
Cessation of Face Mask Use after COVID-19 Vaccination in Patients with Diabetes: Prevalence and Determinants
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dependent Variable
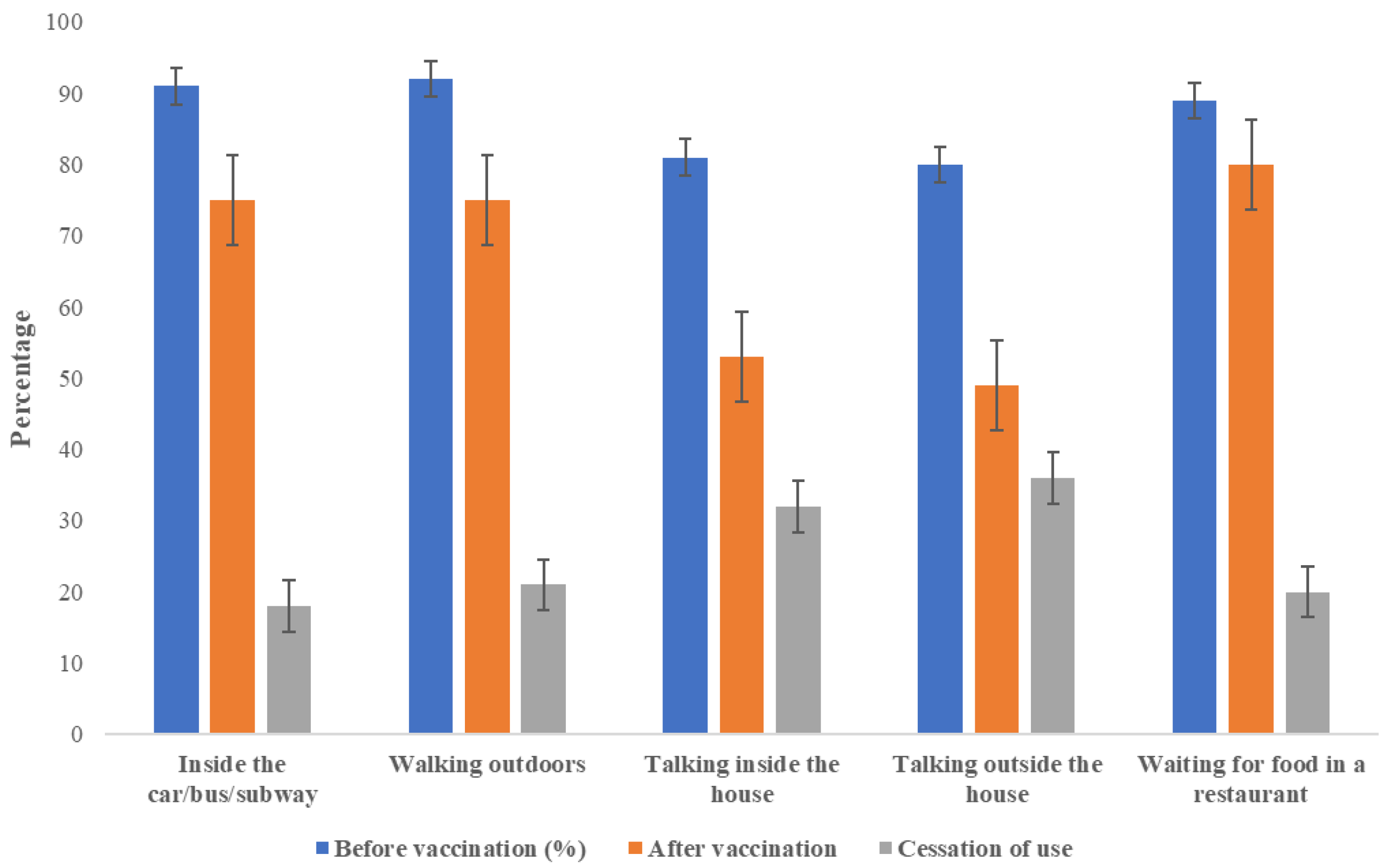
Cessation of Face Mask Use after Receiving the COVID-19 Vaccine
2.2. Independent Variables
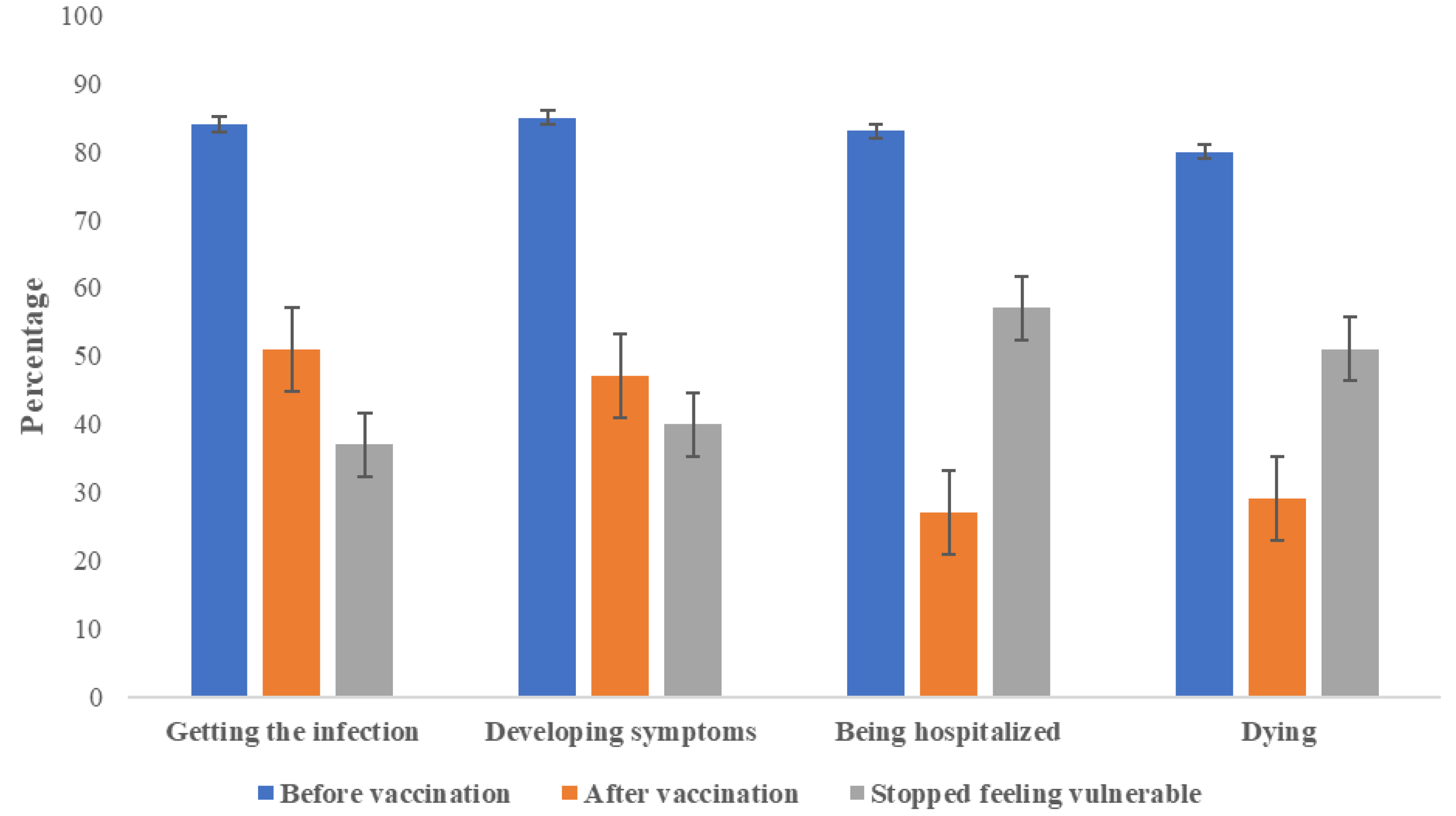
2.2.1. COVID-19 Vulnerability before and after Receiving the COVID-19 Vaccine
2.2.2. Use of Face Masks Benefits
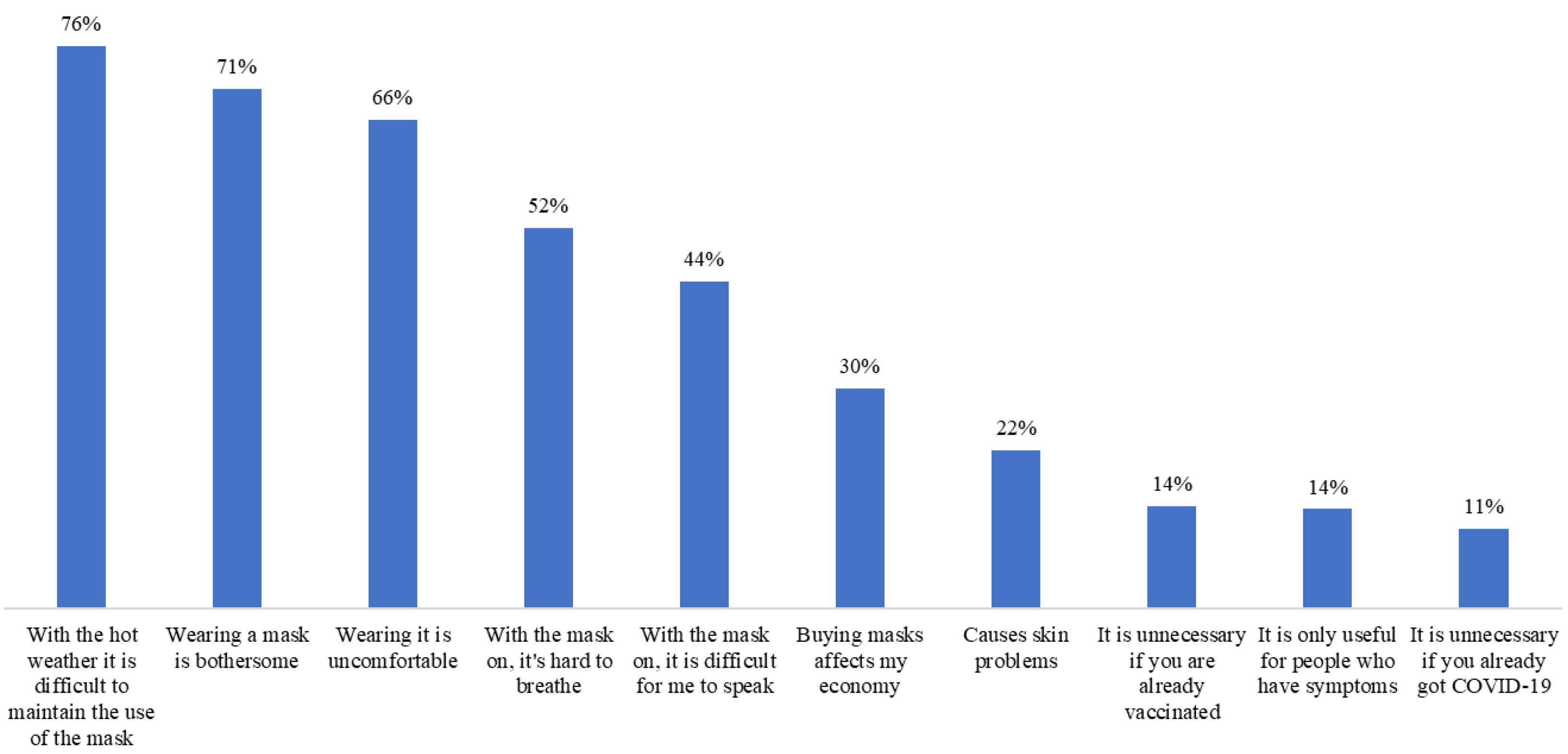
2.2.3. Use of Face Masks Barriers
2.2.4. Use of Face Masks Self-Efficacy
2.2.5. Vaccine’s Realistic Expectations
2.2.6. Vaccine’s Unrealistic Expectations
2.2.7. Other Variables That Can Affect Face Mask Use
2.3. Procedures
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Factors Associated with Cessation of Face Mask Use
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coclite, D.; Napoletano, A.; Gianola, S.; del Monaco, A.; D’Angelo, D.; Fauci, A.; Iacorossi, L.; Latina, R.; Torre, G.L.; Mastroianni, C.M.; et al. Face Mask Use in the Community for Reducing the Spread of COVID-19: A Systematic Review. Front. Med. 2021, 7, 594269. [Google Scholar] [CrossRef]
- Ford, N.; Holmer, H.K.; Chou, R.; Villeneuve, P.J.; Baller, A.; Van Kerkhove, M.; Allegranzi, B. Mask Use in Community Settings in the Context of COVID-19: A Systematic Review of Ecological Data. EClinicalMedicine 2021, 38, 101024. [Google Scholar] [CrossRef]
- Joo, H.; Miller, G.F.; Sunshine, G.; Gakh, M.; Pike, J.; Havers, F.P.; Kim, L.; Weber, R.; Dugmeoglu, S.; Watson, C.; et al. Decline in COVID-19 Hospitalization Growth Rates Associated with Statewide Mask Mandates—10 States, March–October 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 212–216. [Google Scholar] [CrossRef]
- Fischer, C.B.; Adrien, N.; Silguero, J.J.; Hopper, J.J.; Chowdhury, A.I.; Werler, M.M. Mask Adherence and Rate of COVID-19 across the United States. PLoS ONE 2021, 16, e0249891. [Google Scholar] [CrossRef]
- Adjodah, D.; Dinakar, K.; Chinazzi, M.; Fraiberger, S.P.; Pentland, A.; Bates, S.; Staller, K.; Vespignani, A.; Bhatt, D.L. Association between COVID-19 Outcomes and Mask Mandates, Adherence, and Attitudes. PLoS ONE 2021, 16, e0252315. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-Z.; Kuan, C.-C. Vaccination to Reduce Severe COVID-19 and Mortality in COVID-19 Patients: A Systematic Review and Meta-Analysis. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1770–1776. [Google Scholar] [CrossRef]
- Liu, Q.; Qin, C.; Liu, M.; Liu, J. Effectiveness and Safety of SARS-CoV-2 Vaccine in Real-World Studies: A Systematic Review and Meta-Analysis. Infect. Dis. Poverty 2021, 10, 132. [Google Scholar] [CrossRef]
- Maryland, U. The Global COVID-19 Trends and Impact Survey. Available online: https://covidmap.umd.edu/map/results.html?country=Mexico (accessed on 6 May 2022).
- World Health Organization WHO COVID-19 Dashboard. Available online: https://covid19.who.int/region/amro/country/mx (accessed on 17 August 2022).
- School, O.M.; Oxford, U.; Lab, G.C.D. Share of People Vaccinated against COVID-19. 5 May 2022. Available online: https://ourworldindata.org/covid-vaccinations?country=OWID_WRL (accessed on 17 August 2022).
- Nguyen, J.L.; Alfred, T.; Reimbaeva, M.; Malhotra, D.; Khan, F.; Swerdlow, D.; Angulo, F.J. Population Attributable Fractions of Underlying Medical Conditions for Coronavirus Disease 2019 (COVID-19) Diagnosis and COVID-19 Hospitalizations, Ventilations, and Deaths Among Adults in the United States. Open Forum Infect. Dis. 2022, 9, ofac099. [Google Scholar] [CrossRef] [PubMed]
- Pranata, R.; Henrina, J.; Raffaello, W.M.; Lawrensia, S.; Huang, I. Diabetes and COVID-19: The Past, The Present, and The Future. Metabolism 2021, 121, 154814. [Google Scholar] [CrossRef]
- Huang, I.; Lim, M.A.; Pranata, R. Diabetes Mellitus Is Associated with Increased Mortality and Severity of Disease in COVID-19 Pneumonia—A Systematic Review, Meta-Analysis, and Meta-Regression. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Cordero-Franco, H.F.; De La Garza-Salinas, L.H.; Gomez-Garcia, S.; Moreno-Cuevas, J.E.; Vargas-Villarreal, J.; González-Salazar, F. Risk Factors for SARS-CoV-2 Infection, Pneumonia, Intubation, and Death in Northeast Mexico. Front. Public Health 2021, 9, 645739. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors Associated with COVID-19-Related Death Using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Coronavirus Disease (COVID-19). Available online: https://www.who.int/health-topics/coronavirus#tab=tab_2 (accessed on 17 August 2022).
- Centers for Disease Control and Prevention Order: Wearing of Face Masks While on Conveyances and at Transportation Hubs. Available online: https://www.cdc.gov/quarantine/masks/mask-travel-guidance.html (accessed on 17 August 2022).
- American Diabetes Association Diabetes and Coronavirus (COVID-19): Take Everyday Precautions. Available online: https://diabetes.org/coronavirus-covid-19/take-everyday-precautions-for-coronavirus (accessed on 17 August 2022).
- Rosenstock, I.M. Why People Use Health Services. Milbank Q. 2005, 83, 94–124. [Google Scholar] [CrossRef]
- Strecher, V.J.; Champion, V.L.; Rosenstock, I.M. The Health Belief Model. In Handbook of Health Behavior Research I: Personal and Social Determinants; Gochman, D.S., Ed.; Plenum Press: New York, NY, USA, 1997; pp. 71–89. ISBN 0-306-45443-2. [Google Scholar]
- Quah, S.R. The Health Belief Model and Preventive Health Behaviour in Singapore. Soc. Sci. Med. 1985, 21, 351–363. [Google Scholar] [CrossRef]
- DeDonno, M.A.; Longo, J.; Levy, X.; Morris, J.D. Perceived Susceptibility and Severity of COVID-19 on Prevention Practices, Early in the Pandemic in the State of Florida. J. Community Health 2022, 45, 1–8. [Google Scholar] [CrossRef]
- Wang, M.; Zhao, C.; Fan, J. To Wear or Not to Wear: Analysis of Individuals’ Tendency to Wear Masks during the COVID-19 Pandemic in China. Int. J. Environ. Res. Public Health 2021, 18, 11298. [Google Scholar] [CrossRef]
- Cai, Z.; Hu, W.; Zheng, S.; Wen, X.; Wu, K. Cognition and Behavior of COVID-19 Vaccination Based on the Health Belief Model: A Cross-Sectional Study. Vaccines 2022, 10, 544. [Google Scholar] [CrossRef] [PubMed]
- Alagili, D.E.; Bamashmous, M. The Health Belief Model as an Explanatory Framework for COVID-19 Prevention Practices. J. Infect. Public Health 2021, 14, 1398–1403. [Google Scholar] [CrossRef]
- Kollamparambil, U.; Oyenubi, A. Behavioural Response to the Covid-19 Pandemic in South Africa. PLoS ONE 2021, 16, e0250269. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A.; Rowe, G.; Lambert, N.; Waddington, M.; Mahtani, K.; Kenten, C.; Howe, A.; Francis, S. The Measurement of Patients’ Expectations for Health Care: A Review and Psychometric Testing of a Measure of Patients’ Expectations. Health Technol. Assess. Rockv 2012, 16, 1–532. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Lei, H.; Li, L.; Jin, T.; Liu, X.; Miao, D.; Su, B.; Bu, Z.; Fan, L.; Xue, P.; et al. COVID-19 Vaccination Did Not Change the Personal Protective Behaviors of Healthcare Workers in China. Front. Public Health 2021, 9, 777426. [Google Scholar] [CrossRef] [PubMed]
- Si, R.; Yao, Y.; Zhang, X.; Lu, Q.; Aziz, N. Investigating the Links Between Vaccination Against COVID-19 and Public Attitudes Toward Protective Countermeasures: Implications for Public Health. Front. Public Health 2021, 9, 702699. [Google Scholar] [CrossRef] [PubMed]
- Della Polla, G.; Pelullo, C.P.; Di Giuseppe, G.; Angelillo, I.F. Changes in Behaviors and Attitudes in Response to COVID-19 Pandemic and Vaccination in Healthcare Workers and University Students in Italy. Vaccines 2021, 9, 1276. [Google Scholar] [CrossRef] [PubMed]
- Wright, L.; Steptoe, A.; Mak, H.W.; Fancourt, D. Do People Reduce Compliance with COVID-19 Guidelines Following Vaccination? A Longitudinal Analysis of Matched UK Adults. J. Epidemiol. Community Health 2022, 76, 109–115. [Google Scholar] [CrossRef]
- O’Donohue, L.S.; Fletcher-Gutowski, S.; Sidhu, A.; Verma, A.; Phillips, T.C.; Misra, P.G. Mask Use among Health Care Workers and Feelings of Safety at Work Pre- and Post- COVID-19 Vaccine. Am. J. Infect. Control 2022, 50, 503–508. [Google Scholar] [CrossRef]
- Thorpe, A.; Fagerlin, A.; Drews, F.A.; Shoemaker, H.; Scherer, L.D. Self-Reported Health Behaviors and Risk Perceptions Following the COVID-19 Vaccination Rollout in the USA: An Online Survey Study. Public Health 2022, 208, 68–71. [Google Scholar] [CrossRef]
- Kaim, A.; Siman-Tov, M.; Jaffe, E.; Adini, B. From Isolation to Containment: Perceived Fear of Infectivity and Protective Behavioral Changes during the COVID-19 Vaccination Campaign. Int. J. Environ. Res. Public Health 2021, 18, 6503. [Google Scholar] [CrossRef]
- Zhang, N.; Liu, X.; Jin, T.; Zhao, P.; Miao, D.; Lei, H.; Su, B.; Xue, P.; Xie, J.; Li, Y. Weakening Personal Protective Behavior by Chinese University Students after COVID-19 Vaccination. Build. Environ. 2021, 206, 108367. [Google Scholar] [CrossRef]
- Zewude, B.; Melese, B.; Addis, E.; Solomon, W. Changing Patterns of Compliance with Protective Behavioral Recommendations in the Post First-Round COVID-19 Vaccine Period Among Healthcare Workers in Southern Ethiopia. Risk Manag. Healthc. Policy 2021, 14, 3575–3587. [Google Scholar] [CrossRef]
- Hossain, M.E.; Islam, M.S.; Rana, M.J.; Amin, M.R.; Rokonuzzaman, M.; Chakrobortty, S.; Saha, S.M. Scaling the Changes in Lifestyle, Attitude, and Behavioral Patterns among COVID-19 Vaccinated People: Insights from Bangladesh. Hum. Vaccin. Immunother. 2022, 18, 2022920. [Google Scholar] [CrossRef]
- Goldfarb, J.L.; Kreps, S.; Brownstein, J.S.; Kriner, D.L. Beyond the First Dose—Covid-19 Vaccine Follow-through and Continued Protective Measures. N. Engl. J. Med. 2021, 385, 101–103. [Google Scholar] [CrossRef]
- Saha, A.K.; Podder, C.N.; Niger, A.M. Dynamics of Novel COVID-19 in the Presence of Co-Morbidity. Infect. Dis. Model. 2022, 7, 138–160. [Google Scholar] [CrossRef] [PubMed]
- Hervada-Vidal, X.; Santiago-Perez, M.I.; Vazquez-Fernandez, E.; Castillo-Salgado, C.; Loyola-Elizondo, E.; Silva-Ayçaguer, L.C. Epidat: Análisis Epidemiológico de Datos Tabulados, version 3.1. Windows. Xunta de Galicia. Ministry of Public Health: Santiago, Spain, 2005.
- Velasco-Rodríguez, V.M.; Martínez-Ordaz, V.A.; Rois-Hernández, J.; Huazano-García, F.; Nieves-Rentería, A. Cálculo Del Tamaño de La Muestra. In Muestreo y tamaño de la muestra: Una guía práctica para personal de salud que realiza investigación; e-libro.net: Torreón, Mexico, 2002; pp. 39–40. ISBN 987-9499-36-0. [Google Scholar]
- Asociación Médica Mundial Declaración de Helsinki de La AMM—Principios Éticos Para Las Investigaciones Médicas En Humanos. Available online: https://www.wma.net/es/policies-post/declaracion-de-helsinki-de-la-amm-principios-eticos-para-las-investigaciones-medicas-en-seres-humanos/ (accessed on 6 January 2023).
- Schoeni, R.F.; Wiemers, E.E.; Seltzer, J.A.; Langa, K.M. Association Between Risk Factors for Complications From COVID-19, Perceived Chances of Infection and Complications, and Protective Behavior in the US. JAMA Netw. Open 2021, 4, e213984. [Google Scholar] [CrossRef]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk Perceptions of COVID-19 around the World. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Musche, V.; Kohler, H.; Bäuerle, A.; Schweda, A.; Weismüller, B.; Fink, M.; Schadendorf, T.; Robitzsch, A.; Dörrie, N.; Tan, S.; et al. COVID-19-Related Fear, Risk Perception, and Safety Behavior in Individuals with Diabetes. Healthcare 2021, 9, 480. [Google Scholar] [CrossRef]
- Kohler, H.; Bäuerle, A.; Schweda, A.; Weismüller, B.; Fink, M.; Musche, V.; Robitzsch, A.; Pfeiffer, C.; Benecke, A.-V.; Dörrie, N.; et al. Increased COVID-19-Related Fear and Subjective Risk Perception Regarding COVID-19 Affects Behavior in Individuals with Internal High-Risk Diseases. J. Prim. Care Community Health 2021, 12, 215013272199689. [Google Scholar] [CrossRef]
- Zhen, J.; Stefanolo, J.P.; de la Paz Temprano, M.; Seiler, C.L.; Caminero, A.; De-Madaria, E.; Huguet, M.M.; Santiago, V.; Niveloni, S.I.; Smecuol, E.G.; et al. Risk Perception and Knowledge of COVID-19 in Patients with Celiac Disease. World J. Gastroenterol. 2021, 27, 1213–1225. [Google Scholar] [CrossRef]
- Laires, P.A.; Dias, S.; Gama, A.; Moniz, M.; Pedro, A.R.; Soares, P.; Aguiar, P.; Nunes, C. The Association Between Chronic Disease and Serious COVID-19 Outcomes and Its Influence on Risk Perception: Survey Study and Database Analysis. JMIR Public Health Surveill. 2021, 7, e22794. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Burger, R.; Christian, C.; English, R.; Maughan-Brown, B.; Rossouw, L. Predictors of Mask-Wearing during the Advent of the COVID-19 Pandemic: Evidence from South Africa. Transl. Behav. Med. 2022, 12, ibab132. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.T.; Lau, Y.C.; Shan, S.; Ryu, S.; Du, Z.; Wang, L.; Xu, X.-K.; Chen, D.; Xiong, J.; Tae, J.; et al. Prediction of Upcoming Global Infection Burden of Influenza Seasons after Relaxation of Public Health and Social Measures during the COVID-19 Pandemic: A Modelling Study. Lancet Glob. Health 2022, 10, e1612–e1622. [Google Scholar] [CrossRef] [PubMed]
- Cheong, C.-W.; Chen, C.-L.; Li, C.-H.; Seak, C.-J.; Tseng, H.-J.; Hsu, K.-H.; Ng, C.-J.; Chien, C.-Y. Two-Stage Prediction Model for in-Hospital Mortality of Patients with Influenza Infection. BMC Infect. Dis. 2021, 21, 451. [Google Scholar] [CrossRef]
- Shinan-Altman, S. Short Report: Engagement with Health Services during the COVID-19 Outbreak: The Case of Israeli People with Diabetes. Psychol. Health Med. 2022, 27, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, S.M.; O’Shea, K.J.; Chin, K.L.; Strych, U.; Ferguson, M.C.; Bottazzi, M.E.; Wedlock, P.T.; Cox, S.N.; Siegmund, S.S.; Hotez, P.J.; et al. Maintaining Face Mask Use before and after Achieving Different COVID-19 Vaccination Coverage Levels: A Modelling Study. Lancet Public Health 2022, 7, e356–e365. [Google Scholar] [CrossRef]
- Jose, R.; Narendran, M.; Bindu, A.; Beevi, N.; L, M.; Benny, P.V. Public Perception and Preparedness for the Pandemic COVID-19: A Health Belief Model Approach. Clin. Epidemiol. Glob. Health 2021, 9, 41–46. [Google Scholar] [CrossRef]
- Li, M.; Lv, G.; Hsieh, S.; Shao, R.; Yuan, J. Pandemic Worry and Preventive Health Behaviors During the COVID-19 Outbreak. Front. Med. 2021, 8, 700072. [Google Scholar] [CrossRef] [PubMed]
- Rui, J.R.; Yang, K.; Chen, J. Information Sources, Risk Perception, and Efficacy Appraisal’s Prediction of Engagement in Protective Behaviors Against COVID-19 in China: Repeated Cross-Sectional Survey. JMIR Hum. Factors 2021, 8, e23232. [Google Scholar] [CrossRef]
- van Loenhout, J.A.F.; Vanderplanken, K.; Scheen, B.; Van den Broucke, S.; Aujoulat, I. Determinants of Adherence to COVID-19 Measures among the Belgian Population: An Application of the Protection Motivation Theory. Arch. Public Health 2021, 79, 74. [Google Scholar] [CrossRef]
- Baier, M.; Knobloch, M.J.; Osman, F.; Safdar, N. Effectiveness of Mask-Wearing on Respiratory Illness Transmission in Community Settings: A Rapid Review. Disaster Med. Public Health Prep. 2022, 17, 1–8. [Google Scholar] [CrossRef]
- Keller, S.N.; Honea, J.C.; Ollivant, R. How Social Media Comments Inform the Promotion of Mask-Wearing and Other COVID-19 Prevention Strategies. Int. J. Environ. Res. Public Health 2021, 18, 5624. [Google Scholar] [CrossRef]
- Hill, L.M.; Davis, H.; Drewry, M.; Shelus, V.; Bartels, S.M.; Gora Combs, K.; Ribisl, K.M.; Lazard, A.J. Barriers to and Facilitators of COVID-19 Prevention Behaviors Among North Carolina Residents. Health Educ. Behav. 2022, 49, 231–241. [Google Scholar] [CrossRef]
- Tang, C.S.; Wong, C. Factors Influencing the Wearing of Facemasks to Prevent the Severe Acute Respiratory Syndrome among Adult Chinese in Hong Kong. Prev. Med. Baltim 2004, 39, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Zdziarski, K.; Landowski, M.; Zabielska, P.; Karakiewicz, B. Subjective Feelings of Polish Doctors after Receiving the COVID-19 Vaccine. Int. J. Environ. Res. Public Health 2021, 18, 6291. [Google Scholar] [CrossRef] [PubMed]
- Kalra, S.; Chaudhary, S.; Kantroo, V.; Ahuja, J. Mask Fatigue. J. Pak. Med. Assoc. 2020, 70, 2484. [Google Scholar] [PubMed]
- Jiang, L.; Liu, S.; Li, H.; Xie, L.; Jiang, Y. The Role of Health Beliefs in Affecting Patients’ Chronic Diabetic Complication Screening: A Path Analysis Based on the Health Belief Model. J. Clin. Nurs. 2021, 30, 2948–2959. [Google Scholar] [CrossRef]
- Schmidt, S.K.; Hemmestad, L.; MacDonald, C.S.; Langberg, H.; Valentiner, L.S. Motivation and Barriers to Maintaining Lifestyle Changes in Patients with Type 2 Diabetes after an Intensive Lifestyle Intervention (The U-TURN Trial): A Longitudinal Qualitative Study. Int. J. Environ. Res. Public Health 2020, 17, 7454. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Frequency n (%) |
|---|---|
| Sociodemographic | |
| Sex, female | 187 (64.9) |
| Marital status, lives with a partner | 227 (78.8) |
| Occupation, economically active | 112 (38.9) |
| Schooling, high school, or less | 151 (52.4) |
| Smoking | 125 (44.4) |
| Medical history | |
| Hypertension | 208 (72.2) |
| Cardiovascular disease | 35 (12.2) |
| Chronic obstructive pulmonary disease | 25 (8.7) |
| Immunosuppression | 7 (2.4) |
| Chronic kidney disease | 7 (2.4) |
| Cancer | 5 (1.7) |
| Type of vaccine | |
| AZD-1222 (virus vector) | 184 (63.9) |
| BNT162b2 (mRNA) | 53 (18.4) |
| CoronaVac (inactivated virus) | 17 (5.9) |
| mRNA-1273 (mRNA) | 17 (5.9) |
| Ad5-nCoV (virus vector) | 4 (1.4) |
| JNJ-78436735 (virus vector) | 2 (0.7) |
| Unknown | 11 (3.8) |
| Number of doses | |
| One | 18 (6.3) |
| Two | 153 (53.1) |
| Three or more | 117 (40.6) |
| COVID-19 infection | |
| Before the 1st dose | 82 (70.1) |
| Before the 2nd dose | 1 (0.9) |
| After the 2nd dose | 34 (29.1) |
| Needed hospitalization | 6 (5.1) |
| A family member got sick with COVID-19 | 243 (84.4) |
| A family member died because of COVID-19 | 1 (0.4) |
| Cessation of Use | Unadjusted OR | Adjusted OR a | ||
|---|---|---|---|---|
| Yes (n = 73) n (%) | No (n = 215) n (%) | (95% CI) | (95% CI) | |
| Not feeling vulnerable after vaccination | ||||
| For getting the infection | 39 (53.4) | 66 (30.7) | 2.59 (1.51, 4.45) | 2.07 (0.75, 5.70) |
| For developing symptoms | 39 (53.4) | 75 (34.9) | 2.14 (1.25, 3.66) | 0.93 (0.34, 2.54) |
| For being hospitalized | 59 (80.8) | 105 (48.8) | 4.41 (2.34, 8.31) | 3.26 (1.23, 8.60) |
| For dying from the disease | 52 (71.2) | 95 (44.2) | 3.13 (1.77, 5.52) | 1.18 (0.49, 2.82) |
| Perception of benefits | 61 (83.6) | 196 (91.2) | 0.49 (0.23, 1.06) | 0.36 (0.15, 0.86) |
| Perception of barriers | 13 (17.8) | 60 (27.9) | 0.56 (0.29, 1.09) | 0.62 (0.30, 1.29) |
| High and very high self-efficacy | 71 (97.3) | 206 (95.8) | 1.55 (0.33, 7.35) | 1.17 (0.20, 6.78) |
| Vaccine’s realistic expectations | 59 (80.8) | 174 (80.9) | 0.99 (0.51, 1.94) | 0.91 (0.42, 1.97) |
| Vaccine’s unrealistic expectations | 10 (13.7) | 32 (14.9) | 0.91 (0.43, 1.93) | 1.15 (0.49, 2.70) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordero Franco, H.F.; Salinas Martínez, A.M.; Martínez Martínez, D.L.; Santiago Jarquin, B.R.; Guzmán de la Garza, F.J. Cessation of Face Mask Use after COVID-19 Vaccination in Patients with Diabetes: Prevalence and Determinants. Int. J. Environ. Res. Public Health 2023, 20, 2768. https://doi.org/10.3390/ijerph20042768
Cordero Franco HF, Salinas Martínez AM, Martínez Martínez DL, Santiago Jarquin BR, Guzmán de la Garza FJ. Cessation of Face Mask Use after COVID-19 Vaccination in Patients with Diabetes: Prevalence and Determinants. International Journal of Environmental Research and Public Health. 2023; 20(4):2768. https://doi.org/10.3390/ijerph20042768
Chicago/Turabian StyleCordero Franco, Hid Felizardo, Ana María Salinas Martínez, Diana Laura Martínez Martínez, Blanca Reyna Santiago Jarquin, and Francisco Javier Guzmán de la Garza. 2023. "Cessation of Face Mask Use after COVID-19 Vaccination in Patients with Diabetes: Prevalence and Determinants" International Journal of Environmental Research and Public Health 20, no. 4: 2768. https://doi.org/10.3390/ijerph20042768