
Cardiovascular Risk in Patients with Dyslipidemia and Their Degree of Control as Perceived by Primary Care Physicians in a Survey—TERESA-Opinion Study
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Sample
2.3. Variables
2.4. Ethical Aspects
2.5. Statistical Analysis
3. Results
3.1. Physicians Who Responded to the Survey
3.2. Magnitude of Dyslipidemia
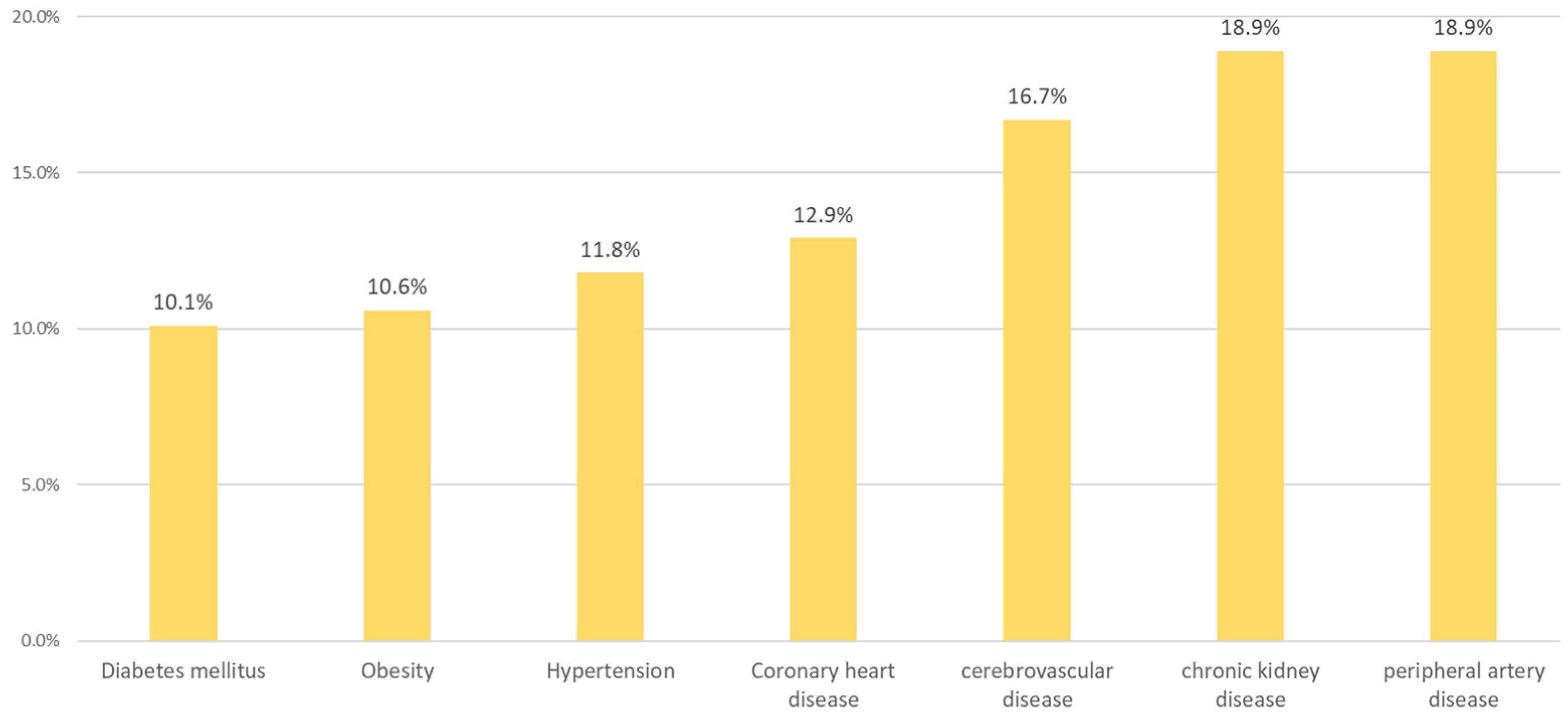
3.3. Comorbidities in Patients with Dyslipidemia
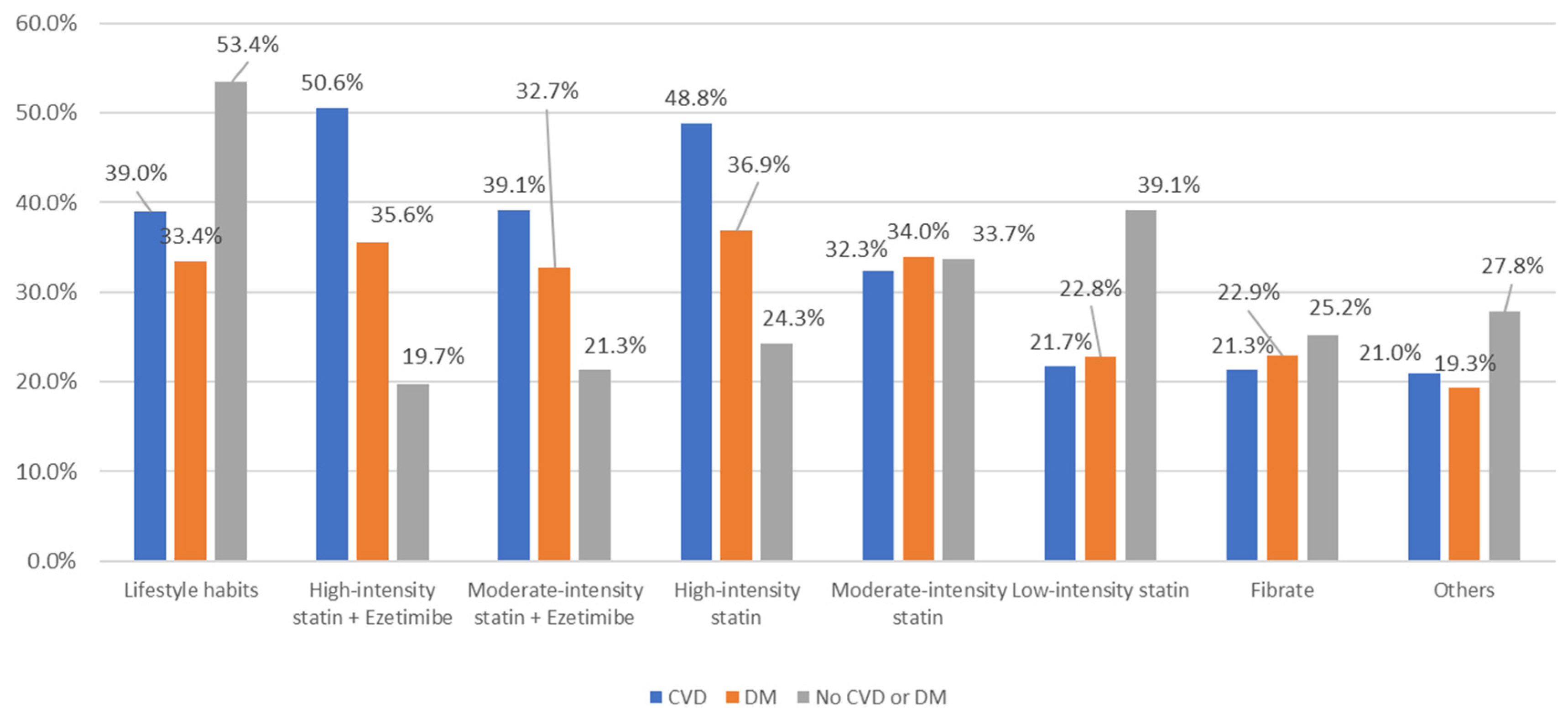
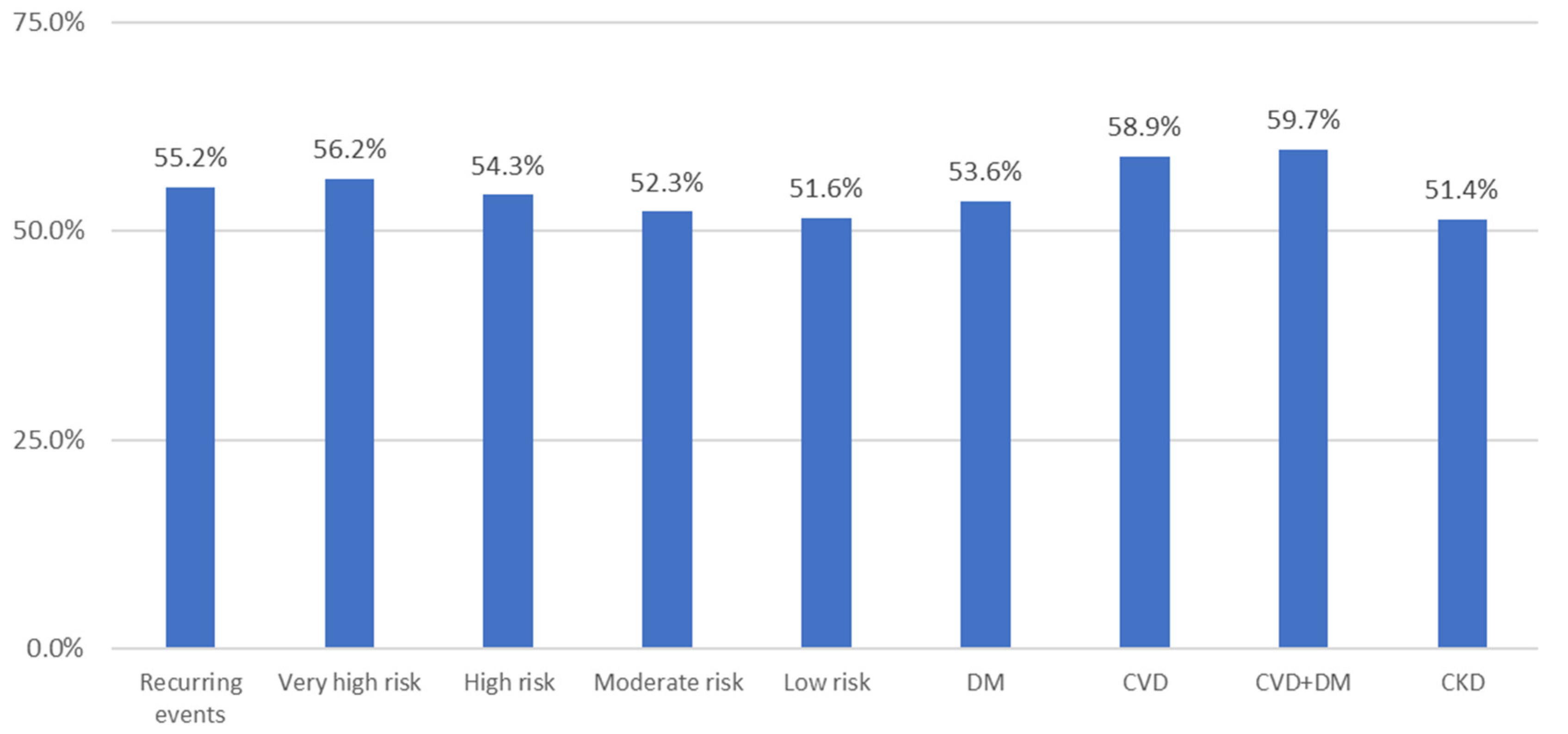
3.4. Opinion on the Degree of Control of Patients
3.5. Safety of Statins
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 29 July 2022).
- Achenbach, S.; Aleksandrova, K.; Amiano, P.; Sebastian, D.-S.; Amouyel, P.; Andersson, J.; Bakker, S.J.L.; da Providencia Costa, R.B.; Beulens, J.W.J.; Blaha, M.; et al. SCORE2 Risk Prediction Algorithms: New Models to Estimate 10-Year Risk of Cardiovascular Disease in Europe. Eur. Heart J. 2021, 42, 2439–2454. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Cai, A.; Nie, Z.; Ou, Y.; Wang, J.; Chen, Y.; Lu, Z.; Liang, Y.; Zhou, Y.; Feng, Y. Association between Sociodemographic Status and Cardiovascular Risk Factors Burden in Community Populations: Implication for Reducing Cardiovascular Disease Burden. BMC Public Health 2022, 22, 1996. [Google Scholar] [CrossRef] [PubMed]
- Cinza Sanjurjo, S.; Llisterri Caro, J.L.; Barquilla García, A.; Polo García, J.; Velilla Zancada, S.; Rodríguez Roca, G.C.; Micó Pérez, R.M.; Martín Sánchez, V.; Prieto Díaz, M.Á. Descripción de La Muestra, Diseño y Métodos Del Estudio Para La Identificación de La Población Española de Riesgo Cardiovascular y Renal (IBERICAN). Med. De Fam. Semer. 2020, 46, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhao, D.; Qi, Y. Global Trends in the Epidemiology and Management of Dyslipidemia. J. Clin. Med. 2022, 11, 6377. [Google Scholar] [CrossRef] [PubMed]
- Jakubiak, G.K.; Pawlas, N.; Cieślar, G.; Stanek, A. Chronic Lower Extremity Ischemia and Its Association with the Frailty Syndrome in Patients with Diabetes. Int. J. Environ. Res. Public Health 2020, 17, 9339. [Google Scholar] [CrossRef]
- Romero Vigara, J.C.; Llisterri Caro, J.L.; Turégano Yedro, M.; Cinza Sanjurjo, S.; Muñoz González, L.; Silvero, Y.A.; Segura Fragoso, A.; Santianes Patiño, J.; García García, J.I.; Benítez Rivero, J. Clinical and Socio-Sanitary Characteristics in Adults Older than 65 Years Attended in the Primary Care Setting. The PYCAF Study. Semergen 2019, 45, 366–374. [Google Scholar] [CrossRef]
- Turégano Yedro, M.; Núñez Villén, A.; Romero Vigara, J.C.; Cinza Sanjurjo, S.; Velilla Zancada, S.; Segura-Fragoso, A.; Ignacio Expósito, J.M.; Benítez Rivero, J.; Esteban Rojas, M.B.; Llisterri Caro, J.L. Risk of Falls and Drug Use in Patients over 65 Years of Age. The PYCAF Study. Semergen 2019, 45, 528–534. [Google Scholar] [CrossRef]
- Baigent, C.; Keech, A.; Kearney, P.M.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Efficacy and Safety of Cholesterol-Lowering Treatment: Prospective Meta-Analysis of Data from 90,056 Participants in 14 Randomised Trials of Statins. Lancet 2005, 366, 1267–1278. [Google Scholar] [CrossRef] [PubMed]
- Jakubiak, G.K.; Pawlas, N.; Cieślar, G.; Stanek, A. Pathogenesis and Clinical Significance of In-Stent Restenosis in Patients with Diabetes. Int. J. Environ. Res. Public Health 2021, 18, 11970. [Google Scholar] [CrossRef]
- Banegas, J.R.; López-García, E.; Dallongeville, J.; Guallar, E.; Halcox, J.P.; Borghi, C.; Massó-González, E.L.; Jiménez, F.J.; Perk, J.; Steg, P.G.; et al. Achievement of Treatment Goals for Primary Prevention of Cardiovascular Disease in Clinical Practice across Europe: The EURIKA Study. Eur. Heart J. 2011, 32, 2143–2152. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; de Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García Ruiz, F.J.; Marín Ibáñez, A.; Pérez-Jiménez, F.; Pintó, X.; Nocea, G.; Ahumada, C.; Alemao, E.; Yin, D. Current Lipid Management and Low Cholesterol Goal Attainment in Common Daily Practice in Spain. The REALITY Study. Pharmacoeconomics 2004, 22 (Suppl. 3), 1–12. [Google Scholar] [CrossRef] [PubMed]
- Galve, E.; Cordero, A.; Cequier, A.; Ruiz, E.; González-Juanatey, J.R. Degree of Lipid Control in Patients With Coronary Heart Disease and Measures Adopted by Physicians. REPAR Study. Rev. Esp. Cardiol. (Engl. Ed.) 2016, 69, 931–938. [Google Scholar] [CrossRef]
- Meier, R.; Rachamin, Y.; Rosemann, T.; Markun, S. The Impact of the 2019 European Guideline for Cardiovascular Risk Management: A Cross-Sectional Study in General Practice. J. Clin. Med. 2020, 9, 2140. [Google Scholar] [CrossRef]
- Liu, M.; Zheng, G.; Cao, X.; Chang, X.; Zhang, N.; Liang, G.; Wang, A.; Yu, Y.; Yang, Y.; Zhao, Y.; et al. Better Medications Adherence Lowers Cardiovascular Events, Stroke, and All-Cause Mortality Risk: A Dose-Response Meta-Analysis. J. Cardiovasc. Dev. Dis. 2021, 8, 146. [Google Scholar] [CrossRef] [PubMed]
- Soriano-Maldonado, C.; Lopez-Pineda, A.; Orozco-Beltran, D.; Quesada, J.A.; Alfonso-Sanchez, J.L.; Pallarés-Carratalá, V.; Navarro-Perez, J.; Gil-Guillen, V.F.; Martin-Moreno, J.M.; Carratala-Munuera, C. Gender Differences in the Diagnosis of Dyslipidemia: ESCARVAL-GENERO. Int. J. Environ. Res. Public Health 2021, 18, 12419. [Google Scholar] [CrossRef]
- Palazón-Bru, A.; Sepehri, A.; Ramírez-Prado, D.; Navarro-Cremades, F.; Cortés, E.; Rizo-Baeza, M.; Gil-Guillén, V.F. Diagnostic Inertia in Dyslipidaemia: Results of a Preventative Programme in Spain. PeerJ 2015, 3, e1109. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Chiang, C.W.; Wang, L.; Brock, G.; Milks, M.W.; Cao, W.; Zhang, P.; Zeng, D.; Donneyong, M.; Li, L. A Multistate Transition Model for Statin-Induced Myopathy and Statin Discontinuation. CPT Pharmacomet. Syst. Pharm. 2021, 10, 1236–1244. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.N.; Blankstein, R. Optimizing Dyslipidemia Management for the Prevention of Cardiovascular Disease: A Focus on Risk Assessment and Therapeutic Options. Curr. Cardiol. Rep. 2019, 21, 110. [Google Scholar] [CrossRef]
- Mert, K.U.; Başaran, Ö.; Mert, G.Ö.; Doğan, V.; Rencüzoğulları, İ.; Özlek, B.; Cinier, G.; Şenol, U.; Çelik, O.; Özlek, E.; et al. Management of LDL-Cholesterol Levels in Patients with Diabetes Mellitus in Cardiology Practice: Real-Life Evidence of Under-Treatment from the EPHESUS Registry. Eur. J. Clin. Investig. 2021, 51, e13528. [Google Scholar] [CrossRef] [PubMed]
- Barrios, V.; Escobar, C.; Gamarra, J.; Obaya, J.C.; Pallarés, V. Manejo Del Paciente Con Dislipidemia En España. Proyecto Cardio Right Care Control Del Riesgo Cardiovascular. Med. De Fam. Semer. 2021, 47, 28–37. [Google Scholar] [CrossRef]
- Cinza-Sanjurjo, S.; Micó-Pérez, R.M.; Velilla-Zancada, S.; Prieto-Díaz, M.A.; Rodríguez-Roca, G.C.; Barquilla García, A.; Polo García, J.; Martín Sánchez, V.; Llisterri Caro, J.L. Factores Asociados al Riesgo Cardiovascular y Enfermedad Cardiovascular y Renal En El Estudio IBERICAN (Identificación de La PoBlación Española de RIesgo CArdiovascular y ReNal): Resultados Definitivos. Med. De Fam. Semer. 2020, 46, 368–378. [Google Scholar] [CrossRef]
- Ruiz-García, A.; Arranz-Martínez, E.; García-Álvarez, J.C.; Morales-Cobos, L.E.; García-Fernández, M.E.; de la Peña-Antón, N.; Martín Calle, M.C.; Díez Pérez, M.C.; Montero Costa, A.; Palacios Martínez, D.; et al. Población y Metodología Del Estudio SIMETAP: Prevalencia de Factores de Riesgo Cardiovascular, Enfermedades Cardiovasculares y Enfermedades Metabólicas Relacionadas. Clin. Investig. Arterioscler. 2018, 30, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Cinza Sanjurjo, S.; Prieto Díaz, M.Á.; Llisterri Caro, J.L.; Barquilla García, A.; Rodríguez Padial, L.; Vidal Pérez, R.; Rodríguez Roca, G.C.; Badimón Maestro, J.J.; Pallarés Carratalá, V. Prevalencia de Obesidad y Comorbilidad Cardiovascular Asociada En Los Pacientes Incluidos En El Estudio IBERICAN (Identificación de La PoBlación Española de RIesgo CArdiovascular y ReNal). Med. Fam. Semer. 2019, 45, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Plana, N.; Ibarretxe, D.; Cabré, A.; Ruiz, E.; Masana, L. Prevalence of Atherogenic Dyslipidemia in Primary Care Patients at Moderate-Very High Risk of Cardiovascular Disease. Cardiovascular Risk Perception. Clin. Investig. Arterioscler. 2014, 26, 274–284. [Google Scholar] [CrossRef]
- Barrios, V.; Soronen, J.; Carter, A.M.; Anastassopoulou, A. Lipid Management across Europe in the Real-World Setting: A Rapid Evidence Review. Curr. Med. Res. Opin. 2021, 37, 2049–2059. [Google Scholar] [CrossRef]
- Ruiz-García, A.; Arranz-Martínez, E.; García-Fernández, M.E.; Cabrera-Vélez, R.; García-Pliego, R.A.; Morales-Cobos, L.E.; Sanz-Pozo, B.; Gómez-Díaz, E.; Rodríguez-de-Mingo, E.; Rico-Pérez, M.R.; et al. Related Cardiometabolic Factors and Prevalence of Low HDL-Cholesterol Levels and Atherogenic Dyslipidemia. SIMETAP-AD Study. Clin. Investig. Arterioscler. 2020, 33, 19–29. [Google Scholar] [CrossRef]
- Barrios, V.; Castellanos, M.; Campuzano Ruiz, R.; Gómez Cerezo, J.F.; Egocheaga Cabello, I.; Gámez, J.M.; Martínez López, I.; Mostaza, J.M.; Morant Talamante, N.; Parrondo, J.; et al. Treatment Patterns and Use of Healthcare Resources of Patients with Atherosclerotic Cardiovascular Disease and Hypercholesterolemia and Patients with Familial Hypercholesterolemia in Spain: Protocol of the Reality Study. Front. Cardiovasc. Med. 2022, 9, 966049. [Google Scholar] [CrossRef]
- Maffei, S.; Meloni, A.; Deidda, M.; Sciomer, S.; Cugusi, L.; Cadeddu, C.; Gallina, S.; Franchini, M.; Scambia, G.; Mattioli, A.V.; et al. Cardiovascular Risk Perception and Knowledge among Italian Women: Lessons from IGENDA Protocol. J. Clin. Med. 2022, 11, 1695. [Google Scholar] [CrossRef]
- Mosca, L. Awareness, Perception, and Knowledge of Heart Disease Risk and Prevention Among Women in the United States. Arch. Fam. Med. 2000, 9, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Chapman, N.; McWhirter, R.E.; Schultz, M.G.; Ezzy, D.; Nelson, M.R.; Sharman, J.E. General Practitioner Perceptions of Assessment and Reporting of Absolute Cardiovascular Disease Risk via Pathology Services: A Qualitative Study. Fam. Pract. 2021, 38, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Van Steenkiste, B.; van der Weijden, T.; Stoffers, H.E.; Kester, A.D.; Timmermans, D.R.; Grol, R. Improving Cardiovascular Risk Management: A Randomized, Controlled Trial on the Effect of a Decision Support Tool for Patients and Physicians. Eur. J. Prev. Cardiol. 2007, 14, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Molemans, B.; Schoonen, W.M.; Giovas, P.; Bray, S.; Kiru, G.; Murphy, J.; Banach, M.; de Servi, S.; Gaita, D.; et al. EU-Wide Cross-Sectional Observational Study of Lipid-Modifying Therapy Use in Secondary and Primary Care: The DA VINCI Study. Eur. J. Prev. Cardiol. 2020, 28, 1279–1289. [Google Scholar] [CrossRef] [PubMed]
- Reiner, Ž.; Sonicki, Z.; Tedeschi-Reiner, E. Physicians’ Perception, Knowledge and Awareness of Cardiovascular Risk Factors and Adherence to Prevention Guidelines: The PERCRO-DOC Survey. Atherosclerosis 2010, 213, 598–603. [Google Scholar] [CrossRef]
- Heeley, E.L.; Peiris, D.P.; Patel, A.A.; Cass, A.; Weekes, A.; Morgan, C.; Anderson, C.S.; Chalmers, J.P. Cardiovascular Risk Perception and Evidence–Practice Gaps in Australian General Practice (the AusHEART Study). Med. J. Aust. 2010, 192, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Cinza Sanjurjo, S.; Prieto Díaz, M.Á.; Llisterri Caro, J.L.; Pallarés Carratalá, V.; Barquilla García, A.; Rodríguez Padial, L.; Díaz Rodríguez, Á.; Polo García, J.; Vergara Martín, J.; Vidal Pérez, R.; et al. Características Basales y Manejo Clínico de Los Primeros 3.000 Pacientes Incluidos En El Estudio IBERICAN (Identificación de La Población Española de Riesgo Cardiovascular y Renal). Semer. Med. De Fam. 2017, 43, 493–500. [Google Scholar] [CrossRef]
- Mach, F.; Ray, K.K.; Wiklund, O.; Corsini, A.; Catapano, A.L.; Bruckert, E.; de Backer, G.; Hegele, R.A.; Hovingh, G.K.; Jacobson, T.A.; et al. Adverse Effects of Statin Therapy: Perception vs. the Evidence—Focus on Glucose Homeostasis, Cognitive, Renal and Hepatic Function, Haemorrhagic Stroke and Cataract. Eur. Heart J. 2018, 39, 2526–2539. [Google Scholar] [CrossRef] [Green Version]
- Howard, J.P.; Wood, F.A.; Finegold, J.A.; Nowbar, A.N.; Thompson, D.M.; Arnold, A.D.; Rajkumar, C.A.; Connolly, S.; Cegla, J.; Stride, C.; et al. Side Effect Patterns in a Crossover Trial of Statin, Placebo, and No Treatment. J. Am. Coll. Cardiol. 2021, 78, 1210–1222. [Google Scholar] [CrossRef]
- Gupta, M.; Singh, N.; Tsigoulis, M.; Kajil, M.; Hirjikaka, S.; Quan, A.; Teoh, H.; Verma, S. Perceptions of Canadian Primary Care Physicians Towards Cardiovascular Risk Assessment and Lipid Management. Can. J. Cardiol. 2012, 28, 14–19. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | % | ||
|---|---|---|---|
| Autonomous Community | Andalusia | 45 | 15.0 |
| Aragon | 13 | 4.3 | |
| Principality of Asturias | 8 | 2.7 | |
| Balearic Islands | 6 | 2.0 | |
| Canary Islands | 16 | 5.3 | |
| Cantabria | 4 | 1.3 | |
| Castilla y Leon | 22 | 7.3 | |
| Castilla La Mancha | 16 | 5.3 | |
| Catalonia | 35 | 11.7 | |
| Valencian Community | 40 | 13.3 | |
| Extremadura | 10 | 3.3 | |
| Galicia | 23 | 7.7 | |
| Community of Madrid | 34 | 11.3 | |
| Region of Murcia | 11 | 3.7 | |
| Foral Community of Navarra | 3 | 1.0 | |
| Basque Country | 10 | 3.3 | |
| La Rioja | 1 | 0.3 | |
| Autonomous City of Melilla | 3 | 1.0 | |
| Total | 300 | 100.0 | |
| % | Mean | SD | Median | Q1 | Q3 | Minimum | Maximum | N |
|---|---|---|---|---|---|---|---|---|
| Switch to nutraceutical | 13.1 | 24.5 | 0.0 | 0.0 | 10.0 | 0.0 | 100.0 | 268 |
| Switch to another statin | 79.9 | 28.3 | 90.0 | 70.0 | 100.0 | 5.0 | 100.0 | 35 |
| Switch to another statin or reduce the dose of the same statin | 100.0 | - | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 1 |
| Switch to another drug | 67.5 | 34.8 | 80.0 | 30.0 | 100.0 | 1.0 | 100.0 | 61 |
| Reduce the dose of the same statin | 65.0 | 52.2 | 90.0 | 5.0 | - | 5.0 | 100.0 | 3 |
| Discontinue the statin | 97.5 | 3.5 | 97.5 | 95.0 | - | 95.0 | 100.0 | 2 |
| Others | 52.3 | 42.4 | 40.0 | 7.5 | 95.0 | 5.0 | 100.0 | 13 |
| Lifestyle habits | 34.4 | 38.9 | 20.0 | 5.0 | 70.0 | 5.0 | 100.0 | 9 |
| Lifestyle habits and switch to another drug | 90.0 | - | 90.0 | 90.0 | 90.0 | 90.0 | 90.0 | 1 |
| Others | 93.3 | 5.8 | 90.0 | 90.0 | - | 90.0 | 100.0 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pallarés-Carratalá, V.; Barrios, V.; Fierro-González, D.; Polo-García, J.; Cinza-Sanjurjo, S. Cardiovascular Risk in Patients with Dyslipidemia and Their Degree of Control as Perceived by Primary Care Physicians in a Survey—TERESA-Opinion Study. Int. J. Environ. Res. Public Health 2023, 20, 2388. https://doi.org/10.3390/ijerph20032388
Pallarés-Carratalá V, Barrios V, Fierro-González D, Polo-García J, Cinza-Sanjurjo S. Cardiovascular Risk in Patients with Dyslipidemia and Their Degree of Control as Perceived by Primary Care Physicians in a Survey—TERESA-Opinion Study. International Journal of Environmental Research and Public Health. 2023; 20(3):2388. https://doi.org/10.3390/ijerph20032388
Chicago/Turabian StylePallarés-Carratalá, Vicente, Vivencio Barrios, David Fierro-González, Jose Polo-García, and Sergio Cinza-Sanjurjo. 2023. "Cardiovascular Risk in Patients with Dyslipidemia and Their Degree of Control as Perceived by Primary Care Physicians in a Survey—TERESA-Opinion Study" International Journal of Environmental Research and Public Health 20, no. 3: 2388. https://doi.org/10.3390/ijerph20032388