Pediatric Asthma Emergency Room Visits (ERV) Risks
There have been many studies to investigate the PM-related asthma effects, but only a few have focused its attention on the emergency room visits (ERV) for children (less than 18 years of age) [
14,
21]. Asthma is a chronic disease that has plagued this country since the Industrial Revolution. Over 5.3 million children, less than 18 years of age, in the United States suffer from asthma and it accounts for one in six pediatric emergency room visits [
18]. The unit risk methodology utilized in this assessment can be found in a paper by Levy et al., 2002 [
13]. They were interpreted from the data provided in two previous pediatric asthma ERV investigations. The unit risk for PM
2.5 exposures is .01 or 1% per unit increase (measured in μg/m
3). The unit risk for PM
10 exposures is .007 or .7% per unit increase. Levy et al. pooled the two studies (Norris and Tolbert) performed in Seattle and in Atlanta using a random effects model (i.e. without consideration of race, socioeconomic status, and/or gender) to generate these unit risk factors. They were based upon youth (≤ 18 years of age) for daily PM
2.5 measurements. Thus, we have executed ADD
pot (potential average
daily dose) calculations for our PM measurements.
Bearing in mind that the targeted population in this assessment is youth (0–17 years of age), the body weight and inhalation rate representative of these individuals must be implemented into both the ADD
pot and SFI. The ED and AT for non-carcinogenic effects (i.e. asthma ERV) are equal (ED = AT) and thus, cancel each other out [
23]. The body weight, 33.7 kg, is a weighted average spanning from birth until 18 years of age using Table 7-2 of the US EPA Exposure Factors Handbook (EFH). The inhalation rate, 1.2 m
3/hr, was taken from Table 5–23 of the EFH allowing for a moderate sense of outdoor activity during a short-term exposure. Considering these factors, a sample potential dose calculation performed for PM
2.5 exposure is shown below:
Using the site-averaged conditions of Ward 4 during the summer IOP and the specifics mentioned above,
equation 2 and
equation 3 becomes …
Resulting in an individual risk (R
i) value of …
Upon further review, it is shown that the individual risk is in fact a very simple calculation that does not need to take into account both the body weight and inhalation rate because they are accounted for in the unit risk factor of inhalation. Therefore,
equation 4 becomes R
i = C × UR for non-carcinogenic evaluation, where C = C
youth (5.85 μg/m
3). This C is the PM
2.5 mass concentration that the youth are exposed to [the total PM
2.5 concentration is factorized for the youth population in Ward 4, C
youth = C
W4 × .212 (the percentage of youth in ward 4)].
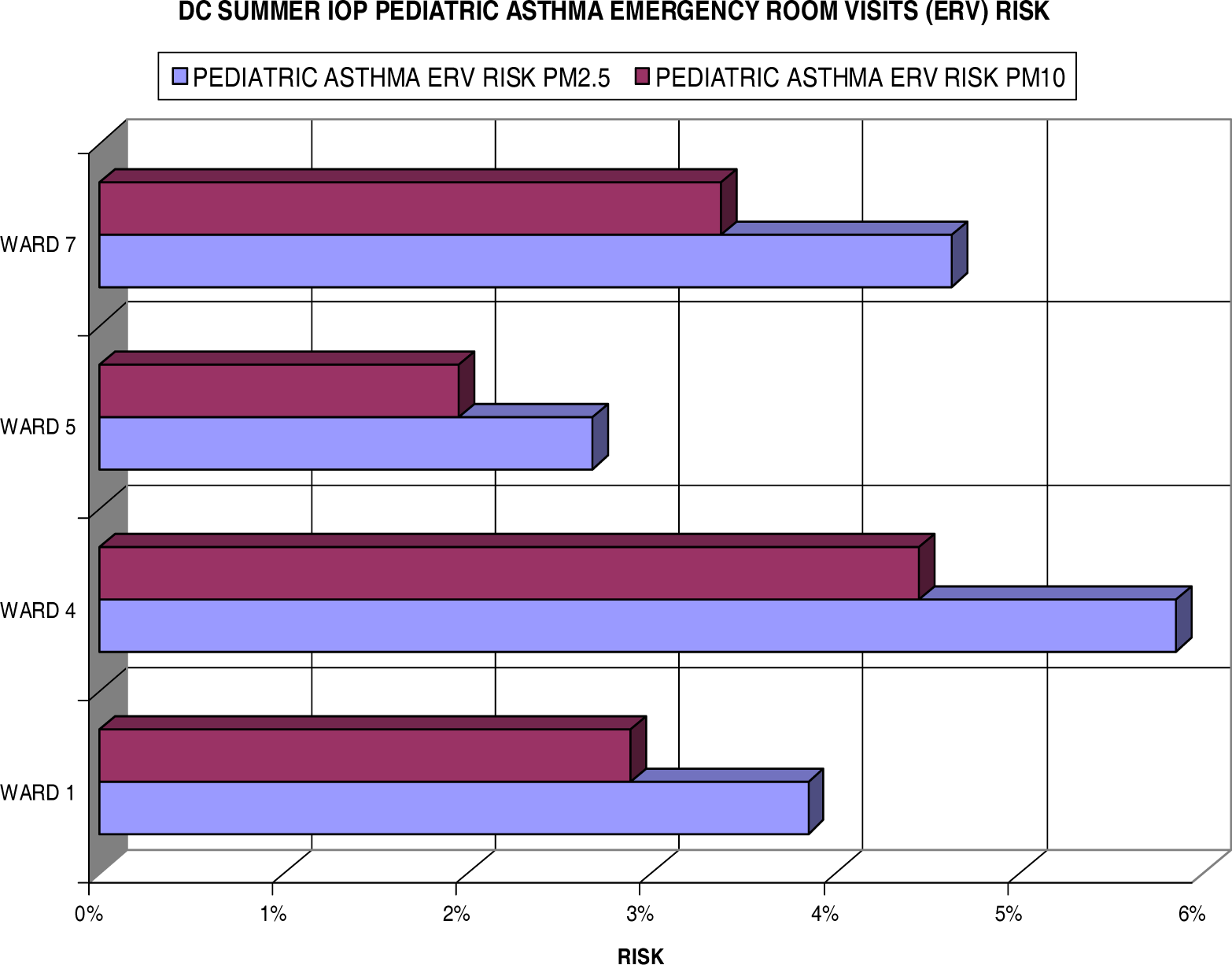
Figure 7 displays the individual risks for these inhabitants of each ward measured in the summer IOP. Most notably, all wards reflect some degree (> 2.5%) of excess risk for pediatric asthma ERV when exposed to fine particulate. Ward 4 showed greater than a 5.8% increase risk in ERV for children with asthma with PM
2.5 exposure and greater than 4% with PM
10 exposure. Ward 7 also showed a health concern to its residents with a 4.6% and 3.3% risk for the fine and coarse particulate (PM
10) respectively. Ward 1 had a slightly lower risk of 3.8% for PM
2.5 and 2.9% for the larger particulate. Ward 5, still significant, only measured a 2.7% increase in risk per unit of fine particulate and less than 2% in the PM
10 size.
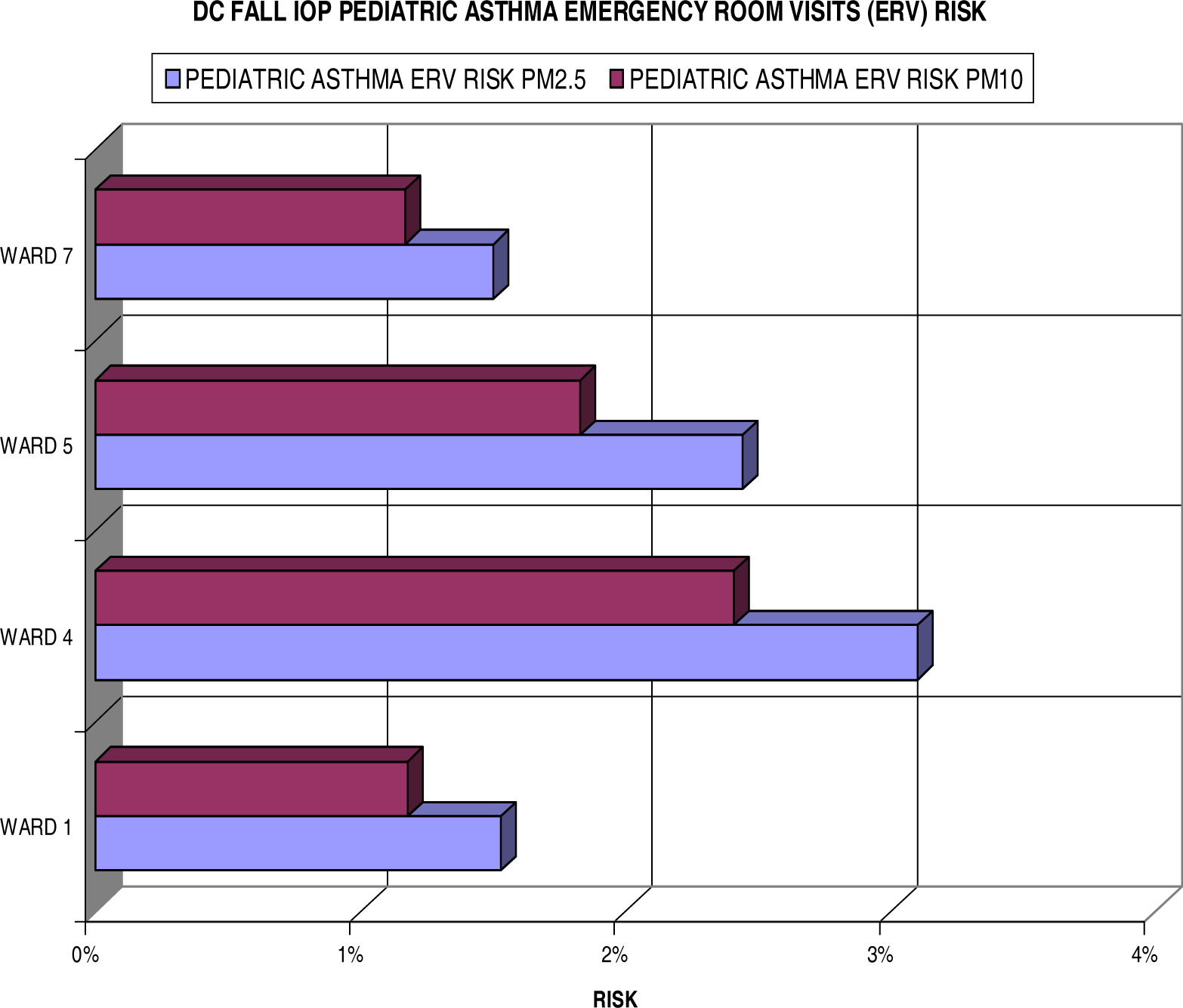
Figure 8 shows the results of individual risks for the fall IOP. In comparison, it clearly shows lower risk in the fall results than the summer IOP. The highest increased risk, found in Ward 4, does not exceed the 4% mark measuring 3.1% for PM
2.5. More interesting, Ward 7 is far less of a concern for pediatric asthma ERV due to risks at only 1.5% and 1.2% for the fine and coarse particulates respectively. Ward 5 exceeds the risks of Ward 1 by 0.9% and 0.6% for the PM
2.5 and PM
10.
Using
equation 5, these individual risk values may be converted into new cases of pediatric asthma ERV or the number of persons that may be affected by the exposure in a specified population. According to the 2000 DC State Data Center report [
10], the population of youth (under 18 years of age) for Wards 1, 4, 5, and 7 in Washington, DC was 63,540 in total, as shown in
Table 1.
The results of these calculations for POP
risk are listed in
tables 2 and
3 for the summer and fall IOP respectively. They show that Ward 4 is more of a concern for pediatric asthma yielding over 900 new cases of ERV for fine particulates in the summer and over 480 in the fall, whereas Ward 7 appears to be a seasonal threat (over 890 new ERV in the summer months and 291 in the fall). This seasonal variability appears to be as common for Ward 1 with a 60% drop in cases during the fall IOP, whereas ERV for pediatric asthma is more constant during both IOPs for Ward 5 with an approximate 7% reduction in the fall.
Lung Cancer Risks
Outdoor air, particularly in densely populated urban environments, contains a variety of known human carcinogens [
2]. In this study, we are investigating five carcinogens (three known and two probable) as classified by the US EPA. It is understood that the exposure to human carcinogens in outdoor air is often the result of proximity to more localized sources, such as power plants, welding shops, auto body shops, municipal facilities, and areas with high traffic volume. These sorts of locations and their associated PM distributions are plotted in figure 30 for the selected areas in DC. Evaluating
equation 2 for the specified carcinogen and relating it to corresponding SFI values can reveal the individual lifetime lung cancer risks for the exposed population. This provides an estimate of the probability that an individual will develop lung cancer over a 70-year lifetime if exposed to a particular carcinogen at the measured concentrations continually. However, adjustments must be made to the averaging time (AT) to account for this exposure period, AT = 70 years. Thus,
equation 2 becomes the following for the potential lifetime average daily dose (LADD
pot) for cancer assessment:
Accordingly, the individual lifetime cancer risk (R
ic) becomes:
We have assumed exposure duration (ED) of 91 days/year for a 70 year period, equating 6,370 days for a lifetime (seasonal) exposure to contaminants. Converting AT into days results in 25,550 days for a lifetime period. The US EPA usually assumes a non-threshold dose-response for carcinogens (i.e. some finite risk no matter how small the dose) [
23].
Commonly speaking, cancer risks vary by particular stages in life. They are typically higher from early-life exposure than from similar exposure durations later in life [
23]. These particular differences in dose and exposure of chemical concentrations in air often result from intake (inhalation rates), metabolism, and/or absorption rates. Thus, it is deemed necessary to include exposure that is measured for all stages of life (baby, child, and adult) according to the US EPA Child-Specific Exposure Factors Handbook (2002). These stages are accounted for utilizing age dependent adjustment factors (ADAF):
▪ For exposures before 2 years of age (spanning a 2 year interval from birth up until child’s second birthday), there is a 10-fold ADAF
▪ For exposures between 2 and 15 years of age (spanning a 14 year period from a child’s second birthday up until their sixteenth birthday), there is a 3-fold ADAF
▪ For exposures between 16 and up, no adjustments are needed
I would like to clarify that the time period, two six-week IOPs, of this study is not considered adequate to establish a one-to-one causal relationship between cancer rates and fine PM emissions in DC, as in a cohort or case-control study, but was rather utilized to compare ward-specific PM levels with public health effects and calculate the individual risks for both pediatric asthma emergency room visits and the onset of (lung) cancer.
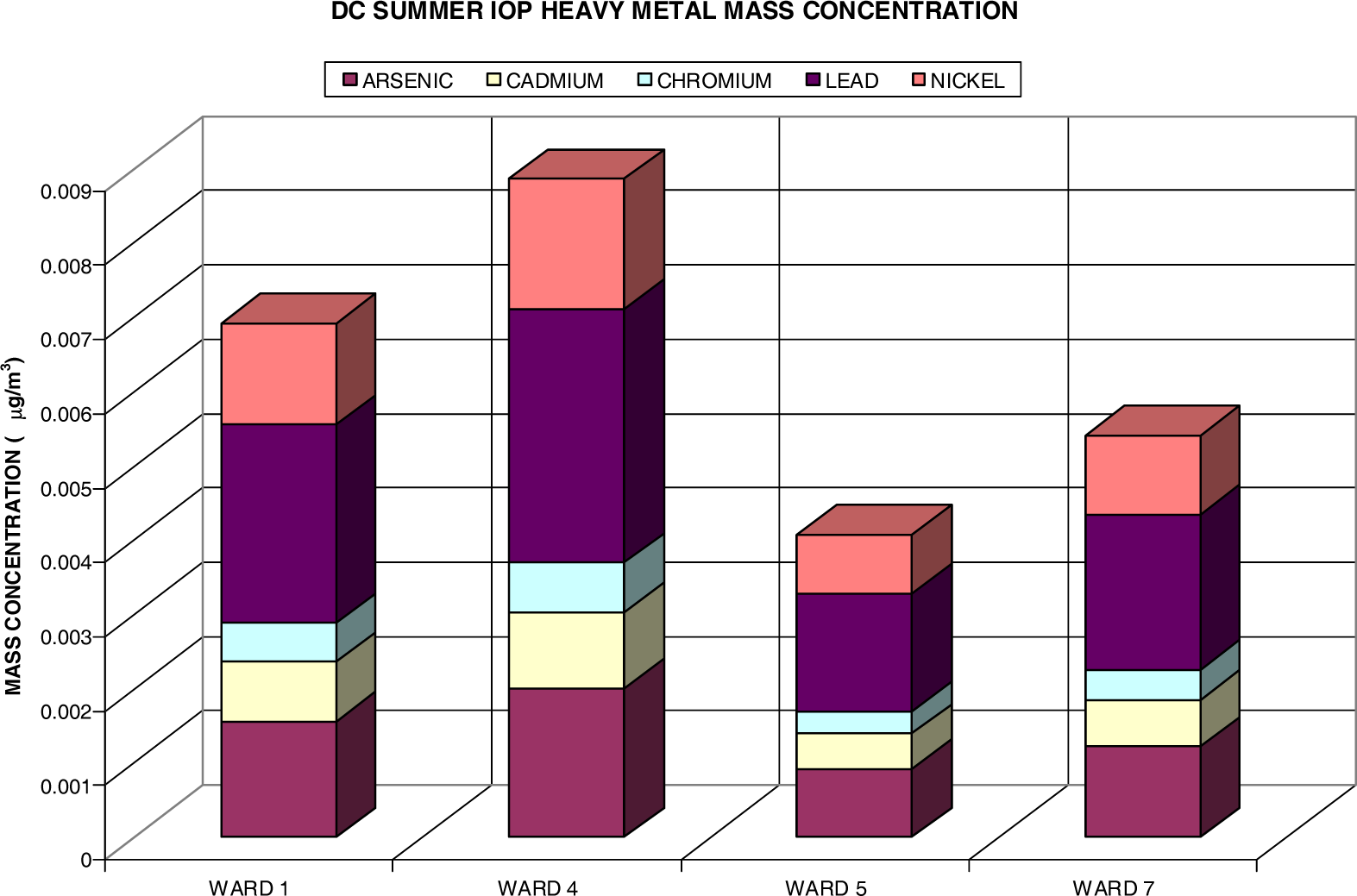
The unit risks (UR) for the three known carcinogens (As, Cr, and Ni) and one probable human carcinogen (Cd) are defined by the US EPA Integrated Risk Information System (IRIS) (
www.epa.gov/iris/). The unit risk for lead (Pb), the Group B2 probable carcinogen, was determined from the Office of Environmental Health Hazard Assessment (
http://www.oehha.ca.gov/pdf/hsca2.pdf; page 331). The unit risk for PM
2.5, which encompasses many more heavy metals, volatile organic carbons (VOCs), and various other constituents not investigated in this research, is according to Pope et al. (2002) [
16]. All values are displayed in
Table 4. The UR for hexavalent chromium [Cr (VI)] and nickel subsulfide was used. Incorporating these UR values into equation 7 reveals the R
ic for the contaminants (PM
2.5, As, Cd, Cr, Pb, and Ni). A sample calculation of these values is shown below:
For residents in Ward 1, the R
ic via exposure to As is determined as …
However, this is not the actual lifetime risk. The ADAF values must be applied to properly assess the lifetime risk over numerous stages.
For baby (0 to 2 years) stage,
For child (2 years to 15 years) stage,
For adult (16 years to 70 years) stage,
Thus, the actual lifetime individual risk (R
ic) is the combination of these lifestage risk values (R
b, R
c, and R
a):
| Ric | 2.87 × 10−6 or 2.9 per 1 million |
Individual lifetime cancer risks (by wards) are displayed in
figures 9,
10, and
11 for the summer and fall IOP.
Figure 9 shows the calculated risks for both IOPs regarding a unit increase in PM
2.5. The data reflects a clear distinction between summer and fall risks with the excess risk for cancer via exposure during the summer months (2.5 in 10) nearly doubling relative to the fall season (1.3 in 10). Particularly, Ward 4 (8.9 in 100) and Ward 1 (7 in 100) surpassed the other two wards for PM-related health effects during the summer IOP. Ward 7 showed a threefold increase to outdoor pollution with 5.5 in 100 (summer) and 1.8 in 100 (fall). However, to gain a more accurate measurement for exposure over a long-term period, such as the time interval for the onset of cancer, it is best to average over the seasonal risks. Therefore, the seasonally-averaged (averaged over summer and fall IOP) individual lifetime cancer risk for each ward is as follows: 4.9 in 100 (Ward 1), 6.8 in 100 (Ward 4), 3.9 in 100 (Ward 5), and 3.7 in 100 (Ward 7).
It should be noted that any cancer risk less than 1×10
−6 (1 in a million, marked by the bold red line in
figures 10 and
11) is considered negligible by the US EPA.
Figure 10 shows the lifetime excess lung cancer risks in the selected four wards in DC. As expected with this methodology, one observes the same distribution pattern as in
figure 9 for the summer IOP fine particulates. Ward 4 has the highest risks for all constituents. This is followed by Ward 1, Ward 7, and then Ward 5. The leading heavy metals are persistently arsenic and chromium. This is primarily due to the content level of the arsenic present in the samples and to the high unit risk of chromium as denoted in
table 4. This indicates that these carcinogens are the most threatening to the population exposed to them in Wards 1, 4, 5, and 7, in which Ward 4 poses an excess risk of 3.5×10
−6 for As and 3.3×10
−6 for Cr. In essence, all wards provided a lifetime excess risk value beyond the threshold (1 in a million) for both As and Cr. The Pb (not present on the chart due to low values) and Ni were negligible estimates at all points.
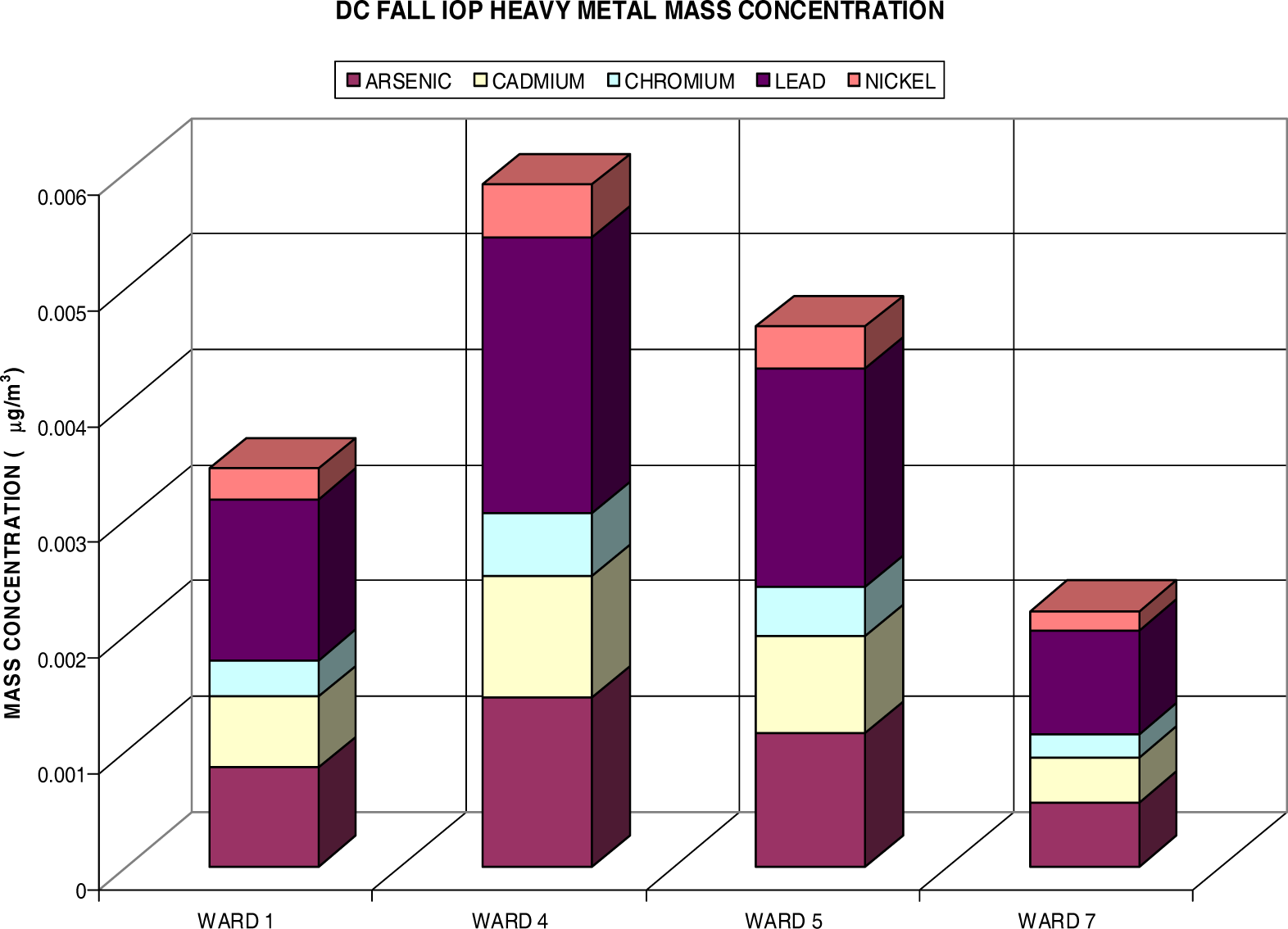
Figure 11 also reflects the distribution of PM
2.5. Ward 4 again exceeds all others in lifetime risk vales, followed by Ward 5, Ward 1, and Ward 7. The lifetime excess risk is now greatest for Cr and followed by As. The largest Cr and As values, nearly equal, are once again evident in Ward 4 at 2.6×10
−6 (Cr) and 2.55×10
−6 (As). All wards, except Ward 7, exceed the threshold levels for both Cr and As. Ward 7 barely missed the 1 per million threshold with .96×10
−6 (As) and .99×10
−6 (Cr). Ni and Pb are insignificant contributors in this assessment for (lung) cancer risks, which helps bring the focus to arsenic and chromium for more stringent limitations on the DC area industrial emissions. It also identifies Ward 4 residents at an increased risk within the DC area. Coincidentally, the average cancer deaths from 1995–2002 say the same with the highest average of 245.5 for Ward 4.
It was mentioned earlier that the effects of air pollution may vary widely across subpopulations. Both
figures 12 and
13 take this point into consideration. When reflecting on
table 1, there is a considerate amount of disparity amongst subgroups in the DC area, specifically in the chosen wards. In reference to Wards 1, 4, 5, and 7, the black population of DC is 74.7%, the white population is 15.2%, and the Hispanic population is 10.3%. The age population is 21.9% youth, 64% adults, and 14.1 % elderly Washingtonians. The female population is 47% and the male population is 53%. In efforts to analyze the disparity among subpopulations in DC, the lifetime excess lung cancer risks have been calculated for these groups individually.
Figure 12 shows the individual risk for eight DC subpopulations amongst the four chosen wards during the summer IOP. At first glance, it is noteworthy that the black, adult, and female populations are at most risk for the development of (lung) cancer with a unit increase in both As and Cr. In the subgroups, Ni and Pb are of very low concern with values well below the 1×10
−6 benchmark. Cd presents an individual risk above 1×10
−6 for both blacks and females. Overall, As poses a serious health threat to blacks with a 7.2 in a million individual risk for cancer development. Cr closely aligns this with 6.7×10
−6. The Hispanic and elderly populations appear to be least likely at risk for lifetime lung cancer development. Moreover, the white population, although it bears risk values pass the threshold mark for both Cr and As, is of no comparison to the black population risk with greater than a 4-fold difference. These findings are also consistent with actual statistics in which blacks in DC exceed the national average for lung cancer rates at 69.8 per 100,000 persons, whereas whites have a rate of 39.3 per 100,000 (
www.cdc.gov/cancer/CancerBurden/dc.htm). Although the risks for youth and elderly do not appear as threatening individually, when combined with other subgroups, they too are at risk over a lifetime exposure. For instance, arsenic poses a risk of 8.31×10
−6 for the black youth and 7.23×10
−6 for the black elderly versus a risk of 2.81×10
−6 for the white youth and 1.73×10
−6 for the white elderly population. It is apparent that the elderly do not appear to have a significant at risk value due to their exposure length. It is factored into the risk equation that the elderly population has only a 6-year exposure interval (65–70 years). Additionally, the elderly population only account for 14.1% of the total ward population.
Figure 13 shows data for the fall IOP. With the exception that Cr surpassed As for all subpopulations, the distribution of individual risks closely mirrors that observed in the summer. The black, female, and adult subgroups emulate that of individual risks in
figure 12 having the highest risks topping about 5.3×10
−6 for blacks exposed to Cr. The Hispanic and youth populations have once more fallen behind the one in a million thresholds. Once again, combining subgroups yield much higher individual risks for the development of lung cancer over a lifetime. Exposure to chromium has established risks of 6.2×10
−6 for the black youth and 5.38×10
−6 for the black elderly, whereas these risks are far less for the white youth (1.9×10
−6) and white elderly (1.22×10
−6) populations.
Like the pediatric asthma ERV excess cases that are displayed in
tables 2 and
3, the estimated number of new cancer cases or the population at risk for the onset of cancer can be calculated using
equation 5. Utilizing the figures from
table 1, the demographics for our subpopulations can be determined and implemented into the equation. The results are shown in
tables 5 and
6. Most effectively, it tells that black DC residents may develop 3.5, adult residents may develop 1.2, male residents may develop 1.4, and female residents may develop 1.8 new cases of (lung) cancer in the period of a lifetime when exposed to levels of contaminants found in the summer IOP. Coincidentally, blacks may develop 2.7, adults nearly 1, males may develop 1.1, and females 1.4 new lung cancer cases if continuously exposed to carcinogens (As, Cd, Cr, Pb, an d Ni) at the concentrations measured during the fall IOP. Merging these two subgroups can result in a considerable health risk to black adults of 4.7 lifetime excess cases utilizing the summer IOP exposures and 3.6 new incidences when exposed to the fall IOP concentrations. Even more impactful black male adults may develop 6.1 and black female adults may develop 6.5 new lung cancer cases when exposed to contaminants in the summer IOP. Thus, combination of these risks yields even more concern for all subgroups. The white, Hispanic, and elderly groups are independently considered minor with new cases below 0.5. However, white adults actually measure an individual risk of 1.4 (summer IOP) and 1.04 (fall IOP) excess lung cancer cases over a lifetime exposure to the carcinogens presented in this study.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}