
Herbal Medicine in Mexico: A Cause of Hepatotoxicity. A Critical Review

Abstract
:1. Introduction
2. History
3. Epidemiology and Geographic Distribution in Mexico

4. Herb-Induced Liver Injury Overview
4.1. General Aspects
4.2. Classification
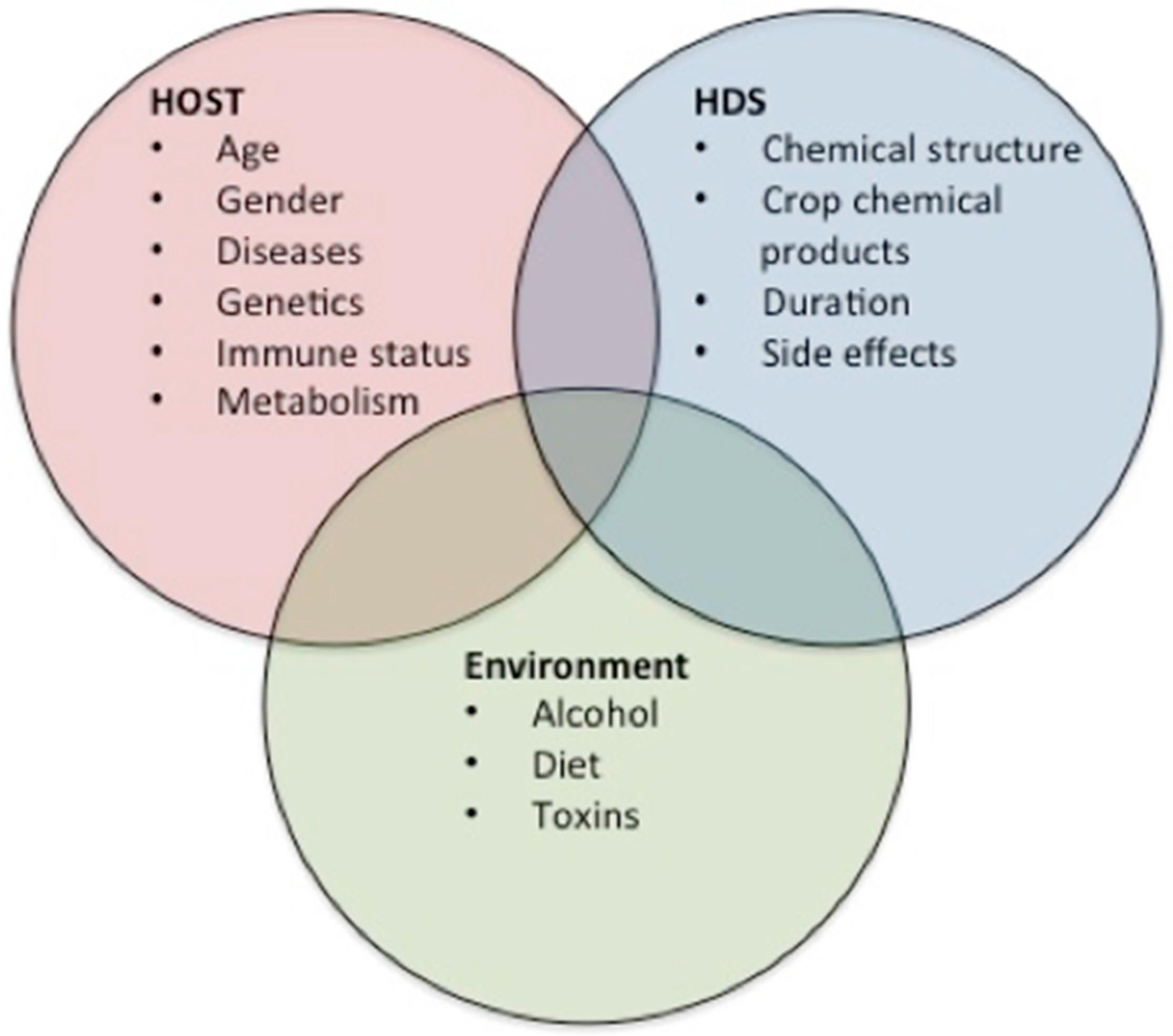
4.3. Risk Factors
4.4. Clinical Course
4.5. Pathogenic Aspects of HILI

5. Traditional Herbal Products Used in Mexico

{kind=link}
{kind=link}
| Medical Plant | Popular Names | Cultural Uses | Active Components | Side Effects |
|---|---|---|---|---|
| Scoparia dulcis L. (Maidenhair) [4] | Anisillo, candejilla, epazote bush, epazote sea grass blow, lentejilla; Michoacan: mishishe (Nahua); Nayarit: golpesal (Heart); Oaxaca: nax podeey (Mixe). | Diarrhea and stomach pain, toothache | Flavonoids apigenin, deflavona hexahydroxy -glucuronide, himenoxín, linarín, luteolin, glycoside; saponaretín, escutelarín, methyl ester, vitexin vicenín; dulcinol diterpenes, escopaduline acids A and B, escopaduline, escopariol; α-amyrin triterpenes, betulinic acid, dulcioico, friedelin | Hepatotoxicity |
| Citrus aurantium L. (Citrus orange) [4] | Orange, orange leaves, lemon, monument, orange, sour orange, sour orange, orange doghouse, orange Castile, cucho orange, orange, sour orange, bitter orange. Morelos: naranjaxocotl; Oaxaca: cajel, ma ji gui ruu, suuikh, tsuiky; Puebla: chichicarajas (Nahua), ixcapehto (Otomi), skeja Lasus (Totonac), Skaja laxux, xocot; Quintana Roo: cituhuk, pakal dzut, suut’spak‘aal (Maya); Veracruz: tsotso; San Luis Potosi; tdimalon lanash, kaxiy lanash (tenek) | Dysentery, stomach pain, abortion, asthma, colds, fever | Monoterpenes camphene, geraniol, limonene and linalool; methyl anthranilate and Citra, flavonoids, Rhamno-glycosides hesperidin, hesperidin glycosides, phenols; the sterols campesterol and β-sitosterol and carotenoid α-tocophero | Hepatotoxicity Teratogenicity |
| Prunus persica L. (Peach) [4] | San Luis Potosí: tulasnu (tenek) | Antiparasitic, dysentery, stomach pain | Epigalato of catechin, the diglucosides of kaempferol and quercetin, and the sterol β-sitosterol | Hepatotoxicity |
| Rosmarinus officinalis L. (Rosemary) [4,23] | Michoacan: romeru | Stomach pain, biliary colic, cold | 1,8-cineol monoterpenes, bornyl acetate, camphor, α- and β-pinene, α-terpineol, nerol, geraniol, eugenol, nerolidol, slime-Neno, verbenol, myrcene | Hepatotoxicity |
| Equisetum hyemale L. (Horse tail) [4,23] | Carricillo. Estado de México: carrizo (mazahua); Michoacán: k uture (purhépecha); Sonora: cab’ bager (pima) | Abdominal pain, urinary tract infections | Carotenoids α- and β-carotene, lutein epoxide, licofíl, violaxantín and zeaxanthin | Hepatotoxicity |
| Tilia mexicana Schlechtendal (Tilia) [4] | Flordetila, flordetilia, tilia; Michoacán: sirimo (purhépecha), cirimo | Calm the nerves, menstrual pain | p-Coumaric acid, kaempferol, quercetin and terpenoid Constituents. Volatile oils, Including citral, citronellal, citronellol, eugenol, and limonene | Hepatotoxicity |
| Morus alba L. (White Mulberry) [4,23] | Moral, mora blanca, mora de tierra caliente, moran, moran hembra; Puebla: kimucucuk kiui (totonaco) | Muscle pain, respiratory diseases | Monoterpene geraniol limonene, linalool, acetate and α-pinene | Hepatotoxicity |
| Opuntia ficusindica (Nopal) [15,24] | Nopal, Cactus | Diabetes and others | Fibrous polysaccharide (fiber) and pectin | Diarrhea, nausea, abdominal fullness and headache |
| Mentha piperita (Peppermint) [15,24] | Mint | Gastrointestinal tract ailments and others | Acetaldehyde, amyl alcohol, menthyl esters, limone, pinene, phellandrene, cadinene, pugelone, and dimethyl sulfide, α-pinene, sabinene, terpinolene, ocimene, γ-terpinene, fenchene, α- and β-thujone, citronellol | Hepatotoxicity |
| Larrea divaricate (Chaparral) [15,25] | Governor, Creosote Bush, Greasewood, Hediondilla, Larreastat | Arthritis and others | Nordihydroguaiaretic acid | Hepatotoxicity |
| Taraxacum officinale (Dandelion) [15,24] | Blowball dandelion, cankerwort, Common Dandelion, Dudal, Herba Taraxaci, Lion‘s Tooth | Hepatic and biliary ailments, viral and bacterial infections, cancer and others | Quercetin, luteolin, luteolin-7-O-gluccoside, p-hydroxyphenylacetic acid, germacranolide acids, chlorogenic acid, chicoric acid, and monocaffeyltartaric acid, scopoletin, aesculetin, aesculin, cichoriin, arnidiol, and faradiol, caffeic acid, taraxacoside, taraxasterol, inulin and high potassium content | Allergic reactions, palpitations, syncope and erythema multiform |
| Verbascum densiflorum (Mullein) [15,24] | Mullein, Aaron's Rod, Adam's Flannel, American Mullein, Orange Mullein, Rag Paper | Inflammatory ailments in respiratory tract and others | Harpagoside, harpagide, aucubin, hesperidin, verbascoside, saponins, and volatile oils | None reported |
| Matricaria recutita (Chamomile) [15,24] | Chamomile, Blue Chamomile, Camomilla, Camomille Allemande, Cham, Echte Kamille, Fleur de Camomile | Gastrointestinal tract ailments and others | Quercetin, apigenin, and coumarins, and the essential oils matricin, chamazulene, α bisaboloid, and bisaboloid oxides | Allergic reactions and conjunctivitis |
| Passiflora incarnate (Passion flower) [15,24] | Crown of Christ, Passion Flower, Madre Selva, Passionflower, Passiflore, passiflorine, Passionaria | Insomnia, and anxiety or nervousness | Flavonoids apigenin, luteolin, quercetin, kaempferol, and vitexin, harmine, harmaline, harmalol, harman, and harmin. Other constituents include maltol and ethyl maltol | Dizziness, confusion and ataxia; Vasculitis; nausea, vomiting, drowsiness, tachycardia; hepatic and pancreatic toxicity |
| Aloe vera (Aloe) [15,24] | Zabila, Aloe Vera, Aloe Latex, Aloe Perfoliata, Burn Plant, Elephant‘s Gall, Gvarapatha, Gvar Patha, Indian Aloe, and others | Gastrointestinal ailments, wound healing and others | Emodin anthrone, dithranol, chrysarobin, carboxypeptidase, magnesium lactate, C-glucosyl chromone, salicylate and allantoin. Aloe latex belongs to the anthraquinone family and contains a tricyclic anthracene nucleus | Decrease platelet aggregation; Prolong bleeding time; Diarrhea and loss of water and electrolytes |
6. Regulation of Herbal Products and Social Implications
7. Conclusions and Future Challenges
Conflicts of Interest
References
- Rousseaux, C.G.; Schachter, H. Regulatory issues concerning the safety, efficacy and quality of herbal remedies. Birth Defects Res. 2003, 68, 505–501. [Google Scholar]
- Korth, C. Drug-induced hepatotoxicity of select herbal therapies. J. Pharm. Pract. 2014, 27, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Teschke, R.; Eickhoff, A. Herbal hepatotoxicity in traditional and modern medicine: Actual key issues and new encouraging steps. Front. Pharmacol. 2015, 6, 2–40. [Google Scholar] [CrossRef] [PubMed]
- Biblioteca Digital de la medicina tradicional Mexicana (Digital Library of Mexican Traditional Medicine). 2009. Available online: http://www.medicinatradicionalmexicana.unam.mx/presenta.html (accessed on 12 January 2015).
- Aguilar, A.; Camacho, J.R.; Chino, S.; Jáquez, P.; López, M.E. Herbal medicinal Mexican Social Security Institute. Mexican Social Security Institute (MSSI). Available online: http://www.medicinatradicionalmexicana.unam.mx/presenta.html (accessed on 12 January 2015).
- Muñetón-Pérez, P. Plantas Medicinales: Un Complemento Vital Para la Salud de los Mexicanos (Medicinal Plants: A Vital Complement to the Health of Mexicans). Available online: http://www.revista.unam.mx/vol.10/num9/art58/int58.htm (accessed on 12 January 2015).
- Raschi, E.; de Ponti, F. Drug- and herb-induced liver injury: Progress, current challenges and emerging signals of postmarketing risk. World J. Hepatol. 2015, 7, 1761–1771. [Google Scholar] [CrossRef] [PubMed]
- Estrada-Castillón, E.; Soto-Mata, B.E.; Garza-López, M.; Villarreal-Quintanilla, J.Á.; Jiménez-Pérez, J.; Pando-Moreno, M.; Sánchez-Salas, J.; Scott-Morales, L.; Cotera-Correa, M. Medicinal plants in the southern region of the State of Nuevo León, México. J. Ethnobiol. Ethonomed. 2012, 8, 1–13. [Google Scholar]
- Giovannini, P.; Heinrich, M. Xki yoma´ (our medicine) and xki tienda (patent medicine)—Interface between traditional and modern medicine among the Mazatecs of Oaxaca, Mexico. J. Ethnopharmacol. 2009, 3, 383–399. [Google Scholar] [CrossRef] [PubMed]
- Frei, B.; Baltisberger, M.; Sticher, O.; Heinrich, M. Medical ethnobotany of the Zapotecs of the Isthmus-Sierra (Oaxaca-Mexico): Documentation and assessment of indigenous uses. J. Ethnopharmacol. 1998, 2, 149–165. [Google Scholar] [CrossRef]
- Ankli, A.; Heinrich, M.; Bork, P.; Wolfram, L.; Bauerfeind, P.; Brun, R.; Schmid, C.; Weiss, C.; Bruggisser, R.; Gertsch, J.; et al. Yucatec Mayan medicinal plants: Evaluation based on indigenous uses. J. Ethnopharmacol. 2002, 1, 43–52. [Google Scholar] [CrossRef]
- Maddukuri, V.C.; Bonkovsky, H.L. Herbal and dietary supplement hepatotoxicity. Clin. Liver Dis. 2014, 1, 1–3. [Google Scholar] [CrossRef]
- Chitturi, S.; Farrell, G.C. Herbal hepatotoxicity: An expanding but poorly defined problem. J. Gastroenterol. Hepatol. 2000, 15, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Stournaras, E.; Tziomalos, K. Herbal medicine-related hepatotoxicity. World J. Hepatol. 2015, 7, 2189–2193. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Fragoso, L.; Reyes-Esparza, J.; Burchiel, S.; Herrera-Ruiz, D. Risks and benefits of commonly used herbal medicines in México. Toxicol. Appl. Pharmacol. 2008, 227, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Navarro, V.J.; Barnhart, H.; Bonkovsky, H.L. Liver injury from herbals and dietary supplements in the U.S. Drug-Induced Liver Injury Network. Hepatology 2014, 60, 1399–1408. [Google Scholar] [CrossRef] [PubMed]
- Schiano, T.D. Hepatotoxicity and complementary and alternative medicines. Clin. Liver Dis. 2003, 7, 453–473. [Google Scholar] [CrossRef]
- Chalasani, N.; Fontana, R.J.; Bonkovsky, H.L. Causes, clinical features, and outcomes from a prospective study of drug-induced liver injury in the United States. Gastroenterology 2008, 135, 1924–1934. [Google Scholar] [CrossRef] [PubMed]
- Suk, K.T.; Kim, D.J.; Kim, C.H. A prospective nationwide study of drug-induced liver injury in Korea. Am. J. Gastroenterol. 2012, 107, 1380–1387. [Google Scholar] [CrossRef] [PubMed]
- Zheng, E.X.; Navarro, V.J. Liver injury from herbal, dietary, and weight loss supplements: A review. J. Clin. Transl. Hepatol. 2015, 3, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Davern, T.J.; Chalasani, N.; Fontana, R.J.; Hayashi, P.H.; Protiva, P.; Kleiner, D.E. Acute hepatitis E infection accounts for some cases of suspected drug-induced liver injury. Gastroenterology 2011, 141, 1665–1672. [Google Scholar] [CrossRef] [PubMed]
- Fontana, R.J. Pathogenesis of idiosyncratic drug-induced liver injury and clinical perspectives. Gastroenterology 2014, 146, 914–928. [Google Scholar] [CrossRef] [PubMed]
- Bunchorntavakul, C.; Reddy, K.R. Review article: Herbal and dietary supplement hepatotoxicity. Aliment. Pharmacol. Ther. 2013, 37, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Calitz, C.; Du Plessis, L.; Gouws, C. Herbal hepatotoxicity: Current status, examples, and challenges. Expert Opin. Drug Metab. Toxicol. 2015, 11, 1551–1565. [Google Scholar] [CrossRef] [PubMed]
- Grant, K.L. Chaparral-induced hepatotoxicity. Int. Med. 1998, 1, 83–87. [Google Scholar] [CrossRef]
- Carillo Esper, R.; Lara Caldera, B.; Ruiz Morales, J.M. Hierbas, medicina herbolaria y su impacto en la práctica clínica (Herbs, herbal medicine and its impacto n clinical practice). Rev. Investig. Med. Sur Mex. 2010, 3, 124–130. [Google Scholar]
- NORMA Oficial Mexicana NOM-072-SSA1–2012, Etiquetado de Medicamentos y de Remedios Herbolarios. Available online: http://www.dof.gob.mx/nota_detalle.php?codigo=5278341&fecha=21/11/2012 (accessed on 12 January 2015).
- Taddei-Bringas, G.A.; Santillana-Macedo, M.A.; Romero-Cancio, J.A.; Romero-Tellez, M.B. Aceptación y uso de la Herbolaria en Medicina Familiar (Acceptance and Use of Herbs in Family Medicine). Salud Pública en México 1999, 41, 216–220. [Google Scholar] [CrossRef]
- Hopkins, A.; Stepp, J.R. Distribution of herbal remedy knowledge in Tabi, Yucatan, Mexico. Econ. Bot. 2012, 66, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Coffman, M.J.; Shobe, M.A. Self-prescription practices in recent Latino immigrants. Public Health Nurs. 2008, 3, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.; Pena, A. Pharmacists’ actions when patients use complementary and alternative medicine with medications: A look at Texas—Mexico border cities. J. Am. Pharm. Assoc. 2003, 51, 619–622. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdivia-Correa, B.; Gómez-Gutiérrez, C.; Uribe, M.; Méndez-Sánchez, N. Herbal Medicine in Mexico: A Cause of Hepatotoxicity. A Critical Review. Int. J. Mol. Sci. 2016, 17, 235. https://doi.org/10.3390/ijms17020235
Valdivia-Correa B, Gómez-Gutiérrez C, Uribe M, Méndez-Sánchez N. Herbal Medicine in Mexico: A Cause of Hepatotoxicity. A Critical Review. International Journal of Molecular Sciences. 2016; 17(2):235. https://doi.org/10.3390/ijms17020235
Chicago/Turabian StyleValdivia-Correa, Bárbara, Cristina Gómez-Gutiérrez, Misael Uribe, and Nahum Méndez-Sánchez. 2016. "Herbal Medicine in Mexico: A Cause of Hepatotoxicity. A Critical Review" International Journal of Molecular Sciences 17, no. 2: 235. https://doi.org/10.3390/ijms17020235