
Prevention of Poor Physical and Mental Health through the Green Social Prescribing Opening Doors to the Outdoors Programme: A Social Return on Investment Analysis
 , , ,
, , ,  and
and
Abstract
:1. Introduction
1.1. Background
1.2. The Outdoor Partnership Programme
1.2.1. Walking Groups
1.2.2. Climbing Groups
2. Methods
2.1. Social Return on Investment Methodology
2.2. Identifying Stakeholders
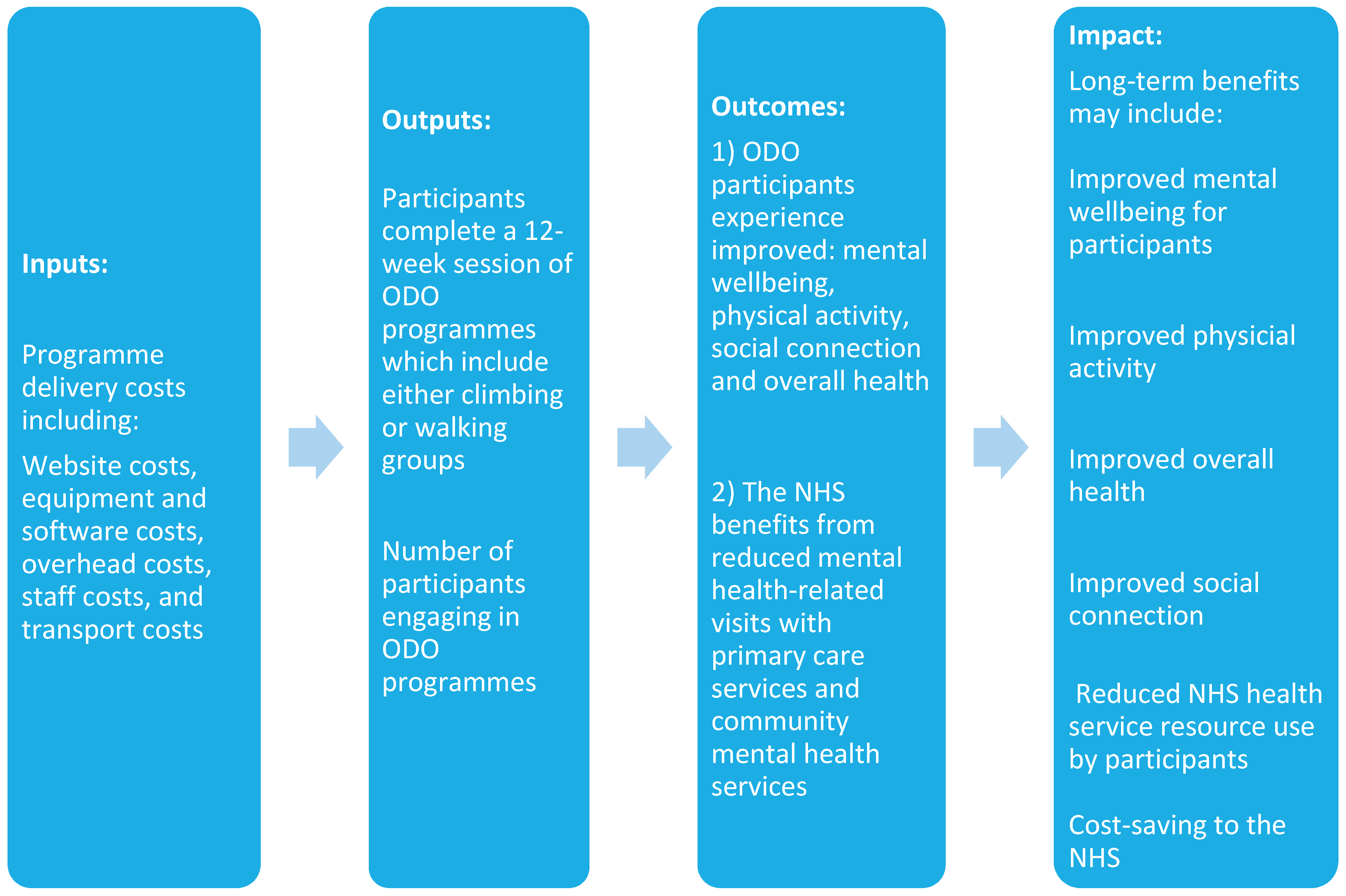
2.3. Developing a Theory of Change
2.4. Calculating Inputs
2.4.1. Website Costs
2.4.2. Equipment and Software Costs
2.4.3. Overhead Costs
2.4.4. Staff Costs
2.4.5. ODO Programme Session Costs
2.4.6. Transport Costs
2.5. Evidencing and Valuing Outcomes
2.5.1. Questionnaires
- Short Warwick–Edinburgh Mental Wellbeing Scale (SWEMWBS)
- 2.
- The New Economics Foundation Social Trust Question NEF Social Trust Question
- 3.
- Overall health question
- 4.
- The International Physical Activity Questionnaire—Short Form (IPAQ—SF)
2.5.2. Client Service Receipt Inventory (CSRI)
2.5.3. Interviews
2.5.4. Wellbeing Valuation Using the Social Value Calculator
2.5.5. Wellbeing Valuation Using the Mental Health Social Value Calculator
Applying Mental Health Social Value Calculator
2.6. Establishing Impact
2.7. Calculating the SROI Ratio
3. Results
- 96% were aged 18 to 64
- 64% were male, 34% women and 2% transgender
- 94% were white British, 4% mixed ethnicity and 2% Asian
3.1. Costs
3.2. Outcomes Using the Social Value Calculator
- To examine the value of good overall health, among participants’ values pre and post evaluations were calculated for improved overall health. The SVB value was estimated for improvements in good overall health at £20,141 per person per year, which was indicated by an improvement of 50% or more, based on pre and post questionnaires.
- To understand the value connected with improvements in Physical Activity among ODO participants, the SVB value estimate indicated an increased value associated with increased physical activity and is estimated at £5281 per person per year, which was the value assigned to a 60-min change per week in regular walking. All value estimates for improvements are outlined in Table 4.

{kind=link}
{kind=link}
{kind=link}
| Outcomes | Indicators | Quantity Improved | Financial Value | Total Social Value for Participants | Social Value per Participant |
|---|---|---|---|---|---|
| Social trust | NEF social trust question | 27/47 reported an increase of 10% or more | £3753 per year for feeling a sense of belonging to neighbourhood | £101,331 | £2156 (n = 47) |
| Good overall health | Overall health question | 19/35 reported an improvement of 50% or more | £20,141 per person per year for significant improvement in good overall health | £382,679 | £10,934 (n = 35) |
| Physical activity(walking) | IPAQ-SF | 22/50 reported an increase of 60 min or more per week | £5281 per year for walking | £116,182 | £2324 (n = 50) |
| £597,883 | £15,414 |
Total Social Value from the Social Value Calculator v.4
3.3. Outcomes Using the Mental Health Social Value Calculator
3.4. Outcomes from the CSRI Questionnaire
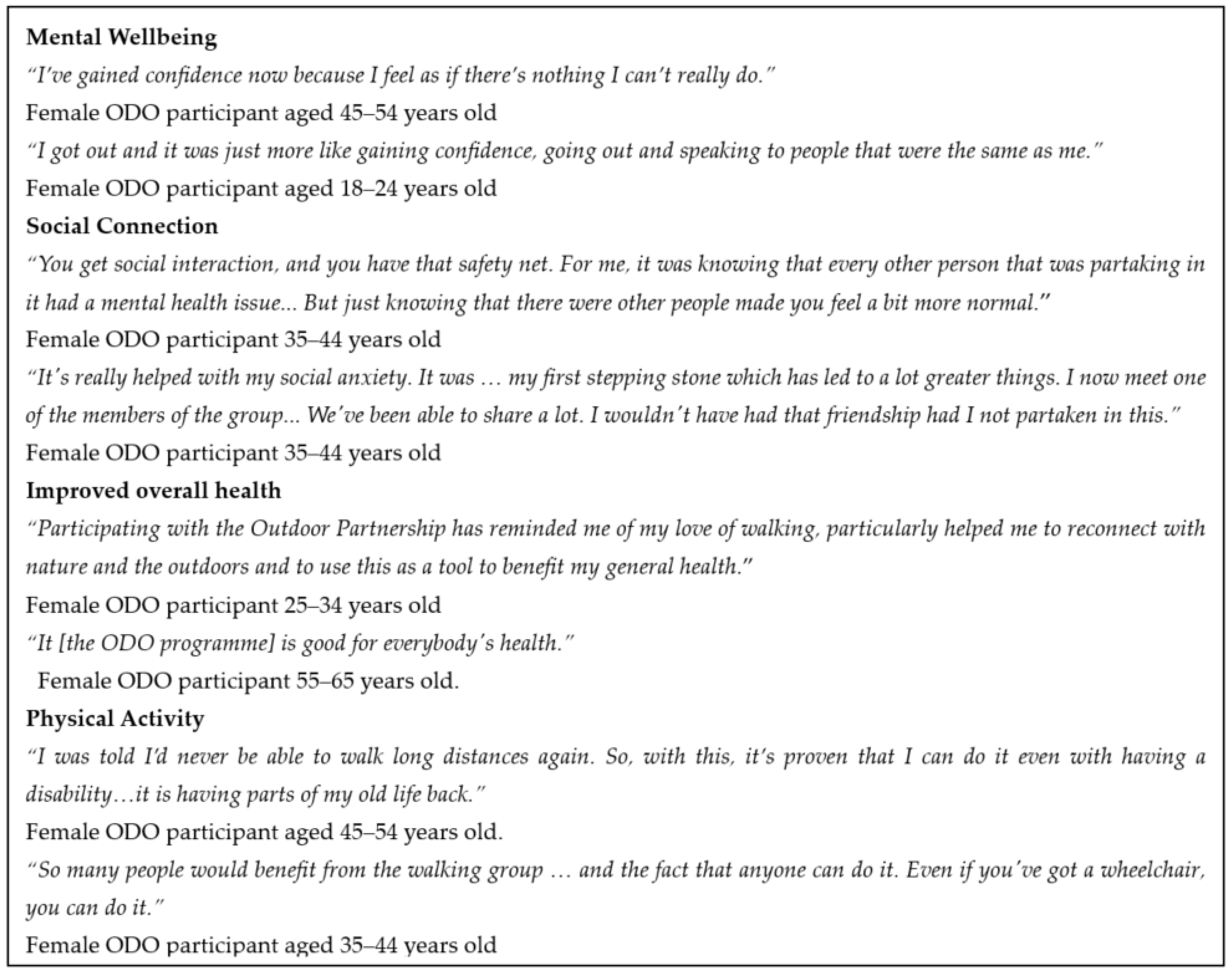
3.5. Qualitative Results from Semi-Structured Interviews
‘Social interaction is actually part of my values, and it is actually needed for good mental health, and I’m an avoider by nature.’(Participant 3)
‘So, it was an opportunity in a safer environment to hit my values if you like. So, to get social interaction, but have that safety net. For me, it was knowing that every other person that was partaking in it had a mental health issue. It didn’t matter if I knew what it was, but that initial realising that we’re all—we’re in different boats, but we’re in the same boat, and it’s something that nobody talks about, really, anyway. Just knowing that there were other people made you feel a bit more normal.’(Participant 2)
‘We’ve been able to share a lot, I wouldn’t have had that friendship had I not partaken in this.’(Participant 1)
‘A really good dose of nature as a freebie so that helped too.’(Participant 5)
3.6. Calculating the SROI Ratio
3.7. Wellbeing Valuation Using the Social Value Bank—Sensitivity Analysis
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Commissioning/Policy Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marconcin, P.; Werneck, A.O.; Peralta, M.; Ihle, A.; Gouveia, É.R.; Ferrari, G.; Sarmento, H.; Marques, A. The association between physical activity and mental health during the first year of the COVID-19 pandemic: A systematic review. BMC Public Health 2022, 22, 209. [Google Scholar] [CrossRef] [PubMed]
- NICE. Physical Activity: Brief Advice for Adults in Primary Care; NICE: Manchester, UK, 2013. [Google Scholar]
- Garcia, L.; Pearce, M.; Abbas, A.; Mok, A.; Strain, T.; Ali, S.; Crippa, A.; Dempsey, P.; Golubic, R.; Kelly, P.; et al. Non-occupational physical activity and risk of cardiovascular disease, cancer and mortality outcomes: A dose–response meta-analysis of large prospective studies. Br. J. Sport. Med. 2023, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, T. Healthcare Expenditure, UK Health Accounts: 2022. Office for National Statistics, 9 May 2022. [Google Scholar]
- Department of Health of Social Care. Physical activity: Applying All Our Health—GOV.UK. Office for Health Improvement and Disparities, 10 March 2022. [Google Scholar]
- Department of Health of Social Care. UK Chief Medical Officers’ Physical Activity Guidelines. Department of Health and Social Care, 7 September 2019. [Google Scholar]
- Office for National Statistics. Coronavirus and Depression in Adults, Great Britain 2022. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/articles/coronavirusanddepressioninadultsgreatbritain/julytoaugust2021#prevalence-of-depressive-symptoms-over-time (accessed on 25 October 2022).
- NHS England. Green Social Prescribing 2022. Available online: https://www.england.nhs.uk/personalisedcare/social-prescribing/green-social-prescribing/ (accessed on 5 December 2022).
- Welsh Government. The Healthy and Active Fund: A process evaluation (summary). Llywodraeth Cymru Welsh Government, 22 March 2021. [Google Scholar]
- Craig, P.; Dieppe, P.; Macintyre, S.; Mitchie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, 979–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Craig, N.; French, D.; McIntosh, E.; Petticrew, M.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef] [PubMed]
- Masters, R.; Anwar, E.; Collins, B.; Cookson, R.; Capewell, S. Return on investment of public health interventions: A systematic review. J. Epidemiol. Community Health 2017, 71, 827–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicholls, J.; Lawlor, E.; Nietzert, E. A Guide to Social Return on Investment; Social Value UK: Liverpool, UK, 2012. [Google Scholar]
- HM Treasury. The Green Book Central Government Guidance on Appraisal and Evaluation. Government Finance Function, 18 November 2022. [Google Scholar]
- New Economics Foundation. Measuring Well-Being A Guide for Practitioners Measuring Well-Being; NEF: London, UK, 2012. [Google Scholar]
- Hamelmann, C.; Turatto, F.; Then, V.; Dyakova, M. Investment for health and development. In Social Return on Investment Accounting for Value in the Context of Implementing Health 2020 and the 2030 Agenda for Sustainable Development; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Maher, R.; Buhmann, K. Meaningful stakeholder engagement: Bottom-up initiatives within global governance frameworks. Geoforum 2019, 107, 231–234. [Google Scholar] [CrossRef]
- Edwards, R.T.; Lawrence, C.L. ‘What You See is All There is’: The Importance of Heuristics in Cost-Benefit Analysis (CBA) and Social Return on Investment (SROI) in the Evaluation of Public Health Interventions. Appl. Health Econ. Health Policy 2021, 19, 653. [Google Scholar] [CrossRef] [PubMed]
- Trotter, L.; Rallings Adams, M.-K. Valuing Improvements in Mental Health: Applying the Wellbeing Valuation Method to WEMWBS; HACT: London, UK, 2017. [Google Scholar]
- Gwynedd, M. Social Return on Investment (SROI) Evaluation Report of the Pathways to Employment Programme Part of the Social Value Cymru Project; Cronfa Gymunedol Community Fund: Edinburgh, Scotland, 2019. [Google Scholar]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verducci, S.; Schröer, A. Social Trust. In International Encyclopedia of Civil Society; Springer: Cham, Switzerland, 2010; pp. 1453–1458. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Ainsworth, B.; Pratt, M.; Ekelund, U.; Yngve, A.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ács, P.; Veress, R.; Rocha, P.; Dóczi, T.; Raposa, B.L.; Baumann, P.; Ostojic, S.; Pérmusz, V.; Makai, A. Criterion validity and reliability of the International Physical Activity Questionnaire—Hungarian short form against the RM42 accelerometer. BMC Public Health 2021, 21, 381. [Google Scholar] [CrossRef] [PubMed]
- Ridyard, C.H.; Hughes, D.A. Methods for the Collection of Resource Use Data within Clinical Trials: A Systematic Review of Studies Funded by the UK Health Technology Assessment Program. Value Health 2010, 13, 867–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Bryman, A.; Burgess, R.G. Analyzing Qualitative Data; Routledge: Milton Park, UK, 1994. [Google Scholar]
- Dancer, S. Homes & Communities Agency Simon Dancer Additionality Guide, 4th ed.; Homes and Communities Agency: London, UK, 2014.
- Taylor, M. What is sensitivity analysis. Consort. YHE Univ. York 2009, 1, 1–8. [Google Scholar]
- Carrick, K.; Lindhof, J. The Value of Walking a Social Return on Investment Study; Greenspace Scotland: Glasgow, Scotland, 2011. [Google Scholar]
- Paths for All. Glasgow Health Walks Making an Impact; Paths for All: Edinburgh, Scotland, 2013. [Google Scholar]
- Hardman, I. Fighting for Life: The Twelve Battles that Made Our NHS, and the Struggle for Its Future; Penguin: London, UK, 2023. [Google Scholar]
- UK Parliament. Prevention in Health and Social Care. 2023. Available online: https://committees.parliament.uk/work/7205/prevention-in-health-and-social-care (accessed on 28 March 2023).



| Outcome | Outcome Measure | Wellbeing Valuation Method |
|---|---|---|
| Mental wellbeing | SWEMWBS | Mental Health Social Value Calculator v.1.0 |
| Social trust | Social trust question | Social Value Calculator v.4.0 |
| Good health | Overall health question | Social Value Calculator v.4.0 |
| Physical activity | IPAQ-SF | Social Value Calculator v.4.0 |
| ODO Participants | |
|---|---|
| Age | 96% 18–64 years-old (average 48 years old) |
| Gender | 64% male, 34% female, 2% transgender |
| Ethnic origin | 94% white British |
| Health status | 71% of participants cited a chronic condition (e.g., anxiety, asthma, COPD, diabetes, depression, epilepsy, multiple sclerosis, psychosis, etc.) |
| ODO participant group distribution | 41 walking participants, 11 climbing participants |
| Employment status | 67% of participants were unemployed at baseline |
| 63% of participants were unemployed at follow-up |
| Cost Category | Total Outdoor Partnership Costs | ODO Programme Costs (17% of Outdoor Partnership Costs) |
|---|---|---|
| Website (Total) | GBP 1608 | GBP 273 |
| GBP 960 | GBP 163 |
| GBP 648 | GBP 110 |
| Equipment and software (Total) | GBP 2422 | GBP 381 |
| GBP 930 | GBP 32 |
| GBP 998 | GBP 34 |
| GBP 216 | GBP 37 |
| GBP 278 | GBP 278 |
| Overheads (Total) | GBP 14,931 | GBP 2538 |
| GBP 4319 | GBP 734 |
| GBP 5098 | GBP 867 |
| GBP 5514 | GBP 937 |
| Staffing (Total) | GBP 71,400 | GBP 34,023 |
| GBP 30,600 | GBP 18,558 |
| GBP 40,800 | GBP 15,465 |
| Session (Total) | GBP 0 | GBP 36,065 |
| n/a | GBP 360 |
| n/a | GBP 35,280 |
| n/a | GBP 425 |
| Transport (Total) | GBP 1626 | GBP 849 |
| GBP 1136 | GBP 193 |
| GBP 490 | GBP 83 |
| n/a | GBP 573 |
| Total cost per year | GBP 91,987 | GBP 74,129 |
| Total cost per person per year 1 | n/a | GBP 706 |
| Outcomes | Total Social Value | Deadweight | Attribution | Displacement | Total Social Value | Total Social Value per Participants |
|---|---|---|---|---|---|---|
| Social trust | £101,331 | 49% (×0.51) | 47% (×0.53) | 17% (×0.83) | £22,734 | £484 (n = 47) |
| Good overall health | £382,679 | 49% (×0.51) | 47% (×0.53) | 17% (×0.83) | £85,854 | £2453 (n = 35) |
| Physical activity | £116,182 | 49% (×0.51) | 47% (×0.53) | 17% (×0.83) | £26,065 | £521 (n = 50) |
| Social impact | £590,921 | £134,653 | £3458 |
| ID# | Baseline (T1) | T1 Social Value | Follow-Up (T2) | T2 Social Value | Difference (T2-T1) | Social Value | After Deadweight (27%) |
|---|---|---|---|---|---|---|---|
| 1 | 26 | £24,225 | 28 | £24,877 | 2 | £652 | £476 |
| 2 | 27 | £24,877 | 19 | £17,561 | −8 | −£7316 | −£5341 |
| 3 | 24 | £22,944 | 24 | £22,944 | 0 | £0 | £0 |
| 4 | 24 | £22,944 | 21 | £21,049 | −3 | −£1895 | −£1383 |
| 5 | 7 | 0 | 19 | £17,561 | 12 | £17,561 | £12,820 |
| 6 | 21 | £21,049 | 21 | £21,049 | 0 | £0 | £0 |
| 7 | 21 | £21,049 | 26 | £24,225 | 5 | £3176 | £2318 |
| 8 | 23 | £22,944 | 25 | £24,225 | 2 | £1281 | £935 |
| 9 | 16 | £9639 | 22 | £21,049 | 6 | £11,410 | £8329 |
| 10 | 21 | £21,049 | 19 | £17,561 | −2 | −£3488 | −£2546 |
| 11 | 19 | £17,561 | 24 | £22,944 | 5 | £5383 | £3930 |
| 12 | 18 | £12,255 | 20 | £17,561 | 2 | £5306 | £3873 |
| 13 | 7 | 0 | 12 | £0 | 5 | £0 | £0 |
| 14 | 14 | 0 | 21 | £21,049 | 7 | £21,049 | £15,366 |
| 15 | 22 | £21,049 | 21 | £21,049 | −1 | £0 | £0 |
| 16 | 7 | 0 | 7 | £0 | 0 | £0 | £0 |
| 17 | 20 | £17,561 | 21 | £21,049 | 1 | £3488 | £2546 |
| 18 | 11 | 0 | 26 | £24,225 | 15 | £24,225 | £17,684 |
| 20 | 27 | £24,877 | 22 | £21,049 | −5 | −£3828 | −£2794 |
| 21 | 23 | £22,944 | 27 | £24,877 | 4 | £1933 | £1411 |
| 22 | 16 | £9639 | 25 | £24,225 | 9 | £14,586 | £10,648 |
| 23 | 20 | £17,561 | 22 | £21,049 | 2 | £3488 | £2546 |
| 24 | 21 | £21,049 | 26 | £24,225 | 5 | £3176 | £2318 |
| 25 | 18 | £12,255 | 20 | £17,561 | 2 | £5306 | £3873 |
| 26 | 17 | £12,255 | 23 | £22,944 | 6 | £10,689 | £7803 |
| 27 | 15 | £9639 | 24 | £22,944 | 9 | £13,305 | £9713 |
| 28 | 18 | £12,255 | 16 | £9639 | −2 | −£2616 | −£1910 |
| 29 | 19 | £17,561 | 26 | £24,225 | 7 | £6664 | £4865 |
| 30 | 28 | £24,877 | 25 | £24,225 | −3 | −£652 | −£476 |
| 31 | 22 | £21,049 | 19 | £17,561 | −3 | -£3488 | −£2546 |
| 32 | 20 | £17,561 | 19 | £17,561 | −1 | £0 | £0 |
| 33 | 28 | £24,877 | 28 | £24,877 | 0 | £0 | £0 |
| 34 | 21 | £21,049 | 21 | £21,049 | 0 | £0 | £0 |
| 35 | 21 | £21,049 | 27 | £24,877 | 6 | £3828 | £2794 |
| 36 | 22 | £21,049 | 28 | £24,877 | 6 | £3828 | £2794 |
| 37 | 21 | £21,049 | 21 | £21,049 | 0 | £0 | £0 |
| 38 | 13 | £0 | 21 | £21,049 | 8 | £21,049 | £15,366 |
| 39 | 16 | £9639 | 18 | £12,255 | 2 | £2616 | £1910 |
| 40 | 15 | £9639 | 28 | £24,877 | 13 | £15,238 | £11,124 |
| 41 | 21 | £21,049 | 23 | £22,944 | 2 | £1895 | £1383 |
| 42 | 21 | £21,049 | 24 | £22,944 | 3 | £1895 | £1383 |
| 43 | 30 | £25,480 | 31 | £26,175 | 1 | £695 | £507 |
| 44 | 10 | 0 | 24 | £22,944 | 14 | £22,944 | £16,749 |
| 45 | 13 | 0 | 23 | £22,944 | 10 | £22,944 | £16,749 |
| 46 | 17 | £12,255 | 26 | £24,225 | 9 | £11,970 | £8738 |
| 47 | 22 | £21,049 | 24 | £22,944 | 2 | £1895 | £1383 |
| 48 | 19 | £17,561 | 29 | £25,480 | 10 | £7919 | £5781 |
| 49 | 23 | £22,944 | 28 | £24,877 | 5 | £1933 | £1411 |
| 50 | 16 | £9639 | 20 | £17,561 | 4 | £7922 | £5783 |
| 51 | 24 | £22,944 | 24 | £22,944 | 0 | £0 | £0 |
| 52 | 20 | £17,561 | 26 | £24,225 | 6 | £6664 | £4865 |
| Total | £802,550 | £1042,955 | £264,630 | £193,180 | |||
| Total social value per participant (n = 51) | £3788 | ||||||
| Category | 3-Months before Programme | 3-Months during Programme | Difference in Visits | Cost per Visit | Cost Saving per 3-Months | Cost Saving per 12-Months |
|---|---|---|---|---|---|---|
| Psychiatrist | 14 | 19 | 5 | £51/visit 1 | −£255 | −£1020 |
| Psychologist | 38 | 36 | −2 | £58/visit 1 | £116 | £464 |
| Mental health nurse | 79 | 73 | −6 | £21/visit 1 | £126 | £504 |
| Total cost saving | −£13 | −£52 | ||||
| Total cost saving per participant (n = 52) | −£1 | |||||
| Outcomes: | Indicators | Quantity Improved | Financial Value | Total Social Value for Participants | Social Value per Participant |
|---|---|---|---|---|---|
| Social Trust | NEF Social Trust Question | 18/47 reported an increase of 20% or more | £3753 per year for feeling a sense of belonging to neighbourhood | £67,554 | £1437 (n = 47) |
| Good Overall Health | Overall health question | 19/35 reported an improvement of 50% or more | £20,141 per person per year for significant improvement in good overall health | £382,679 | £10,934 (n = 35) |
| Physical Activity (Walking) | IPAQ-SF | 13/50 reported an increase of 80 min or more per week | £5281 per year for walking | £68,653 | £1373 (n = 50) |
| £518,886 | £13,744 |
| Outcomes | Total Social Value | Deadweight | Attribution | Displacement | Total Social Value | Total Social Value per Participant |
|---|---|---|---|---|---|---|
| Social trust | £67,554 | 49% (×0.51) | 47% (×0.53) | 17% (×0.83) | £15,156 | £322 (n = 47) |
| Good overall health | £382,679 | 49% (×0.51) | 47% (×0.53) | 17% (×0.83) | £85,854 | £2453 (n = 35) |
| Physical activity | £68,653 | 49% (×0.51) | 47% (×0.53) | 17% (×0.83) | £15,402 | £308 (n = 50) |
| Social impact | £518,886 | £116,412 | £3085 |
| SROI Ratio (Social Value Calculator —Conservative Case) | SROI Ratio (Social Value Calculator) | SROI Ratio (Mental Health Social Value Calculator) | |
|---|---|---|---|
| Total social value per participant | £3085 | £3458 | £3788 |
| NHS cost savings per participant | −£1 | −£1 | −£1 |
| Total social value participant | £3084 | £3457 | £3787 |
| Total cost per participant | £706 | £706 | £706 |
| SROI ratio | £4.37:£1 | £4.90:£1 | £5.36:£1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makanjuola, A.; Lynch, M.; Hartfiel, N.; Cuthbert, A.; Edwards, R.T. Prevention of Poor Physical and Mental Health through the Green Social Prescribing Opening Doors to the Outdoors Programme: A Social Return on Investment Analysis. Int. J. Environ. Res. Public Health 2023, 20, 6111. https://doi.org/10.3390/ijerph20126111
Makanjuola A, Lynch M, Hartfiel N, Cuthbert A, Edwards RT. Prevention of Poor Physical and Mental Health through the Green Social Prescribing Opening Doors to the Outdoors Programme: A Social Return on Investment Analysis. International Journal of Environmental Research and Public Health. 2023; 20(12):6111. https://doi.org/10.3390/ijerph20126111
Chicago/Turabian StyleMakanjuola, Abraham, Mary Lynch, Ned Hartfiel, Andrew Cuthbert, and Rhiannon Tudor Edwards. 2023. "Prevention of Poor Physical and Mental Health through the Green Social Prescribing Opening Doors to the Outdoors Programme: A Social Return on Investment Analysis" International Journal of Environmental Research and Public Health 20, no. 12: 6111. https://doi.org/10.3390/ijerph20126111