
Prevalence and Associated Factors of Post-COVID-19 Syndrome in a Brazilian Cohort after 3 and 6 Months of Hospital Discharge
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Size
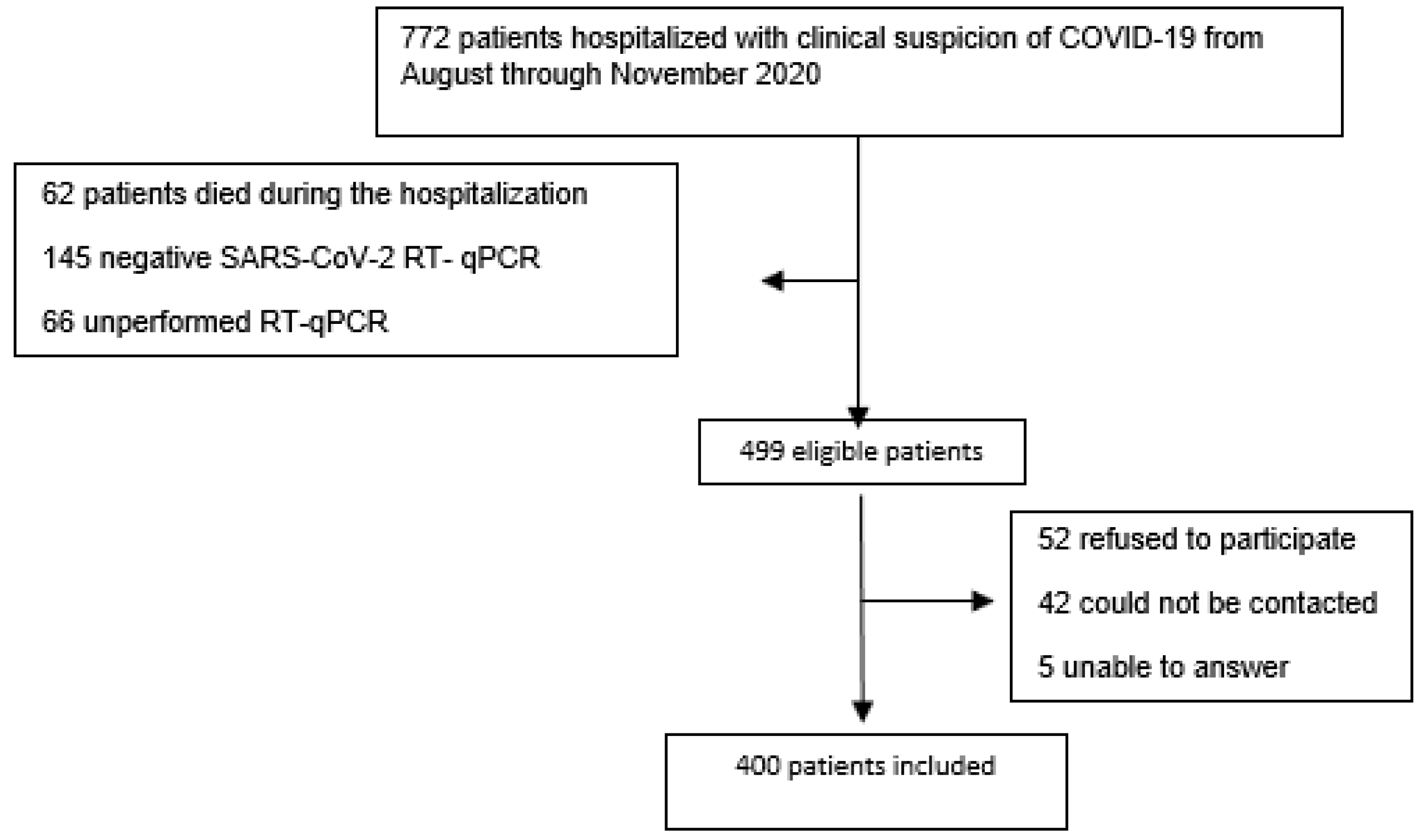
2.3. Participant Eligibility
2.4. Outcomes
2.5. Independent Variables
2.6. Follow-Up Interview after 3 and 6 Months
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pneumonia of Unknown Cause—China. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON229 (accessed on 1 September 2022).
- Coronavírus: Brasil Confirma Primeiro Caso Da Doença—Notícia—UNA-SUS. Available online: https://www.unasus.gov.br/noticia/coronavirus-brasil-confirma-primeiro-caso-da-doenca (accessed on 7 December 2022).
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 16 March 2021).
- National Institute for Health and Care Excellence (Great Britain). COVID-19 Rapid Guideline. 2020. Available online: http://www.ncbi.nlm.nih.gov/books/NBK567261/ (accessed on 26 May 2022).
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. E Clin. Med. 2021, 38, 101019. [Google Scholar]
- Xiong, Q.; Xu, M.; Li, J.; Liu, Y.; Zhang, J.; Xu, Y.; Dong, W. Clinical sequelae of COVID-19 survivors in Wuhan, China: A single-centre longitudinal study. Clin. Microbiol. Infect. 2020, 27, 89–95. [Google Scholar] [CrossRef] [PubMed]
- The Writing Committee for the COMEBAC Study Group; Morin, L.; Savale, L.; Pham, T.; Colle, R.; Figueiredo, S.; Harrois, A.; Gasnier, M.; Lecoq, A.-L.; Meyrignac, O.; et al. Four-Month Clinical Status of a Cohort of Patients After Hospitalization for COVID-19. JAMA 2021, 325, 1525. [Google Scholar] [CrossRef]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef]
- Sigfrid, L.; Drake, T.M.; Pauley, E.; Jesudason, E.C.; Olliaro, P.; Lim, W.S.; Gillesen, A.; Berry, C.; Lowe, D.J.; McPeake, J.; et al. Long Covid in adults discharged from UK hospitals after Covid-19: A prospective, multicentre cohort study using the ISARIC WHO Clinical Characterisation Protocol. Lancet Reg. Health Eur. 2021, 8, 100186. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Antonelli, M.; Canas, L.S.; Molteni, E.; et al. Attributes and predictors of long COVID. Nat Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Evans, R.A.; McAuley, H.; Harrison, E.M.; Shikotra, A.; Singapuri, A.; Sereno, M.; Elneima, O.; Docherty, A.B.; I Lone, N.; Leavy, O.C.; et al. Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): A UK multicentre, prospective cohort study. Lancet Respir. Med. 2021, 9, 1275–1287. [Google Scholar] [CrossRef]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Kim, S.S.; Lindsell, C.J.; Rose, E.B.; Shapiro, N.I.; Files, D.C.; Gibbs, K.W.; Erickson, H.L.; Steingrub, J.S.; Smithline, H.A.; et al. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network—United States, March–June 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 993–998. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Townsend, L.; Dowds, J.; O’Brien, K.; Sheill, G.; Dyer, A.H.; O’Kelly, B.; Hynes, J.P.; Mooney, A.; Dunne, J.; Cheallaigh, C.N.; et al. Persistent Poor Health Post-COVID-19 Is Not Associated with Respiratory Complications or Initial Disease Severity. Annals ATS 2021, 18, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- de Miranda, D.A.P.; Gomes, S.V.C.; Filgueiras, P.S.; Corsini, C.A.; Almeida, N.B.F.; Silva, R.A.; Medeiros, M.L.; Vilela, R.V.R.; Fernandes, G.R.; Grenfell, R.F.Q. Long COVID-19 syndrome: A 14-months longitudinal study during the two first epidemic peaks in Southeast Brazil. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Secretaria de Vigilância em Saúde. Guia de Vigilância Epidemiológica—Emergência de Saúde Pública DE Importância Nacional Pela Doença Pelo Coronavírus 2019; Ministério da Saúde: Brasilia, Brazil, 2021; Volume 2, p. 88.
- Fernández-De-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- de Oliveira, J.F.; de Ávila, R.E.; de Oliveira, N.R.; da Cunha Severino Sampaio, N.; Botelho, M.; Gonçalves, F.A.; Neto, C.J.F.; de Almeida Milagres, A.C.; Gomes, T.C.C.; Pereira, T.L.; et al. Persistent symptoms, quality of life, and risk factors in long COVID: A cross-sectional study of hospitalized patients in Brazil. Int. J. Infect. Dis. 2022, 122, 1044–1051. [Google Scholar] [CrossRef]
- Titze-de-Almeida, R.; Thaylise R da, C.; Dias dos Santos Silva, L.; Santos Ferreira, C.; Pena Silva, C. Persistent, new-onset symptoms and mental health complaints in Long COVID in a Brazilian cohort of non-hospitalized patients. Proc. Natl. Acad. Sci. USA 2021, 118, e2024358118. [Google Scholar] [CrossRef]
- Petersen, M.S.; Kristiansen, M.F.; Hanusson, K.D.; Danielsen, M.E.; Steig, B.; Gaini, S.; Strøm, M.; Weihe, P. Long COVID in the Faroe Islands: A Longitudinal Study Among Nonhospitalized Patients. Clin. Infect. Dis. 2020, 73, e4058–e4063. [Google Scholar] [CrossRef]
- Han, Q.; Zheng, B.; Daines, L.; Sheikh, A. Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens 2022, 11, 269. [Google Scholar] [CrossRef]
- Zeng, F.; Dai, C.; Cai, P.; Wang, J.; Xu, L.; Li, J.; Hu, G.; Wang, Z.; Zheng, F.; Wang, L. A comparison study of SARS-CoV-2 IgG antibody between male and female COVID-19 patients: A possible reason underlying different outcome between sex. J. Med Virol. 2020, 92, 2050–2054. [Google Scholar] [CrossRef]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, M.C.; Ramonell, R.P.; Haddad, N.S.; Anam, F.A.; Rudolph, M.E.; Walker, T.A.; Truong, A.D..; Dixit, A.N..; Han, J.E..; Cabrera-Mora, M.; et al. Dysregulated naive B cells and de novo autoreactivity in severe COVID-19. Nature 2022, 611, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.Y.; Mao, T.; Klein, J.; Dai, Y.; Huck, J.D.; Jaycox, J.R.; Liu, F.; Zhou, T.; Israelow, B.; Wong, P.; et al. Diverse functional autoantibodies in patients with COVID-19. Nature 2021, 595, 283–288. [Google Scholar] [CrossRef]
- Prins, J.B.; van der Meer, J.W.; Bleijenberg, G. Chronic fatigue syndrome. Lancet 2006, 367, 346–355. [Google Scholar] [CrossRef]
- Meini, S.; Suardi, L.R.; Busoni, M.; Roberts, A.T.; Fortini, A. Olfactory and gustatory dysfunctions in 100 patients hospitalized for COVID-19: Sex differences and recovery time in real-life. Eur. Arch. Oto-Rhino-Laryngology 2020, 277, 3519–3523. [Google Scholar] [CrossRef] [PubMed]
- Mendes Paranhos, A.C.; Nazareth Dias, Á.R.; Machado da Silva, L.C.; Vieira Hennemann Koury, G.; de Jesus Sousa, E.; Cerasi, A.J.; Souza, G.S.; Quaresma, J.A.S.; Falcão, L.F.M. Sociodemographic Characteristics and Comorbidities of Patients With Long COVID and Persistent Olfactory Dysfunction. JAMA Netw Open 2022, 5, e2230637. [Google Scholar] [CrossRef]
- Loosen, S.H.; Jensen, B.-E.O.; Tanislav, C.; Luedde, T.; Roderburg, C.; Kostev, K. Obesity and lipid metabolism disorders determine the risk for development of long COVID syndrome: A cross-sectional study from 50,402 COVID-19 patients. Infection 2022, 50, 1165–1170. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Torres-Macho, J.; Elvira-Martínez, C.M.; Molina-Trigueros, L.J.; Sebastián-Viana, T.; Hernández-Barrera, V. Obesity is associated with a greater number of long-term post-COVID symptoms and poor sleep quality: A multicentre case-control study. Int. J. Clin. Pract. 2021, 75. Available online: https://onlinelibrary.wiley.com/doi/10.1111/ijcp.14917 (accessed on 8 December 2022). [CrossRef]
- O’Rourke, R.W.; Lumeng, C.N. Pathways to Severe COVID-19 for People with Obesity. Obesity 2020, 29, 645–653. [Google Scholar] [CrossRef]
- Bell, M.L.; Catalfamo, C.J.; Farland, L.V.; Ernst, K.C.; Jacobs, E.T.; Klimentidis, Y.C.; Jehn, M.; Pogreba-Brown, K. Post-acute sequelae of COVID-19 in a non-hospitalized cohort: Results from the Arizona CoVHORT. PLoS ONE 2021, 16, e0254347. [Google Scholar] [CrossRef]
- Goërtz, Y.M.J.; Van Herck, M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.C.; Houben-Wilke, S.; Burtin, C.; Posthuma, R.; Franssen, F.M.E.; et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: The post-COVID-19 syndrome? ERJ Open Res. 2020, 6, 00542–02020. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde, Secretaria de Ciência, Tecnologia, Inovação e Insumos Estratégicos em Saúde. Informe Semanal n° 01 de Evidências sobre Variantes de Atenção de SARS-CoV-2; Ministério da Saúde: Brasília, Brazil, 2021.



{kind=link}
{kind=link}
| Variables | n = 400 | (%) |
|---|---|---|
| Male b | 207 | 51.8 |
| Age b | 57 a | 46–67 a |
| Race c,d | ||
| Non-white | 255 | 63.8 |
| White | 140 | 35 |
| Educational status (years of schooling) c | ||
| <1 year | 22 | 5.5 |
| ≥1 year and <8 years | 109 | 27.3 |
| ≥8 years and <12 years | 64 | 16 |
| ≥12 years | 184 | 46 |
| Individual income e,f (R$) | 1500 | (1000–3000) |
| Comorbidities b | 290 | 72.5 |
| Hypertension b | 196 | 67.8 |
| Diabetes b | 113 | 39.1 |
| Obesity b | 57 | 19.7 |
| Hypercholesterolemia b | 43 | 14.9 |
| Hypothyroidism b | 29 | 10.0 |
| Current or former smoker b | 133 | 33.2 |
| n = 400 | % | |
|---|---|---|
| Symptoms | ||
| Cough | 263 | 66.4 |
| Dyspnea | 253 | 63.9 |
| Fever | 230 | 57.6 |
| Myalgia | 138 | 34.8 |
| Fatigue | 135 | 33.6 |
| Headache | 117 | 29.5 |
| Diarrhea | 88 | 22.2 |
| Anosmia | 80 | 20.2 |
| Chest pain | 68 | 17.2 |
| Ageusia | 66 | 16.7 |
| Nausea | 47 | 11.9 |
| Vomiting | 42 | 10.6 |
| Rhinorrhea | 41 | 10.4 |
| Throat pain | 24 | 6.1 |
| Anorexia/hyperoxia | 23 | 5.7 |
| Sneeze | 2 | 0.5 |
| Median oxygen saturation at admission a | 92 | 90–95 |
| Pulmonary involvement on tomography | ||
| <25% | 65 | 17.2 |
| 25–50% | 211 | 55.8 |
| 50–75% | 93 | 24.6 |
| >75% | 9 | 2.4 |
| Required supplemental oxygen | 344 | 85.5 |
| Invasive mechanical ventilation | 9 | 2.25 |
| Stroke | 3 | 0.9 |
| Length of hospital stay, days a | 8 | 6–13 |
| Prone position | ||
| Not Applied | 270 | 67.3 |
| Awake | 128 | 32 |
| Intubated | 2 | 0.5 |
| WHO COVID-19 scale b | ||
| 4 | 56 | 14.0 |
| 5 | 253 | 63.2 |
| 6, 7, 8, 9 | 91 | 22.8 |
| 3 Months | % | 6 Months a | % | |
|---|---|---|---|---|
| 0 | 77 | 19.3 | 142 | 39.2 |
| 1 | 54 | 13.5 | 82 | 20.5 |
| 2 | 43 | 10.8 | 40 | 10.0 |
| 3 | 39 | 9.8 | 38 | 9.5 |
| 4 | 45 | 11.2 | 27 | 6.8 |
| 5 | 34 | 8.5 | 22 | 5.5 |
| 6 | 31 | 7.7 | 15 | 3.7 |
| 7 | 21 | 5.3 | 12 | 3.0 |
| 8 | 19 | 4.7 | 9 | 2.2 |
| 9 | 9 | 2.3 | 6 | 2.5 |
| 10 | 12 | 3.0 | 3 | 0.8 |
| 11 | 7 | 1.8 | 1 | 0.2 |
| 12 | 6 | 1.5 | 1 | 0.3 |
| 13 | 2 | 0.5 | 2 | 0.5 |
| 14 | 1 | 0.2 | 0 | 0 |
| 15 | 0 | 0 | 0 | 0 |
| 16 | 0 | 0 | 0 | 0 |
| 17 | 0 | 0 | 0 | 0 |
| 3 Months | 6 Months e | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | PCS | PR | PRR a (95% CI) | aPRR a,b,c (95% CI) | n | PCS | PR | PRR a (95% CI) | aPRR a,b,d (95% CI) | |
| Total | 400 | 323 | 0.81 | 362 | 220 | 0.61 | ||||
| Age | ||||||||||
| ≥57 years | 199 | 164 | 0.82 | 1.04 (0.94–1.14) | 0.99 (0.89–1.11) | 180 | 113 | 0.63 | 1.07 (0.90–1.26) | 1.02 (0.86–1.20) |
| <57 years | 201 | 159 | 0.79 | Ref | Ref | 182 | 107 | 0.59 | Ref | Ref |
| Sex | ||||||||||
| Female | 193 | 177 | 0.92 | 1.3 (1.18–1.43) | 1.28 (1.16–1.41) | 171 | 130 | 0.76 | 1.61 (1.36–1.92) | 1.60 (1.34–1.90) |
| Male | 207 | 146 | 0.70 | Ref | Ref | 191 | 90 | 0.47 | Ref | Ref |
| Race (White x non-white) | ||||||||||
| Non-white | 260 | 210 | 0.81 | 1.00 (0.91–1.11) | 0.98 (0.88–1.08) | 240 | 144 | 0.60 | 0.96 (0.81–1.14) | 0.95 (0.80–1.12) |
| White | 140 | 113 | 0.81 | Ref | Ref | 122 | 76 | 0.62 | Ref | Ref |
| Educational status (years of schooling) | ||||||||||
| ≥12 years | 204 | 166 | 0.80 | 1.02 (0.92–1.12) | 1.11 (1.00–1.24) | 186 | 113 | 0.61 | 1.00 (0.85–1.18) | 1.06 (0.89–1.26) |
| <12 years | 196 | 157 | 0.81 | Ref | Ref | 176 | 107 | 0.61 | Ref | Ref |
| Individual income | ||||||||||
| ≤R$ 1500 | 183 | 157 | 0.86 | 1.12 (1.02–1.23) | 1.00 (0.99–1.00) | 166 | 109 | 0.65 | 1.16 (0.98–1.37) | 1.09 (0.92–1.29) |
| >R$ 1500 | 217 | 166 | 0.76 | Ref | Ref | 196 | 111 | 0.57 | Ref | Ref |
| Comorbidities | ||||||||||
| Yes | 290 | 241 | 0.83 | 1.11 (0.99–1.26) | 261 | 164 | 0.63 | 1.13 (0.93–1.38) | ||
| No | 110 | 82 | 0.74 | Ref | 101 | 56 | 0.55 | Ref | ||
| Hypertension | ||||||||||
| Yes | 196 | 161 | 0.83 | 1.05 (0.95–1.15) | 175 | 113 | 0.65 | 1.13 (0.96–1.33) | ||
| No | 204 | 162 | 0.79 | Ref | 187 | 107 | 0.57 | Ref | ||
| Diabetes | ||||||||||
| Yes | 113 | 100 | 0.88 | 1.14 (1.04–1.24) | 1.09 (1.00–1.19) | 98 | 69 | 0.70 | 1.23 (1.04–1.45) | 1.15 (0.97–1.36) |
| No | 287 | 223 | 0.78 | Ref | Ref | 264 | 151 | 0.57 | Ref | Ref |
| Obesity | ||||||||||
| Yes | 57 | 50 | 0.88 | 1.10 (0.99–1.23) | 54 | 40 | 0.74 | 1.27 (1.05–1.52) | 1.22 (1.03–1.45) | |
| No | 343 | 273 | 0.80 | Ref | 308 | 180 | 0.58 | Ref | Ref | |
| Hypercholesterolemia | ||||||||||
| Yes | 43 | 40 | 0.93 | 1.17 (1.06–1.29) | 1.15 (1.04–1.27) | 38 | 26 | 0.68 | 1.14 (0.90–1.44) | |
| No | 357 | 283 | 0.79 | Ref | Ref | 324 | 194 | 0.60 | Ref | |
| Hypothyroidism | ||||||||||
| Yes | 30 | 28 | 0.93 | 1.17 (1.05–1.30) | 27 | 20 | 0.74 | 1.24 (0.97–1.58) | ||
| No | 370 | 295 | 0.80 | Ref | 335 | 200 | 0.60 | Ref | ||
| Supplemental oxygen | ||||||||||
| Yes | 344 | 279 | 0.81 | 1.02 (0.87–1.18) | 310 | 186 | 0.60 | 0.92 (0.73–1.14) | 0.86 (0.70–1.06) | |
| No | 56 | 44 | 0.79 | Ref | 52 | 34 | 0.65 | Ref | Ref | |
| Length of hospital stay | ||||||||||
| >8 days | 198 | 168 | 0.85 | 1.10 (1.00–1.21) | 1.08 (0.98–1.20) | 176 | 112 | 0.64 | 1.10 (0.93–1.29) | |
| ≤8 days | 202 | 155 | 0.77 | Ref | Ref | 186 | 108 | 0.58 | Ref | |
| Pronation | ||||||||||
| Yes | 130 | 105 | 0.81 | 1.00 (0.90–1.11) | 118 | 77 | 0.65 | 1.12 (0.94–1.32) | 1.15 (1.06–1.25) | |
| No | 270 | 217 | 0.81 | 244 | 142 | 0.58 | Ref | Ref | ||
| Severity | ||||||||||
| Mild | 56 | 44 | 0.79 | Ref | 52 | 34 | 0.65 | Ref | ||
| Moderate | 253 | 203 | 0.80 | 1.04 (0.89–1.20) | 230 | 134 | 0.58 | 0.89 (0.71–1.12) | ||
| Severe | 91 | 75 | 0.83 | 1.08 (0.91–1.27) | 80 | 52 | 0.65 | 0.99 (0.77–1.28) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lapa, J.; Rosa, D.; Mendes, J.P.L.; Deusdará, R.; Romero, G.A.S. Prevalence and Associated Factors of Post-COVID-19 Syndrome in a Brazilian Cohort after 3 and 6 Months of Hospital Discharge. Int. J. Environ. Res. Public Health 2023, 20, 848. https://doi.org/10.3390/ijerph20010848
Lapa J, Rosa D, Mendes JPL, Deusdará R, Romero GAS. Prevalence and Associated Factors of Post-COVID-19 Syndrome in a Brazilian Cohort after 3 and 6 Months of Hospital Discharge. International Journal of Environmental Research and Public Health. 2023; 20(1):848. https://doi.org/10.3390/ijerph20010848
Chicago/Turabian StyleLapa, Juliana, Davi Rosa, João Pedro Lima Mendes, Rodolfo Deusdará, and Gustavo Adolfo Sierra Romero. 2023. "Prevalence and Associated Factors of Post-COVID-19 Syndrome in a Brazilian Cohort after 3 and 6 Months of Hospital Discharge" International Journal of Environmental Research and Public Health 20, no. 1: 848. https://doi.org/10.3390/ijerph20010848