Resveratrol-Coated Balloon Catheters in Porcine Coronary and Peripheral Arteries

 ,
,
Abstract
:1. Introduction
2. Results
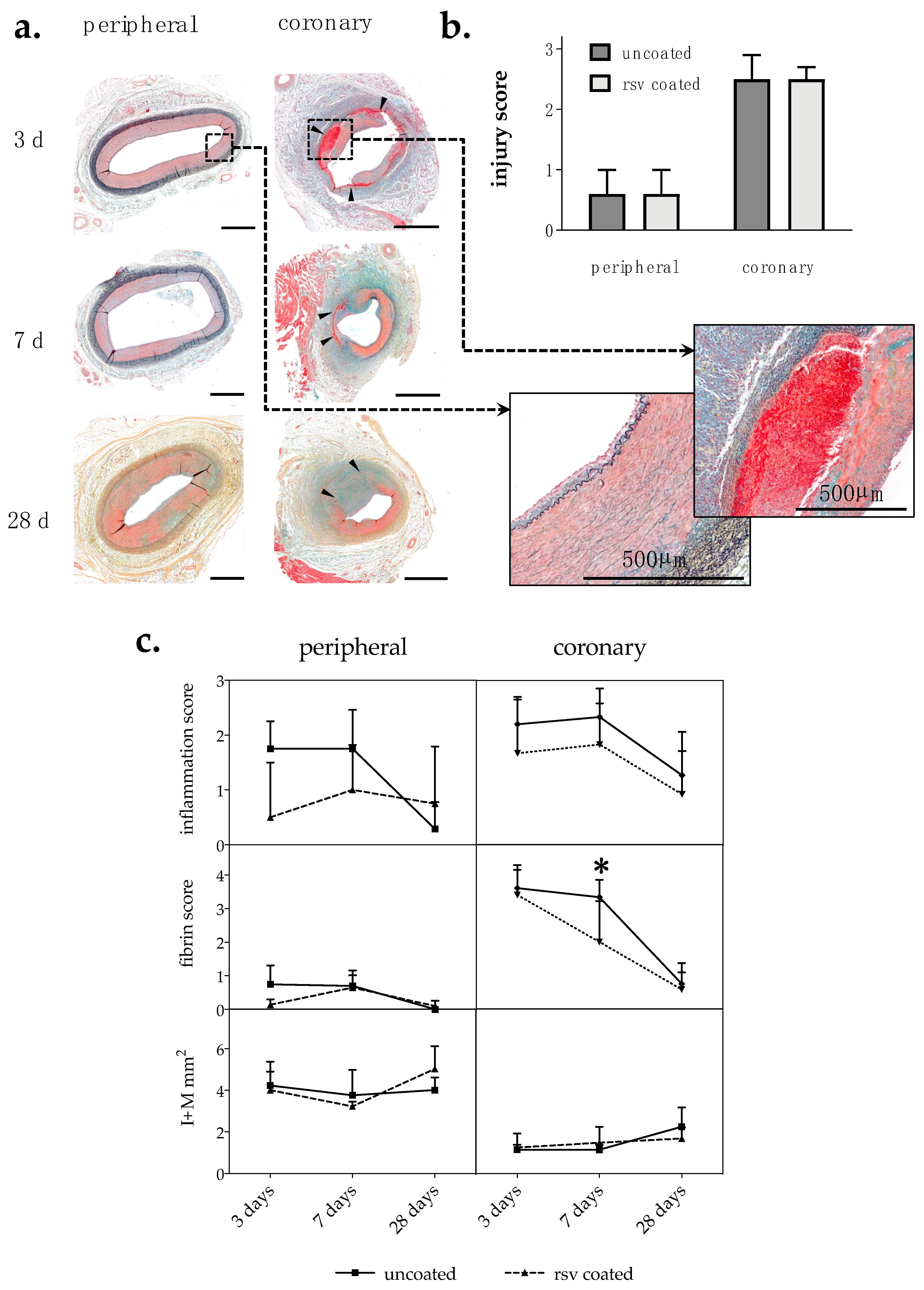
2.1. Histological Analysis
2.1.1. Injury Score and Morphometry
2.1.2. Inflammation Score and Fibrin Score
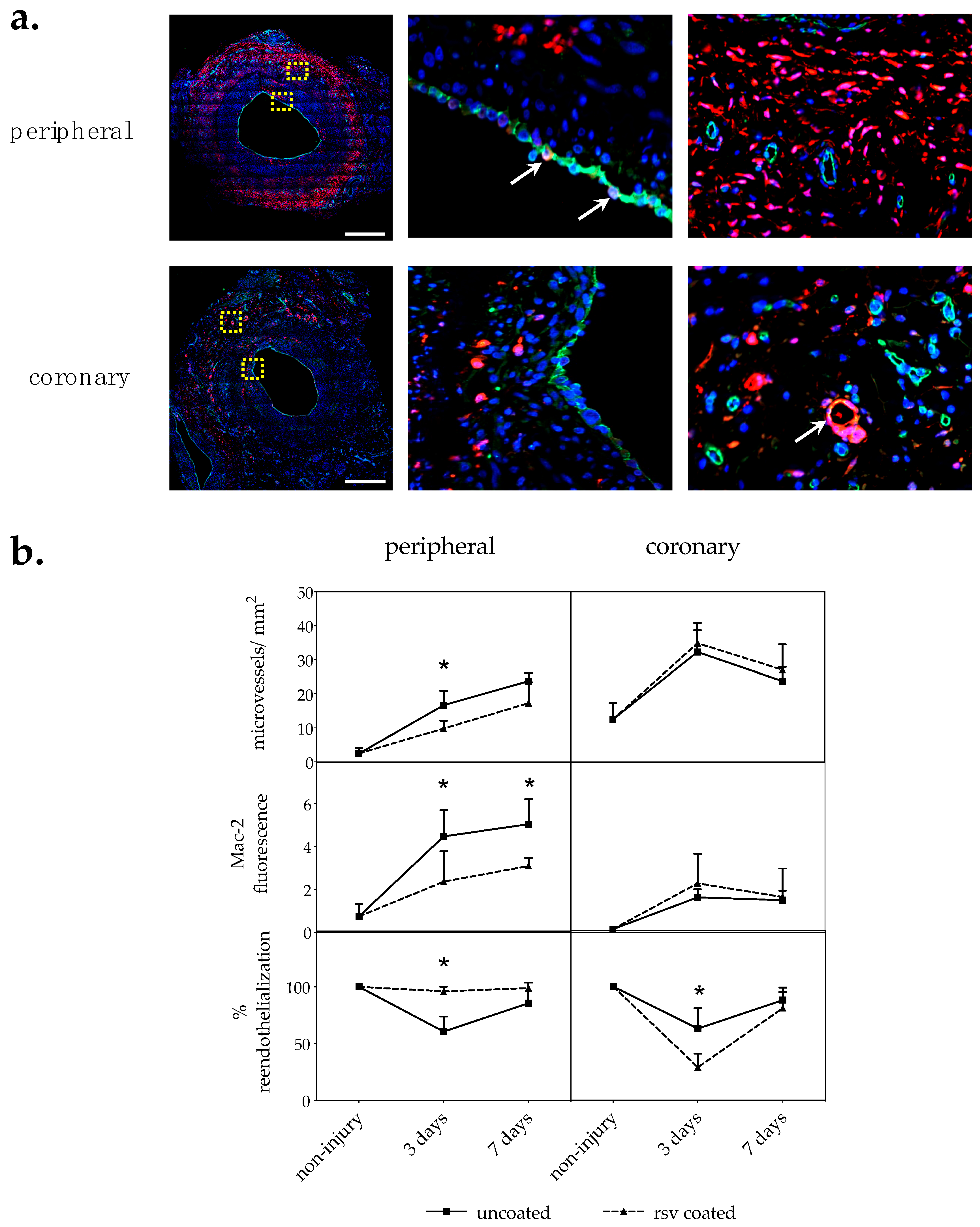
2.2. Immunofluorescent Analyses
2.2.1. Vasa Vasorum Neovascularization
2.2.2. Macrophages
2.2.3. Reendothelialization
3. Discussion
4. Materials and Methods
4.1. Angioplasty Balloon Catheters and Coating Procedure
4.2. Animal Experiments
4.3. Histochemistry and Morphometry
4.4. Immunohistochemistry
4.5. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CD31/PECAM | Cluster of differentiation 31/platelet endothelial cell adhesion molecule |
| DCB | Drug-coated balloon |
| DAPI | 4′,6-diamidino-2-phenylindole |
| EC | Endothelial cell |
| EEL | External elastic lamina |
| IEL | Internal elastic lamina |
| I/M | Intima–media ratio |
| I + M | Intima–media area |
| LAD | Left anterior descending artery |
| LCX | Left circumflex coronary artery |
| Mac-2 | Macrophage marker 2 (galactoside-binding protein of macrophages, also known as Galectin 3) |
| PTX | Paclitaxel |
| p.i. | Post injury |
| RCA | Right coronary artery |
| RSV | Resveratrol |
| VSMC | Vascular smooth muscle cell |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Animals | Survival | Artery Type | Staining Method | Vessels (Uncoated, rsv-Coated) | Section Levels | Sections Per Level | Sections Total |
|---|---|---|---|---|---|---|---|
| 4 | 3 days | peripheral | Movat | 4, 4 | 3 | 1 | 24 |
| Mac-2/CD31 | 4, 4 | 3 | 2 | 48 | |||
| coronary | Movat | 5, 5 | 3 | 1 | 30 | ||
| Mac-2/CD31 | 6, 5 | 3 | 2 | 66 | |||
| 4 | 7 days | peripheral | Movat | 4, 4 | 3 | 1 | 24 |
| Mac-2/CD31 | 4, 4 | 3 | 2 | 48 | |||
| coronary | Movat | 6, 5 | 3 | 1 | 33 | ||
| Mac-2/CD31 | 6, 5 | 3 | 2 | 66 | |||
| 8 | 28 days | peripheral | Movat | 7, 8 | 3 | 1 | 45 |
| coronary | Movat | 11, 12 | 3 | 1 | 69 |

References
- Clever, Y.P.; Cremers, B.; Krauss, B.; Bohm, M.; Speck, U.; Laufs, U.; Scheller, B. Paclitaxel and sirolimus differentially affect growth and motility of endothelial progenitor cells and coronary artery smooth muscle cells. EuroIntervention 2011, 7, K32–K42. [Google Scholar] [CrossRef] [PubMed]
- Iakovou, I.; Schmidt, T.; Bonizzoni, E.; Ge, L.; Sangiorgi, G.M.; Stankovic, G.; Airoldi, F.; Chieffo, A.; Montorfano, M.; Carlino, M.; et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005, 293, 2126–2130. [Google Scholar] [CrossRef]
- McFadden, E.P.; Stabile, E.; Regar, E.; Cheneau, E.; Ong, A.T.; Kinnaird, T.; Suddath, W.O.; Weissman, N.J.; Torguson, R.; Kent, K.M.; et al. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet 2004, 364, 1519–1521. [Google Scholar] [CrossRef]
- Speck, U.; Hackel, A.; Schellenberger, E.; Kamann, S.; Lochel, M.; Clever, Y.P.; Peters, D.; Scheller, B.; Trog, S.; Bettink, S. Drug Distribution and Basic Pharmacology of Paclitaxel/Resveratrol-Coated Balloon Catheters. Cardiovasc. Intervent. Radiol. 2018, 41, 1599–1610. [Google Scholar] [CrossRef]
- Albrecht, T.; Waliszewski, M.; Roca, C.; Redlich, U.; Tautenhahn, J.; Pech, M.; Halloul, Z.; Gogebakan, O.; Meyer, D.R.; Gemeinhardt, I.; et al. Two-Year Clinical Outcomes of the CONSEQUENT Trial: Can Femoropopliteal Lesions be Treated with Sustainable Clinical Results that are Economically Sound? Cardiovasc. Intervent. Radiol. 2018, 41, 1008–1014. [Google Scholar] [CrossRef]
- Tepe, G.; Gogebakan, O.; Redlich, U.; Tautenhahn, J.; Ricke, J.; Halloul, Z.; Meyer, D.R.; Waliszewski, M.; Schnorr, B.; Zeller, T.; et al. Angiographic and Clinical Outcomes After Treatment of Femoro-Popliteal Lesions with a Novel Paclitaxel-Matrix-Coated Balloon Catheter. Cardiovasc. Intervent. Radiol. 2017, 40, 1535–1544. [Google Scholar] [CrossRef]
- Zou, J.; Huang, Y.; Cao, K.; Yang, G.; Yin, H.; Len, J.; Hsieh, T.C.; Wu, J.M. Effect of resveratrol on intimal hyperplasia after endothelial denudation in an experimental rabbit model. Life Sci. 2000, 68, 153–163. [Google Scholar] [CrossRef]
- Yurdagul, A., Jr.; Kleinedler, J.J.; McInnis, M.C.; Khandelwal, A.R.; Spence, A.L.; Orr, A.W.; Dugas, T.R. Resveratrol promotes endothelial cell wound healing under laminar shear stress through an estrogen receptor-alpha-dependent pathway. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H797–H806. [Google Scholar] [CrossRef]
- Breen, D.M.; Dolinsky, V.W.; Zhang, H.; Ghanim, H.; Guo, J.; Mroziewicz, M.; Tsiani, E.L.; Bendeck, M.P.; Dandona, P.; Dyck, J.R.; et al. Resveratrol inhibits neointimal formation after arterial injury through an endothelial nitric oxide synthase-dependent mechanism. Atherosclerosis 2012, 222, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, A.R.; Hebert, V.Y.; Dugas, T.R. Essential role of ER-alpha-dependent NO production in resveratrol-mediated inhibition of restenosis. Am. J. Physiol. Heart Circ. Physiol. 2010, 299, H1451–H1458. [Google Scholar] [CrossRef] [PubMed]
- Kleinedler, J.J.; Foley, J.D.; Orchard, E.A.; Dugas, T.R. Novel nanocomposite stent coating releasing resveratrol and quercetin reduces neointimal hyperplasia and promotes re-endothelialization. J. Control. Release 2012, 159, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Tolva, V.; Mazzola, S.; Zerbi, P.; Casana, R.; Albertini, M.; Calvillo, L.; Selmin, F.; Cilurzo, F. A successful experimental model for intimal hyperplasia prevention using a resveratrol-delivering balloon. J. Vasc. Surg. 2016, 63, 788–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugas, T.R.; Brewer, G.; Longwell, M.; Fradella, T.; Braun, J.; Astete, C.E.; Jennings, M.H.; Sabliov, C.M. Nanoentrapped polyphenol coating for sustained drug release from a balloon catheter. J. Biomed. Mater. Res. B Appl. Biomater 2018. [Google Scholar] [CrossRef]
- Shamseddin, A.; Crauste, C.; Durand, E.; Villeneuve, P.; Dubois, G.; Pavlickova, T.; Durand, T.; Vercauteren, J.; Veas, F. Resveratrol-Linoleate protects from exacerbated endothelial permeability via a drastic inhibition of the MMP-9 activity. Biosci. Rep. 2018, 38. [Google Scholar] [CrossRef]
- Joner, M.; Radke, P.W.; Byrne, R.A.; Hartwig, S.; Steigerwald, K.; Leclerc, G.; Wittchow, E. Preclinical evaluation of a novel drug-eluting balloon in an animal model of in-stent stenosis. J. Biomater Appl. 2013, 27, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Galili, O.; Herrmann, J.; Woodrum, J.; Sattler, K.J.; Lerman, L.O.; Lerman, A. Adventitial vasa vasorum heterogeneity among different vascular beds. J. Vasc. Surg. 2004, 40, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Hildebrandt, H.A.; Gossl, M.; Mannheim, D.; Versari, D.; Herrmann, J.; Spendlove, D.; Bajanowski, T.; Malyar, N.M.; Erbel, R.; Lerman, L.O.; et al. Differential distribution of vasa vasorum in different vascular beds in humans. Atherosclerosis 2008, 199, 47–54. [Google Scholar] [CrossRef]
- Dong, S.; Hughes, R.C. Macrophage surface glycoproteins binding to galectin-3 (Mac-2-antigen). Glycoconj. J. 1997, 14, 267–274. [Google Scholar] [CrossRef]
- Kwon, H.M.; Sangiorgi, G.; Ritman, E.L.; Lerman, A.; McKenna, C.; Virmani, R.; Edwards, W.D.; Holmes, D.R.; Schwartz, R.S. Adventitial vasa vasorum in balloon-injured coronary arteries: visualization and quantitation by a microscopic three-dimensional computed tomography technique. J. Am. Coll. Cardiol. 1998, 32, 2072–2079. [Google Scholar] [CrossRef]
- Ye, M.; Zhang, B.G.; Zhang, L.; Xie, H.; Zhang, H. Quantification of Adventitial Vasa Vasorum Vascularization in Double-injury Restenotic Arteries. Chin. Med. J. 2015, 128, 2090–2096. [Google Scholar] [CrossRef] [PubMed]
- Moulton, K.S.; Vakili, K.; Zurakowski, D.; Soliman, M.; Butterfield, C.; Sylvin, E.; Lo, K.M.; Gillies, S.; Javaherian, K.; Folkman, J. Inhibition of plaque neovascularization reduces macrophage accumulation and progression of advanced atherosclerosis. Proc. Natl. Acad. Sci. USA 2003, 100, 4736–4741. [Google Scholar] [CrossRef] [Green Version]
- Gossl, M.; Herrmann, J.; Tang, H.; Versari, D.; Galili, O.; Mannheim, D.; Rajkumar, S.V.; Lerman, L.O.; Lerman, A. Prevention of vasa vasorum neovascularization attenuates early neointima formation in experimental hypercholesterolemia. Basic Res. Cardiol. 2009, 104, 695–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaabane, C.; Otsuka, F.; Virmani, R.; Bochaton-Piallat, M.L. Biological responses in stented arteries. Cardiovasc. Res. 2013, 99, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wight, T.N.; Potter-Perigo, S. The extracellular matrix: an active or passive player in fibrosis? Am. J. Physiol. Gastrointest Liver Physiol. 2011, 301, G950–G955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, X.; Cheng, C.; Zhong, J.; Liu, B.; Luo, C.; Ou, W.; Mo, P.; Huang, Q.; Liu, S. Resveratrol inhibits angiotensin IIinduced proliferation of A7r5 cells and decreases neointimal hyperplasia by inhibiting the CaMKIIHDAC4 signaling pathway. Mol. Med. Rep. 2018, 18, 1007–1014. [Google Scholar] [CrossRef]
- Patel, K.R.; Andreadi, C.; Britton, R.G.; Horner-Glister, E.; Karmokar, A.; Sale, S.; Brown, V.A.; Brenner, D.E.; Singh, R.; Steward, W.P.; et al. Sulfate metabolites provide an intracellular pool for resveratrol generation and induce autophagy with senescence. Sci. Transl. Med. 2013, 5, 205ra133. [Google Scholar] [CrossRef]
- Gertz, M.; Nguyen, G.T.; Fischer, F.; Suenkel, B.; Schlicker, C.; Franzel, B.; Tomaschewski, J.; Aladini, F.; Becker, C.; Wolters, D.; et al. A molecular mechanism for direct sirtuin activation by resveratrol. PLoS ONE 2012, 7, e49761. [Google Scholar] [CrossRef]
- Kelsch, B.; Scheller, B.; Biedermann, M.; Clever, Y.P.; Schaffner, S.; Mahnkopf, D.; Speck, U.; Cremers, B. Dose response to Paclitaxel-coated balloon catheters in the porcine coronary overstretch and stent implantation model. Invest. Radiol. 2011, 46, 255–263. [Google Scholar] [CrossRef]
- Schwartz, R.S.; Huber, K.C.; Murphy, J.G.; Edwards, W.D.; Camrud, A.R.; Vlietstra, R.E.; Holmes, D.R. Restenosis and the proportional neointimal response to coronary artery injury: results in a porcine model. J. Am. Coll. Cardiol. 1992, 19, 267–274. [Google Scholar] [CrossRef]
- Kornowski, R.; Hong, M.K.; Tio, F.O.; Bramwell, O.; Wu, H.; Leon, M.B. In-stent restenosis: contributions of inflammatory responses and arterial injury to neointimal hyperplasia. J. Am. Coll. Cardiol. 1998, 31, 224–230. [Google Scholar] [CrossRef]


| Survival | Analysis Parameter | Peripheral | p-Value | Coronary 1 | p-Value | ||
|---|---|---|---|---|---|---|---|
| Uncoated | rsv-Coated | Uncoated | rsv-Coated | ||||
| 3 days | n-value | 4 | 4 | 6 | 5 | ||
| Injury score | 1.00 ± 1.41 | 0.00 ± 0.00 | 3.00 ± 0.00 | 2.60 ± 0.55 | |||
| Inflammation score | 1.75 ± 0.50 | 0.50 ± 1.00 | 0.143 | 2.20 ± 0.45 | 1.67 ± 1.03 | 0.515 | |
| Fibrin score | 2.00 ± 0.82 | 0.75 ± 0.50 | 0.114 | 3.60 ± 0.55 | 3.40 ± 0.89 | 0.999 | |
| I + M (mm2) | 4.23 ± 1.15 | 4.01 ± 0.89 | 0.999 | 1.15 ± 0.23 | 1.25 ± 0.67 | 0.999 | |
| Macrophages | 4.47 ± 1.22 | 2.36 ± 1.42 | 0.013 * | 1.62 ± 0.38 | 2.28 ± 1.38 | 0.400 | |
| % Reendothelialization | 61 ± 13 | 96 ± 4 | 0.029 * | 63 ± 18 | 29 ± 12 | 0.019 * | |
| Neovascularization | 16.67 ± 4.21 | 9.82 ± 2.28 | 0.029 * | 38.79 ± 7.73 | 41.92 ± 7.14 | 0.792 | |
| 7 days | n-value | 4 | 4 | 6 | 5 | ||
| Injury score | 1.00 ± 1.41 | 0.25 ± 0.50 | 3.00 ± 0.00 | 2.20 ± 1.30 | |||
| Inflammation score | 1.75 ± 0.71 | 1.00 ± 0.82 | 0.486 | 2.33 ± 0.52 | 1.83 ± 0.75 | 0.394 | |
| Fibrin score | 1.50 ± 1.00 | 1.50 ± 0.58 | 0.999 | 3.33 ± 0.52 | 2.00 ± 1.22 | 0.033 * | |
| I + M (mm2) | 3.76 ± 1.22 | 3.23 ± 0.22 | 0.343 | 1.14 ± 0.23 | 1.48 ± 0.76 | 0.792 | |
| Macrophages | 5.04 ± 1.17 | 3.09 ± 0.38 | 0.029 * | 1.49 ± 0.44 | 1.64 ± 1.33 | 0.931 | |
| % Reendothelialization | 86 ± 18 | 99 ± 1 | 0.114 | 88 ± 7 | 81 ± 18 | 0.879 | |
| Neovascularization | 23.77 ± 2.38 | 17.33 ± 6.12 | 0.114 | 28.51 ± 4.99 | 32.52 ± 9.02 | 0.537 | |
| 28 days | n-value | 7 | 7 | 12 | 12 | ||
| Injury score | 0.14 ± 0.38 | 1.00 ± 1.31 | 2.08 ± 0.90 | 2.50 ± 0.52 | |||
| Inflammation score | 0.29 ± 0.49 | 0.75 ± 1.04 | 0.511 | 1.27 ± 0.79 | 0.92 ± 0.79 | 0.214 | |
| Fibrin score | 0.00 ± 0.00 | 0.50 ± 0.76 | 0.200 | 0.75 ± 0.62 | 0.58 ± 0.51 | 0.720 | |
| I + M (mm2) | 4.01 ± 0.61 | 5.03 ± 1.09 | 0.073 | 2.25 ± 0.92 | 1.68 ± 0.53 | 0.151 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamann, S.; Haase, T.; Stolzenburg, N.; Löchel, M.; Peters, D.; Schnorr, J. Resveratrol-Coated Balloon Catheters in Porcine Coronary and Peripheral Arteries. Int. J. Mol. Sci. 2019, 20, 2285. https://doi.org/10.3390/ijms20092285
Kamann S, Haase T, Stolzenburg N, Löchel M, Peters D, Schnorr J. Resveratrol-Coated Balloon Catheters in Porcine Coronary and Peripheral Arteries. International Journal of Molecular Sciences. 2019; 20(9):2285. https://doi.org/10.3390/ijms20092285
Chicago/Turabian StyleKamann, Stefanie, Tobias Haase, Nicola Stolzenburg, Melanie Löchel, Daniel Peters, and Jörg Schnorr. 2019. "Resveratrol-Coated Balloon Catheters in Porcine Coronary and Peripheral Arteries" International Journal of Molecular Sciences 20, no. 9: 2285. https://doi.org/10.3390/ijms20092285