
Prevention of Type 1 Diabetes in Children: A Worthy Challenge?


Department of Pediatrics, University of Chieti, Via dei Vestini, 66100 Chieti, Italy
*
Author to whom correspondence should be addressed.
Int. J. Environ. Res. Public Health 2023, 20(11), 5962; https://doi.org/10.3390/ijerph20115962
Submission received: 31 January 2023
/
Revised: 19 March 2023
/
Accepted: 21 May 2023
/
Published: 26 May 2023
(This article belongs to the Special Issue Diabetes: Screening, Prevention, Diagnosis and Therapy)
{kind=link}
{kind=link}
Abstract
:Nowadays, the development of new immuno-therapeutic drugs has made it possible to alter the course of many autoimmune diseases. Type 1 diabetes is a chronic disease with a progressive dependence on exogenous insulin administration. The ability to intercept individuals at high risk of developing type 1 diabetes is the first step toward the development of therapies that can delay the process of β-cell destruction, thus permitting a better glycemic control and reducing the incidence of ketoacidosis. The knowledge of the main pathogenetic mechanisms underlying the three stages of the disease may be helpful to identify the best immune therapeutic approach. In this review, we aim to give an overview of the most important clinical trials conducted during the primary, secondary and tertiary phases of prevention.
1. Introduction
Type 1 diabetes (T1D) is a chronic autoimmune disease with an insufficient insulin release due to a destruction of pancreatic β-cells, resulting in hyperglycemia. Islet autoantibodies that develop as the result of β-cells damage include autoantibodies against insulin (IAA), insulinoma-associated antigen-2 (IA-2), glutamic acid decarboxylase (GAD), zinc-transporter 8 (ZnT8), and islet cell antibodies (ICA) [1]. Over the last decades the incidence of T1D has dramatically increased, especially in toddlers and preschool children, imposing a huge economic burden on the global health system. In 2021, Ogle et al. estimated more than 108,300 new diagnoses of T1D among children and adolescents under 15 years of age [2]. The median age at seroconversion is before 3 years of age. Genetic predisposition and environmental factors are the main risk factors that influence T1D onset.
The first susceptibility genes to be identified were human leucocyte antigens (HLA), responsible for up to 50% of diabetes cases [3]. The susceptibility haplotypes most correlated to T1D are DR3.DQ2 and DR4.DQ8 haplotypes [4]. Genome-wide association studies (GWAS) detected more than 50 non-HLA loci associated with the risk of development of T1D [5]. HLA and non-HLA loci (PTPN22, CTLA4, IL2RA and INS) concur with the heritability of T1D, for approximately 80% of cases [6]. The insulin gene (INS) is the strongest genetic factor correlated to T1D, which may affect the immune reactivity to insulin [7]. A genetic risk score (GRS) that incorporated 30 T1D-associated SNPs from both HLA and non-HLA loci was developed in order to evaluate the risk of T1D progression. The GRS was shown to be a strong predictor tool of progression from single to multiple autoantibodies, and to the clinical development of T1D in high-risk individuals [8].
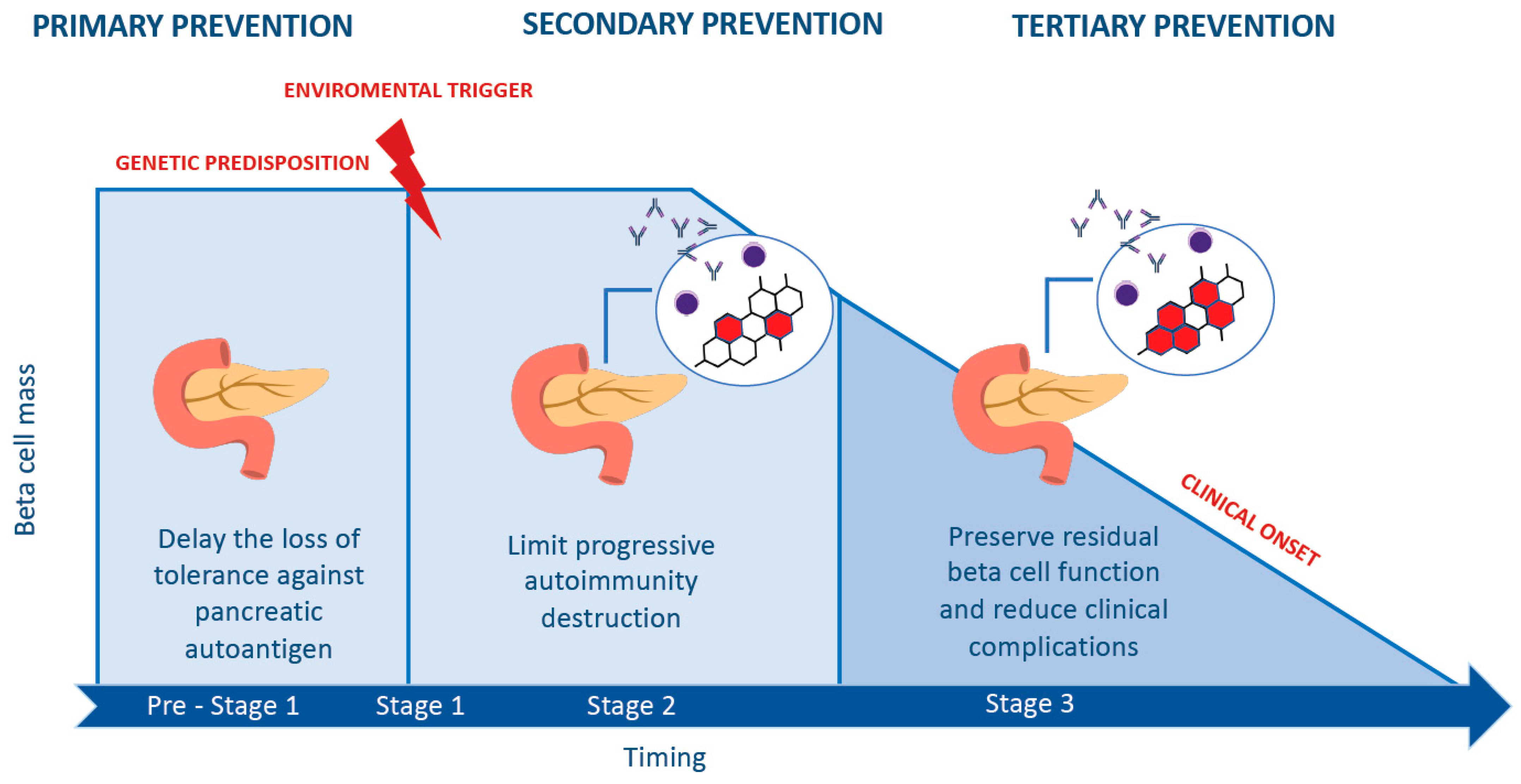
Several studies demonstrated the pivotal role of environmental factors that act as triggers at different time points in the course of the disease. Interestingly, Eisenbarth proposed a model of the natural history of T1D, representing the β-cell mass as a function of age. The first step is characterized by genetic predisposition, followed by an environmental trigger that determines the onset of immunological abnormalities, up to the development of overt diabetes [3]. Insel et al. recently proposed a staging classification based on the presence of autoantibodies, glycemia level and the manifestation of signs and symptoms of diabetes [9] (Figure 1). Depending on the number and the islet autoantibody type in circulation, it is possible to define a high or low probability of developing T1D. In particular, a high risk of progression rate is reported among those who have multiple islet autoantibodies. Moreover, the presence of IAA and IA-2 accelerates the timing of progression to diabetes from the time of seroconversion [10].
2. The Road to Prevention
The adoption of Eisenbarth and Insel’s pathogenetic staging of T1D has provided not only a standardized taxonomy [11], but also the possibility to identify subjects at risk of developing T1D, thus paving the way to its prevention. About 15,000 children and young adults who are first- or second-degree relatives of individuals with T1D are screened annually for islet autoantibodies through TrialNet [12]. Through the years, in addition to studies in family members, genetic testing of those without familial predisposition also proved to be a good tool, since only up to 15% of cases of newly diagnosed T1D have an identifiable family history [13,14]. A formidable accomplishment of this approach comes from Bavaria, Germany in the so-called “Fr1da” study, where Ziegler et al. screened 90,632 pre-school children aged between 2 and 5 years during primary care visits. Of these children, 280 (0.31%) had 2 or more islet autoantibodies, 62 developed clinical T1D, and 2 had mild or moderate diabetic ketoacidosis [15]. Before this, smaller studies had assessed screening of school-age children only [16,17,18,19].
Another relevant example of a large trial in the general population is the study “The Environmental Determinants of Diabetes in the Young” (TEDDY), a prospective cohort study that monitored 8667 genetically at-risk children at 3- to 6-month intervals from birth from 2004, for the development of islet autoantibodies and T1D [20]. The long-term goal of the TEDDY study was the identification of infectious agents, dietary factors, or other environmental agents, including psychosocial factors, that could trigger or protect from T1D in genetically susceptible individuals. As Bonifacio et al. reported [21], the risk of multiple seroconversion in these children declines exponentially with age, since the 5-year risk of developing multiple islet autoantibodies was 4.3% at 7.5 months of age and declined to 1.1% at a landmark age of 6.25 years [21]. Since genetic factors seem to influence the risk only in the first year of life, a practical aspect of this age-related seroconversion is the possibility to have an “efficient window” for multiple Ab diagnosis and T1D prevention: the highest sensitivity and positive predictive value was achieved by autoantibody screening at 2 years, and again at 5–7 years of age [21]. In another recent study, where 20,303 children with an increased T1D risk from Finland, Germany, and USA were screened and followed up to 18 years of age, the time from seroconversion to diabetes diagnosis was increased by 0.64 years for each 1-year increment of diagnosis age. Single screening at the age of 10 years was 90% sensitive, with a positive predictive value of 66% for clinical diabetes. Screening at two ages (10 years and 14 years) increased sensitivity to 93%, but lowered the positive predictive value to 55% [22]. These studies not only demonstrate that screening programs for T1D are possible, but they also may reduce the clinical burden of ketoacidosis (DKA) thanks to an earlier diagnosis. DKA is a life-threatening event which occurs in 30–60% of children newly diagnosed with T1D [23,24]; the incidence of DKA has dramatically increased during the COVID-19 pandemic [25]. In Fr1da, the prevalence of DKA was less than 5%, much lower than 20–30% in unscreened German children [26].
As in many other chronic and non-communicable diseases, prevention consists of three levels of intervention: primary prevention, aimed at avoiding development of autoimmunity against islet autoantigens; secondary prevention, interfering instead with β-cell destruction after the seroconversion; and finally, tertiary prevention, which is focused on preventing the clinical complications of T1D, with the main goal of delaying at least their onset, thus preserving residual β cell-function (Figure 1 and Figure 2).
3. Primary Prevention
It is evident that primary prevention has a strong reason for being, since it concerns the first period in life where the influence of genetic and environmental factors is the highest in the process of immunological tolerance. Primary prevention should start from pregnancy, since the influence of several factors on the risk of developing T1D has been observed in this phase. A prospective cohort study in Denmark analyzed the association between prenatal gluten exposure and offspring risk of T1D. High gluten intake during pregnancy seems to be correlated with an elevated risk of the offspring developing T1D. Overweight/obese women may be more sensitive to gluten intake than younger women or women of normal weight. The mechanism that could be responsible for this effect is not known, but it could include increased inflammation and a complex interaction between diet, immune development, microbiota and intestinal permeability. However, more evidence is needed to confirm these suggestive trends [27]. The correlation between maternal weight and the risk of developing T1D has been analyzed in several studies. A population-based study from Sweden, which included 1,263,358 children who were followed from birth, demonstrated how a high maternal BMI during the first trimester increases the incidence of T1D in the offspring of parents without diabetes. Thus, the prevention of excess weight and obesity in women of reproductive age may contribute to a decreased incidence of T1D [28]. In addition, maternal infection during pregnancy is considered to be a risk factor for developing T1D. A meta-analysis based on studies conducted in Finland and Sweden showed that maternal gestational infection is associated with 32% increased odds of T1DM or islet auto-immunity in offspring [29]. In particular, enterovirus infection during pregnancy increased the risk of T1D in offspring by up to 54%. This effect could be explained by the molecular mimicry between β-islet cell antigens and pathogens [30]. Prenatal protective factors for the development of autoimmunity include maternal vitamin D intake. The study “Diabetes Autoimmunity Study in the Young” (DAISY) evidenced the protective role of maternal intake of vitamin D via food during pregnancy on the risk of the onset of T1D in offspring. This protective effect may be due to the suppression role of vitamin D on the inflammatory cytokines in utero life [31].
All RCTs for the primary prevention of T1D have included early life dietary interventions and antigen-based therapy in newborns and toddlers, with the aim being to delay the loss of tolerance against pancreatic autoantigens. Interestingly, Vehik et al. [32] suggested that environmental exposure can trigger T1D in subjects who are less genetically susceptible, since high-risk HLA genotypes are becoming less frequent over time in some populations.
Breast milk has been found to contain various anti-inflammatory bioactive molecules such as immunoglobulins, adipokines, oligosaccharides, insulin, lactoferrin, lysozyme, cytokines, beneficial bacteria and vitamins, which can give infants a lifelong immunity against many diseases, including T1D. As hypoadiponectinemia is a risk factor for gestational diabetes mellitus (GDM), it has been suggested that adipokines in breast milk could have a potential role in increasing β-cell function in newborns [33]. Despite this, the association between breastfeeding and T1D remains controversial. In a meta-analysis of 43 studies, breastfeeding demonstrated a weak protective effect on T1D risk [34]; however, it should always be encouraged in children at risk, as for the general population.
Instead, based on the evidence in animal models that early exposure to cow’s milk proteins may increase the risk of β-cell autoimmunity [35], the TRIGR (“Trial to Reduce IDDM in Genetically at Risk”) was the first to be proposed as a dietary RCT in 5156 infants at genetic risk for type 1 diabetes, with a high retention and documented protocol adherence [36]. Unfortunately, the use of a hydrolyzed formula compared with a conventional formula did not reduce the incidence of β-cell autoimmunity after 7 years. Interestingly, a cumulative incidence of 9.9% by the age of 6 years for multiple seroconversion in the control group was estimated. TRIGR study results are in contrast to data from the TRIGR pilot study [37] performed in 230 Finnish children, which reported that weaning to an extensively hydrolyzed formula in infancy was associated with an almost 50% reduction in the cumulative incidence of β-cell autoimmunity by the age of 10 years in similar children.
Another dietary intervention trial is The Finnish Dietary Intervention Trial for the Prevention of Type 1 Diabetes (FINDIA), which assessed the impact of complete avoidance of bovine insulin in infants in Finland. It randomized high risk infants to cow’s milk formula, whey-based hydrolyzed formula, or whey-based formula free of bovine insulin during the first 6 months of life. A reduced rate of development of one islet autoantibody was seen in the bovine insulin-free group [38].
T1D and celiac disease (CD) are autoimmune diseases with a clinical and pathogenic overlap. In addition, an early introduction of cereals in infants had been associated with T1D [39]. In the open randomized controlled BABYDIET study [40], 150 newborns with genetic high risk were randomly assigned to a first gluten exposure at the age of 6 months (control group) or 12 months (late exposure group), and were followed at 3 monthly intervals until the age of 3 years. Again, delaying gluten exposure until the age of 12 months did not substantially reduce the risk for islet autoimmunity.
Implementation in the diet of omega-3 fatty acids, whose anti-inflammatory properties are well known, has been associated with a lower risk of T1D [41,42,43]. The Pilot Trial “Nutritional Intervention to Prevent Type 1 Diabetes” (NIP) was a double-blind placebo-controlled study of omega 3 fatty acid supplementation with docosahexaenoic acid (DHA). The aim of this study was to prevent islet cell autoimmunity in infants with an increased risk of developing T1D and who entered the study in the third trimester of pregnancy, or infants aged younger than 5 months with a first-degree family member with T1D. Thus far, no effect on autoimmunity has been noted [44].
Insulin has also been employed as an antigen-based therapy. Antigen-based therapy is based on the evidence that the administration of antigens can lead to an immunological tolerance [45,46,47]. The GPPAD-POInT Study is a randomized, placebo-controlled, double-blind phase IIb study that aimed to induce immune tolerance to β-cell autoantigens through regular exposure to oral insulin from 29 to 32 months. The study objective is to determine whether daily administration of oral insulin from 4 months to 7 months until the age of 3 years old to children with elevated genetic risk for T1D reduces the cumulative incidence of β-cell autoantibodies and diabetes in childhood. No data are available as yet [48]. Previously, oral insulin therapy at a modest daily dose of 7.5 mg did not delay progression to type 1 diabetes in first-degree relatives with insulin autoantibodies and ICA, except for a subgroup of relatives with high levels of insulin antibodies [49].
Within the environmental factors, viral infections have a predominant role in the pathogenesis of T1D in children with an elevated genetic risk. A viral infection could both cause β-cell cytolysis or indirectly trigger progressive diabetes autoimmunity [50]. Above all, viruses that have been evaluated to be potentially involved in T1D pathogenesis—the persistence of silent and chronic enterovirus infections, especially Coxsackie virus B1 (CVB)—have been strongly associated with the appearance of islet autoantibodies and an increased risk of T1D [51]. For this reason, vaccines can be one of the strategies on the road to primary prevention of T1D, such as an enteroviral serotypes vaccine [52]. Recent preclinical studies have outlined the concept that a CVB vaccine prevents viral infection and diabetes induction in mice [53]. In humans, an enterovirus vaccine may be effective for the primary prevention of T1D by blocking the triggering of autoimmunity and the onset of immune-mediated beta cell dysfunction [54]. Interestingly, an association between the Rotavirus vaccination and the incidence of T1D was noted [55]. In a cohort study of 1,474,535 infants in the United States from 2001 to 2017, a 33% reduction in the risk of T1D was reported with the completion of the Rotavirus vaccine series compared to the unvaccinated [55], suggesting a potential role of the Rotavirus vaccination in the prevention of the disease.
Gut microbiota has a primary role in the pathogenesis of T1D, affecting intestinal permeability, molecular mimicry, and modulating the innate and adaptive immune system. In the TEDDY study, modest alterations of microbial composition have been reported in patients with autoantibodies or T1D, particularly in the higher numbers of genes involved in fermentation pathways and the production of Short Chain Fatty Acids (SCFA). Butyrate, a SCFA product, is well known for its role in gut epithelial integrity maintenance and promoting anti-inflammatory responses [56,57]. In a mice model of T1D, the administration of Lactobacillus johnsonii delayed the development and the progression of the disease [58]. For all of these reasons, exploring the role of the microbiome may provide new highlights into developing safe strategies to modulate immune regulation in infants and children.
Finally, although most of these trials have failed in their primary outcomes, we may draw several lessons from them: primary prevention trials in first-degree relatives and beyond are feasible and may show a great adherence, offering the opportunity to have a second chance at prevention (secondary) if children develop β-cell autoantibodies [58].
4. Secondary Prevention
Secondary prevention includes several therapeutic strategies that are implemented during stage 1 and 2 of T1D when the autoimmune process has already been established. This is characterized by the presence of at least two auto-antibodies against β-pancreatic cells, the absence of dysglycemic states and clinical manifestations [1]. In this stage, the β-pancreatic cell population is still minimally affected, allowing an optimal glycemic control, although metabolic alterations can be evidenced after oral (OGTT) and intravenous glucose tolerance tests (IVGTT). Therefore, the main purpose of secondary prevention therapies is to limit, contain and stop the autoimmune process, prolonging the duration of stage 1 and 2 of T1D and preventing the onset of the clinical phase of diabetes [59]. Secondary prevention therapies may act on two fronts: the first is based on the induction of immunotolerance toward autoantigens, while the second consists of an immunomodulatory function in order to block the mechanisms and cells of autoimmunity [60,61]. Regarding the first, several clinical trials have been carried out, analyzing the effects of prolonged administration of low doses of specific self-antigens on the development of autoantibodies against β-pancreatic cells.
The “Diabetes Prevention Trial-Type 1” (DPT-1) clinical trial evaluated the effects of subcutaneous and oral insulin administration in patients with stage 2 T1D. Eligible patients aged between 1 and 45 years and with familiarity for T1D were screened by autoantibody assay, and then by IVGTT and OGTT. Patients with autoantibodies and positive glucose tolerance test were considered high-risk, while those with positive autoantibodies and a normal glucose tolerance test were considered medium-risk. The study population was then divided into a control group and two intervention groups, respectively, following subcutaneous insulin therapy at a dosage of 0.125 IU/Kg 2 vv/day combined with continuous intravenous insulin administration for 4 days at baseline and at T + 12 months (high-risk group), and one with oral insulin at a dosage of 7.5 mg/day (medium-risk group). Unfortunately, no results were obtained regarding the prevention of T1D in either intervention group compared with the placebo, although a subgroup with a high titer of IAA treated with oral insulin has shown a significant reduction in the incidence of T1D compared with the placebo [62,63,64]. The TrialNet study, conducted in a population with at least two autoantibody positivity and alterations at IVGTT, who were administered oral insulin at a dosage of 7.5 mg/day, showed no improvement in terms of prevention compared with the placebo; however, an insulin-treated subgroup highlighted a delay in the diagnosis of overt diabetes and a reduction in incidence compared with the placebo [65]. In the “Belgian Parenteral Study” trial, a test was carried out to discover whether regular administration of ultrarapid subcutaneous insulin before carbohydrate-rich meals may contribute to the maintenance of functional β-cell integrity in patients with autoantibody positivity and without alterations of glucose tolerance. A reduction in the incidence of T1D was observed compared with the placebo, albeit it was not statistically significant [66]. Intranasal insulin administration was then evaluated in subjects with familiarity for T1D and autoantibody positivity. The “Intranasal Insulin Trials” (INIT-1, INIT-II) did not demonstrate a clear benefit in the absence of adverse reactions [67,68]. The “Diabetes Prediction and Prevention Study” (DIPP) trial was performed in a population with a genetic predisposition for developing T1D and positivity for at least two autoantibodies through intranasal insulin administration; however, this trial was stopped due to a lack of benefit, even though the safety of intranasal insulin was demonstrated [69,70].
Another autoantigen tested in experimental trials has been GAD. In the clinical trial “Diabetes Prevention-Immune Tolerance” (DIAPREV-IT), the effect of administration of GAD conjugated to aluminum hydroxide (GAD-alum) was studied in normoglycemic children with anti-GAD antibodies and another type of positive antibody. This study showed differences that, although not statistically significant, compared with the placebo, since the treatment would result in an increase in Treg lymphocytes that would limit the action of anti-GAD65 T-lymphocytes; the safety of the drug was also demonstrated, but efficacy needs to be improved [71,72]. The main limitation of preventive therapies based on the immunotolerance mechanism is that the action of T-lymphocytes is not directed toward a single self-antigen, but is a complex reaction involving numerous self-antigens [73]. Another pharmacological approach is based on the immunomodulation through the administration of antibodies directed against specific targets. The main effectors of adaptive immunity are T and B lymphocytes; immunomodulatory therapies can act on these two cell lines by regulating their activity, which is typically unbalanced in autoimmune processes [74,75]. The effect of monoclonal antibodies against the TCR receptor complex of CD3+ T-lymphocytes was evaluated. The TrialNet study highlighted that Teplizumab, an anti-CD3 monoclonal antibody, delays the onset of clinical T1D in stage 2 patients with autoimmunity and dysglycemia [76]. The long-term effects of this treatment are the expansion of Treg and control of effector T-lymphocytes. It has been shown that Teplizumab is able to reduce the risk of disease progression to stage 3 by nearly 60% [77,78]. Teplizumab was approved by the Food and drug Administration (FDA) on November 2022 for adults and children of at least 8 years, and is the first approved drug that delays the onset of T1D. Therapy with Teplizumab consists of infusion of the drug intravenously once daily for 14 consecutive days. The main side effects are leukopenia, skin rash and headache [79].
Abatacept is a chimeric protein consisting of the extracellular Cytotoxic T-Lymphocyte Antigen 4 (CTLA4-Ig) domain bound to the Fc portion of human IgG1, which suppresses T-lymphocyte activity. Abatacept binds to signal molecules (CD80 and CD86), which, through binding to their respective receptors on T-lymphocytes, result in their activation and proliferation [80,81]. The Abatacept TrialNet study was conducted in a sample with autoimmunity and without dysglycemia, and is still ongoing. Immunomodulatory therapies that are directed toward B-lymphocytes act through limiting β-cell damage and regulating pancreatic T-lymphocyte infiltration [82,83]. Preclinical studies in mouse models have shown that depletion of B-lymphocytes by anti-CD20 antibodies (Rituximab) would correlate with the arrest of the autoimmune process. The major limiting factors are the important side effects related to B-cell depletion, such as increased susceptibility to opportunistic infections. The use of anti-CD20 antibodies also target the IL-10-producing subpopulation of regulatory B-cells (Breg), which play an important function in the mechanisms of immunotolerance. Finally, depletion of the B population also indirectly affects the Treg lymphocyte response. A possible strategy in order to limit these side effects could be the use of drugs that selectively target islet-responsive B-lymphocytes, and the use of combination therapies with other drugs that limit the side effects of anti-CD20 antibodies [84].
Regarding other types of pharmacological approaches, the effect of cyclosporine has been investigated, although limited data exist. It would seem that cyclosporine decreases the incidence of T1D in patients with autoimmunity and familiarity through its immunosuppressive effect on T-lymphocytes. However, considering the many associated side effects such as nephrotoxicity, its long-term use would be inappropriate [74]. In addition, nonpharmacological approaches such as the administration of high doses of vitamin B3, which would reduce free radical-induced damage to β-cells, have been evaluated in “The Deutsche Nicotinamide Intervention Study” (DENIS) and “The European Nicotinamide Diabetes Intervention Trial” (ENDIT) clinical trials. Although a positive effect was shown in animal models, in patients with familial and autoimmunity, no preventive benefit was shown in comparison with the placebo [85,86,87]. A possible preventive effect of vitamin D with omega-3 fatty acids was evaluated in the POSEIDON trial, evaluating their combined anti-inflammatory and immunomodulating effect [88].
5. Tertiary Prevention
At the time of diagnosis, more than 80% of β-cells mass is destroyed by specific CD4+ and CD8+ T-cells as well as B-cells; for this reason, a lifelong exogenous insulin is needed [89]. Tertiary prevention includes several strategies, with the main goals of preserving residual β-cells, thus reducing exogenous insulin requirement, and delaying the onset of complications. Several studies have demonstrated a correlation between lower HbA1c values and preserved C-peptide levels, with a reduction in long-term complications and better metabolic control [23].
In the last 12 years, various RCTs have been conducted in order to detect immune therapies that may ameliorate β-cells function in patients with T1D [90].
A single-blinded randomized placebo-controlled study demonstrated a preservation of C-peptide in patients with established T1D, through the combination of anti-thymocyte globulin (ATG) and pegylated G-CSF for 12 months following treatment. This study suggested an improvement of β-cells function up to 12 months following ATG and G-CSF treatment. This combination may affect the immune system, causing a reduction of CD4+ T cells and a preservation of CD8+ T cells [91]. The Type 1 Diabetes TrialNet Study Group performed a three-arm, randomized, double-masked, placebo-controlled trial in which the primary outpoint was to evaluate the area under the curve (AUC) of C-peptide by comparing ATG and ATG + G-CSF treatments. The group that received a low dose of ATG (2.5 mg/kg) had a better AUC C-peptide at 1 year than in those receiving ATG and G-CSF (respectively, 2.5 mg/kg and 6 mg subcutaneously every 2 weeks for 6 doses). At 1 year, HbA1c was lower in both treated groups, despite no significant differences in HbA1c levels, which were registered confronting ATG and ATG + G-CSF groups versus the placebo group [92].
The T1GER study was a phase 2 trial that tested Golimumab, a human monoclonal antibody specific for TNF alpha, among children and young adults with a recent T1D diagnosis. At 52 weeks, comparing golimumab versus the placebo group, a preservation of C-peptide and a reduction of the total daily insulin was documented. Despite no significative differences reported in Hb1Ac between the two groups, golimumab was correlated with a longer duration of partial remission characterized by minimal insulin production, which provides a glycemic control [93]. Beneficial effects were reported in the golimumab group after 2 years following the discontinuation of therapy. In particular, golimumab arrested β-cells loss, preserving their function while undergoing treatment [94]. The activation of lymphocytes T cells requires two stimulations: the first one is the interaction between the antigen, presented by the major histocompatibility complex (MHC) or the antigen-presenting cells (APC) and the T cells receptor. The second stimulation is a costimulatory signal between CD80/86 and CD28, which has a pivotal role in the full activation and survival of T cells. Abatacept prevents the costimulatory signal binding CD80/86, thereby sending an inhibitory signal inside the T cells. Some authors demonstrated that abatacept (CTLA4-Ig) preserves β-cells function in patients with a recent onset of T1D, slowing the decline of C-peptide during the 2 years of treatment by 9.6 months [95]. IL-21 cytokines stimulate CD8 + T lymphocytes, which play an important role in the pathogenesis of β-cells damage and the onset of T1D [96].
Moreover, the GLP-1 receptor agonist reduces β-cells stress and apoptosis, increases proinsulin/insulin ratio, and preserves insulin release glucose induced by stress factors. A double-blind randomized phase 2 trial studied the combination of anti-IL-21 and liraglutide in 308 patients with a recent T1D onset. This trial reported a better endogenous insulin secretion, assessed as a smaller decline in MMTT-stimulated C-peptide concentration, and a glucose metabolism improvement in the treated group from baseline to 54 weeks [97]. IL-2 plays an important role in the immune homeostasis, activating CD4 + FOXP3 + Tregs which limit the action of autoreactive anti-β-cell T effector cells (Teff). T1D pathogenesis susceptibility is due to a lacking regulation of Teffs by Tregs, which promote autoreactive Teffs expansion. Previous studies, such as DILT1D and DILfrequency performed in adults with T1D, provided reassuring information about the safety of aldesleukin administration [98,99]. The “Interleukin-2 Therapy of Autoimmunity in Diabetes (ITAD)” is an ongoing clinical phase 2, double-blind and placebo-controlled trial that included children and adolescents within 6 weeks from a T1D diagnosis. A total of 45 participants were included and randomized to receive an ultra-low dose of IL-2 (aldesleukin) or placebo for 6 months. The main goal of the ITAD trial is to assess the efficacy of aldesleukin treatment on β-cells function, as evaluated by C-peptide on a dried blood spot [100]. As previously stated, Teplizumab has been currently approved by FDA in children above 8 years of age as a disease-modifying therapy. Several trials have studied anti-CD3 monoclonal antibody efficacy in reducing insulin deterioration and β-cells damage [101,102]. Protégé was a phase 3 trial with 516 enrolled patients with a new onset of T1D who would receive Teplizumab administration. At 2 years, a reduced loss of AUC mean C-peptide was documented among those who received a 14-day full dose regimen of Teplizumab [103]. Moreover, the Autoimmunity-Blocking Antibody for Tolerance (AbATE) trial studied the action of Teplizumab in patients recently diagnosed with T1D for 7 years. At 1 year, a reduced loss of C-peptide was detected in drug treated responders, which was characterized by an augmentation of programmed cell death protein 1-positive central memory and CD8+ T cells. In addition, otelixizumab, another anti-CD 3 humanized antibody, has shown to affect the disease course only if administered in a high dose, despite stimulating an EBV reactivation. At the same time, a lower dose was not associated with a β-cells protection. The best effectiveness in preserving β-cells function is correlated with the positivity of IAA in patients with a recent T1D diagnosis [104,105]. It is anticipated that gene therapy will be a potential cure for T1D. The objective of gene therapy is based on transforming alternative cells in β-cells, thus preventing an attack on the immune system. Xiao et al. reprogrammed α-cells in β-cells through the infusion of an adeno-associated virus carrying Pdx1 and Maf, in autoimmune non-obese diabetic (NOD) mice. Pdx is a transcription factor required for β-cell maturation and proliferation, whereas MafA is a transcription factor that is able to regulate insulin expression [106]. The normal blood level in NOD mice lasts up to 4 months, but this result can be affected by the mouse lifespan. However, it is not possible to predict the immune system response in humans. Moreover, some studies focused on the identification of mechanisms able to stop the immune system from damaging β-cells. In the literature, the role of the antiapoptotic gene A20, which normally inhibits NF-κB activation was demonstrated. The overexpression of the A20 level by means of an adenoviral vector is able to improve islet transplantation outcomes, reducing the expression of inflammatory mediators. This effect is based on the inhibition of NF-κB and JNK/AP1 pathways [107,108]. Currently, the literature has described only pre-clinical trials on gene-therapy; although the results are very promising, more studies are needed.
6. Conclusions
T1D is a chronic autoimmune disease whose course is characterized by a pre-clinical and a clinical phase. The aim of prevention is to intervene during the early development of the disease by slowing or halting its progression. The first step in achieving valid results in prevention is to strengthen screening in the general population, and make them a part of the “Standard of Care”. Screening strategies could allow to identify individuals at risk for T1D in order to enroll them in clinical trials. Another possible benefit of screening programs is the purpose of reducing the incidence of DKA at the time of diagnosis [109], as well as the opportunity to offer psychological, emotional and social support to children and families at the time of diagnosis [24]. The importance of clinical trials is to identify new therapies that are safe and effective in changing the natural history of disease evolution. Although the alarming incidence of T1D in children increases the necessity of its prevention, there are several gaps and limitations concerning prevention strategies. Unfortunately, T1D is still considered a low prevalence disease in children, unlike other metabolic diseases such as obesity; the risk of false positives in screening tests is very high when the incidence of the disease is low [110]. For this reason, the lack of cost-effective and clinically advantageous screening programs makes it difficult to identify asymptomatic subjects and their participation in clinical trials. Moreover, the extraordinary technological advances in insulin therapy (including new insulin analogues, insulin pumps, continuous glucose monitoring systems, and automated insulin delivery systems) ensure that insulin still remains the “standard of care” in the treatment of diabetes, decreasing the rates of disease complications in proportion to glycemic control [111]. Besides insulin, only Teplizumab has been approved by FDA as the first drug that mildly delays the onset of T1D. Lastly, prevention strategies may lead to family and individual anxiety due to unwillingness to accept a treatment in the asymptomatic phases. We believe that this gap can only be conquered by a multidisciplinary approach, which provides not only good clinical practice but also psychological support to families.
A pivotal element in identifying possible new therapeutic strategies is to improve the knowledge of molecular mechanisms underlying the pathogenesis of T1D. A better understanding of these mechanisms could make it easier to identify possible targets for new immunological therapies. Although numerous clinical trials have not highlighted significant results, a winning strategy may be to use combination immunotherapies that act on several fronts. At present, several clinical trials have been conducted or are still ongoing; however, further studies are needed, and although the way to find safe and effective preventive therapies is still far, the obtained results are very promising.
Author Contributions
Conceptualization and supervision: F.C., D.M.F.I., M.T.Q. and A.Q. have equally contributed to the final version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data are contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Primavera, M.; Giannini, C.; Chiarelli, F. Prediction and Prevention of Type 1 Diabetes. Front. Endocrinol. Lausanne 2020, 11, 248. [Google Scholar] [CrossRef] [PubMed]
- Ogle, G.D.; James, S.; Dabelea, D.; Pihoker, C.; Svennson, J.; Maniam, J.; Klatman, E.L.; Patterson, C.C. Global estimates of incidence of type 1 diabetes in children and adolescents: Results from the International Diabetes Federation Atlas, 10th edition. Diabetes Res. Clin. Pract. 2022, 183, 109083. [Google Scholar] [CrossRef] [PubMed]
- DiMeglio, L.A.; Evans-Molina, C.; Oram, R.A. Type 1 diabetes. Lancet 2018, 391, 2449–2462. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.A. Molecular aspects of type 1 diabetes. Mol. Pathol. 2003, 56, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Redondo, M.J.; Steck, A.K.; Pugliese, A. Genetics of type 1 diabetes. Pediatr. Diabetes 2018, 19, 346–353. [Google Scholar] [CrossRef]
- Cerolsaletti, K.; Hao, W.; Greenbaum, C.J. Genetics Coming of Age in Type 1 Diabetes. Diabetes Care 2019, 42, 189–191. [Google Scholar] [CrossRef]
- Barrett, J.C.; Clayton, D.G.; Concannon, P.; Akolkar, B.; Cooper, J.D.; Erlich, H.A.; Julier, C.; Morahan, G.; Nerup, J.; Nierras, C.; et al. Genome-wide association study and meta-analysis find that over 40 loci affect risk of type 1 diabetes. Nat. Genet. 2009, 41, 703–707. [Google Scholar] [CrossRef]
- Redondo, M.J.; Geyer, S.; Steck, A.K.; Sharp, S.; Wentworth, J.M.; Weedon, M.N.; Antinozzi, P.; Sosenko, J.; Atkinson, M.; Pugliese, A.; et al. A Type 1 Diabetes Genetic Risk Score Predicts Progression of Islet Autoimmunity and Development of Type 1 Diabetes in Individuals at Risk. Diabetes Care 2018, 41, 1887–1894. [Google Scholar] [CrossRef]
- Insel, R.A.; Dunne, J.L.; Atkinson, M.A.; Chiang, J.L.; Dabelea, D.; Gottlieb, P.A.; Greenbaum, C.J.; Herold, K.C.; Krischer, J.P.; Lernmark, Å.; et al. Staging Presymptomatic Type 1 Diabetes: A Scientific Statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care 2015, 38, 1964–1974. [Google Scholar] [CrossRef]
- Ziegler, A.G.; Rewers, M.; Simell, O.; Simell, T.; Lempainen, J.; Steck, A.; Winkler, C.; Ilonen, J.; Veijola, R.; Knip, M.; et al. Seroconversion to Multiple Islet Autoantibodies and Risk of Progression to Diabetes in Children. JAMA 2013, 309, 2473. [Google Scholar] [CrossRef]
- Atkinson, M.A.; Eisenbarth, G.S.; Michels, A.W. Type 1 diabetes. Lancet 2014, 383, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Mahon, J.L.; Sosenko, J.M.; Rafkin-Mervis, L.; Krause-Steinrauf, H.; Lachin, J.M.; Thompson, C.; Bingley, P.J.; Bonifacio, E.; Palmer, J.P.; Eisenbarth, G.S.; et al. The TrialNet Natural History Study of the Development of Type 1 Diabetes: Objectives, design, and initial results. Pediatr. Diabetes 2009, 10, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Kostraba, J.N.; Gay, E.C.; Cai, Y.; Cruickshanks, K.J.; Rewers, M.J.; Klingensmith, G.J.; Chase, H.P.; Hamman, R.F. Incidence of Insulin-Dependent Diabetes Mellitus in Colorado. Epidemiology 1992, 3, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Eurodiab Ace Study Group; The Eurodiab Ace Substudy 2 Study Group. Familial Risk of Type I diabetes in European Children. Diabetologia 1998, 41, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, A.G.; Kick, K.; Bonifacio, E.; Haupt, F.; Hippich, M.; Dunstheimer, D.; Lang, M.; Laub, O.; Warncke, K.; Lange, K.; et al. Yield of a Public Health Screening of Children for Islet Autoantibodies in Bavaria, Germany. JAMA 2020, 323, 339. [Google Scholar] [CrossRef]
- Schatz, D.; Krischer, J.; Horne, G.; Riley, W.; Spillar, R.; Silverstein, J.; Winter, W.; Muir, A.; Derovanesian, D.; Shah, S. Islet cell antibodies predict insulin-dependent diabetes in United States school age children as powerfully as in unaffected relatives. J. Clin. Investig. 1994, 93, 2403–2407. [Google Scholar] [CrossRef]
- Velluzzi, F.; The Sardinian Autoimmunity Study Group; Secci, G.; Sepe, V.; Klersy, C.; Shattock, M.; Foxon, R.; Songini, M.; Mariotti, S.; Locatelli, M.; et al. Prediction of type 1 diabetes in Sardinian schoolchildren using islet cell autoantibodies: 10-year follow-up of the Sardinian schoolchildren type 1 diabetes prediction study. Acta Diabetol. 2016, 53, 73–79. [Google Scholar] [CrossRef]
- Strebelow, M.; Schlosser, M.; Ziegler, B.; Rjasanowski, I.; Ziegler, M. Karlsburg Type I diabetes risk study of a general population: Frequencies and interactions of the four major Type I diabetes-associated autoantibodies studied in 9419 schoolchildren. Diabetologia 1999, 42, 661–670. [Google Scholar] [CrossRef]
- Parikka, V.; Näntö-Salonen, K.; Saarinen, M.; Simell, T.; Ilonen, J.; Hyoty, H.; Veijola, R.; Knip, M.; Simell, O. Early seroconversion and rapidly increasing autoantibody concentrations predict prepubertal manifestation of type 1 diabetes in children at genetic risk. Diabetologia 2012, 55, 1926–1936. [Google Scholar] [CrossRef]
- TEDDY Study Group. The Environmental Determinants of Diabetes in the Young (TEDDY) study: Study design. Pediatr. Diabetes 2007, 8, 286–298. [Google Scholar] [CrossRef]
- Bonifacio, E.; Weiß, A.; Winkler, C.; Hippich, M.; Rewers, M.J.; Toppari, J.; Lernmark, Å.; She, J.-X.; Hagopian, W.A.; Krischer, J.P.; et al. An Age-Related Exponential Decline in the Risk of Multiple Islet Autoantibody Seroconversion During Childhood. Diabetes Care 2021, 44, 2260–2268. [Google Scholar] [CrossRef] [PubMed]
- Ghalwash, M.; Anand, V.; Lou, O.; Martin, F.; Rewers, M.; Ziegler, A.-G.; Toppari, J.; Hagopian, W.A.; Veijola, R.; Achenbach, P.; et al. Islet autoantibody screening in at-risk adolescents to predict type 1 diabetes until young adulthood: A prospective cohort study. Lancet Child Adolesc. Health 2023, 7, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Chiarelli, F.; Rewers, M.; Phillip, M. Screening of Islet Autoantibodies for Children in the General Population: A Position Statement Endorsed by the European Society for Paediatric Endocrinology. Horm Res Paediatr. 2022, 95, 393–396. [Google Scholar] [CrossRef]
- Cherubini, V.; Grimsmann, J.M.; Åkesson, K.; Birkebæk, N.H.; Cinek, O.; Dovč, K.; Gesuita, R.; Gregory, J.W.; Hanas, R.; Hofer, S.E.; et al. Temporal trends in diabetic ketoacidosis at diagnosis of paediatric type 1 diabetes between 2006 and 2016: Results from 13 countries in three continents. Diabetologia 2020, 63, 1530–1541. [Google Scholar] [CrossRef]
- Ho, J.; Rosolowsky, E.; Pacaud, D.; Huang, C.; Bsc, J.L.; Brockman, N.; Rath, M.; Doulla, M. Diabetic ketoacidosis at type 1 diabetes diagnosis in children during the COVID-19 pandemic. Pediatr. Diabetes 2021, 22, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Große, J.; Hornstein, H.; Manuwald, U.; Kugler, J.; Glauche, I.; Rothe, U. Incidence of Diabetic Ketoacidosis of New-Onset Type 1 Diabetes in Children and Adolescents in Different Countries Correlates with Human Development Index (HDI): An Updated Systematic Review, Meta-Analysis, and Meta-Regression. Horm. Metab. Res. 2018, 50, 209–222. [Google Scholar] [PubMed]
- Antvorskov, J.C.; Halldorsson, T.I.; Josefsen, K.; Svensson, J.; Granström, C.; Roep, B.O.; Olesen, T.H.; Hrolfsdottir, L.; Buschard, K.; Olsen, S.F. Association between maternal gluten intake and type 1 diabetes in offspring: National prospective cohort study in Denmark. BMJ 2018, 362, k3547. [Google Scholar] [CrossRef] [PubMed]
- Hussen, H.I.; Persson, M.; Moradi, T. Maternal overweight and obesity are associated with increased risk of type 1 diabetes in offspring of parents without diabetes regardless of ethnicity. Diabetologia 2015, 58, 1464–1473. [Google Scholar] [CrossRef]
- Yue, Y.; Tang, Y.; Tang, J.; Shi, J.; Zhu, T.; Huang, J.; Qiu, X.; Zeng, Y.; Li, W.; Qu, Y.; et al. Maternal infection during pregnancy and type 1 diabetes mellitus in offspring: A systematic review and meta-analysis. Epidemiol. Infect. 2018, 146, 2131–2138. [Google Scholar] [CrossRef]
- Craig, M.E.; Kim, K.W.; Isaacs, S.R.; Penno, M.A.; Hamilton-Williams, E.E.; Couper, J.J.; Rawlinson, W.D. Early-life factors contributing to type 1 diabetes. Diabetologia 2019, 62, 1823–1834. [Google Scholar] [CrossRef]
- Fronczak, C.M.; Barón, A.E.; Chase, H.P.; Ross, C.; Brady, H.L.; Hoffman, M.; Eisenbarth, G.S.; Rewers, M.; Norris, J.M. In Utero Dietary Exposures and Risk of Islet Autoimmunity in Children. Diabetes Care 2003, 26, 3237–3242. [Google Scholar] [CrossRef] [PubMed]
- Vehik, K.; Hamman, R.F.; Lezotte, D.; Norris, J.M.; Klingensmith, G.J.; Rewers, M.; Dabelea, D. Trends in High-Risk HLA Susceptibility Genes Among Colorado Youth With Type 1 Diabetes. Diabetes Care 2008, 31, 1392–1396. [Google Scholar] [CrossRef] [PubMed]
- Yahaya, T.; Shemishere, U. Association between Bioactive Molecules in Breast Milk and Type 1 Diabetes Mellitus. Sultan Qaboos Univ. Med. J. 2020, 20, 5. [Google Scholar] [CrossRef]
- Cardwell, C.R.; Stene, L.C.; Ludvigsson, J.; Rosenbauer, J.; Cinek, O.; Svensson, J.; Perez-Bravo, F.; Memon, A.; Gimeno, S.G.; Wadsworth, E.J.; et al. Breast-Feeding and Childhood-Onset Type 1 Diabetes. Diabetes Care 2012, 35, 2215–2225. [Google Scholar] [CrossRef] [PubMed]
- Chia, J.; McRae, J.; Enjapoori, A.; Lefèvre, C.; Kukuljan, S.; Dwyer, K. Dietary Cows’ Milk Protein A1 Beta-Casein Increases the Incidence of T1D in NOD Mice. Nutrients 2018, 10, 1291. [Google Scholar] [CrossRef]
- Knip, M.; Åkerblom, H.K.; Becker, D.; Dosch, H.-M.; Dupre, J.; Fraser, W.; Howard, N.; Ilonen, J.; Krischer, J.P.; Kordonouri, O.; et al. Hydrolyzed Infant Formula and Early β-Cell Autoimmunity. JAMA 2014, 311, 2279. [Google Scholar] [CrossRef] [PubMed]
- Åkerblom, H.K.; Virtanen, S.; Ilonen, J.; Savilahti, E.; Vaarala, O.; Reunanen, A.; Teramo, K.; Hämäläinen, A.-M.; Paronen, J.; Riikjärv, M.-A.; et al. Dietary manipulation of beta cell autoimmunity in infants at increased risk of type 1 diabetes: A pilot study. Diabetologia 2005, 48, 829–837. [Google Scholar] [CrossRef]
- Vaarala, O.; Ilonen, J.; Ruohtula, T.; Pesola, J.; Virtanen, S.; Härkönen, T.; Koski, M.; Kallioinen, H.; Tossavainen, O.; Poussa, T.; et al. Removal of Bovine Insulin From Cow’s Milk Formula and Early Initiation of Beta-Cell Autoimmunity in the FINDIA Pilot Study. Arch. Pediatr. Adolesc. Med. 2012, 166, 608. [Google Scholar] [CrossRef]
- Norris, J.M. Timing of Initial Cereal Exposure in Infancy and Risk of Islet Autoimmunity. JAMA 2003, 290, 1713. [Google Scholar] [CrossRef]
- Hummel, S.; Pflüger, M.; Hummel, M.; Bonifacio, E.; Ziegler, A.G. Primary Dietary Intervention Study to Reduce the Risk of Islet Autoimmunity in Children at Increased Risk for Type 1 Diabetes. Diabetes Care 2011, 34, 1301–1305. [Google Scholar] [CrossRef]
- Joner, G.; Søvik, O. The incidence of Type 1 (insulin-dependent) diabetes mellitus 15–29 years in Norway 1978–1982. Diabetologia 1991, 34, 271–274. [Google Scholar] [CrossRef]
- Norris, J.M.; Yin, X.; Lamb, M.M.; Barriga, K.; Seifert, J.; Hoffman, M.; Orton, H.D.; Barón, A.E.; Clare-Salzler, M.; Chase, H.P.; et al. Omega-3 Polyunsaturated Fatty Acid Intake and Islet Autoimmunity in Children at Increased Risk for Type 1 Diabetes. JAMA 2007, 298, 1420. [Google Scholar] [CrossRef] [PubMed]
- Stene, L.C.; Ulriksen, J.; Magnus, P.; Joner, G. Use of cod liver oil during pregnancy associated with lower risk of Type I diabetes in the offspring. Diabetologia 2000, 43, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Chase, H.P.; Boulware, D.; Rodriguez, H.; Donaldson, D.; Chritton, S.; Rafkin-Mervis, L.; Krischer, J.; Skyler, J.S.; Clare-Salzler, M. Effect of docosahexaenoic acid supplementation on inflammatory cytokine levels in infants at high genetic risk for type 1 diabetes. Pediatr. Diabetes 2015, 16, 271–279. [Google Scholar] [CrossRef]
- Harrison, L.C. Vaccination against self to prevent autoimmune disease: The type 1 diabetes model. Immunol. Cell Biol. 2008, 86, 139–145. [Google Scholar] [CrossRef]
- Harrison, L.C.; Hafler, D.A. Antigen-specific therapy for autoimmune disease. Curr. Opin. Immunol. 2000, 12, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, A.G.; Nepom, G.T. Prediction and Pathogenesis in Type 1 Diabetes. Immunity 2010, 32, 468–478. [Google Scholar] [CrossRef]
- Ziegler, A.G.; Achenbach, P.; Berner, R.; Casteels, K.; Danne, T.; Gündert, M.; Hasford, J.; Hoffmann, V.S.; Kordonouri, O.; Lange, K.; et al. Oral insulin therapy for primary prevention of type 1 diabetes in infants with high genetic risk: The GPPAD-POInT (global platform for the prevention of autoimmune diabetes primary oral insulin trial) study protocol. BMJ Open. 2019, 9, e028578. [Google Scholar] [CrossRef]
- Skyler, J.S.; Krischer, J.P.; Wolfsdorf, J.; Cowie, C. Effects of Oral Insulin in Relatives of Patients With Type 1 Diabetes. Diabetes Care 2005, 28, 1068–1076. [Google Scholar]
- Houeiss, P.; Luce, S.; Boitard, C. Environmental Triggering of Type 1 Diabetes Autoimmunity. Front. Endocrinol. Lausanne 2022, 13, 1551. [Google Scholar] [CrossRef]
- Laitinen, O.H.; Honkanen, H.; Pakkanen, O.; Oikarinen, S.; Hankaniemi, M.M.; Huhtala, H.; Ruokoranta, T.; Lecouturier, V.; André, P.; Harju, R.; et al. Coxsackievirus B1 Is Associated With Induction of β-Cell Autoimmunity That Portends Type 1 Diabetes. Diabetes 2014, 63, 446–455. [Google Scholar] [CrossRef]
- Insel, R.; Dunne, J.L. JDRF’s vision and strategy for prevention of type 1 diabetes. Pediatr. Diabetes 2016, 17, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Stone, V.M.; Hankaniemi, M.M.; Svedin, E.; Sioofy-Khojine, A.; Oikarinen, S.; Hyöty, H.; Laitinen, O.H.; Hytönen, V.P.; Flodström-Tullberg, M. A Coxsackievirus B vaccine protects against virus-induced diabetes in an experimental mouse model of type 1 diabetes. Diabetologia 2018, 61, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Dunne, J.L.; Richardson, S.J.; Atkinson, M.A.; Craig, M.E.; Dahl-Jørgensen, K.; Flodström-Tullberg, M.; Hyöty, H.; Insel, R.A.; Lernmark, Å.; Lloyd, R.E.; et al. Rationale for enteroviral vaccination and antiviral therapies in human type 1 diabetes. Diabetologia 2019, 62, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.A.M.; Basu, T.; Kim, C. Lower Incidence Rate of Type 1 Diabetes after Receipt of the Rotavirus Vaccine in the United States, 2001–2017. Sci. Rep. 2019, 9, 7727. [Google Scholar] [CrossRef]
- Stewart, C.J.; Ajami, N.J.; O’brien, J.L.; Hutchinson, D.S.; Smith, D.P.; Wong, M.C.; Ross, M.C.; Lloyd, R.E.; Doddapaneni, H.; Metcalf, G.A.; et al. Temporal development of the gut microbiome in early childhood from the TEDDY study. Nature 2018, 562, 583–588. [Google Scholar] [CrossRef]
- Vatanen, T.; Franzosa, E.A.; Schwager, R.; Tripathi, S.; Arthur, T.D.; Vehik, K.; Lernmark, Å.; Hagopian, W.A.; Rewers, M.J.; She, J.-X.; et al. The human gut microbiome in early-onset type 1 diabetes from the TEDDY study. Nature 2018, 562, 589–594. [Google Scholar] [CrossRef]
- Valladares, R.; Sankar, D.; Li, N.; Williams, E.; Lai, K.-K.; Abdelgeliel, A.S.; Gonzalez, C.F.; Wasserfall, C.H.; Larkin, J.; Schatz, D.; et al. Lactobacillus johnsonii N6.2 Mitigates the Development of Type 1 Diabetes in BB-DP Rats. PLoS ONE 2010, 5, e10507. [Google Scholar] [CrossRef]
- Dayan, C.M.; Besser, R.E.J.; Oram, R.A.; Hagopian, W.; Vatish, M.; Bendor-Samuel, O.; Snape, M.D.; Todd, J.A. Preventing type 1 diabetes in childhood. Science 2021, 373, 506–510. [Google Scholar] [CrossRef]
- Warshauer, J.T.; Bluestone, J.A.; Anderson, M.S. New Frontiers in the Treatment of Type 1 Diabetes. Cell Metab. 2020, 31, 46–61. [Google Scholar] [CrossRef]
- Allen, L.A.; Dayan, C.M. Immunotherapy for type 1 diabetes. Br. Med. Bull 2021, 140, 76–90. [Google Scholar] [CrossRef] [PubMed]
- Rapini, N.; Schiaffini, R.; Fierabracci, A. Immunotherapy Strategies for the Prevention and Treatment of Distinct Stages of Type 1 Diabetes: An Overview. Int. J. Mol. Sci. 2020, 21, 2103. [Google Scholar] [CrossRef]
- Sosenko, J.M.; Skyler, J.S.; Krischer, J.P.; Greenbaum, C.J.; Mahon, J.; Rafkin, L.E.; Cuthbertson, D.; Cowie, C.; Herold, K.; Eisenbarth, G.; et al. Glucose Excursions Between States of Glycemia with Progression to Type 1 Diabetes in the Diabetes Prevention Trial–Type 1 (DPT-1). Diabetes 2010, 59, 2386–2389. [Google Scholar] [CrossRef]
- Voss, M.G.; Cuthbertson, D.D.; Cleves, M.M.; Xu, P.; Evans-Molina, C.; Palmer, J.P.; Redondo, M.J.; Steck, A.K.; Lundgren, M.; Larsson, H.; et al. Time to Peak Glucose and Peak C-Peptide During the Progression to Type 1 Diabetes in the Diabetes Prevention Trial and TrialNet Cohorts. Diabetes Care 2021, 44, 2329–2336. [Google Scholar] [CrossRef]
- Sosenko, J.M.; Skyler, J.S.; Herold, K.C.; Schatz, D.A.; Haller, M.J.; Pugliese, A.; Cleves, M.; Geyer, S.; Rafkin, L.E.; Matheson, D.; et al. Slowed Metabolic Decline After 1 Year of Oral Insulin Treatment Among Individuals at High Risk for Type 1 Diabetes in the Diabetes Prevention Trial–Type 1 (DPT-1) and TrialNet Oral Insulin Prevention Trials. Diabetes 2020, 69, 1827–1832. [Google Scholar] [CrossRef] [PubMed]
- Vandemeulebroucke, E.; Gorus, F.; Decochez, K.; Weets, I.; Keymeulen, B.; De Block, C.; Tits, J.; Pipeleers, D.; Mathieu, C. Insulin treatment in IA-2A-positive relatives of type 1 diabetic patients. Diabetes Metab. 2009, 35, 319–327. [Google Scholar] [CrossRef]
- Harrison, L.C.; Honeyman, M.C.; Steele, C.E.; Stone, N.L.; Sarugeri, E.; Bonifacio, E.; Couper, J.J.; Colman, P.G. Pancreatic β-Cell Function and Immune Responses to Insulin After Administration of Intranasal Insulin to Humans At Risk for Type 1 Diabetes. Diabetes Care 2004, 27, 2348–2355. [Google Scholar] [CrossRef] [PubMed]
- Fourlanos, S.; Perry, C.; Gellert, S.A.; Martinuzzi, E.; Mallone, R.; Butler, J.; Colman, P.G.; Harrison, L.C. Evidence That Nasal Insulin Induces Immune Tolerance to Insulin in Adults with Autoimmune Diabetes. Diabetes 2011, 60, 1237–1245. [Google Scholar] [CrossRef]
- Kanta, A.; Lyka, E.; Koufakis, T.; Zebekakis, P.; Kotsa, K. Prevention strategies for type 1 diabetes: A story of promising efforts and unmet expectations. Hormones 2020, 19, 453–465. [Google Scholar] [CrossRef]
- Näntö-Salonen, K.; Kupila, A.; Simell, S.; Siljander, H.; Salonsaari, T.; Hekkala, A.; Korhonen, S.; Erkkola, R.; Sipilä, J.I.; Haavisto, L.; et al. Nasal insulin to prevent type 1 diabetes in children with HLA genotypes and autoantibodies conferring increased risk of disease: A double-blind, randomised controlled trial. Lancet 2008, 372, 1746–1755. [Google Scholar] [CrossRef]
- Larsson, H.E.; Lernmark, Å. Does immune-tolerance treatment with Alum-formulated GAD65 protect insulin-production in the pancreatic islet β cells? Hum. Vaccin. 2011, 7, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Salami, F.; Spiliopoulos, L.; Maziarz, M.; Lundgren, M.; Brundin, C.; Bennet, R.; Hillman, M.; Törn, C.; Larsson, H.E. Long-Term GAD-alum Treatment Effect on Different T-Cell Subpopulations in Healthy Children Positive for Multiple Beta Cell Autoantibodies. J. Immunol. Res. 2022, 2022, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Hamad, A.R.A.; Ahmed, R.; Donner, T.; Fousteri, G. B cell-targeted immunotherapy for type 1 diabetes: What can make it work? Discov. Med. 2016, 21, 213–219. [Google Scholar]
- Brusko, T.M.; Russ, H.A.; Stabler, C.L. Strategies for durable β cell replacement in type 1 diabetes. Science 2021, 373, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Dariya, B.; Chalikonda, G.; Srivani, G.; Alam, A.; Nagaraju, G.P. Pathophysiology, Etiology, Epidemiology of Type 1 Diabetes and Computational Approaches for Immune Targets and Therapy. Crit. Rev. Immunol. 2019, 39, 239–265. [Google Scholar] [CrossRef]
- Mignogna, C.; Maddaloni, E.; D’Onofrio, L.; Buzzetti, R. Investigational therapies targeting CD3 for prevention and treatment of type 1 diabetes. Expert Opin. Investig. Drugs 2021, 30, 1209–1219. [Google Scholar] [CrossRef] [PubMed]
- Herold, K.C.; Bundy, B.N.; Long, S.A.; Bluestone, J.A.; DiMeglio, L.A.; Dufort, M.J.; Gitelman, S.E.; Gottlieb, P.A.; Krischer, J.P.; Linsley, P.S.; et al. An Anti-CD3 Antibody, Teplizumab, in Relatives at Risk for Type 1 Diabetes. N. Engl. J. Med. 2019, 381, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Sims, E.K.; Bundy, B.N.; Stier, K.; Serti, E.; Lim, N.; Long, S.A.; Geyer, S.M.; Moran, A.; Greenbaum, C.J.; Evans-Molina, C.; et al. Teplizumab improves and stabilizes beta cell function in antibody-positive high-risk individuals. Sci. Transl. Med. 2021, 13, eabc8980. [Google Scholar] [CrossRef]
- Hirsch, J.S. FDA approves teplizumab: A milestone in type 1 diabetes. Lancet Diabetes Endocrinol. 2023, 11, 18. [Google Scholar] [CrossRef]
- Skyler, J.S.; Pugliese, A. Immunotherapy Trials for Type 1 Diabetes: The Contribution of George Eisenbarth. Diabetes Technol. 2013, 15, S2-13–S2-20. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, A.; Gharibi, T.; Marofi, F.; Babaloo, Z.; Baradaran, B. CTLA-4: From mechanism to autoimmune therapy. Int. Immunopharmacol. 2020, 80, 106221. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, S.M.; Engle, S.; Kaldunski, M.; Jia, S.; Geoffrey, R.; Simpson, P.; Szabo, A.; Speake, C.; Greenbaum, C.J.; Chen, Y.-G.; et al. Innate immune activity as a predictor of persistent insulin secretion and association with responsiveness to CTLA4-Ig treatment in recent-onset type 1 diabetes. Diabetologia 2018, 61, 2356–2370. [Google Scholar] [CrossRef] [PubMed]
- Orban, T.; Bundy, B.; Becker, D.J.; DiMeglio, L.A.; Gitelman, S.E.; Goland, R.; Gottlieb, P.A.; Greenbaum, C.J.; Marks, J.B.; Monzavi, R.; et al. Costimulation modulation with abatacept in patients with recent-onset type 1 diabetes: Follow-up 1 year after cessation of treatment. Diabetes Care 2014, 37, 1069–1075. [Google Scholar] [CrossRef]
- Hinman, R.M.; Cambier, J.C. Role of B Lymphocytes in the Pathogenesis of Type 1 Diabetes. Curr. Diab. Rep. 2014, 14, 543. [Google Scholar] [CrossRef]
- Schatz, D.A.; Bingley, P.J. Update on major trials for the prevention of type 1 diabetes mellitus: The American Diabetes Prevention Trial (DPT-1) and the European Nicotinamide Diabetes Intervention Trial (ENDIT). J. Pediatr. Endocrinol. Metab. 2001, 14 (Suppl. 1), 619–622. [Google Scholar] [CrossRef]
- European Nicotinamide Diabetes Intervention Trial Group. Intervening before the onset of Type 1 diabetes: Baseline data from the European Nicotinamide Diabetes Intervention Trial (ENDIT). Diabetologia 2003, 46, 339–346. [Google Scholar] [CrossRef]
- Lampeter, E.F.; Klinghammer, A.; Scherbaum, W.A.; Heinze, E.; Haastert, B.; Giani, G.; Kolb, H. The Deutsche Nicotinamide Intervention Study: An attempt to prevent type 1 diabetes. DENIS Group. Diabetes 1998, 47, 980–984. [Google Scholar] [CrossRef] [PubMed]
- Baidal, D.A.; Sanchez, J.; Alejandro, R.; Blaschke, C.E.; Hirani, K.; Matheson, D.L.; Messinger, S.; Pugliese, A.; Rafkin, L.E.; Roque, L.A.; et al. POSEIDON study: A pilot, safety and feasibility trial of high-dose omega3 fatty acids and high-dose cholecalciferol supplementation in type 1 diabetes. CellR4 Repair Replace Regen Reprogram 2018, 6, e2489. [Google Scholar]
- Chen, C.; Cohrs, C.M.; Stertmann, J.; Bozsak, R.; Speier, S. Human beta cell mass and function in diabetes: Recent advances in knowledge and technologies to understand disease pathogenesis. Mol. Metab. 2017, 6, 943–957. [Google Scholar] [CrossRef]
- Greenbaum, C.J. A Key to T1D Prevention: Screening and Monitoring Relatives as Part of Clinical Care. Diabetes 2021, 70, 1029–1037. [Google Scholar] [CrossRef]
- Haller, M.J.; Gitelman, S.E.; Gottlieb, P.A.; Michels, A.W.; Perry, D.J.; Schultz, A.R.; Hulme, M.A.; Shuster, J.J.; Zou, B.; Wasserfall, C.H.; et al. Antithymocyte Globulin Plus G-CSF Combination Therapy Leads to Sustained Immunomodulatory and Metabolic Effects in a Subset of Responders With Established Type 1 Diabetes. Diabetes 2016, 65, 3765–3775. [Google Scholar] [CrossRef]
- Haller, M.J.; Schatz, D.A.; Skyler, J.S.; Krischer, J.P.; Bundy, B.N.; Miller, J.L.; Atkinson, M.A.; Becker, D.J.; Baidal, D.; DiMeglio, L.A.; et al. Low-Dose Anti-Thymocyte Globulin (ATG) Preserves β-Cell Function and Improves HbA1c in New-Onset Type 1 Diabetes. Diabetes Care 2018, 41, 1917–1925. [Google Scholar] [CrossRef]
- Quattrin, T.; Haller, M.J.; Steck, A.K.; Felner, E.I.; Li, Y.; Xia, Y.; Leu, J.H.; Zoka, R.; Hedrick, J.A.; Rigby, M.R.; et al. Golimumab and Beta-Cell Function in Youth with New-Onset Type 1 Diabetes. N. Engl. J. Med. 2020, 383, 2007–2017. [Google Scholar] [CrossRef] [PubMed]
- Rigby, M.R.; Hayes, B.; Li, Y.; Vercruysse, F.; Hedrick, J.A.; Quattrin, T. Two-Year Follow-up from the T1GER Study: Continued Off-Therapy Metabolic Improvements in Children and Young Adults with New-Onset T1D Treated with Golimumab and Characterization of Responders. Diabetes Care 2023, 46, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Orban, T.; Bundy, B.; Becker, D.J.; DiMeglio, L.A.; Gitelman, S.E.; Goland, R.; Gottlieb, P.; Greenbaum, C.J.; Marks, J.B.; Monzavi, R.; et al. Co-stimulation modulation with abatacept in patients with recent-onset type 1 diabetes: A randomised, double-blind, placebo-controlled trial. Lancet 2011, 378, 412–419. [Google Scholar] [CrossRef]
- Van Belle, T.L.; Nierkens, S.; Arens, R.; von Herrath, M.G. Interleukin-21 Receptor-Mediated Signals Control Autoreactive T Cell Infiltration in Pancreatic Islets. Immunity 2012, 36, 1060–1072. [Google Scholar] [CrossRef]
- von Herrath, M.; Bain, S.C.; Bode, B.; Clausen, J.O.; Coppieters, K.; Gaysina, L.; Gumprecht, J.; Hansen, T.K.; Mathieu, C.; Morales, C.; et al. Anti-interleukin-21 antibody and liraglutide for the preservation of β-cell function in adults with recent-onset type 1 diabetes: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Diabetes Endocrinol. 2021, 9, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Todd, J.A.; Evangelou, M.; Cutler, A.J.; Pekalski, M.L.; Walker, N.M.; Stevens, H.E.; Porter, L.; Smyth, D.J.; Rainbow, D.B.; Ferreira, R.C.; et al. Regulatory T Cell Responses in Participants with Type 1 Diabetes after a Single Dose of Interleukin-2: A Non-Randomised, Open Label, Adaptive Dose-Finding Trial. PLoS Med. 2016, 13, e1002139. [Google Scholar] [CrossRef]
- Seelig, E.; Howlett, J.; Porter, L.; Truman, L.; Heywood, J.; Kennet, J.; Arbon, E.L.; Anselmiova, K.; Walker, N.M.; Atkar, R.; et al. The DILfrequency study is an adaptive trial to identify optimal IL-2 dosing in patients with type 1 diabetes. JCI Insight 2018, 3, e99306. [Google Scholar] [CrossRef]
- Marcovecchio, M.L.; Wicker, L.S.; Dunger, D.B.; Dutton, S.J.; Kopijasz, S.; Scudder, C.; Todd, J.A.; Johnson, P.R.V. Interleukin-2 Therapy of Autoimmunity in Diabetes (ITAD): A phase 2, multicentre, double-blind, randomized, placebo-controlled trial. Wellcome Open Res. 2020, 5, 49. [Google Scholar] [CrossRef]
- Herold, K.C.; Gitelman, S.E.; Ehlers, M.R.; Gottlieb, P.A.; Greenbaum, C.J.; Hagopian, W.; Boyle, K.D.; Keyes-Elstein, L.; Aggarwal, S.; Phippard, D.; et al. Teplizumab (Anti-CD3 mAb) Treatment Preserves C-Peptide Responses in Patients With New-Onset Type 1 Diabetes in a Randomized Controlled Trial. Diabetes 2013, 62, 3766–3774. [Google Scholar] [CrossRef] [PubMed]
- Herold, K.C.; Hagopian, W.; Auger, J.A.; Poumian-Ruiz, E.; Taylor, L.; Donaldson, D.; Gitelman, S.E.; Harlan, D.M.; Xu, D.; Zivin, R.A.; et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N. Engl. J. Med. 2002, 346, 1692–1698. [Google Scholar] [CrossRef] [PubMed]
- Perdigoto, A.L.; Network, T.I.T.; Preston-Hurlburt, P.; Clark, P.; Long, S.A.; Linsley, P.S.; Harris, K.M.; Gitelman, S.E.; Greenbaum, C.J.; Gottlieb, P.A.; et al. Treatment of type 1 diabetes with teplizumab: Clinical and immunological follow-up after 7 years from diagnosis. Diabetologia 2019, 62, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, C.; Williams, S.R.; del Toro, R.; Pozzilli, P. Efficacy and safety of otelixizumab use in new-onset type 1 diabetes mellitus. Expert. Opin. Biol. 2016, 16, 841–846. [Google Scholar] [CrossRef]
- Nagy, G.; Szekely, T.E.; Somogyi, A.; Herold, M.; Herold, Z. New therapeutic approaches for type 1 diabetes: Disease-modifying therapies. World J. Diabetes 2022, 13, 835–850. [Google Scholar] [CrossRef]
- Xiao, X.; Guo, P.; Shiota, C.; Zhang, T.; Coudriet, G.M.; Fischbach, S.; Prasadan, K.; Fusco, J.; Ramachandran, S.; Witkowski, P.; et al. Endogenous Reprogramming of Alpha Cells into Beta Cells, Induced by Viral Gene Therapy, Reverses Autoimmune Diabetes. Cell Stem Cell 2018, 22, 78–90.e4. [Google Scholar] [CrossRef]
- Zammit, N.W.; Walters, S.N.; Seeberger, K.L.; O’Connell, P.J.; Korbutt, G.S.; Grey, S.T. A20 as an immune tolerance factor can determine islet transplant outcomes. JCI Insight 2019, 4, e131028. [Google Scholar] [CrossRef]
- Grey, S.T.; Arvelo, M.B.; Hasenkamp, W.; Bach, F.H.; Ferran, C. A20 Inhibits Cytokine-Induced Apoptosis and Nuclear Factor κB–Dependent Gene Activation in Islets. J. Exp. Med. 1999, 190, 1135–1146. [Google Scholar] [CrossRef]
- Winkler, C.; Schober, E.; Ziegler, A.G.; Holl, R.W. Markedly reduced rate of diabetic ketoacidosis at onset of type 1 diabetes in relatives screened for islet autoantibodies. Pediatr. Diabetes 2012, 13, 308–313. [Google Scholar] [CrossRef]
- Dickinson, J.A.; Pimlott, N.; Grad, R.; Singh, H.; Szafran, O.; Wilson, B.J.; Groulx, S.; Thériault, G.; Bell, N.R. Screening: When things go wrong. Can. Fam. Physician 2018, 64, 502–508. [Google Scholar]
- Sherwood, J.S.; Russell, S.J.; Putman, M.S. New and Emerging Technologies in Type 1 Diabetes. Endocrinol. Metab. Clin. N. Am. 2020, 49, 667–678. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Types of prevention according to T1D stages.

Figure 2.
Main prevention and treatment options for different stages of T1D.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ingrosso, D.M.F.; Quarta, M.T.; Quarta, A.; Chiarelli, F. Prevention of Type 1 Diabetes in Children: A Worthy Challenge? Int. J. Environ. Res. Public Health 2023, 20, 5962. https://doi.org/10.3390/ijerph20115962
AMA Style
Ingrosso DMF, Quarta MT, Quarta A, Chiarelli F. Prevention of Type 1 Diabetes in Children: A Worthy Challenge? International Journal of Environmental Research and Public Health. 2023; 20(11):5962. https://doi.org/10.3390/ijerph20115962
Chicago/Turabian StyleIngrosso, Diletta Maria Francesca, Maria Teresa Quarta, Alessia Quarta, and Francesco Chiarelli. 2023. "Prevention of Type 1 Diabetes in Children: A Worthy Challenge?" International Journal of Environmental Research and Public Health 20, no. 11: 5962. https://doi.org/10.3390/ijerph20115962
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.