapeutic plasma apheresis as a treatment for 35 severely Ill children and adolescents with pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections. J. Child Adolesc. Psychopharmacol. 2015, 25, 70–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moretti, G.; Pasquini, M.; Mandarelli, G.; Tarsitani, L.; Biondi, M. What every psychiatrist should know about PANDAS: A review. Clin. Pract. Epidemiol. Ment. Health 2008, 4, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dale, R. Autoimmunity and the basal ganglia: New insights into old diseases. QJM 2003, 96, 183–191. [Google Scholar] [CrossRef]
- Singer, H.S.; Loiselle, C.R.; Lee, O.; Minzer, K.; Swedo, S.; Grus, F.H. Anti-basal ganglia antibodies in PANDAS. Mov. Disord. 2004, 19, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Yazici, K.U.; Percinel Yazici, I.; Ustundag, B. Vitamin D levels in children and adolescents with obsessive-compulsive disorder. Nord. J. Psychiatry 2018, 72, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Stagi, S.; Lepri, G.; Rigante, D.; Cerinic, M.M.; Falcini, F. Cross-Sectional Evaluation of Plasma Vitamin D Levels in a Large Cohort of Italian Patients with Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections. J. Child Adolesc. Psychopharmacol. 2018, 28, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Boileau, B. A review of obsessive-compulsive disorder in children and adolescents. Dialogues Clin. Neurosci. 2011, 13, 401–411. [Google Scholar] [PubMed]
- Centonze, D.; Gubellini, P.; Pisani, A.; Bernardi, G.; Calabresi, P. Dopamine, Acetylcholine and Nitric Oxide Systems Interact to Induce Corticostriatal Synaptic Plasticity. Rev. Neurosci. 2003, 14, 207–216. [Google Scholar] [CrossRef]


{kind=link}
| Psychiatric Syndrome | Symptoms | Changes in CNS | Changes in Microbiota | Genetic Alterations/Mutations | Presence of Antibodies | Available Treatment |
|---|---|---|---|---|---|---|
| PANDAS | OCD, tics, obsessions, compulsions [60], anxiety, agitation, aggression, insomnia, impulsiveness, emotional lability, depression, hyperactivity, suicidality [54], dysuric symptoms, dilated pupils, inattention, behavioral regress, dysgraphia, visual and auditory hallucinations, irritation [61] | Enlarged striatum, caudate, putamen, basal ganglia and globus pallidus [62,63], dysregulation within striatal interneurons [64], overactivation of microglia [65], increased number of antineuronal antibody titers [63] | Higher percentage of Bacteroidetes, Rikenellaceae and Odoribacteriaceae; lower of Firmicutes and Actinobacteria; absence of Saccharibacteria and Turicibacteraceae, Tissierellaceae, Gemellaceae, and Carnobacteriaceae (Bacilli class), Corynebacteriaceae and Lachnospiracea (Clostridia class) [66] | MBL2 [67], TNF-α −308 AA polymorphism [68] | Autoantibodies against: dopamine D1, D2 receptor, tubulin, lysoganglioside, antipyruvate kinase [69,70], calcium calmodulin dependent kinase II [71] | Penicillin V, amoxicillin, azithromycin [72,73], steroids, antipsychoactive drugs (risperidone) [74], immunotherapeutic, plasmapheresis [75], intravenous immunoglobulins [76], cognitive-behavioral therapy, SSRIs [77], vitamin D supplementation [78] |
| PANS | OCD, tics, impaired food intake, anxiety, separation fear, motor dysfunctions, dysgraphia, behavioral regress, regress in school outcome, emotional lability, irritability, aggression, oppositional behaviours, dysuric symptoms, insomnia | ND | Higher percentage of Bacteroidaceae, Rikenellaceae, and Odoribacteriaceae lower level of Firmicutes, absence of Turicibacteraceae, Tissierellaceae, Gemellaceae, and Carnobacteriaceae (Bacilli class); Corynebacteriaceae and Lachnospiraceae (Clostridia class); Bifidobacteriaceae (Actinobacteria) and Erysipelotrichaceae [66] | ND | Autoantibodies against: dopamine D1, D2 receptor, tubulin, lysoganglioside, calcium calmodulin dependent kinase II [71] | First-line antibiotics: penicillin, amoxicillin Alternative antibiotics: azithromycin, cefadroxil, cephalexin, cefpodoxime Other: Intravenous immunoglobulin, therapeutic plasma exchange, corticosteroids, SSRIs, non-SSRI-antidepressants, ADHD medication, antipsychotics, anxiolytics, mood-stabilizers, cognitive-behaviour therapy [79,80] |
| Sydenham’s chorea | OCD, tics, ADHD, generalized anxiety, mood disorders, psychotic features, emotional lability, irritability, regressive behaviour, separation anxiety, panic disorder, phobias, social phobia, agoraphobia, executive dysfunction [81] | Permanent basal ganglia damage, dysfunction in the connection between the basal ganglia and the superior colliculi [56] | ND | ND | Autoantibodies against: dopamine receptor D2, anti-basal ganglia antibodies [82] | Penicillin, neuroleptics (risperidone, haloperidol), sodium valproate, corticosteroids, plasma exchange, intravenous immunoglobulins, dopamine depleters (tetrabenazine, deutetrabenazine, valbenazine), dopamine antagonists [83] |
| Tourette’s syndrome | OCD, tics, ADHD, depression, bipolar disorder, anxiety, personality disorder, learning disability, speech and language disorder, intellectual disability, trichotillomania, sleep disorders, pathologic nail-biting, simple phobia, social phobia, agoraphobia, impulse control disorders (intermittent), explosive disorder, self-injurious behavior, impulsive-compulsive sexual behavior [84,85] | Increased functional connectivity between the basal ganglia nuclei (right and left caudate, putamen and left pallidum) and cortex (superior temporal gyrus, medial temporal gyrus, paracingulate gyrus, precuneus, angular gyrus, insular cortex) Increased connectivity between left thalamus and the cortex (right planum temporale, right superior temporal gyrus) [86,87] | ND | CELSR3, FLT3, COL27A1, SLITRK1, SLITRK5, HDC, NRXN1, CNTN6, DRD3, GDNF, KCNJ5, AADAC [88,89] | Antibodies against: rheumatogenic GAS serotypes (M12, M19), anti-neuronal antibodies, antibodies to membrane isoforms of glycolytic enzymes (aldolase C, enolase, pyruvate kinase M1), anti-HCN4 antibodies [90,91,92] | First line: aripiprazole, sulpiride, risperidone Second line: clonidine, guanfacine Third line: topiramate, pimozide, tetrabenazine Fourth line: clonazepam, haloperidol Also: botulinum toxin, SSRIs (sertraline), tricyclics (clomipramine), stimulants (methylphenidate, dextroamphetamin), non-stimulants (atomoxetine, clonidine, guanfacine) Other: behavioural treatments, deep brain stimulation [87] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baj, J.; Sitarz, E.; Forma, A.; Wróblewska, K.; Karakuła-Juchnowicz, H. Alterations in the Nervous System and Gut Microbiota after β-Hemolytic Streptococcus Group A Infection—Characteristics and Diagnostic Criteria of PANDAS Recognition. Int. J. Mol. Sci. 2020, 21, 1476. https://doi.org/10.3390/ijms21041476
Baj J, Sitarz E, Forma A, Wróblewska K, Karakuła-Juchnowicz H. Alterations in the Nervous System and Gut Microbiota after β-Hemolytic Streptococcus Group A Infection—Characteristics and Diagnostic Criteria of PANDAS Recognition. International Journal of Molecular Sciences. 2020; 21(4):1476. https://doi.org/10.3390/ijms21041476
Chicago/Turabian StyleBaj, Jacek, Elżbieta Sitarz, Alicja Forma, Katarzyna Wróblewska, and Hanna Karakuła-Juchnowicz. 2020. "Alterations in the Nervous System and Gut Microbiota after β-Hemolytic Streptococcus Group A Infection—Characteristics and Diagnostic Criteria of PANDAS Recognition" International Journal of Molecular Sciences 21, no. 4: 1476. https://doi.org/10.3390/ijms21041476