
Lifestyle Habits Determinants of Health-Related Quality of Life in Moroccan College Students
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Health-Related Quality of Life Measures
2.3. Validity of the Daily Lifestyle Habits Questionnaire
2.3.1. Content Validity
2.3.2. Test–Retest Reliability
2.3.3. Internal Consistency Reliability
2.4. Statistical Analysis
3. Results
3.1. Participants’ General Characteristics
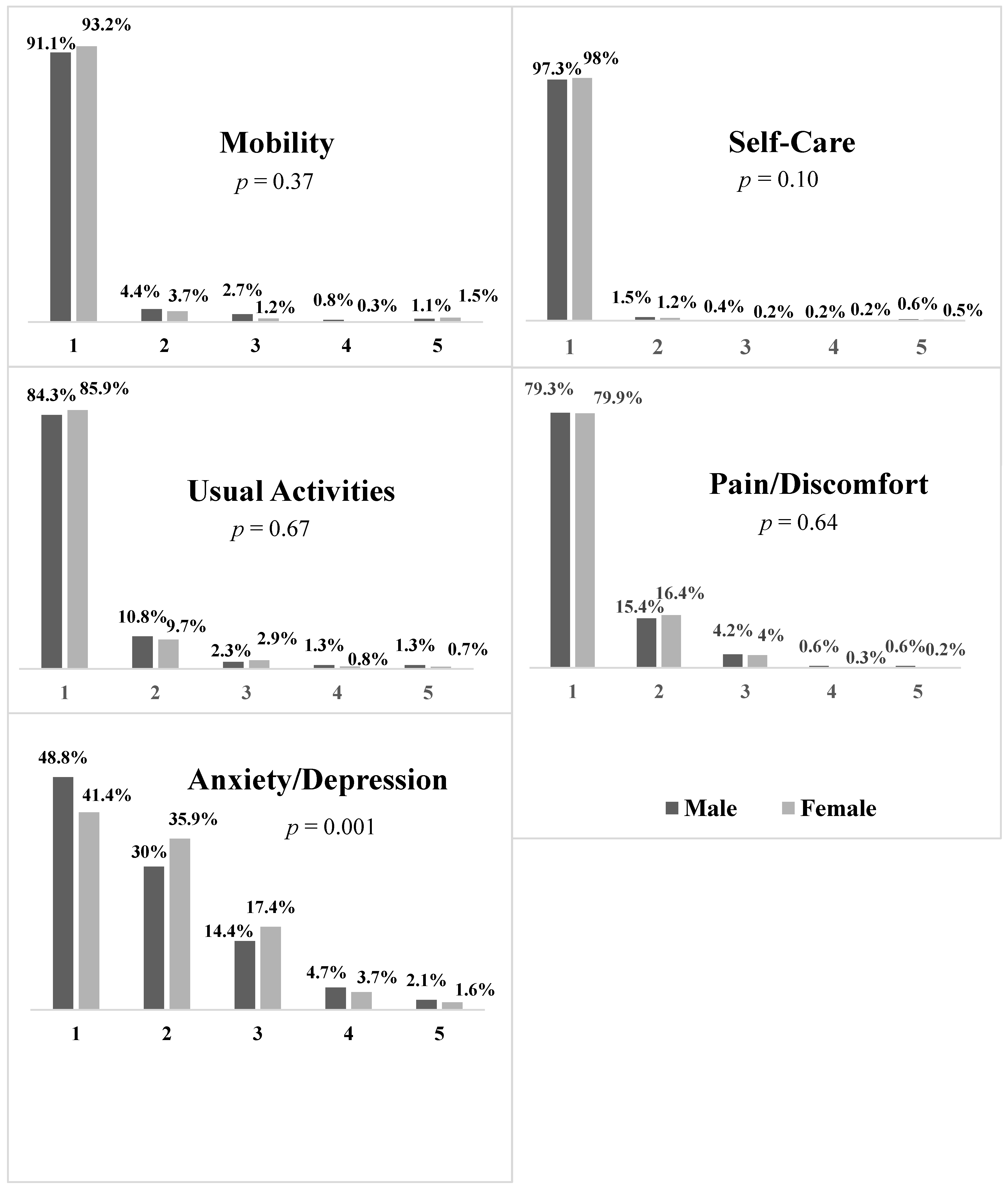
3.2. Health-Related Quality of Life of Students
3.3. Daily Lifestyle Habits of Participants
3.4. Association between Daily Lifestyle Habits and Health-Related Quality of Life
4. Discussion
5. Implications of the Study
6. Limitations of the Study
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Health-Related Quality of Life (HRQOL)|CDC. Available online: https://www.cdc.gov/hrqol/index.htm (accessed on 13 December 2021).
- Sivaramakrishnan, D.; Fitzsimons, C.; Kelly, P.; Ludwig, K.; Mutrie, N.; Saunders, D.H.; Baker, G. The Effects of Yoga Compared to Active and Inactive Controls on Physical Function and Health Related Quality of Life in Older Adults-Systematic Review and Meta-Analysis of Randomised Controlled Trials. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faílde Garrido, J.M.; Ruiz Soriano, L.; Pérez Fernández, M.R.; Lameiras Fernández, M.; Rodríguez Castro, Y. Evolution of Quality of Life and Health-related Behaviors among Spanish University Students. Int. J. Health Plann. Mgmt. 2019, 34, e789–e801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaez, M.; Voss, M.; Laflamme, L. Health-Related Quality of Life Among University Students. In Handbook of Disease Burdens and Quality of Life Measures; Preedy, V.R., Watson, R.R., Eds.; Springer: New York, NY, USA, 2010; pp. 2555–2577. ISBN 978-0-387-78664-3. [Google Scholar]
- Deforche, B.; Van Dyck, D.; Deliens, T.; De Bourdeaudhuij, I. Changes in Weight, Physical Activity, Sedentary Behaviour and Dietary Intake during the Transition to Higher Education: A Prospective Study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 16. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, Í.J.S.; Pereira, R.; Freire, I.V.; de Oliveira, B.G.; Casotti, C.A.; Boery, E.N. Stress and Quality of Life Among University Students: A Systematic Literature Review. Health Prof. Educ. 2018, 4, 70–77. [Google Scholar] [CrossRef]
- Barayan, S.S.; Al Dabal, B.K.; Abdelwahab, M.M.; Shafey, M.M.; Al Omar, R.S. Health-Related Quality of Life among Female University Students in Dammam District: Is Internet Use Related? J. Fam. Community Med. 2018, 25, 20–28. [Google Scholar] [CrossRef]
- Hadjimbei, E.; Botsaris, G.; Gekas, V.; Panayiotou, A.G. Adherence to the Mediterranean Diet and Lifestyle Characteristics of University Students in Cyprus: A Cross-Sectional Survey. J. Nutr. Metab. 2016, 2016, 2742841. [Google Scholar] [CrossRef] [Green Version]
- Ge, Y.; Xin, S.; Luan, D.; Zou, Z.; Liu, M.; Bai, X.; Gao, Q. Association of Physical Activity, Sedentary Time, and Sleep Duration on the Health-Related Quality of Life of College Students in Northeast China. Health Qual. Life Outcomes 2019, 17, 124. [Google Scholar] [CrossRef] [Green Version]
- Calestine, J.; Bopp, M.; Bopp, C.M.; Papalia, Z. College Student Work Habits are Related to Physical Activity and Fitness. Int. J. Exerc. Sci. 2017, 10, 1009–1017. [Google Scholar]
- Joseph, R.P.; Royse, K.E.; Benitez, T.J.; Pekmezi, D.W. Physical Activity and Quality of Life among University Students: Exploring Self-Efficacy, Self-Esteem, and Affect as Potential Mediators. Qual. Life Res. 2014, 23, 659–667. [Google Scholar] [CrossRef] [Green Version]
- Milic, M.; Gazibara, T.; Pekmezovic, T.; Kisic Tepavcevic, D.; Maric, G.; Popovic, A.; Stevanovic, J.; Patil, K.H.; Levine, H. Tobacco Smoking and Health-Related Quality of Life among University Students: Mediating Effect of Depression. PLoS ONE 2020, 15, e0227042. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Flynn, T.; Stevens, K.; Brazier, J.; Huynh, E.; Sawyer, M.; Roberts, R.; Ratcliffe, J. Assessing the Health-Related Quality of Life of Australian Adolescents: An Empirical Comparison of the Child Health Utility 9D and EQ-5D-Y Instruments. Value Health 2015, 18, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.-S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric Properties of the EQ-5D-5L: A Systematic Review of the Literature. Qual. Life Res. 2021, 30, 647–673. [Google Scholar] [CrossRef] [PubMed]
- Ahlam, A.; Hind, M.; Haddou Rahou, B.; Rachid, R.; Hassan, E. Quality of Life of Moroccan Patients on the Palliative Phase of Advanced Cancer. BMC Res. Notes 2019, 12, 351. [Google Scholar] [CrossRef] [PubMed]
- Azizi, A.; Achak, D.; Aboudi, K.; Saad, E.; Nejjari, C.; Nouira, Y.; Hilali, A.; Youlyouz-Marfak, I.; Marfak, A. Health-Related Quality of Life and Behavior-Related Lifestyle Changes Due to the COVID-19 Home Confinement: Dataset from a Moroccan Sample. Data Brief 2020, 32, 106239. [Google Scholar] [CrossRef] [PubMed]
- El Fakir, S.; El Rhazi, K.; Zidouh, A.; Bennani, M.; Benider, A.; Errihani, H.; Mellass, N.; Bekkali, R.; Nejjari, C. Health-Related Quality of Life among Breast Cancer Patients and Influencing Factors in Morocco. APJCP 2016, 17, 5063. [Google Scholar] [CrossRef]
- Lemtiri Chelieh, M.; Kadhum, M.; Lewis, T.; Molodynski, A.; Abouqal, R.; Belayachi, J.; Bhugra, D. Mental health and wellbeing among Moroccan medical students: A descriptive study. Int. Rev. Psychiatry 2019, 31, 608–612. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and Preliminary Testing of the New Five-Level Version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- HESS, J.M.; Satya, S.J.; Joanne, S.L. What is a snack, why do we snack, and how can we choose better snacks? A review of the definitions of snacking, motivations to snack, contributions to dietary intake, and recommendations for improvement. Adv. Nutr. 2016, 7, 466–475. [Google Scholar] [CrossRef] [Green Version]
- 2018 Physical Activity Guidelines Advisory Committee Scientific Report. 779. Available online: https://health.gov/our-work/physical-activity/current-guidelines/scientific-report (accessed on 15 April 2022).
- McGuire, S. Scientific Report of the 2015 Dietary Guidelines Advisory Committee. Washington, DC: US Departments of Agriculture and Health and Human Services. Adv. Nutr. 2016, 7, 202–204. [Google Scholar] [CrossRef] [Green Version]
- Sangoseni, O.; Hellman, M.; Hill, C. Development and Validation of a Questionnaire to Assess the Effect of Online Learning on Behaviors, Attitudes, and Clinical Practices of Physical Therapists in the United States Regarding Evidenced-Based Clinical Practice. Internet J. Allied Health Sci. Pract. 2013, 11, 7. [Google Scholar] [CrossRef]
- Ibrahim, A.K.; Kelly, S.J.; Adams, C.E.; Glazebrook, C. A Systematic Review of Studies of Depression Prevalence in University Students. J. Psychiatry Res. 2013, 47, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Solis, A.C.; Lotufo-Neto, F. Predictors of quality of life in Brazilian medical students: A systematic review and meta-analysis. Braz. J. Psychiatry 2019, 41, 556–567. [Google Scholar] [CrossRef] [PubMed]
- Tadi, N.; Pillay, K.; Ejoke, U.P.; Khumalo, I.P. Sex Differences in Depression and Anxiety Symptoms: Measurement Invariance, Prevalence, and Symptom Heterogeneity Among University Students in South Africa. Front. Psychol. 2022, 13, 2872. [Google Scholar] [CrossRef] [PubMed]
- Stok, F.; Renner, B.; Clarys, P.; Lien, N.; Lakerveld, J.; Deliens, T. Understanding Eating Behavior during the Transition from Adolescence to Young Adulthood: A Literature Review and Perspective on Future Research Directions. Nutrients 2018, 10, 667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greaney, M.L.; Less, F.D.; White, A.A.; Dayton, S.F.; Riebe, D.; Blissmer, B.; Shoff, S.; Walsh, J.R.; Greene, G.W. College Students’ Barriers and Enablers for Healthful Weight Management: A Qualitative Study. J. Nutr. Educ. Behav. 2009, 41, 281–286. [Google Scholar] [CrossRef]
- Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2015.
- Deliens, T.; Van Crombruggen, R.; Verbruggen, S.; De Bourdeaudhuij, I.; Deforche, B.; Clarys, P. Dietary Interventions among University Students: A Systematic Review. Appetite 2016, 105, 14–26. [Google Scholar] [CrossRef]
- Kelly, N.R.; Mazzeo, S.E.; Bean, M.K. Systematic Review of Dietary Interventions with College Students: Directions for Future Research and Practice. J. Nutr. Educ. Behav. 2013, 45, 304–313. [Google Scholar] [CrossRef]
- Pratt, M.; Ramirez Varela, A.; Salvo, D.; Kohl III, H.W.; Ding, D. Attacking the Pandemic of Physical Inactivity: What Is Holding Us Back? Br. J. Sports Med. 2020, 54, 760–762. [Google Scholar] [CrossRef]
- Abbasi, P.; Kianipour, N.; Demir Özdenk, G.; Ziapour, A. Dataset of leisure time among students at Kermanshah University of Medical Sciences and its relationship with health-related quality of life (HRQOL). Data Brief 2018, 21, 122–127. [Google Scholar] [CrossRef]
- Nowak, P.F.; Bożek, A.; Blukacz, M. Physical Activity, Sedentary Behavior, and Quality of Life among University Students. BioMed Res. Int. 2019, 2019, 9791281. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N.; Fisher, E.B. Ecological models of health behavior. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; John Wiley & Sons: San Francisco, CA, USA, 2015; pp. 43–64. [Google Scholar]


{kind=link}
| Variables | n (%) |
|---|---|
| Gender | |
| Female | 1892 (78.2) |
| Male | 527 (21.80) |
| Age | |
| 18–20 | 982 (40.6) |
| 21–23 | 925 (38.2) |
| ≥24 | 512 (21.2) |
| Trainings | |
| Bachelor’s program | 1025 (42.4) |
| Medicine–Dental–Pharmacy program | 814 (33.7) |
| Master’s program | 307 (12.7) |
| PhD program | 154 (6.3) |
| Engineering program | 119 (4.9) |
| Discipline of trainings | |
| Health sciences | 1235 (51.1) |
| Technical sciences and engineering | 452 (18.7) |
| Economics | 212 (8.7) |
| Human and social sciences | 249 (10.3) |
| Education sciences | 73 (3.0) |
| Others | 198 (8.2) |
| Regions of Morocco | |
| Casablanca–Settat | 1014 (41.91) |
| Rabat–Sale–Kenitra | 363 (15.01) |
| Fez–Meknes | 314 (12.98) |
| Marrakesh–Safi | 264 (10.91) |
| Oriental | 156 (6.45) |
| Souss–Massa | 122 (5.04) |
| Tangier–Tetouan–Alhouceima | 79 (3.27) |
| Beni Mellal–Khenira | 32 (1.32) |
| Daraa–Tafilalet | 26 (1.07) |
| Guelmim–Oued Noun | 19 (0.79) |
| Laayoune–Sakia Elhamra | 19 (0.79) |
| Dakhla–Oued Ed–Dahab | 11 (0.46) |
| Under medical treatment | |
| Allergy | 237 (9.8) |
| Anxiety/depression | 204 (8.4) |
| Anemia | 215 (8.9) |
| Asthma | 177 (7.3) |
| None | 1586 (65.6) |
| Variables | n (%) | Variables | n (%) |
|---|---|---|---|
| Meal per day | Daily hygiene | ||
| 1–2 | 602 (24.9) | Less than 30 min | 685 (28.3) |
| 3–4 | 1731 (71.6) | 30 min–1 h | 1195 (49.4) |
| >4 | 86 (3.6) | 1 h–1 h 30 | 402 (16.6) |
| Snacking per day | >1 h 30 | 137 (5.7) | |
| None | 653 (27) | Daily household activities | |
| 1–2 | 1406 (58.1) | <1 h | 1408 (58.2) |
| 3–4 | 314 (13) | 1 h–2 h | 797 (32.9) |
| >4 | 46 (1.9) | 2 h–4 h | 194 (8) |
| Interval between Meals (h) | >4 h | 20 (0.8) | |
| 1–2 | 397 (16.4) | Daily homework | |
| 3–4 | 1182 (48.9) | <1 h | 369 (15.3) |
| >4 | 840 (34.7) | 1 h–3 h | 1191 (49.2) |
| Usual bedtime | 3 h–5 h | 642 (26.5) | |
| 8.00 p.m.–10.00 p.m.—22 h | 158 (6.5) | >5 h | 217 (9) |
| 10.00 p.m.–12.00 a.m. | 1487 (61.5) | Time watching TV | |
| 12.00 a.m.–2.00 a.m. | 714 (29.5) | Less than 2 h | 2208 (91.3) |
| After 2.00 a.m. | 60 (2.5) | 2 h–4 h | 189 (7.8) |
| Usual wake-up time | 4 h–6 h | 15 (0.6) | |
| Before 6.00 a.m. | 158 (6.5) | >6 h | 7 (0.3) |
| 6.00 a.m.–8.00 a.m. | 1554 (64.2) | Daily screen time | |
| 8.00 a.m.–10.00 a.m. | 614 (25.4) | Less than 2 h | 399 (16.5) |
| 10.00 a.m.–12.00 p.m. | 80 (3.3) | 2 h–4 h | 1129 (46.7) |
| After 12.00 p.m. | 13 (0.5) | 4 h–6 h | 655 (27.1) |
| Usual nap length | 6 h–8 h | 180 (7.4) | |
| None | 1204 (49.8) | Daily phone calls and SMS | |
| Less than 30 min | 599 (24.8) | Less than 30 min | 1308 (54.1) |
| 30 min–1 h | 444 (18.4) | 30 min–1 h | 671 (27.7) |
| 1 h–2 h | 149 (6.2) | 1 h–2 h | 314 (13) |
| >2 h | 23 (1) | >2 h | 126 (5.2) |
| Daily leisure | Daily social media time | ||
| <1 h | 1254 (51.8) | Less than 30 min | 445 (18.4) |
| 1 h–3 h | 942 (38.9) | 30 min–1 h | 823 (34) |
| 3 h–5 h | 200 (8.3) | 1 h–2 h | 716(29.6) |
| >5 h | 23 (1) | >2 h | 435 (18) |
| Daily physical activity | >8 h | 56 (2.3) | |
| None | 791 (32.7) | ||
| Less than 30 min | 700 (28.9) | ||
| 30 min–1 h | 627 (25.9) | ||
| 1 h–1 h 30 | 215 (8.9) | ||
| >1 h 30 | 86 (3.6) |
| Covariates | β [95% CI] | p-Value |
|---|---|---|
| Under medical treatment | −3.82 [−6.19; −1.46] | 0.002 |
| Meals per day | 0.003 [−1.77; 1.50] | 0.872 |
| Snacking per day | 0.7 [−0.39; 1.78] | 0.208 |
| Sleep time | 5.25 [4.78; 5.72] | <0.0001 |
| Usual nap length | −1.08 [−1.77; −0.39] | 0.002 |
| Daily physical activity | 3.06 [2.16; 3.96] | <0.0001 |
| Daily leisure | 1.87 [0.92; 2.83] | <0.0001 |
| Daily hygiene | 2.39 [1.41; 3.37] | <0.0001 |
| Daily household activities | 1.71 [0.75; 2.67] | <0.0001 |
| Daily homework | 3.61 [2.66; 4.56] | <0.0001 |
| Daily time watching TV | −0.43 [−1.48; 0.63] | 0.43 |
| Daily screen time (smartphone tablet, laptop, and computer) | 0.19 [−0.82; 1.19] | 0.712 |
| Daily social media time | 2.84 [1.77; 3.91] | <0.0001 |
| Daily phone calls and SMS | −0.64 [−1.46; 0.18] | 0.128 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Achak, D.; El-Ammari, A.; Azizi, A.; Youlyouz-Marfak, I.; Saad, E.; Nejjari, C.; Hilali, A.; Marfak, A. Lifestyle Habits Determinants of Health-Related Quality of Life in Moroccan College Students. Int. J. Environ. Res. Public Health 2023, 20, 2394. https://doi.org/10.3390/ijerph20032394
Achak D, El-Ammari A, Azizi A, Youlyouz-Marfak I, Saad E, Nejjari C, Hilali A, Marfak A. Lifestyle Habits Determinants of Health-Related Quality of Life in Moroccan College Students. International Journal of Environmental Research and Public Health. 2023; 20(3):2394. https://doi.org/10.3390/ijerph20032394
Chicago/Turabian StyleAchak, Doha, Abdelghaffar El-Ammari, Asmaa Azizi, Ibtissam Youlyouz-Marfak, Elmadani Saad, Chakib Nejjari, Abderraouf Hilali, and Abdelghafour Marfak. 2023. "Lifestyle Habits Determinants of Health-Related Quality of Life in Moroccan College Students" International Journal of Environmental Research and Public Health 20, no. 3: 2394. https://doi.org/10.3390/ijerph20032394