

Eight Weeks of High-Intensity Interval Training Using Elevation Mask May Improve Cardiorespiratory Fitness, Pulmonary Functions, and Hematological Variables in University Athletes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Anthropometry
2.4. Blood Parameters
2.5. Procedures
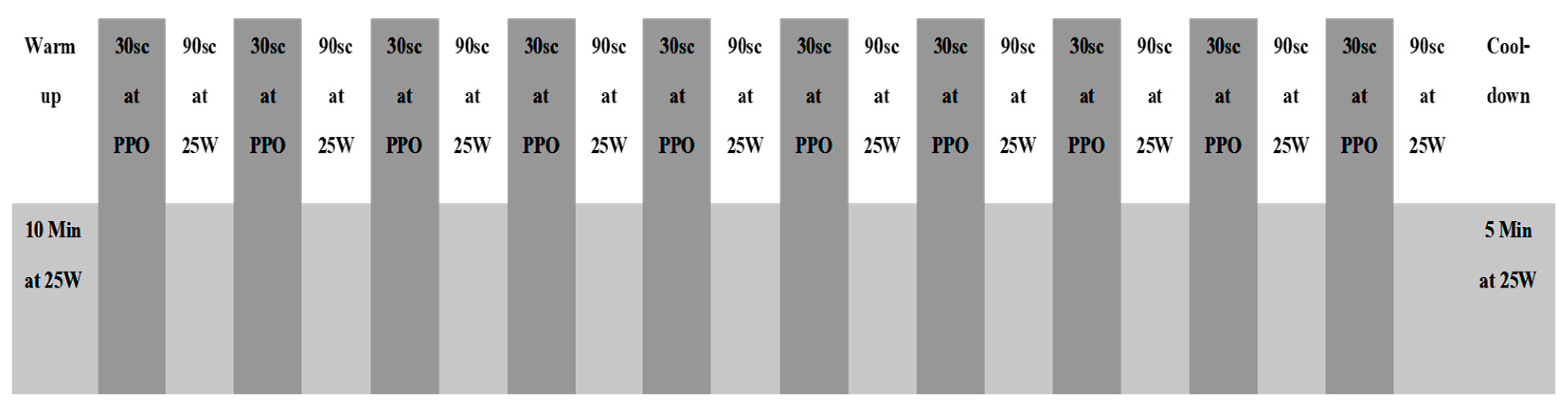
2.6. Training Program Protocol
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Romero-Arenas, S.; López-Pérez, E.; Colomer-Poveda, D.; Márquez, G. Oxygenation Responses While Wearing the Elevation Training Mask During an Incremental Cycling Test. J. Strength Cond. Res. 2021, 35, 1897–1904. [Google Scholar] [CrossRef] [PubMed]
- Trainingmsk Training Mask Official Store USA. Available online: https://www.trainingmask.com/ (accessed on 15 October 2022).
- Balke, B.; Nagle, F.J.; Daniels, J. Altitude and Maximum Performance in Work and Sports Activity. JAMA 1965, 194, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.D. Intermittent Hypoxic Training: Fact and Fancy. High Alt. Med. Biol. 2002, 3, 177–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westmacott, A.; Sanal-Hayes, N.E.M.; McLaughlin, M.; Mair, J.L.; Hayes, L.D. High-Intensity Interval Training (HIIT) in Hypoxia Improves Maximal Aerobic Capacity More Than HIIT in Normoxia: A Systematic Review, Meta-Analysis, and Meta-Regression. Int. J. Environ. Res. Public Health 2022, 19, 14261. [Google Scholar] [CrossRef]
- Porcari, J.P.; Probst, L.; Forrester, K.; Doberstein, S.; Foster, C.; Cress, M.L.; Schmidt, K. Effect of Wearing the Elevation Training Mask on Aerobic Capacity, Lung Function, and Hematological Variables. J. Sport. Sci. Med. 2016, 15, 379–386. [Google Scholar]
- Lundby, C.; Robach, P. Does ‘Altitude Training’ Increase Exercise Performance in Elite Athletes? Exp. Physiol. 2016, 101, 783–788. [Google Scholar] [CrossRef] [Green Version]
- Ga, B. Psychophysical Bases of Perceived Exertion. Med. Sci. Sport. Exerc. 1982, 14, 377–381. [Google Scholar]
- Faiss, R.; Girard, O.; Millet, G.P. Advancing Hypoxic Training in Team Sports: From Intermittent Hypoxic Training to Repeated Sprint Training in Hypoxia. Br. J. Sport. Med. 2013, 47, i45–i50. [Google Scholar] [CrossRef] [Green Version]
- Foster, C. Blood Lactate and Respiratory Measurement of the Capacity for Sustained Exercise. Physiol. Assess. Hum. Fit. 1995, 5, 57–72. [Google Scholar]
- Sellers, J.H.; Monaghan, T.P.; Schnaiter, J.A.; Jacobson, B.H.; Pope, Z.K. Efficacy of a Ventilatory Training Mask to Improve Anaerobic and Aerobic Capacity in Reserve Officers’ Training Corps Cadets. J. Strength Cond. Res. 2016, 30, 1155–1160. [Google Scholar] [CrossRef]
- Warren, B.; Spaniol, F.; Bonnette, R. The Effects of an Elevation Training Mask on VO2max of Male Reserve Officers Training Corps Cadets. Int. J. Exerc. Sci. 2017, 10, 37–43. [Google Scholar]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S.; Doleshal, P.; Dodge, C. A New Approach to Monitoring Exercise Training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar] [PubMed]
- Gething, A.D.; Passfield, L.; Davies, B. The Effects of Different Inspiratory Muscle Training Intensities on Exercising Heart Rate and Perceived Exertion. Eur. J. Appl. Physiol. 2004, 92, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Radak, Z. The Physiology of Physical Training; Academic Press: Cambridge, MA, USA, 2018; ISBN 978-0-12-815138-9. [Google Scholar]
- Kido, S.; Nakajima, Y.; Miyasaka, T.; Maeda, Y.; Tanaka, T.; Yu, W.; Maruoka, H.; Takayanagi, K. Effects of Combined Training with Breathing Resistance and Sustained Physical Exertion to Improve Endurance Capacity and Respiratory Muscle Function in Healthy Young Adults. J. Phys. Sci. 2013, 25, 605–610. [Google Scholar] [CrossRef] [Green Version]
- Granados, J.; Gillum, T.L.; Castillo, W.; Christmas, K.M.; Kuennen, M.R. “Functional” Respiratory Muscle Training During Endurance Exercise Causes Modest Hypoxemia but Overall Is Well Tolerated. J. Strength Cond. Res. 2016, 30, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Drust, B.; Waterhouse, J. Exercise at Altitude. Scott. Med. J. 2010, 55, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Garvican-Lewis, L.A.; Halliday, I.; Abbiss, C.R.; Saunders, P.U.; Gore, C.J. Altitude Exposure at 1800 m Increases Haemoglobin Mass in Distance Runners. J. Sport. Sci. Med. 2015, 14, 413–417. [Google Scholar]
- Frese, F.; Friedmann-Bette, B. Effects of repetitive training at low altitude on erythropoiesis in 400 and 800 m runners. Int. J. Sport. Med. 2010, 31, 382–388. [Google Scholar] [CrossRef]
- Garvican, L.; Martin, D.; Quod, M.; Stephens, B.; Sassi, A.; Gore, C. Time course of the hemoglobin mass response to natural altitude training in elite endurance cyclists. Scand. J. Med. Sci. Sport. 2012, 22, 95–103. [Google Scholar] [CrossRef]
- Lukanova-Jakubowska, A.; Piechota, K.; Grzywacz, T.; Ambroży, T.; Rydzik, Ł.; Ozimek, M. The Impact of Four High-Altitude Training Camps on the Aerobic Capacity of a Short Track PyeongChang 2018 Olympian: A Case Study. Int. J. Env. Res. Public Health 2022, 19, 3814. [Google Scholar] [CrossRef]
- Biggs, N.C.; England, B.S.; Turcotte, N.J.; Cook, M.R.; Williams, A.L. Effects of simulated altitude on maximal oxygen uptake and inspiratory fitness. Int. J. Exerc. Sci. 2017, 10, 127. [Google Scholar] [PubMed]


{kind=link}
| Variables | With-ETM | Non-ETM |
|---|---|---|
| Age (years) | 20.56 ± 1.01 | 21.81 ± 0.21 |
| Height (cm) | 180.89 ± 2.79 | 179.82 ± 2.39 |
| Weight (Kg) | 79.21 ± 3.19 | 78.13 ± 2.41 |
| Body Mass Index | 24.27 ± 1.28 | 24.17 ± 1.03 |
| Variables | N | Pre-Training | Post-Training | Changes | Z | p |
|---|---|---|---|---|---|---|
| FVC (L) | 22 | 5.28 ± 0.53 | 5.06 ± 0.48 | −0.22 ± 0.14 | −4.051 | 0.001 |
| FEV₁ (L) | 22 | 4.35 ± 0.13 | 4.38 ± 0.01 | 0.03 ± 0.13 | −0.991 | NS |
| FEV₁ (L)/FVC (L) | 22 | 81.91 ± 4.55 | 82.81 ± 3.05 | 0.90 ± 3.28 | −2.171 | NS |
| MIP (cmH₂o) | 22 | 80.85 ± 14.96 | 87.45 ± 9.39 | 6.60 ± 11.10 | −3.589 | 0.001 |
| Hb (g/dL) | 22 | 13.26 ± 0.33 | 14.00 ± 0.48 | 0.75 ± 0.35 | 4.051 | 0.001 |
| Hct (%) | 22 | 42.00 ± 0.97 | 43.44 ± 0.18 | 1.44 ± 0.92 | −4.113 | 0.001 |
| VO₂max (mL/kg/min) | 22 | 46.58 ± 2.14 | 47.58 ± 2.14 | 1.00 ± 3.09 | −3.428 | 0.001 |
| PPO (watts) | 22 | 276.68 ± 27.66 | 302.50 ± 23.89 | 25.82 ± 25.75 | −3.702 | 0.001 |
| VT1 (mL/kg/min) | 22 | 29.18 ± 3.41 | 29.31 ± 2.55 | 0.13 ± 4.48 | −0.087 | NS |
| PO at VT (watts | 22 | 158.09 ± 11.11 | 169.82 ± 10.49 | 11.73 ± 5.61 | −4.017 | 0.001 |
| VT2 (mL∙kg−1 min−1) | 22 | 38.70 ± 4.24 | 39.48 ± 3.27 | 0.78 ± 1.24 | −4.107 | 0.001 |
| PO at VT2 (watts) | 22 | 254.82 ± 17.26 | 266.59 ± 19.57 | 11.77 ± 26.14 | −3.320 | 0.001 |
| MHR (bpm) | 22 | 183.41 ± 8.91 | 184.57 ± 8.68 | 1.16 ± 2.37 | −2.070 | NS |
| Variables | N | Pre-Training | Post-Training | Changes | Z | p |
|---|---|---|---|---|---|---|
| FVC (L) | 22 | 5.11 ± 0.44 | 5.24 ± 0.34 | 0.12 ± 0.11 | −4.156 | 0.001 |
| FEV₁ (L) | 22 | 4.36 ± 0.22 | 4.76 ± 0.14 | 0.40 ± 0.22 | −4.076 | 0.001 |
| FEV₁ (L)/FVC (L) | 22 | 82.14 ± 5.68 | 83.17 ± 4.42 | 1.03 ± 3.45 | −2.363 | NS |
| MIP (cmH₂o) | 22 | 80.23 ± 14.59 | 88.21 ± 8.76 | 7.98 ± 10.75 | −4.130 | 0.001 |
| Hb (g/dL) | 22 | 12.80 ± 0.41 | 13.80 ± 0.68 | 1.00 ± 0.47 | 4.047 | 0.001 |
| Hct (%) | 22 | 41.27 ± 1.56 | 42.37 ± 1.48 | 1.10 ± 0.95 | −3.948 | 0.001 |
| VO₂max (mL/kg/min) | 22 | 46.80 ± 3.19 | 52.09 ± 3.17 | 5.29 ± 1.91 | −4.108 | 0.001 |
| PPO (watts) | 22 | 269.37 ± 29.98 | 312.73 ± 25.74 | 43.36 ± 29.27 | −4.075 | 0.001 |
| VT1 (mL/kg/min) | 22 | 29.47 ± 4.28 | 33.10 ± 3.13 | 3.64 ± 3.62 | −3.820 | 0.001 |
| PO at VT (watts) | 22 | 162.23 ± 14.18 | 191.50 ± 14.76 | 29.27 ± 10.12 | −4.113 | 0.001 |
| VT2 (mL∙kg−1 min−1) | 22 | 39.00 ± 5.11 | 43.80 ± 3.33 | 4.80 ± 4.05 | −4.108 | 0.001 |
| PO at VT2 (watts) | 22 | 240.13 ± 22.34 | 282.52 ± 21.93 | 42.40 ± 19.78 | −4.107 | 0.001 |
| MHR (bpm) | 22 | 183.59 ± 9.33 | 184.73 ± 8.07 | 1.14 ± 4.50 | −0.647 | NS |
| Variables | N | Control Group | Experimental Group | Z | p |
|---|---|---|---|---|---|
| FVC (L) | 22 | 5.28 ± 0.53 | 5.11 ± 0.44 | −2.480 | NS |
| FEV₁ (L) | 22 | 4.35 ± 0.13 | 4.36 ± 0.22 | −0.459 | NS |
| FEV₁ (L)/FVC (L) | 22 | 81.91 ± 4.55 | 82.14 ± 5.68 | −0.400 | NS |
| MIP (cmH₂o) | 22 | 80.85 ± 14.96 | 80.23 ± 14.59 | −0.413 | NS |
| Hb (g/dL) | 22 | 14.00 ± 0.48 | 13.80 ± 0.68 | −1.016 | NS |
| Hct (%) | 22 | 42.00 ± 0.97 | 41.27 ± 1.56 | −2.911 | 0.004 |
| VO₂max (mL/kg/min) | 22 | 46.58 ± 2.14 | 46.80 ± 3.19 | −2.038 | NS |
| PPO (watts) | 22 | 276.68 ± 27.66 | 269.37 ± 29.98 | −1.257 | NS |
| VT1 (mL/kg/min) | 22 | 29.18 ± 3.41 | 29.47 ± 4.28 | −0.611 | NS |
| PO at VT1 (watts) | 22 | 158.09 ± 11.11 | 162.23 ± 14.18 | −2.753 | 0.006 |
| VT2 (mL∙kg−1 min−1) | 22 | 38.70 ± 4.24 | 39.00 ± 5.11 | −2.335 | NS |
| PO at VT2 (watts) | 22 | 254.82 ± 17.26 | 240.13 ± 22.34 | −3.748 | 0.001 |
| MHR (bpm) | 22 | 183.41 ± 8.91 | 183.59 ± 9.33 | −1.256 | NS |
| Variables | Groups | N | Changes | Z | p |
|---|---|---|---|---|---|
| FVC (L) | Control Group | 22 | −0.22 ± 0.14 | −5.74 | 0.001 |
| Experimental Group | 22 | 0.12 ± 0.11 | |||
| FEV₁ (L) | Control Group | 22 | 0.03 ± 0.13 | −4.990 | 0.001 |
| Experimental Group | 22 | 0.40 ± 0.22 | |||
| FEV₁ (L)/FVC (L) | Control Group | 22 | 0.90 ± 3.28 | −1.222 | NS |
| Experimental Group | 22 | 1.03 ± 3.45 | |||
| MIP (cmH₂o) | Control Group | 22 | 6.60 ± 11.10 | −1.122 | NS |
| Experimental Group | 22 | 7.98 ± 10.75 | |||
| Hb (g/dL) | Control Group | 22 | 0.75 ± 0.35 | −2.346 | NS |
| Experimental Group | 22 | 1.00 ± 0.47 | |||
| Hct (%) | Control Group | 22 | 1.44 ± 0.92 | −1.755 | NS |
| Experimental Group | 22 | 1.10 ± 0.95 | |||
| VO₂max (mL/kg/min) | Control Group | 22 | 1.00 ± 3.09 | −5.167 | 0.001 |
| Experimental Group | 22 | 5.29 ± 1.91 | |||
| PPO (watts) | Control Group | 22 | 25.82 ± 25.75 | −2.313 | NS |
| Experimental Group | 22 | 43.36 ± 29.27 | |||
| VT1 (mL/kg/min) | Control Group | 22 | 0.13 ± 4.48 | −3.336 | 0.001 |
| Experimental Group | 22 | 3.64 ± 3.62 | |||
| PO at VT (watts) | Control Group | 22 | 11.73 ± 5.61 | −5.359 | 0.001 |
| Experimental Group | 22 | 29.27 ± 10.12 | |||
| VT2 (mL∙kg−1 min−1) | Control Group | 22 | 0.78 ± 1.24 | −5.153 | 0.001 |
| Experimental Group | 22 | 4.80 ± 4.05 | |||
| PO at VT2 (watts) | Control Group | 22 | 11.77 ± 26.14 | −4.508 | 0.001 |
| Experimental Group | 22 | 42.40 ± 19.78 | |||
| MHR (bpm) | Control Group | 22 | 1.16 ± 2.37 | −1.299 | NS |
| Experimental Group | 22 | 1.14 ± 4.50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abouzeid, N.; ELnaggar, M.; FathAllah, H.; Amira, M. Eight Weeks of High-Intensity Interval Training Using Elevation Mask May Improve Cardiorespiratory Fitness, Pulmonary Functions, and Hematological Variables in University Athletes. Int. J. Environ. Res. Public Health 2023, 20, 3533. https://doi.org/10.3390/ijerph20043533
Abouzeid N, ELnaggar M, FathAllah H, Amira M. Eight Weeks of High-Intensity Interval Training Using Elevation Mask May Improve Cardiorespiratory Fitness, Pulmonary Functions, and Hematological Variables in University Athletes. International Journal of Environmental Research and Public Health. 2023; 20(4):3533. https://doi.org/10.3390/ijerph20043533
Chicago/Turabian StyleAbouzeid, Nasser, Mahmoud ELnaggar, Haytham FathAllah, and Mostafa Amira. 2023. "Eight Weeks of High-Intensity Interval Training Using Elevation Mask May Improve Cardiorespiratory Fitness, Pulmonary Functions, and Hematological Variables in University Athletes" International Journal of Environmental Research and Public Health 20, no. 4: 3533. https://doi.org/10.3390/ijerph20043533