
Efficacy of Varenicline in the Treatment of Alcohol Dependence: An Updated Meta-Analysis and Meta-Regression
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection and Data Extraction
2.3. Quality Assessment
2.4. Outcomes and Statistical Analysis
3. Results
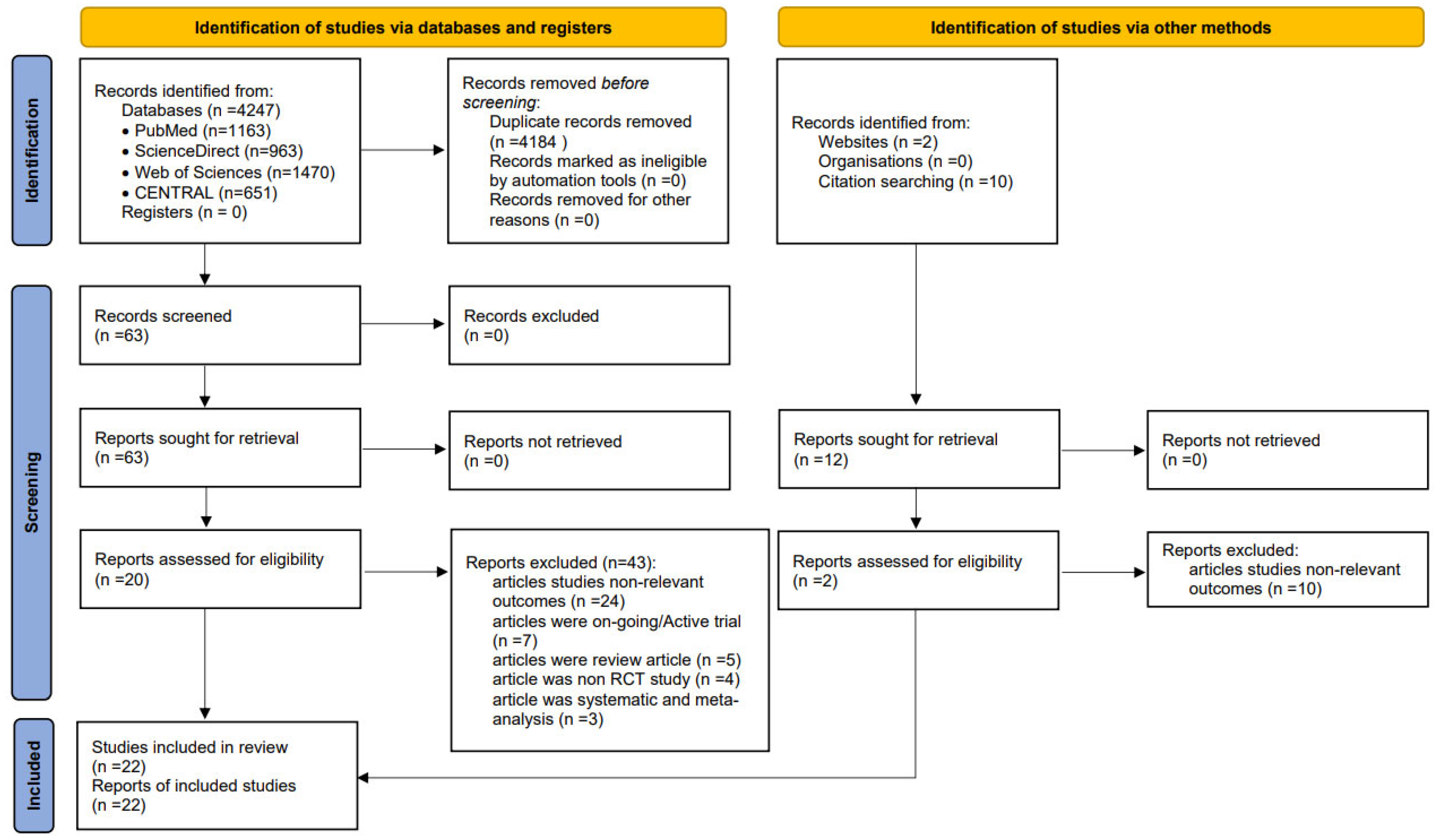
3.1. Study Search and Selection
3.2. Study Characteristics
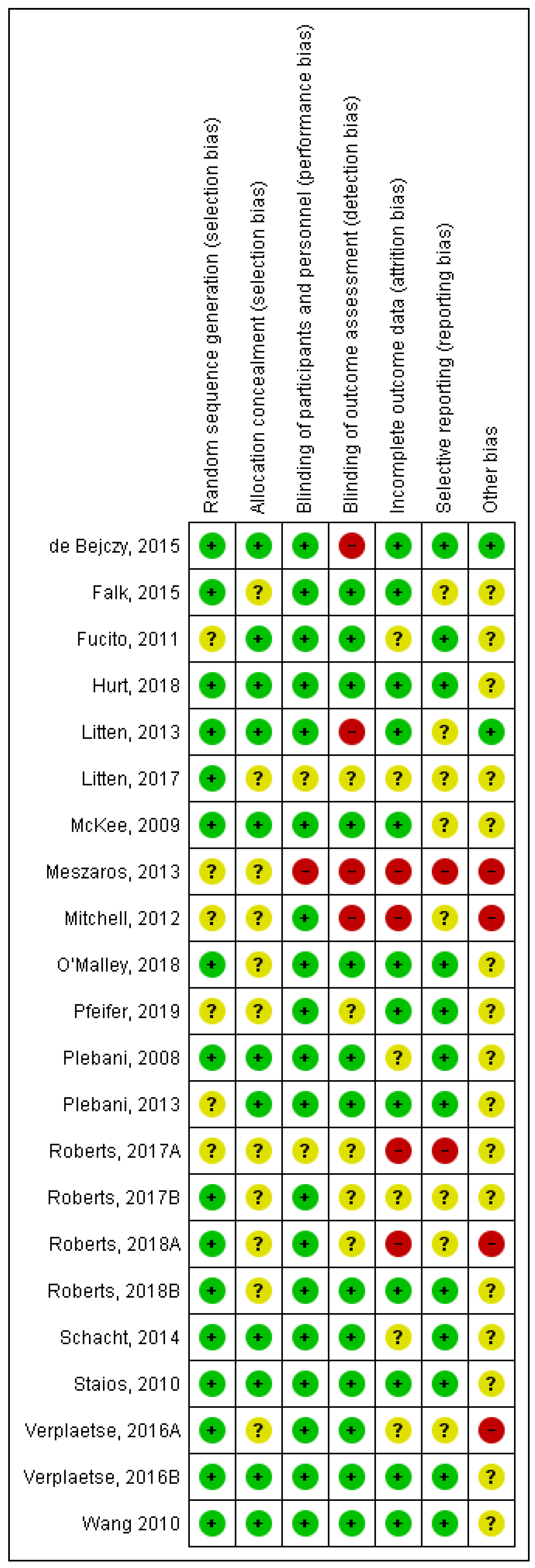
3.3. ROB in Included Trials
3.4. Clinical Outcomes
3.4.1. Primary Outcomes
Abstinence Rate
Percentage of Abstinent Days
Percentage of Drinking Days
Percentage of Heavy Drinking Days
Drinks per Day
Drinks per Drinking Day
Alcohol Intoxication
Alcohol Craving Evaluation
3.4.2. Secondary Outcome: AE
3.4.3. Sensitivity Analysis
3.4.4. Subgroup Analysis
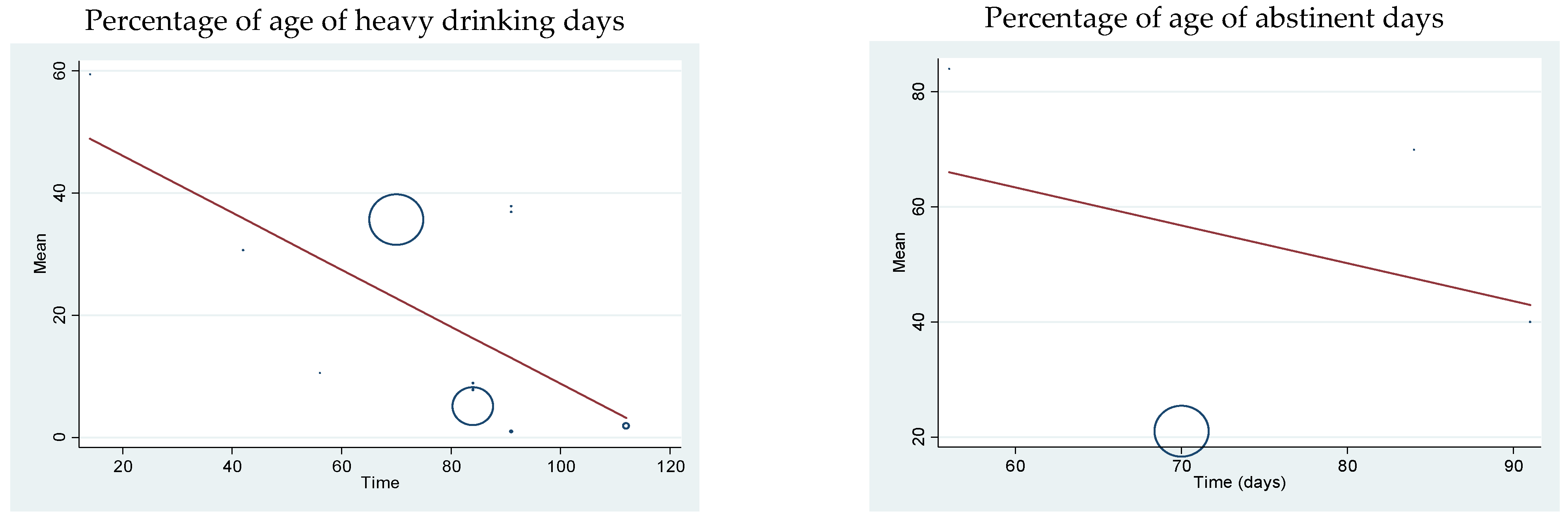
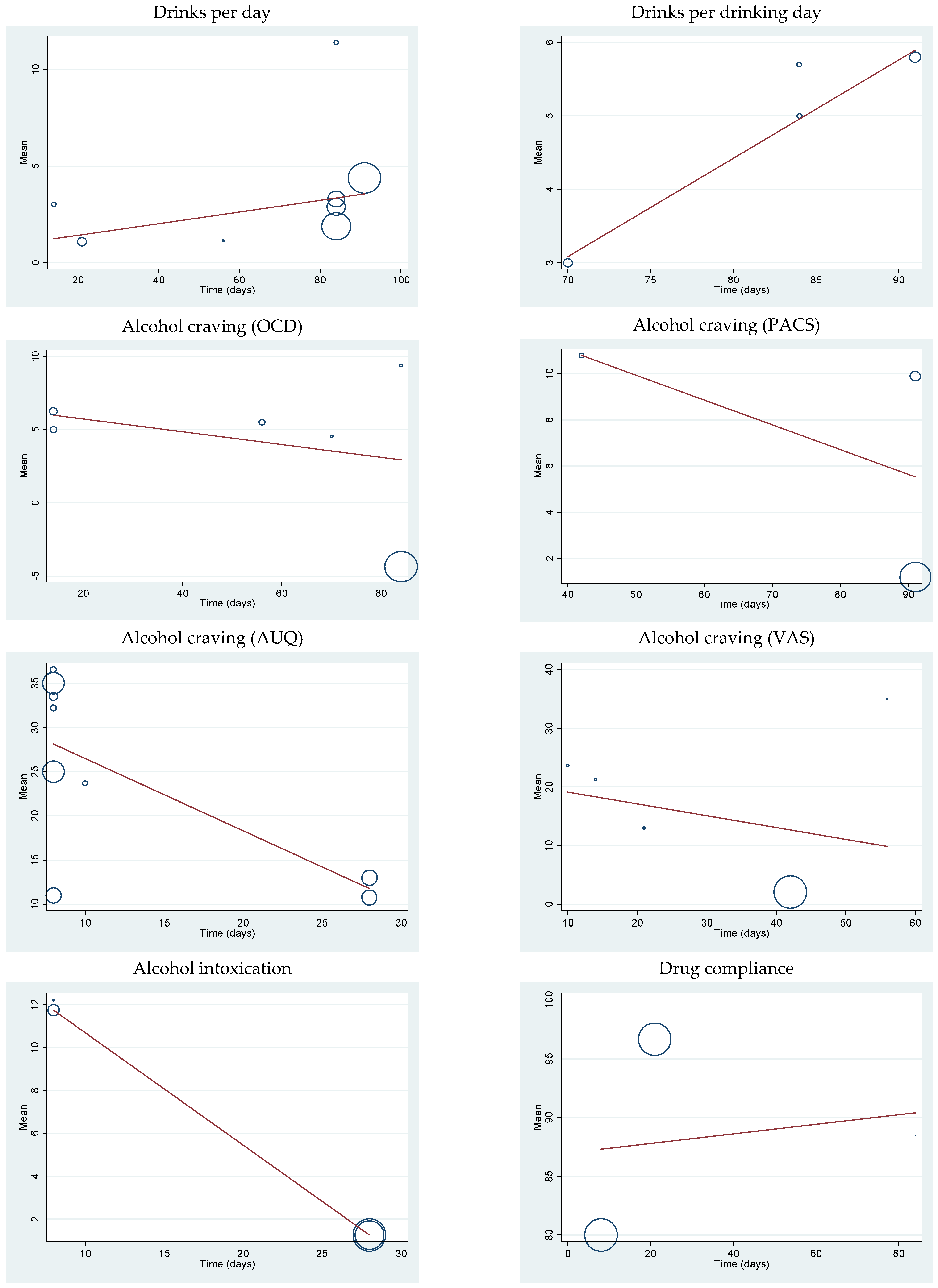
3.4.5. Meta-Regression
3.4.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
- Study Protocol
- Review Question
- Searches
- Types of studies included
- Condition or domain studied
- Participants/population
- Intervention(s), exposure(s)
- Comparators/control
- Context
- Data extraction (Selection and coding)
- Risk of bias (quality) assessment
- Strategy for data synthesis
- Analysis of subgroups or subsets
- Meta-regression
- Anticipated or actual start date
- Anticipated completion date
- Funding sources/sponsors
- Conflicts of interest
- Language
- Country
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Location | Study Duration | Participants | Age (Years) | Intervention/ Comparator (N) | Outcomes | AE Reported | Jadad Score |
|---|---|---|---|---|---|---|---|---|
| Pfeifer et al., (2019) [10] | Germany | 84 days | alcohol and nicotine dependence patients (N = 28) | 45.0 ± 8.12 |
| Percentage ofage of days without alcohol consumption, number of standardized drinks per day, percentage ofage of heavy drinking days, and alcohol craving (OCD scale) | ✓ | 4 |
| Roberts et al., (2017) [15] | USA | 8 days | heavy drinking tobacco users (N = 30) | 33.59 ± 9.86 |
| Alcohol craving (AUQ scale) and subjective alcohol intoxication effects | ✓ | 5 |
| Hurt et al., (2018) [11] | USA | 84 days | drinking smokers (N = 33) | 39.5 ± 11.15 |
| Number of heavy drinking days, average drinks per day, average drinks per drinking day, and number of drinking days | ✓ | 4 |
| Roberts et al., (2018) [38] | USA | 10 days | heavy drinkers (with smokers or nonsmokers) (N = 77) | 34.26 ± 9.78 |
| Alcohol-cue-induced craving (AUQ scale) | ✕ | 3 |
| Verplaetse et al., (2016) [17] | USA | 28 days | alcohol abuse or alcohol dependence patients (N = 44) | 33.78 ± 9.02 |
| Alcohol craving (AUQ scale) and alcohol intoxication | ✕ | 3 |
| Roberts et al., (2018) [39] | USA | 8 days | Alcohol abuse or dependence patients (N = 55) | 34.26 ± 9.78 |
| ad-libitum alcohol consumption and total number of drinks | ✕ | 5 |
| O’Malley et al., (2018) [14] | USA | 112 days | Alcohol-dependent smokers (N = 131) | 42.75 ± 11.75 |
| Percentage ofage of heavy drinking days | ✓ | 5 |
| Verplaetse et al., (2016) [40] | USA | 8 days | Alcohol consumers (N = 60) | 33.90 ± 9.88 |
| Alcohol craving (AUQ scale) and number of Ad-libitum drinks in drinking period | ✓ | 5 |
| de Bejczy et al., (2015) [18] | Sweden | 70 days | Alcohol-dependent subjects (N = 171) | 55.10 ± 7.99 |
| Proportion of heavy drinking days, proportion of abstaining days, alcohol consumption drinks per drinking day, and alcohol craving (OCD scale) | ✓ | 5 |
| Litten et al., (2017) [41] | USA | 42 days | Alcohol drinkers (N = 47) | ≥21 years |
| Percentage of heavy drinking days, Percentage ofage of age of subjects abstinent during the last month of treatment, and Alcohol craving (Penn alcohol craving scale (PACS)) | ✓ | 4 |
| Mitchell et al., (2012) [28] | USA | 84 days | Social smoking drinkers (N = 64) | 27.0 ± 7.63 |
| alcoholic drinks per week, alcohol craving (OCD scale), and cumulative alcoholic drinks consumed | ✓ | 5 |
| Plebani et al., (2013) [29] | USA | 84 days | Alcoholism patients (N = 40) | 18–70 years |
| Rate of heavy drinking days per week and addiction severity index (ASI) | ✓ | 4 |
| Schacht et al., (2014) [16] | USA | 14 days | Drinkers seeking treatment (N = 35) | 30.25 ± 8.15 |
| percentage ofage of heavy drinking days and alcohol craving (OCD scale) | ✓ | 4 |
| Falk et al., (2015) [30] | USA | 91 days | Alcohol dependence patients (N = 200) | 48.1 ± 6.7 |
| Percentage ofage of heavy drinking days | ✕ | 5 |
| Litten et al., (2013) [31] | USA | 91 days | Alcohol dependent patients (N = 198) | 45.5 ± 12.1 |
| Percentage ofage of heavy drinking days, drinks per day, drinks per drinking day, percentage ofage of very heavy drinking days, percentage ofage of abstinent days, percentage ofage of subjects abstinent, percentage ofage of subjects with no heavy drinking days, alcohol craving (PACS scale), alcohol-related consequences (ImBIBe score), and quality of life (SF-12 physical/mental aggregate score) | ✓ | 5 |
| Staios (2010) [32] | USA | 21 days | Treatment seeking smokers, mild drinkers (N = 24) | 33.17 ± 9.91 |
| cue-induced craving after exposure to alcohol cues, self-reported changes in consumption of alcohol (drinks per day), and overall craving alcohol | ✓ | 5 |
| Roberts et al., (2017) [33] | USA | 8 days | Depressed-alcohol heavy drinkers (N = 60) | 33.75 ± 10.69 |
| Ad-libitum alcohol consumption, alcohol craving before drinking (tonic craving), and alcohol craving after drinking (AUQ scale) | ✕ | 3 |
| Plebani et al., (2008) [37] | USA | 91 days | Alcohol dependent patients (N = 40) | 46.45 ± 11.4 |
| Week days of alcohol use, presence/absence of alcohol use, numbers of heavy drinking days presence/absence of heavy drinking, alcohol craving (PACS scale), and addiction severity index (ASI) | ✕ | 4 |
| Fucito et al., (2011) [34] | USA | 56 days | Heavy drinking smokers (N = 30) | 43.12 ± 8.26 |
| Percentage ofage of heavy drinking days, percentage ofage of abstinent days, alcohol craving (OCD scale), and alcohol sedating effect | ✓ | 5 |
| McKee et al., (2009) [9] | USA | 8 days | Non-alcohol-dependent heavy drinkers (N = 20) | 34.75 ± 12.4 |
| Number of drinks consumed during Ad-libitum period, alcohol craving (AUQ scale), and alcohol intoxication effects | ✓ | 5 |
| Meszaros et al., (2013) [35] | USA | 56 days | Schizophrenia alcoholic and smoking patients (N = 10) | 43.0 ± 7.0 |
| Number of standard drinks consumed per week, percentage ofage of abstinent days from alcohol a month, and alcohol craving | ✓ | 2 |
| Wang (2010) [36] | Canada | 14 days | Tobacco dependence and Heavy alcohol users (N = 24) | 36.10 ± 11.30 |
| visual analogue scale in tobacco-alcohol cues (VAS), obsessive compulsive drinking scale (OCDS), and alcoholic drinks consumed per day | ✓ | 5 |
Appendix C
| Outcomes | No. of Trial | Effect Size | 95% CI | I2 (%) | P for Effect Size | Pa | |
|---|---|---|---|---|---|---|---|
| (1) Abstinent rate | |||||||
| Treatment duration (days) | |||||||
| 30–90 | 1 | 0.52 | 0.11, 2.58 | N/A | 0.42 | N/A | |
| >90 | 1 | 1.04 | 0.15, 7.25 | N/A | 0.97 | N/A | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 2 | 0.70 | 0.21, 2.35 | 0.0% | 0.56 | 0.59 | |
| Participants’ characteristic | |||||||
| AD | 2 | 0.70 | 0.21, 2.35 | 0.0% | 0.56 | 0.59 | |
| (2) Percentage ofage of drinking days | |||||||
| Treatment duration (days) | |||||||
| 30–90 | 2 | −0.10 | −0.58, 0.38 | 0.0% | 0.69 | 0.90 | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 2 | −0.10 | −0.58, 0.38 | 0.0% | 0.69 | 0.90 | |
| Participants’ characteristic | |||||||
| AD | 2 | −0.10 | −0.58, 0.38 | 0.0% | 0.69 | 0.90 | |
| (3) Percentage ofage of heavy drinking days | |||||||
| Treatment duration (days) | |||||||
| <30 | 1 | 0.10 | −0.56, 0.77 | N/A | 0.76 | N/A | |
| 30–90 | 6 | −0.29 | −2.19, 1.61 | 98% | 0.78 | <0.00001 | |
| >90 | 4 | −0.02 | −0.28, 0.23 | 54% | 0.86 | 0.09 | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 8 | −0.01 | −0.98, 0.96 | 97% | 0.99 | <0.00001 | |
| Low (30–59 g/d) | 1 | −0.79 | −1.53, −0.04 | N/A | 0.04 * | N/A | |
| N/A | 2 | −0.08 | −0.56, 0.39 | 0.0% | 0.73 | 0.84 | |
| Participants’ characteristic | |||||||
| AD | 7 | −0.06 | −1.35, 1.24 | 98% | 0.93 | <0.00001 | |
| AD with smoking | 4 | −0.10 | −0.37, 0.17 | 9.0% | 0.47 | 0.36 | |
| (4) Percentage ofage of abstinent days | |||||||
| Treatment duration (days) | |||||||
| 30–90 | 3 | 5.71 | −2.64, 14.07 | 99% | 0.18 | <0.00001 | |
| >90 | 1 | 0.14 | −0.14, 0.42 | N/A | 0.33 | N/A | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 2 | 8.76 | −8.19, 25.70 | 100% | 0.31 | <0.00001 | |
| Low (30–59 g/d) | 1 | 0.05 | −1.19, 1.29 | N/A | 0.94 | N/A | |
| N/A | 1 | −0.18 | −0.93, 0.56 | N/A | 0.63 | N/A | |
| Participants’ characteristic | |||||||
| AD | 2 | 8.76 | −8.19, 25.70 | 100% | 0.31 | <0.00001 | |
| AD with smoking | 2 | −0.12 | −0.76, 0.52 | 0.0% | 0.71 | 0.75 | |
| (5) Drinks per day | |||||||
| Treatment duration (days) | |||||||
| ≤30 | 2 | −0.03 | −0.60, 0.54 | 0.0% | 0.92 | 0.97 | |
| 30–90 | 4 | −0.31 | −0.61, −0.00 | 0.0% | 0.05 | 0.78 | |
| >90 | 1 | −0.22 | −0.50, 0.06 | N/A | 0.12 | N/A | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 2 | −0.23 | −0.47, 0.02 | 0.0% | 0.07 | 0.99 | |
| Low (30–59 g/d) | 4 | −0.13 | −0.49, 0.22 | 0.0% | 0.47 | 0.96 | |
| N/A | 1 | −0.77 | −1.55, 0.00 | N/A | 0.05 | N/A | |
| Participants’ characteristic | |||||||
| AD | 1 | −0.22 | −0.50, 0.06 | N/A | 0.12 | N/A | |
| AD with smoking | 6 | −0.24 | −0.51, 0.03 | 0.0% | 0.08 | 0.87 | |
| (6) Drinks per drinking day | |||||||
| Treatment duration (days) | |||||||
| 30–90 | 2 | −0.25 | −0.51, 0.01 | 44% | 0.06 | 0.17 | |
| >90 | 1 | −0.24 | −0.52, 0.04 | N/A | 0.09 | N/A | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 3 | −0.24 | −0.44, −0.05 | 16% | 0.01 * | 0.31 | |
| Participants’ characteristic | |||||||
| AD | 2 | 0.17 | −0.38, 0.03 | 0.0% | 0.10 | 0.49 | |
| AD with smoking | 1 | −0.62 | −1.33, 0.08 | N/A | 0.08 | N/A | |
| (7) Alcohol craving (OCDS) | |||||||
| Treatment duration (days) | |||||||
| <30 | 2 | 0.02 | −1.53, 1.49 | 87% | 0.98 | 0.005 | |
| 30–90 | 4 | −0.33 | −0.84, 0.19 | 72% | 0.21 | 0.001 | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 2 | −0.37 | −1.00, 0.27 | 66% | 0.26 | 0.09 | |
| Low (30–59 g/d) | 3 | −0.02 | −1.12, 1.08 | 87% | 0.97 | 0.0004 | |
| N/A | 1 | −0.42 | −1.17, 0.33 | N/A | 0.27 | N/A | |
| Participants’ characteristic | |||||||
| AD | 2 | −0.37 | −1.00, 0.27 | 66% | 0.26 | 0.09 | |
| AD with smoking | 4 | −0.13 | −0.93, 0.66 | 81% | 0.74 | 0.001 | |
| (8) Alcohol craving (PACS) | |||||||
| Treatment duration (days) | |||||||
| 30–90 | 1 | −0.02 | −0.59, 0.55 | N/A | 0.95 | N/A | |
| >90 | 2 | −0.42 | −0.68, −0.16 | 46% | 0.001 * | 0.17 | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 2 | −0.28 | −0.53, −0.03 | 0.0% | 0.03 * | 0.32 | |
| N/A | 1 | −0.84 | −1.49, −0.19 | N/A | 0.01 * | N/A | |
| Participants’ characteristic | |||||||
| AD | 3 | −0.35 | −0.59, −0.12 | 42% | 0.003 * | 0.18 | |
| (9) Alcohol craving (AUQ) | |||||||
| Varenicline dose | |||||||
| 1 mg/day | 3 | −1.11 | −2.35, 0.13 | 88% | 0.08 | 0.0002 | |
| 2 mg/day | 3 | −1.59 | −2.56, −0.62 | 89% | 0.001 * | <0.00001 | |
| Treatment duration (days) | |||||||
| <30 | 6 | −1.41 | −2.12, −0.71 | 87% | <0.0001 * | <0.00001 | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 4 | −1.41 | −2.26, −0.56 | 88% | 0.001 * | <0.00001 | |
| Low (30–59 g/d) | 2 | −1.58 | −3.99, 0.82 | 91% | 0.20 | 0.0006 | |
| Participants’ characteristic | |||||||
| AD | 4 | −1.72 | −2.65, −0.79 | 89% | 0.0003 * | <0.00001 | |
| AD with smoking | 2 | −0.46 | −0.87, −0.06 | 0.0% | 0.02 * | 0.78 | |
| (10) Alcohol craving (VAS) | |||||||
| Treatment duration (days) | |||||||
| <30 | 3 | −0.34 | −0.70, 0.01 | 0.0% | 0.06 | 0.72 | |
| 30–90 | 2 | −0.07 | −0.59, 0.45 | 0.0% | 0.79 | 0.88 | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 1 | −0.05 | −0.62, 0.52 | N/A | 0.86 | N/A | |
| Low (30–59 g/d) | 4 | −0.33 | −0.67, 0.01 | 0.0% | 0.06 | 0.86 | |
| (11) Alcohol intoxication | |||||||
| Varenicline dose | |||||||
| 1 mg/day | 1 | −0.88 | −1.65, −0.10 | N/A | 0.03 * | N/A | |
| 2 mg/day | 3 | −0.87 | −1.76, 0.03 | 76% | 0.06 | 0.006 | |
| Treatment duration (days) | |||||||
| <30 | 3 | −0.87 | −1.76, 0.03 | 76% | 0.06 | 0.006 | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 2 | −0.50 | −1.25, 0.25 | 62% | 0.19 | 0.07 | |
| Low (30–59 g/d) | 1 | −2.29 | −3.47, −1.11 | N/A | 0.0001 * | N/A | |
| Participants’ characteristic | |||||||
| AD | 2 | −1.22 | −1.98, −0.46 | 57% | 0.002 * | 0.10 | |
| AD with smoking | 1 | 0.36 | −0.55, 1.26 | N/A | 0.44 | N/A | |
| (12) Drug compliance | |||||||
| Treatment duration (days) | |||||||
| <30 | 2 | 1.61 | −1.61, 4.82 | 94% | 0.33 | <0.0001 | |
| 30–90 | 1 | 0.00 | −0.74, 0.74 | N/A | 1.00 | N/A | |
| Alcohol consumption level risk | |||||||
| Medium (60–89 g/d) | 1 | 0.00 | −0.90, 0.90 | N/A | 1.00 | N/A | |
| Low (30–59 g/d) | 1 | 3.28 | 1.99, 4.58 | N/A | <0.00001 * | N/A | |
| N/A | 1 | 0.00 | −0.74, 0.74 | N/A | 1.00 | N/A | |
| Participants’ characteristic | |||||||
| AD | 1 | 3.28 | 1.99, 4.58 | N/A | <0.00001 * | N/A | |
| AD with smoking | 2 | 0.00 | −0.57, 0.57 | 0.0% | 1.00 | 1.00 | |
Appendix D


References
- World Health Organization. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2018; Volume 1, pp. 38–115.
- World Health Organization. Epidemiology of Alcohol Use in the WHO South-East Asia Region; World Health Organization, Regional Office for South-East Asia: New Delhi, India, 2017; Volume 1, pp. 1–32.
- Rehm, J. The Risks Associated with Alcohol Use and Alcoholism. Alcohol Res. Health 2011, 34, 135–143. [Google Scholar] [PubMed]
- Saunders, J.B.; Degenhardt, L.; Reed, G.M.; Poznyak, V. Alcohol Use Disorders in ICD-11: Past, Present, and Future. Alcohol. Clin. Exp. Res. 2019, 43, 1617–1631. [Google Scholar] [CrossRef] [PubMed]
- Lundin, A.; Waern, M.; Löve, J.; Lövestad, S.; Hensing, G.; Danielsson, A.-K. Towards ICD-11 for Alcohol Dependence: Diagnostic Agreement with ICD-10, DSM-5, DSM-IV, DSM-III-R and DSM-III Diagnoses in a Swedish General Population of Women. Drug Alcohol Depend. 2021, 227, 108925. [Google Scholar] [CrossRef]
- Kaewpramkusol, R.; Senior, K.; Chenhall, R.; Nanthamongkolchai, S.; Chaiyasong, S. A Qualitative Exploration of Thai Alcohol Policy in Regulating Availability and Access. Int. J. Drug Policy 2018, 58, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaiyasong, S.; Jankhotkaew, J.; Nasueb, S.; Markchang, K.; Jindarattanaporn, N.; Saramunee, K. Thailand Alcohol Policy Model Development. Available online: https://cas.or.th/wp-content/uploads/2019/07/22.59-A1-0018_APM_final-report_-20190305.pdf (accessed on 1 November 2021).
- Babor, T.; Caetano, R.; Casswell, S.; Edwards, G.; Giesbrecht, N.; Graham, K. Alcohol: No Ordinary Commodity—Research and Public Policy, 2nd ed.; Blackwell Publishing Ltd.: Oxford, UK, 2010. [Google Scholar]
- McKee, S.A.; Harrison, E.L.R.; O’Malley, S.S.; Krishnan-Sarin, S.; Shi, J.; Tetrault, J.M.; Picciotto, M.R.; Petrakis, I.L.; Estevez, N.; Balchunas, E. Varenicline Reduces Alcohol Self-Administration in Heavy-Drinking Smokers. Biol. Psychiatry 2009, 66, 185–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfeifer, P.; Fehr, C. Efficacy of Varenicline in Patients with Severe Alcohol Dependence. J. Clin. Psychopharmacol. 2019, 39, 398–402. [Google Scholar] [CrossRef]
- Hurt, R.T.; Ebbert, J.O.; Croghan, I.T.; Schroeder, D.R.; Hurt, R.D.; Hays, J.T. Varenicline for Tobacco-Dependence Treatment in Alcohol-Dependent Smokers: A Randomized Controlled Trial. Drug Alcohol Depend. 2018, 184, 12–17. [Google Scholar] [CrossRef]
- Oon-Arom, A.; Likhitsathain, S.; Srisurapanont, M. Efficacy and Acceptability of Varenicline for Alcoholism: A Systematic Review and Meta-Analysis of Randomized-Controlled Trials. Drug Alcohol Depend. 2019, 205, 107631. [Google Scholar] [CrossRef]
- Gandhi, K.D.; Mansukhani, M.P.; Karpyak, V.M.; Schneekloth, T.D.; Wang, Z.; Kolla, B.P. The Impact of Varenicline on Alcohol Consumption in Subjects With Alcohol Use Disorders. J. Clin. Psychiatry 2020, 81, 19r12924. [Google Scholar] [CrossRef]
- O’Malley, S.S.; Zweben, A.; Fucito, L.M.; Wu, R.; Piepmeier, M.E.; Ockert, D.M.; Bold, K.W.; Petrakis, I.; Muvvala, S.; Jatlow, P.; et al. Effect of Varenicline Combined with Medical Management on Alcohol Use Disorder with Comorbid Cigarette Smoking. JAMA Psychiatry 2018, 75, 129. [Google Scholar] [CrossRef] [Green Version]
- Roberts, W.; Harrison, E.L.R.; McKee, S.A. Effects of Varenicline on Alcohol Cue Reactivity in Heavy Drinkers. Psychopharmacology 2017, 234, 2737–2745. [Google Scholar] [CrossRef] [PubMed]
- Schacht, J.P.; Anton, R.F.; Randall, P.K.; Li, X.; Henderson, S.; Myrick, H. Varenicline Effects on Drinking, Craving and Neural Reward Processing among Non-Treatment-Seeking Alcohol-Dependent Individuals. Psychopharmacology 2014, 231, 3799–3807. [Google Scholar] [CrossRef] [Green Version]
- Verplaetse, T.L.; Pittman, B.P.; Shi, J.M.; Tetrault, J.M.; Coppola, S.; McKee, S.A. Effect of Lowering the Dose of Varenicline on Alcohol Self-Administration in Drinkers with Alcohol Use Disorders. J. Addict. Med. 2016, 10, 166–173. [Google Scholar] [CrossRef]
- de Bejczy, A.; Löf, E.; Walther, L.; Guterstam, J.; Hammarberg, A.; Asanovska, G.; Franck, J.; Isaksson, A.; Söderpalm, B. Varenicline for Treatment of Alcohol Dependence: A Randomized, Placebo-Controlled Trial. Alcohol. Clin. Exp. Res. 2015, 39, 2189–2199. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the Quality of Reports of Randomized Clinical Trials: Is Blinding Necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Comparison of Two Methods to Detect Publication Bias in Meta-Analysis. JAMA 2006, 295, 676–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. A Basic Introduction to Fixed-Effect and Random-Effects Models for Meta-Analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef]
- Mitchell, J.M.; Teague, C.H.; Kayser, A.S.; Bartlett, S.E.; Fields, H.L. Varenicline Decreases Alcohol Consumption in Heavy-Drinking Smokers. Psychopharmacology 2012, 223, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Plebani, J.G.; Lynch, K.G.; Rennert, L.; Pettinati, H.M.; O’Brien, C.P.; Kampman, K.M. Results from a Pilot Clinical Trial of Varenicline for the Treatment of Alcohol Dependence. Drug Alcohol Depend. 2013, 133, 754–758. [Google Scholar] [CrossRef] [Green Version]
- Falk, D.E.; Castle, I.-J.P.; Ryan, M.; Fertig, J.; Litten, R.Z. Moderators of Varenicline Treatment Effects in a Double-Blind, Placebo-Controlled Trial for Alcohol Dependence. J. Addict. Med. 2015, 9, 296–303. [Google Scholar] [CrossRef] [Green Version]
- Litten, R.Z.; Ryan, M.L.; Fertig, J.B.; Falk, D.E.; Johnson, B.; Dunn, K.E.; Green, A.I.; Pettinati, H.M.; Ciraulo, D.A.; Sarid-Segal, O.; et al. A Double-Blind, Placebo-Controlled Trial Assessing the Efficacy of Varenicline Tartrate for Alcohol Dependence. J. Addict. Med. 2013, 7, 277–286. [Google Scholar] [CrossRef] [Green Version]
- Staios, G. Effect of Varenicline vs. Placebo on Reactivity to Tobacco and Alcohol Cues in Smokers Who Are Light Drinkers. Ph.D. Thesis, University of Toronto, Toronto, ON, Canada, 2010. [Google Scholar]
- Roberts, W.; Verplaetse, T.L.; Moore, K.; Oberleitner, L.; Picciotto, M.R.; McKee, S.A. Effects of Varenicline on Alcohol Self-Administration and Craving in Drinkers with Depressive Symptoms. J. Psychopharmacol. 2017, 31, 906–914. [Google Scholar] [CrossRef]
- Fucito, L.M.; Toll, B.A.; Wu, R.; Romano, D.M.; Tek, E.; O’Malley, S.S. A Preliminary Investigation of Varenicline for Heavy Drinking Smokers. Psychopharmacology 2011, 215, 655–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meszaros, Z.S.; Abdul-Malak, Y.; Dimmock, J.A.; Wang, D.; Ajagbe, T.O.; Batki, S.L. Varenicline Treatment of Concurrent Alcohol and Nicotine Dependence in Schizophrenia. J. Clin. Psychopharmacol. 2013, 33, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Wang, S. Effects of Varenicline on Cue-Reactivity in Individuals with Concurrent Tobacco Dependence and Heavy Alcohol Use: A Randomized, Double-Blind, Placebo-Controlled Trial. Ph.D. Thesis, University of Toronto, Toronto, ON, Canada, 2010. [Google Scholar]
- Plebani, J. Varenicline (ChantixTM) for the Treatment of Alcohol Dependence (ChA) (Online). National Institute on Drug Abuse (NIDA). Available online: https://clinicaltrials.gov/ct2/show/results/NCT00705523 (accessed on 15 August 2021).
- Roberts, W.; McKee, S.A. Effects of Varenicline on Cognitive Performance in Heavy Drinkers: Dose-Response Effects and Associations with Drinking Outcomes. Exp. Clin. Psychopharmacol. 2018, 26, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.; Shi, J.M.; Tetrault, J.M.; McKee, S.A. Effects of Varenicline Alone and in Combination with Low-Dose Naltrexone on Alcohol-Primed Smoking in Heavy-Drinking Tobacco Users: A Preliminary Laboratory Study. J. Addict. Med. 2018, 12, 227–233. [Google Scholar] [CrossRef]
- Verplaetse, T.L.; Pittman, B.P.; Shi, J.M.; Tetrault, J.M.; Coppola, S.; McKee, S.A. Effect of Varenicline Combined with High-Dose Alcohol on Craving, Subjective Intoxication, Perceptual Motor Response, and Executive Cognitive Function in Adults with Alcohol Use Disorders: Preliminary Findings. Alcohol. Clin. Exp. Res. 2016, 40, 1567–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litten, R. Human Laboratory Study of Varenicline for Alcohol Use Disorder (Online). National Institute on Alcohol Abuse and Alcoholism (NIAAA). Available online: https://clinicaltrials.gov/ct2/show/results/NCT03035708 (accessed on 15 August 2021).
- Erwin, B.L.; Slaton, R.M. Varenicline in the Treatment of Alcohol Use Disorders. Ann. Pharmacother. 2014, 48, 1445–1455. [Google Scholar] [CrossRef] [PubMed]
- Swan, G.E.; Javitz, H.S.; Jack, L.M.; Wessel, J.; Michel, M.; Hinds, D.A.; Stokowksi, R.P.; McClure, J.B.; Catz, S.L.; Richards, J.; et al. Varenicline for Smoking Cessation: Nausea Severity and Variation in Nicotinic Receptor Genes. Pharmacogenom. J. 2012, 12, 349–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, R.L.; Zekarias, A.; Caduff-Janosa, P. Varenicline and Abnormal Sleep Related Events. Sleep 2015, 38, 833–837. [Google Scholar] [CrossRef] [Green Version]
- Garbutt, J.C.; Kampov-Polevoy, A.B.; Gallop, R.; Kalka-Juhl, L.; Flannery, B.A. Efficacy and Safety of Baclofen for Alcohol Dependence: A Randomized, Double-Blind, Placebo-Controlled Trial. Alcohol. Clin. Exp. Res. 2010, 34, 1849–1857. [Google Scholar] [CrossRef] [Green Version]
- Mann, K.; Lehert, P.; Morgan, M.Y. The Efficacy of Acamprosate in the Maintenance of Abstinence in Alcohol-Dependent Individuals: Results of a Meta-Analysis. Alcohol. Clin. Exp. Res. 2004, 28, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Anthenelli, R.M.; Benowitz, N.L.; West, R.; St Aubin, L.; McRae, T.; Lawrence, D.; Ascher, J.; Russ, C.; Krishen, A.; Evins, A.E. Neuropsychiatric Safety and Efficacy of Varenicline, Bupropion, and Nicotine Patch in Smokers with and without Psychiatric Disorders (EAGLES): A Double-Blind, Randomised, Placebo-Controlled Clinical Trial. Lancet 2016, 387, 2507–2520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorenby, D.E. Efficacy of Varenicline, an A4β2 Nicotinic Acetylcholine Receptor Partial Agonist, vs Placebo or Sustained-Release Bupropion for Smoking Cessation—A Randomized Controlled Trial. JAMA 2006, 296, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brezner, I. Proposed Mechanism for Drug-Induced Nightmares. Sci. J. Lander Coll. Arts Sci. 2011, 4, 75–84. [Google Scholar]
- European Medicines Agency Nitrosamines in Varenicline: Questions and Answers. Available online: https://www.ema.europa.eu/en/documents/referral/nitrosamines-emea-h-a53-1490-questions-answers-marketing-authorisation-holders/applicants-chmp-opinion-article-53-regulation-ec-no-726/2004-referral-nitrosamine-impurities-human-medicinal-products_en.pdf (accessed on 16 January 2023).
- Lang, A.E.; Patel, U.; Fitzpatrick, J.; Lee, T.; McFarland, M.; Good, C.B. Association of the Chantix Recall With US Prescribing of Varenicline and Other Medications for Nicotine Dependence. JAMA Netw. Open 2023, 6, e2254655. [Google Scholar] [CrossRef] [PubMed]


| Outcomes | Main Analysis | References |
|---|---|---|
| Abstinent rate | RR = 0.70 (95% CI: 0.21, 2.35; p = 0.56); I2 = 0.0% (FE) | [31,41] |
| Percentage of abstinent days | SMD = 4.20 days (0.21, 8.19; p = 0.04); I2 = 99.0% * (RE) | [10,17,18,31] |
| Percentage of drinking days | SMD = −0.10 days (−0.58, 0.38; p = 0.69); I2 = 0.0% (FE) | [11] |
| Percentage of heavy drinking days | SMD = −0.07 days (−0.85, 0.71; p = 0.87); I2 = 96.0% (RE) | [10,11,14,16,18,29,30,31,34,37,41] |
| Drinks per day | SMD = −0.23 drinks (−0.43, −0.04; p = 0.02); I2 = 0.0% * (FE) | [10,11,28,31,32,35,36] |
| Drinks per drinking day | SMD = −0.24 drinks (−0.44, −0.05; p = 0.01); I2 = 16.0% * (FE) | [11,18,31] |
| Alcohol intoxication | SMD = −0.87 drinks (−1.76, 0.03; p = 0.06); I2 = 76.0% (RE) | [9,39,40] |
| Alcohol craving (OCDS scale) | SMD = −0.25 (−0.72, 0.22; p = 0.22); I2 = 73.0% (RE) | [16,18,34,36] |
| Alcohol craving (PACS scale) | SMD = −0.35; 95% CI −0.59, −0.12; p = 0.003; I2 = 42.0% * (FE) | [31,37,41] |
| Alcohol craving (AUQ scale) | SMD = −1.41 (−2.12, −0.71; p < 0.00001); I2 = 87.0% * (RE) | [9,15,17,33,39,40] |
| Alcohol craving (VAS) | SMD = −0.26 (−0.55, 0.04; p = 0.09); I2 = 0.0% (FE) | [32,33,35,36,41] |
| Adverse Effect (No. of Studies) | No of Events/ No. of Patients in Varenicline Groups (%) | No of Events/ No. of Patients in Placebo Groups (%) | Pooled Risk Ratio (95% CI) | I2 | Pa |
|---|---|---|---|---|---|
| (1) Gastrointestinal system | |||||
| Nausea/Vomiting (14) | 152/432 (35.19) | 66/425 (15.5) | 2.31 (1.81, 2.96) * | 0.0% | 0.63 |
| Constipation (5) | 14/168 (8.33) | 7/152 (4.61) | 1.68 (0.75, 3.73) | 32% | 0.21 |
| Flatulence (4) | 7/72 (9.72) | 9/51 (17.65) | 0.66 (0.3, 1.45) | 0.0% | 0.94 |
| Abdominal pain (3) | 12/91 (13.19) | 3/98 (3.06) | 3.82 (1.23, 11.84) * | 0.0% | 0.88 |
| Diarrhea (5) | 28/265 (10.57) | 27/282 (9.57) | 1.11 (0.68, 1.82) | 49% | 0.1 |
| Dry mouth (4) | 19/190 (10.00) | 14/180 (7.78) | 1.18 (0.64, 2.16) | 73% | 0.01 |
| Abdominal discomfort (1) | 4/77 (5.19) | 4/83 (4.82) | 1.08 (0.28, 4.16) | N/A | N/A |
| Dysgeusia (1) | 6/96 (6.25) | 1/101 (0.99) | 6.31 (0.77, 51.47) | N/A | N/A |
| Heartburn (1) | 3/12 (25.00) | 0/12 (0.00) | 7.0 (0.40, 122.44) | N/A | N/A |
| (2) Nervous system | |||||
| Headache (9) | 63/344 (18.31) | 61/359 (16.99) | 1.09 (0.80, 1.49) | 0.0% | 0.51 |
| Vivid dream/nightmares (11) | 72/392 (18.37) | 38/389 (9.77) | 1.89 (1.33, 2.69) * | 0.0% | 0.56 |
| Erratic behavior (2) | 0/49 (0.00) | 0/30 (0.00) | N/A | N/A | N/A |
| Insomnia (8) | 35/341 (10.26) | 27/337 (8.01) | 1.25 (0.78, 2.01) | 0.0% | 0.98 |
| Suicidal thoughts (4) | 1/87 (1.15) | 2/66 (3.03) | 0.58 (0.09, 3.90) | 0.0% | 0.57 |
| Depression (6) | 23/222 (10.36) | 20/237 (8.43) | 1.22 (0.7, 2.13) | 0.0% | 0.89 |
| Appetite change (2) | 7/73 (9.59) | 7/77 (9.09) | 1.06 (0.4, 2.79) | 31% | 0.23 |
| Sleep problem (4) | 11/136 (8.09) | 10/141 (7.09) | 1.14 (0.52, 2.49) | 16% | 0.31 |
| Anxiety (5) | 16/207 (7.73) | 18/218 (8.26) | 0.94 (0.5, 1.75) | 4.0% | 0.39 |
| Drowsiness (2) | 11/76 (14.47) | 8/79 (10.13) | 1.42 (0.6, 3.36) | 56% | 0.13 |
| Vertigo (1) | 7/77 (9.09) | 6/83 (7.23) | 1.26 (0.44, 3.58) | N/A | N/A |
| Pyrexia (1) | 1/77 (1.30) | 6/83 (7.23) | 0.18 (0.02, 1.46) | N/A | N/A |
| Seizure (1) | 1/23 (4.35) | 0/24 (0.00) | 3.13 (0.13, 73.01) | N/A | N/A |
| Agitation (3) | 13/152 (8.55) | 18/156 (11.54) | 0.77 (0.4, 1.47) | 0.0% | 0.5 |
| Anger (1) | 2/33 (6.06) | 0/31 (0.00) | 4.71 (0.23, 94.31) | N/A | N/A |
| Aggression (1) | 1/33 (3.03) | 0/31 (0.00) | 2.82 (0.12, 66.82) | N/A | N/A |
| Somnolence (1) | 6/96 (6.25) | 13/101 (12.87) | 0.49 (0.19, 1.23) | N/A | N/A |
| Dizziness (1) | 11/96 (11.46) | 6/101 (5.94) | 1.93 (0.74, 5.01) | N/A | N/A |
| Irritability (2) | 13/101 (12.87) | 8/106 (7.55) | 1.69 (0.76, 3.76) | 58% | 0.12 |
| Hostility (1) | 6/96 (6.25) | 4/101 (3.96) | 1.58 (0.46, 5.42) | N/A | N/A |
| Auditory visual hallucination (1) | 0/5 (0.00) | 1/5 (20.00) | 0.33 (0.02, 6.65) | N/A | N/A |
| Paranoia (1) | 0/5 (0.00) | 1/5 (20.00) | 0.33 (0.02, 6.65) | N/A | N/A |
| (3) Eye/ear/nose/throat (EENT) and respiratory system | |||||
| Difficulty breathing (2) | 2/49 (4.08) | 1/30 (3.33) | 1.29 (0.17, 9.67) | 0.0% | 0.88 |
| Blurred vision (2) | 3/87 (3.45) | 2/91 (2.20) | 1.57 (0.27, 9.05) | 0.0% | 0.71 |
| Rhinorrhea (1) | 8/64 (12.50) | 4/67 (5.97) | 2.09 (0.66, 6.61) | N/A | N/A |
| Shortness of breath (1) | 1/40 (2.50) | 1/20 (5.00) | 0.5 (0.03, 7.59) | N/A | N/A |
| Nasopharyngitis/Upper respiratory tract infection (3) | 27/196 (13.78) | 38/208 (18.27) | 0.76 (0.48, 1.19) | 25% | 0.26 |
| Cough (2) | 1/96 (1.04) | 6/104 (5.77) | 0.25 (0.04, 1.45) | 36% | 0.21 |
| (4) Musculoskeletal system and skin | |||||
| Fatigue (2) | 31/173 (17.92) | 20/184 (10.87) | 1.65 (0.98, 2.78) | 0.0% | 0.43 |
| Arthralgia (2) | 13/173 (7.51) | 16/184 (8.70) | 0.86 (0.43, 1.75) | 47% | 0.17 |
| Back pain (2) | 10/173 (5.78) | 17/184 (9.24) | 0.63 (0.29, 1.33) | 0.0% | 0.74 |
| Body ache (1) | 5/19 (26.32) | 4/21 (19.05) | 1.38 (0.43, 4.4) | N/A | N/A |
| Rash (1) | 3/96 (3.13) | 6/101 (5.94) | 0.53 (0.14, 2.04) | N/A | N/A |
| (5) Circulatory system | |||||
| Chest pain (3) | 1/145 (0.69) | 7/131 (5.34) | 0.21 (0.01, 1.19) | 49% | 0.16 |
| Fast heartbeat (2) | 4/49 (8.16) | 1/30 (3.33) | 1.97 (0.34, 11.47) | 0.0% | 0.68 |
| High blood pressure (2) | 2/24 (8.33) | 4/26 (15.38) | 0.53 (0.11, 2.47) | 0.0% | 0.95 |
| Raynaud phenomenon (1) | 0/5 (0.00) | 1/5 (20.00) | 0.33 (0.02, 6.65) | N/A | N/A |
| (6) Urinary and reproductive system | |||||
| Bright urine (1) | 3/23 (13.04) | 1/24 (4.17) | 3.13 (0.35, 27.96) | N/A | N/A |
| Gynecological bleeding (1) | 1/23 (4.35) | 2/24 (8.33) | 0.52 (0.05, 5.37) | N/A | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phimarn, W.; Sakhancord, R.; Paitoon, P.; Saramunee, K.; Sungthong, B. Efficacy of Varenicline in the Treatment of Alcohol Dependence: An Updated Meta-Analysis and Meta-Regression. Int. J. Environ. Res. Public Health 2023, 20, 4091. https://doi.org/10.3390/ijerph20054091
Phimarn W, Sakhancord R, Paitoon P, Saramunee K, Sungthong B. Efficacy of Varenicline in the Treatment of Alcohol Dependence: An Updated Meta-Analysis and Meta-Regression. International Journal of Environmental Research and Public Health. 2023; 20(5):4091. https://doi.org/10.3390/ijerph20054091
Chicago/Turabian StylePhimarn, Wiraphol, Rotjanawat Sakhancord, Peerasaran Paitoon, Kritsanee Saramunee, and Bunleu Sungthong. 2023. "Efficacy of Varenicline in the Treatment of Alcohol Dependence: An Updated Meta-Analysis and Meta-Regression" International Journal of Environmental Research and Public Health 20, no. 5: 4091. https://doi.org/10.3390/ijerph20054091