

Stressors and Impact of the COVID-19 Pandemic on Vulnerable Hispanic Caregivers and Children

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Instruments
2.3. Statistical Analysis
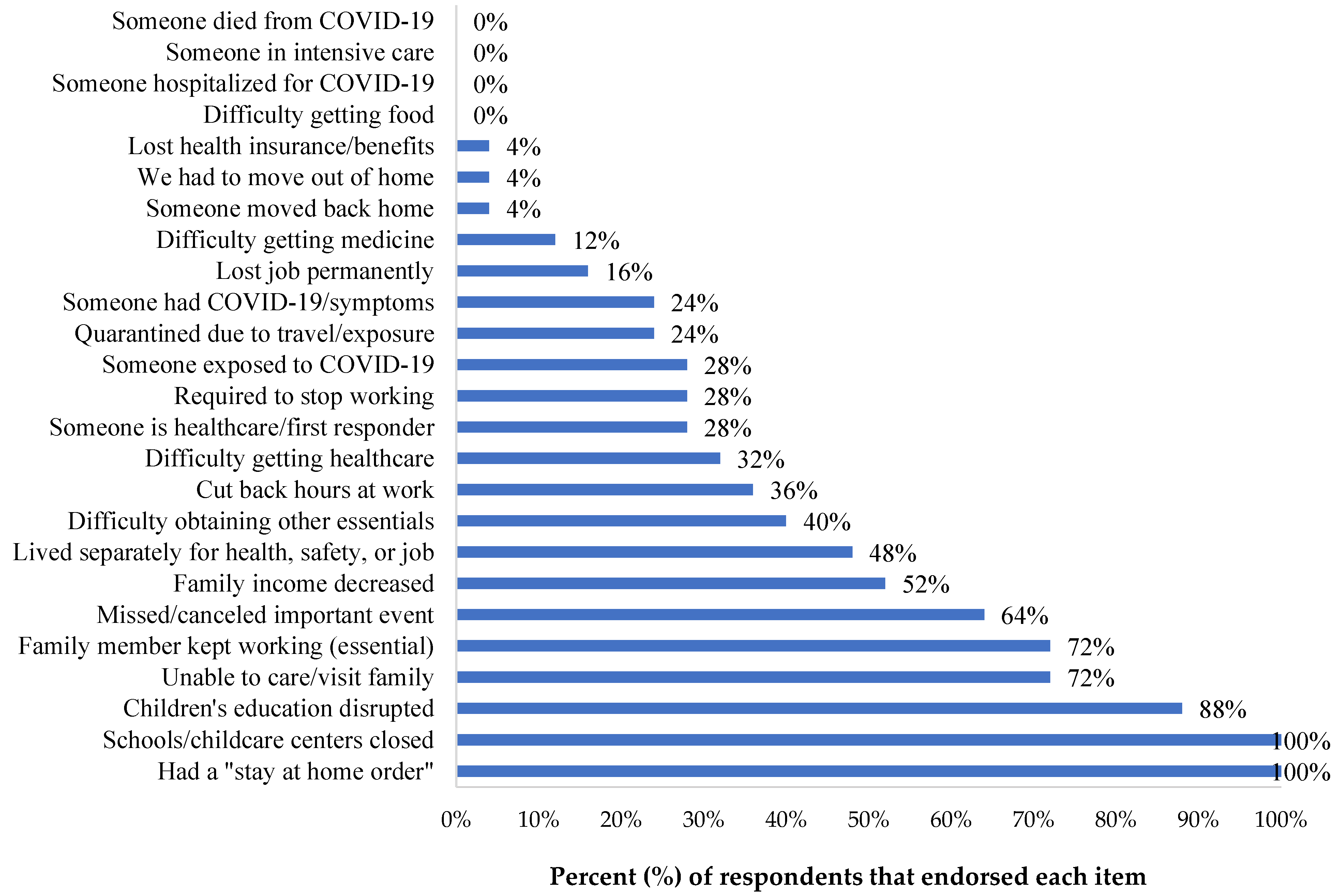
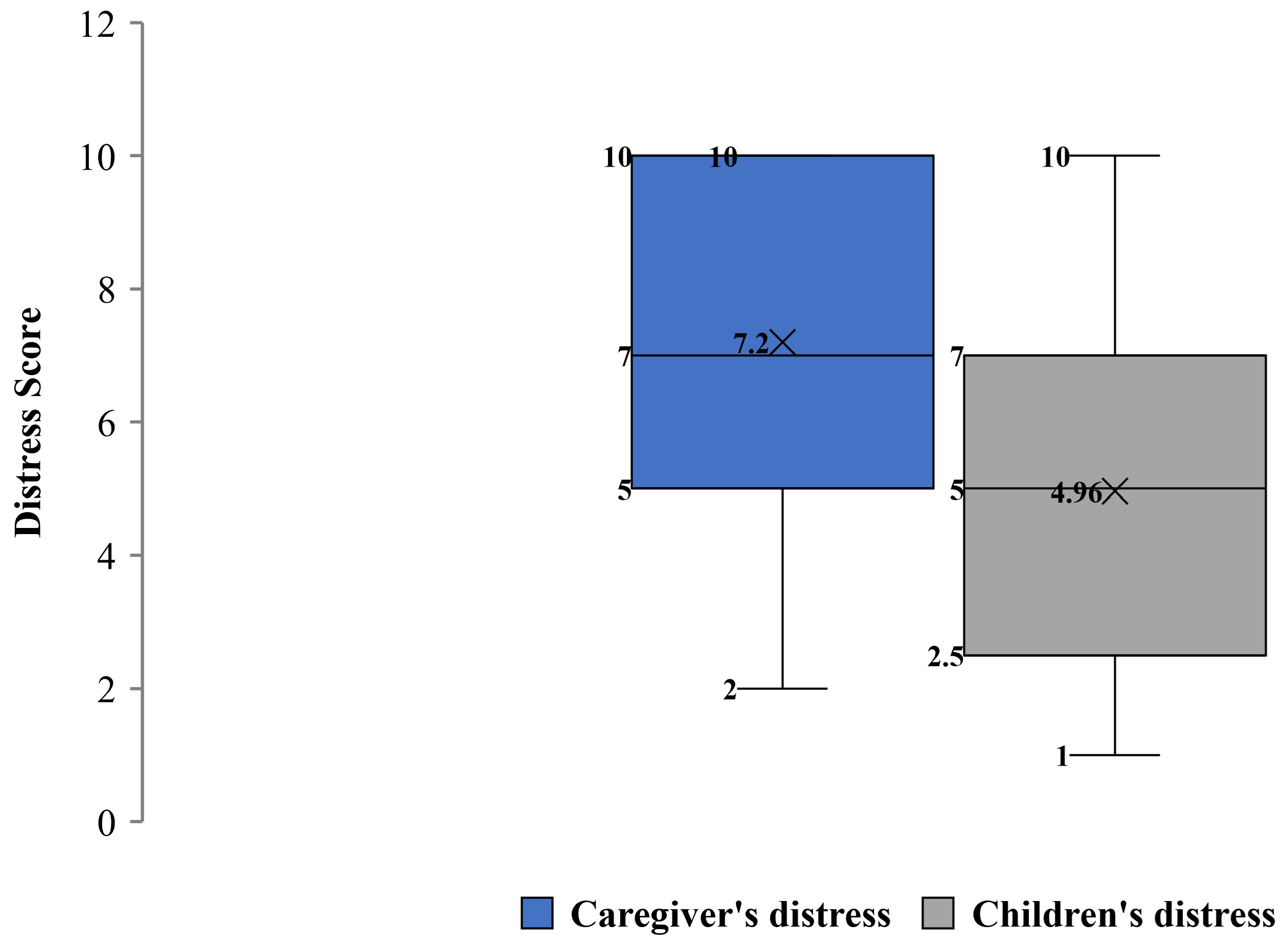
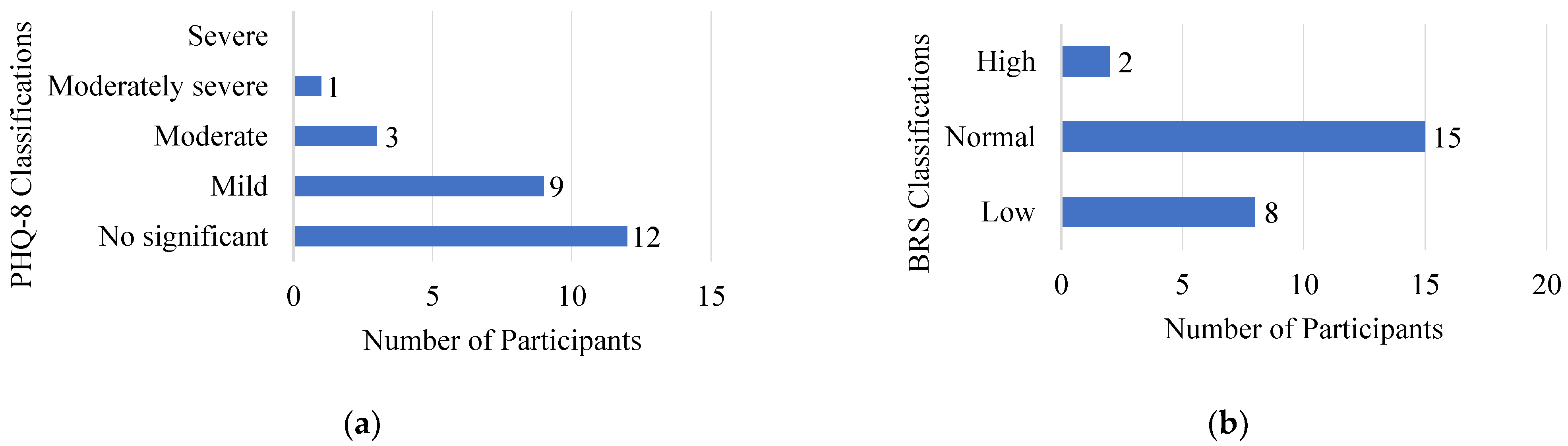
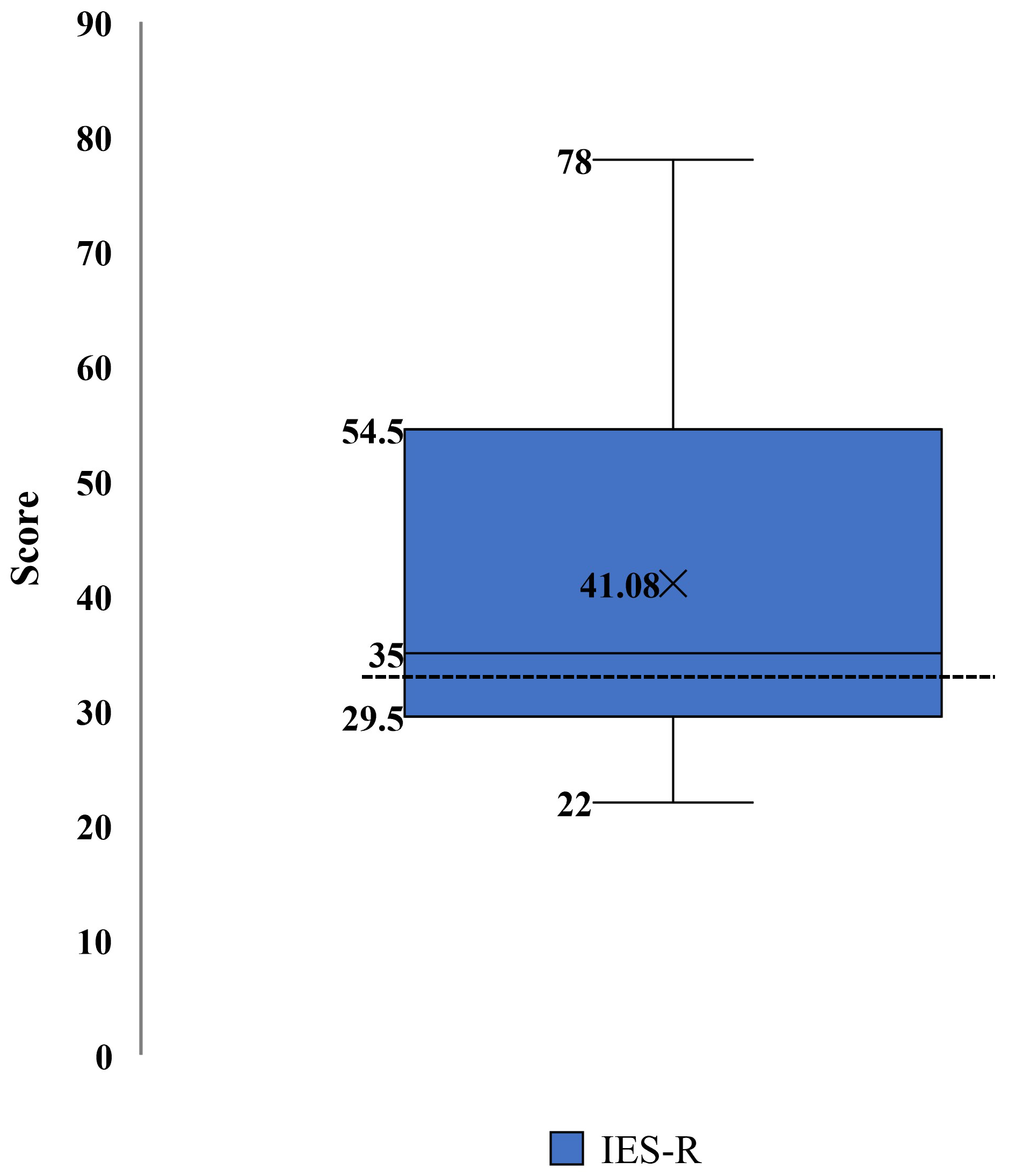
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Center on the Developing Child. The Impact of Early Adversity on Child Development (InBrief). Available online: www.developingchild.harvard.edu (accessed on 15 May 2022).
- Delardas, O.; Kechagias, K.S.; Pontikos, P.N.; Giannos, P. Socio-Economic Impacts and Challenges of the Coronavirus Pandemic (COVID-19): An Updated Review. Sustainability 2022, 14, 9699. [Google Scholar] [CrossRef]
- Russell, B.S.; Hutchison, M.; Tambling, R.; Tomkunas, A.J.; Horton, A.L. Initial Challenges of Caregiving During COVID-19: Caregiver Burden, Mental Health, and the Parent–Child Relationship. Child Psychiatry Hum. Dev. 2020, 51, 671–682. [Google Scholar] [CrossRef]
- Prime, H.; Wade, M.; Browne, D.T. Pandemic-Related Disruption and Positive Adaptation: Profiles of Family Function at the Onset of the Pandemic. Advers. Resil. Sci. 2022, 3, 321–333. [Google Scholar] [CrossRef]
- Cluver, L.; Lachman, J.M.; Sherr, L.; Wessels, I.; Krug, E.; Rakotomalala, S.; Blight, S.; Hillis, S.; Bachman, G.; Green, O.; et al. Parenting in a time of COVID-19. Lancet 2020, 395, e64. [Google Scholar] [CrossRef]
- Hong, S.; Kim, H.; Park, M.K. Impact of COVID-19 on post-traumatic stress symptoms in the general population: An integrative review. Int. J. Ment. Health Nurs. 2021, 30, 834–846. [Google Scholar] [CrossRef]
- Nurius, P.S.; Green, S.; Logan-Greene, P.; Borja, S. Life course pathways of adverse childhood experiences toward adult psychological well-being: A stress process analysis. Child Abus. Negl. 2015, 45, 143–153. [Google Scholar] [CrossRef] [Green Version]
- Nelson, C.A.; Scott, R.D.; Bhutta, Z.A.; Harris, N.B.; Danese, A.; Samara, M. Adversity in childhood is linked to mental and physical health throughout life. BMJ 2020, 371, m3048. [Google Scholar] [CrossRef]
- Duffy, A.R.; Schminkey, D.L.; Groer, M.W.; Shelton, M.; Dutra, S. Comparison of Hair Cortisol Levels and Perceived Stress in Mothers Who Deliver at Preterm and Term. Biol. Res. Nurs. 2018, 20, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Garner, A.; Yogman, M.; Committee on Psychosocial Aspects of Child and Family Health. Preventing Childhood Toxic Stress: Partnering With Families and Communities to Promote Relational Health. Pediatrics 2021, 148, e2021052582. [Google Scholar] [CrossRef] [PubMed]
- Davidson, B.; Schmidt, E.; Mallar, C.; Mahmoud, F.; Rothenberg, W.; Hernandez, J.; Berkovits, M.; Jent, J.; Delamater, A.; Natale, R. Risk and resilience of well-being in caregivers of young children in response to the COVID-19 pandemic. Transl. Behav. Med. 2020, 11, 305–313. [Google Scholar] [CrossRef]
- Davico, C.; Ghiggia, A.; Marcotulli, D.; Ricci, F.; Amianto, F.; Vitiello, B. Psychological Impact of the COVID-19 Pandemic on Adults and Their Children in Italy. Front. Psychiatry 2021, 12, 572997. [Google Scholar] [CrossRef] [PubMed]
- Coller, R.J.; Webber, S. COVID-19 and the Well-being of Children and Families. Pediatrics 2020, 146, e2020022079. [Google Scholar] [CrossRef] [PubMed]
- Scaramutti, C.; Salas-Wright, C.P.; Vos, S.R.; Schwartz, S.J. The Mental Health Impact of Hurricane Maria on Puerto Ricans in Puerto Rico and Florida. Disaster Med. Public Health Prep. 2019, 13, 24–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, S.J.; Montero-Zamora, P.; Salas-Wright, C.P.; Brown, E.C.; Garcia, M.F.; Scaramutti, C.; Rodríguez, J.; Piñeros-Leaño, M.; Bates, M.M.; Maldonado-Molina, M.M. After Hurricane Maria: Effects of disaster trauma on Puerto Rican survivors on the U.S. mainland. Psychol. Trauma Theory Res. Pract. Policy 2022. [Google Scholar] [CrossRef]
- Rodriguez-Rabassa, M.; Hernandez, R.; Rodriguez, Z.; Colon-Echevarria, C.B.; Maldonado, L.; Tollinchi, N.; Torres-Marrero, E.; Mulero, A.; Albors, D.; Perez-Morales, J.; et al. Impact of a natural disaster on access to care and biopsychosocial outcomes among Hispanic/Latino cancer survivors. Sci. Rep. 2020, 10, 10376. [Google Scholar] [CrossRef] [PubMed]
- Peña-Vargas, C.; Toro-Morales, Y.; Valentin, P.; López, M.; Rodriguez-Castro, Z.; Hernandez-Torres, R.; Tollinchi-Natali, N.; Torres-Blasco, N.; Pereira, C.; Armaiz-Pena, G.N.; et al. Impact of Seismic Activity on Access to Health Care in Hispanic/Latino Cancer Patients from Puerto Rico. Int. J. Environ. Res. Public Health 2022, 19, 4246. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. Quick Facts: Puerto Rico. Available online: https://www.census.gov/quickfacts/PR (accessed on 8 May 2020).
- U.S. Census Bureau. Quick Facts: United States. Available online: https://www.census.gov/quickfacts/fact/table/US/PST045222 (accessed on 26 December 2022).
- Instituto del Desarrollo de la Juventud. Un Futuro de Pobreza Infantil: ¿Cuánto nos Cuesta y qué Podemos Hacer? Available online: https://www.cuantonoscuesta.com/_files/ugd/011d36_e9e87928b7e049fe990fceb25ce6d944.pdf (accessed on 5 December 2022).
- Easterly, C.; Kim, D.; Steiner, M.J.; Dejong, N.A. Childcare and Employment Disruptions in 2020 Among Caregivers of Children With and Without Special Health Care Needs. JAMA Pediatr. 2022, 176, 941–943. [Google Scholar] [CrossRef]
- Alvarado-Domenech, L.I.; Rivera-Amill, V.; Appleton, A.A.; Rosario-Villafañe, V.; Repollet-Carrer, I.; Borges-Rodríguez, M.; Pérez-Rodríguez, N.M.; Olivieri-Ramos, O.; González, M.; González-Montalvo, C.; et al. Early Childhood Neurodevelopmental Outcomes in Children with Prenatal Zika Virus Exposure: A Cohort Study in Puerto Rico. J. Pediatr. 2022, 247, 38–45.e5. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, C.M.; Strader, L.C.; Pratt, J.G.; Maiese, D.; Hendershot, T.; Kwok, R.; Hammond, J.A.; Huggins, W.; Jackman, D.; Pan, H.; et al. The PhenX Toolkit: Get the Most From Your Measures. Am. J. Epidemiol. 2011, 174, 253–260. [Google Scholar] [CrossRef]
- A cross-cultural study of spirituality, religion, and personal beliefs as components of quality of life. Soc. Sci. Med. 2006, 62, 1486–1497. [CrossRef] [PubMed]
- Kazak, A.E.; Alderfer, M.; Enlow, P.T.; Lewis, A.M.; Vega, G.; Barakat, L.; Kassam-Adams, N.; Pai, A.; Canter, K.S.; Hildenbrand, A.K.; et al. COVID-19 Exposure and Family Impact Scales: Factor Structure and Initial Psychometrics. J. Pediatr. Psychol. 2021, 46, 504–513. [Google Scholar] [CrossRef]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Epstein, E.E.; Oritz, J.A.; Christopher, P.K.; Tooley, E.M. The Foundations of Resilience: What are the critical resources for bouncing back from stress? In Resilience in Children, Adolescents, and Adults: Translating Research into Practice; Prince-Embury, S., Saklofske, D.H., Eds.; Springer: New York, NY, USA, 2013. [Google Scholar]
- Weiss, D.S.; Marmar, C.R. The Impact of Event Scale-Revised; Wilson, J.P., Keane, T.M., Eds.; Guilford: New York, NY, USA, 1997. [Google Scholar]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the Impact of Event Scale—Revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef]
- Kirschbaum, C.; Tietze, A.; Skoluda, N.; Dettenborn, L. Hair as a retrospective calendar of cortisol production—Increased cortisol incorporation into hair in the third trimester of pregnancy. Psychoneuroendocrinology 2009, 34, 32–37. [Google Scholar] [CrossRef]
- Short, S.J.; Stalder, T.; Marceau, K.; Entringer, S.; Moog, N.K.; Shirtcliff, E.A.; Wadhwa, P.D.; Buss, C. Correspondence between hair cortisol concentrations and 30-day integrated daily salivary and weekly urinary cortisol measures. Psychoneuroendocrinology 2016, 71, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Meyer, J.; Novak, M.; Hamel, A.; Rosenberg, K. Extraction and Analysis of Cortisol from Human and Monkey Hair. J. Vis. Exp. 2014, 83, e50882. [Google Scholar] [CrossRef] [Green Version]
- Kroshko, T.; Kapronczai, L.; Cattet, M.R.; Macbeth, B.J.; Stenhouse, G.B.; Obbard, M.E.; Janz, D.M. Comparison of methanol and isopropanol as wash solvents for determination of hair cortisol concentration in grizzly bears and polar bears. MethodsX 2017, 4, 68–75. [Google Scholar] [CrossRef]
- Schneider, A.; Hommel, G.; Blettner, M. Linear regression analysis: Part 14 of a series on evaluation of scientific publications. Dtsch. Arztebl. Int. 2010, 107, 776–782. [Google Scholar] [CrossRef]
- IBM SPSS Statistics for Windows, Version 28.0; IBM Corp: Armonk, NY, USA, 2021.
- Bayley, N. Bayley Scales of Infant and Toddler Development: Administration Manual; Pearson: London, UK, 2006. [Google Scholar]
- Goldman, N.; Pebley, A.R.; Lee, K.; Andrasfay, T.; Pratt, B. Racial and ethnic differentials in COVID-19-related job exposures by occupational standing in the US. PLoS ONE 2021, 16, e0256085. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Balcazar, Y.; Mirza, M.; Errisuriz, V.; Zeng, W.; Brown, J.; Vanegas, S.; Heydarian, N.; Parra-Medina, D.; Morales, P.; Torres, H.; et al. Impact of COVID-19 on the Mental Health and Well-Being of Latinx Caregivers of Children with Intellectual and Developmental Disabilities. Int. J. Environ. Res. Public Health 2021, 18, 7971. [Google Scholar] [CrossRef] [PubMed]
- Deeb, S.; Madden, D.; Ghebretinsae, T.; Lin, J.; Ozbek, U.; Mayer, V.; Vangeepuram, N. Child Disruptions, Remote Learning, and Parent Mental Health during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 6442. [Google Scholar] [CrossRef]
- Enlow, P.T.; Phan, T.-L.T.; Lewis, A.M.; Hildenbrand, A.K.; Sood, E.; Canter, K.S.; Vega, G.; Alderfer, M.A.; Kazak, A.E. Validation of the COVID-19 Exposure and Family Impact Scales. J. Pediatr. Psychol. 2021, 47, 259–269. [Google Scholar] [CrossRef]
- Patrick, S.W.; Henkhaus, L.E.; Zickafoose, J.S.; Lovell, K.; Halvorson, A.; Loch, S.; Letterie, M.; Davis, M.M. Well-being of Parents and Children During the COVID-19 Pandemic: A National Survey. PEDIATRICS 2020, 146, e2020016824. [Google Scholar] [CrossRef]
- Yue, J.; Zang, X.; Le, Y.; An, Y. Anxiety, depression and PTSD among children and their parent during 2019 novel coronavirus disease (COVID-19) outbreak in China. Curr. Psychol. 2020, 41, 5723–5730. [Google Scholar] [CrossRef]
- Carducci, C.; Rapini, N.; Deodati, A.; Pampanini, V.; Cianfarani, S.; Schiaffini, R. Post-traumatic stress disorder (PTSD) in parents of children with type 1 diabetes during Covid-19 pandemic. Ital. J. Pediatr. 2021, 47, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Partika, A.; Castle, S.; Horm, D.; Johnson, A.D. Both sides of the screen: Predictors of parents’ and teachers’ depression and food insecurity during COVID-19-related distance learning. Early Child. Res. Q. 2022, 60, 237–249. [Google Scholar] [CrossRef]
- Barrero-Castillero, A.; Morton, S.U.; Nelson, C.A.; Smith, V.C. Psychosocial Stress and Adversity: Effects from the Perinatal Period to Adulthood. Neoreviews 2019, 20, e686–e696. [Google Scholar] [CrossRef]
- Kitani, R.A.; Letsou, K.; Kokka, I.; Kanaka-Gantenbein, C.; Bacopoulou, F. Difference in Hair Cortisol Concentrations between Obese and Non-Obese Children and Adolescents: A Systematic Review. Children 2022, 9, 715. [Google Scholar] [CrossRef]
- Prado-Gascó, V.; De La Barrera, U.; Sancho-Castillo, S.; De La Rubia-Ortí, J.E.; Montoya-Castilla, I. Perceived stress and reference ranges of hair cortisol in healthy adolescents. PLoS ONE 2019, 14, e0214856. [Google Scholar] [CrossRef] [PubMed]
- Sauvé, B.; Koren, G.; Walsh, G.; Tokmakejian, S.; Van Uum, S.H. Measurement of cortisol in human Hair as a biomarker of systemic exposure. Clin. Investig. Med. 2007, 30, E183–E191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steudte, S.; Kirschbaum, C.; Gao, W.; Alexander, N.; Schönfeld, S.; Hoyer, J.; Stalder, T. Hair Cortisol as a Biomarker of Traumatization in Healthy Individuals and Posttraumatic Stress Disorder Patients. Biol. Psychiatry 2013, 74, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Van Zuiden, M.; Savas, M.; Koch, S.B.; Nawijn, L.; Staufenbiel, S.M.; Frijling, J.L.; Veltman, D.J.; Van Rossum, E.F.; Olff, M. Associations Among Hair Cortisol Concentrations, Posttraumatic Stress Disorder Status, and Amygdala Reactivity to Negative Affective Stimuli in Female Police Officers. J. Trauma. Stress 2019, 32, 238–248. [Google Scholar] [CrossRef]
- Steudte-Schmiedgen, S.; Stalder, T.; Schönfeld, S.; Wittchen, H.-U.; Trautmann, S.; Alexander, N.; Miller, R.; Kirschbaum, C. Hair cortisol concentrations and cortisol stress reactivity predict PTSD symptom increase after trauma exposure during military deployment. Psychoneuroendocrinology 2015, 59, 123–133. [Google Scholar] [CrossRef]
- Forseth, B.; Dean, K.M.; Murray, M.; Killian, H.J.; Bakula, D.; Romine, R.E.S.; Fleming, K.; Befort, C.A.; England, K.M.; Bhagat, R.; et al. The impact of COVID-19 on rural treatment-seeking families with children with overweight or obesity. Child. Health Care 2022, 51, 300–315. [Google Scholar] [CrossRef]
- Valenzuela, J.M.; Dimentstein, K.; Yee, S.; Pan, B.; Snyder, M.C.; Wolf, R.M. Psychosocial Impact of the COVID-19 Pandemic in Racially/Ethnically Diverse Youth With Diabetes. J. Pediatr. Psychol. 2022. [Google Scholar] [CrossRef]
- Lim, T.S.H.; Tan, M.Y.; Aishworiya, R.; Kang, Y.Q.; Koh, M.Y.; Shen, L.; Chong, S.C. Factors Contributing to Psychological Ill-Effects and Resilience of Caregivers of Children with Developmental Disabilities During a Nation-wide Lockdown During the COVID-19 Pandemic. J. Autism Dev. Disord. 2021, 52, 3015–3025. [Google Scholar] [CrossRef]
- Singh, G.K.; Daus, G.P.; Allender, M.; Ramey, C.T.; Martin, E.K.; Perry, C.; Reyes, A.A.D.L.; Vedamuthu, I.P. Social Determinants of Health in the United States: Addressing Major Health Inequality Trends for the Nation, 1935-2016. Int. J. MCH AIDS 2017, 6, 139–164. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Caregiver’s Characteristics | n (%) |
|---|---|
| Age in years, mean ± standard deviation | 30.4 ± 6.59 |
| Sex, female | 23 (92.0) |
| Household income | |
| Less than $10,000 | 12 (48.0) |
| $10,000–$14,999 | 7 (28.0) |
| $15,000–$24,999 | 4 (16.0) |
| $35,000–$49,999 | 2 (8.0) |
| Educational attainment | |
| High school | 8 (32.0) |
| Technical/occupational degree | 11 (44.0) |
| Associate or bachelor’s degree | 6 (24.0) |
| Employment status, not working | 17 (68.0) |
| Marital status | |
| Married/cohabitating | 15 (60.0) |
| Single | 8 (32.0) |
| Other * | 2 (8.0) |
| Health insurance | |
| Public | 20 (80.0) |
| Private | 4 (16.0) |
| None | 1 (4.0) |
| Race | |
| White | 5 (20.0) |
| Other [Mexican, Puerto Rican, Cuban, Dominican, South American] | 19 (76.0) |
| “Don’t know” | 1 (4.0) |
| History of mental health problems | |
| Anxiety or depression | 3 (12.0) |
| None | 22 (88.0) |
| Food security indicator | |
| High or marginal food security | 15 (60.0) |
| Low or very low food security | 10 (40.0) |
| Participants’ POPZE child characteristics | |
| Age in years, mean ± standard deviation | 2.8 ± 0.71 |
| Sex, female | 15 (60.0) |
| Race | |
| White | 5 (20.0) |
| Other [Mexican, Puerto Rican, Cuban, Dominican, South American] | 19 (76.0) |
| “Don’t know” | 1 (4.0) |
| Had developmental delay # at 24 months (n = 21) | 13 (61.9) |
| Receive specialized services † | 13 (52.0) |
| Interruptions on specialized services | 6 (46.2) |
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. HCC (pg/mg) | 1 | |||||
| 2. CEFIS Exposure Scale | 0.32 | 1 | ||||
| 3. CEFIS Impact Scale | 0.31 | 0.23 | 1 | |||
| 4. PHQ-8 scores | 0.22 | 0.53 ** | 0.20 | 1 | ||
| 5. IES-R scores | −0.16 | 0.26 | 0.23 | 0.43 * | 1 | |
| 6. BRS scores | 0.04 | −0.31 | −0.18 | −0.56 ** | −0.43 * | 1 |
| Stressor | Beta | SE | p-Value |
|---|---|---|---|
| IES-R continuous score | −0.02 | 0.02 | 0.29 |
| IES-R classification—possible trauma | −1.11 | 0.51 | 0.04 |
| Food insecurity | 1.01 | 0.48 | 0.049 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Rabassa, M.; Torres-Marrero, E.; López, P.; Muniz-Rodriguez, K.; Borges-Rodríguez, M.; Appleton, A.A.; Avilés-Santa, L.; Alvarado-Domenech, L.I. Stressors and Impact of the COVID-19 Pandemic on Vulnerable Hispanic Caregivers and Children. Int. J. Environ. Res. Public Health 2023, 20, 1838. https://doi.org/10.3390/ijerph20031838
Rodríguez-Rabassa M, Torres-Marrero E, López P, Muniz-Rodriguez K, Borges-Rodríguez M, Appleton AA, Avilés-Santa L, Alvarado-Domenech LI. Stressors and Impact of the COVID-19 Pandemic on Vulnerable Hispanic Caregivers and Children. International Journal of Environmental Research and Public Health. 2023; 20(3):1838. https://doi.org/10.3390/ijerph20031838
Chicago/Turabian StyleRodríguez-Rabassa, Mary, Estefanía Torres-Marrero, Pablo López, Kamalich Muniz-Rodriguez, Marilyn Borges-Rodríguez, Allison A. Appleton, Larissa Avilés-Santa, and Luisa I. Alvarado-Domenech. 2023. "Stressors and Impact of the COVID-19 Pandemic on Vulnerable Hispanic Caregivers and Children" International Journal of Environmental Research and Public Health 20, no. 3: 1838. https://doi.org/10.3390/ijerph20031838