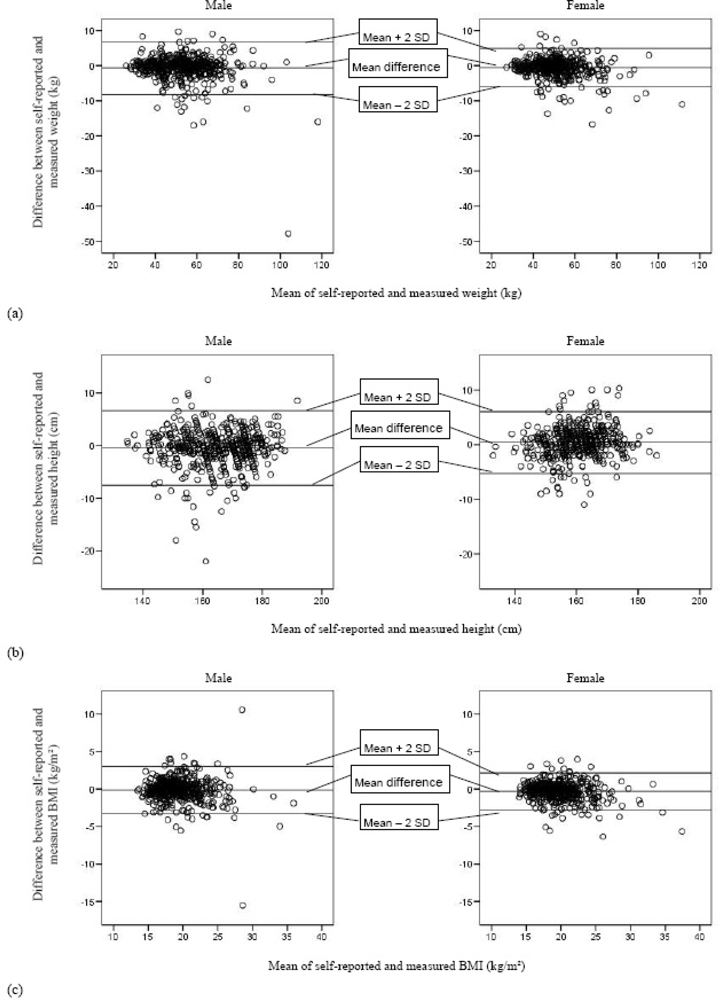
This study showed that the self-reported height and weight of adolescents cannot replace the measured values for determining their BMI-category and thus measured weight and weight are highly recommended for the diagnosis of underweight, overweight and obesity. However, the adolescents as a group were actually quite capable of reporting their height and weight, despite the fact that their body undergoes large physical changes during the adolescent period of life. Although statistically significant differences arose between self-reported and measured weight, height and BMI (the latter only for girls) of the adolescents on group level, the magnitudes of these differences were trivial, given the low values for the effect size indices (Cohen’s d). However, B&A plots showed that these differences at individual level can be quite large, which indicated limited usefulness of the self-reported values on an individual level and for investigating the association with other health-related parameters. For height, the magnitude of the differences tended to slightly increase with increasing mean height, given the slightly divergent patterns in the B&A plots. This is also the case for BMI in boys, whereas in girls this divergent pattern is less present. Both boys and girls slightly, but significantly, underestimated their weight. This is in agreement with the findings of previous surveys [
9–
11,
14]. However, other studies found that boys underestimated their weight to a lesser extent than girls did [
6,
7,
12,
13]. Elgar
et al. and Abalkhail
et al. reported only a significant underestimation of weight for girls [
8,
15]. The present study confirmed previous studies [
7,
9,
11,
13–
15] with the finding that adolescent girls significantly overestimated their height, while only Strauss
et al. [
6] found a significant underestimation of height by girls. Adolescent boys in the present study significantly underestimated their height, which was reported previously by Strauss
et al. [
6], but in conflict with the previously reported overestimation in boys [
7,
11,
13,
14]. Other surveys found no significant over- or underestimation of height for both genders [
8,
10,
12]. The present study showed only for girls a significant underestimation of BMI. This could be declared by the opposite biases in height (overestimation) and weight (underestimation) in girls. This effect is not seen in boys, where the biases are in the same direction (weight and height underestimated). Goodman
et al. also reported an underestimation of BMI in girls, but they found a minor overestimation of BMI for boys [
12]. Other surveys found for both genders an underestimation of BMI [
7–
11,
13,
17]. Correlations between self-reported and measured anthropometrics in the present study were rather high and comparable with results from previous studies [
9–
12], but slightly higher than those from others [
6–
8,
13,
16]. However, as mentioned before, the correlation coefficient is not an ideal measure for agreement, since systematic over- or underreports cannot be taken into account. A high correlation does not automatically imply a good agreement between two measurements.
When using the adolescents’ self-reported anthropometrics for classification in BMI-categories according to the national and international cut-off points, respectively 86.5% and 84.1% of the adolescents were correctly classified in the present study. Some misclassification errors occurred, in general leading to a statistically significant underestimation of the prevalence of overweight and obesity (only according to the international criteria), as also reported by Elgar
et al. [
8] and Tokmakidis
et al. [
11], and overestimation of the prevalence of underweight, the latter only being found by Danubio and colleagues in young adult girls (18–35 years) [
17]. The relative magnitudes of these under- (15.5% for overweight and 41% for obesity) and overestimations (24.7% for underweight) are indicative of a substantial significance on clinical or public health level. The conclusions for overweight are in line with those made by Sherry and colleagues, who made a literature review on this topic of studies performed in the United States [
31]. The overestimation of underweight in adolescents in the present study is, to our knowledge, new information. Weighted κ-values (≥0.63) illustrated a good statistical agreement between the self-reported and measured BMI-categories for both national and international cut-offs. However, the sensitivity and specificity values and PVs of self-reported anthropometrics for predicting underweight, overweight and obesity questioned the diagnostic value of self-reported anthropometrics to identify actual underweight, overweight and obesity in epidemiological surveys. Previous studies reported similar values for sensitivity and specificity as in the present study [
8,
12,
15]. However, direct comparison is not always feasible since other cut-off criteria for the BMI-categories were implemented. In general, classification according to the national criteria resulted in higher sensitivity and specificity values, indicative for a better classification. A possible explanation for this finding could be the higher agreement between the study sample and the population on which the national cut-off criteria are based on. When comparing the classification of adolescents in BMI categories based on their self-reported and measured BMI, at least 25% of the adolescents who should be targeted for nutritional advice on base of their actual overweight/obese status would be missed for intervention purposes when using self-reported weight and height values. Conversely, about half of the adolescents being classified as underweight when using self-reported data could be wrongly encouraged to gain weight. From those results one can conclude that an important number of adolescents within the target group would be missed for interventions, while almost half of the adolescents who would get an intervention for gaining weight won’t need this intervention. Therefore, self-reported weight and height should not be used when aiming at classifying adolescents for intervention purposes.
The present study demonstrated that boys and the adolescents with a higher educational level had a higher accuracy of their self-reported BMI, compared to girls and those with a lower educational level respectively. This gender difference again illustrates the strengthening effect of opposite biases in weight and height for girls, as mentioned above, resulting in a lower accuracy of self-reported BMI. The finding that girls underestimated their weight and overestimated their height could be explained by the fact that they want to meet the social desirability to be thin and tall, but further investigation is needed to confirm this assumption. The difference across educational levels is somewhat more complex and possible explanations could be the lack of interest or the lower capability to estimate their height in the adolescents from a lower educational level. Further research is necessary to investigate these assumptions. The accuracy of the self-reported weight was only positively influenced by actual weighing during the last year and not by educational level nor gender. Elgar
et al. also did not find an influence of gender on the accuracy of self-reported weight, but they found that self-perceptions of body size predicted bias in self-reported weight [
8]. This could not be investigated in the present study. The effect of weighing behaviour on the accuracy of self-reported weight should be considered when planning self-reported anthropometric assessments in future surveys where measuring height and weight of adolescents is not feasible. One could give the guideline to the adolescents weigh themselves at home before completing the survey in order to obtain a more accurate self-reported weight. However, to our knowledge, little is known about the guideline compliance of adolescents in this context. The lack of good-quality equipment at home could also give a wrong indication of their weight. Future research should investigate the effect of above-mentioned guideline and the influence of measurement conditions at home on the accuracy self-reporting.




{kind=link}