
The Presence of Ankylosing Spondylitis and the Incidence of Subsequent External Eye Diseases: A Population-Based Cohort Study
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database Details
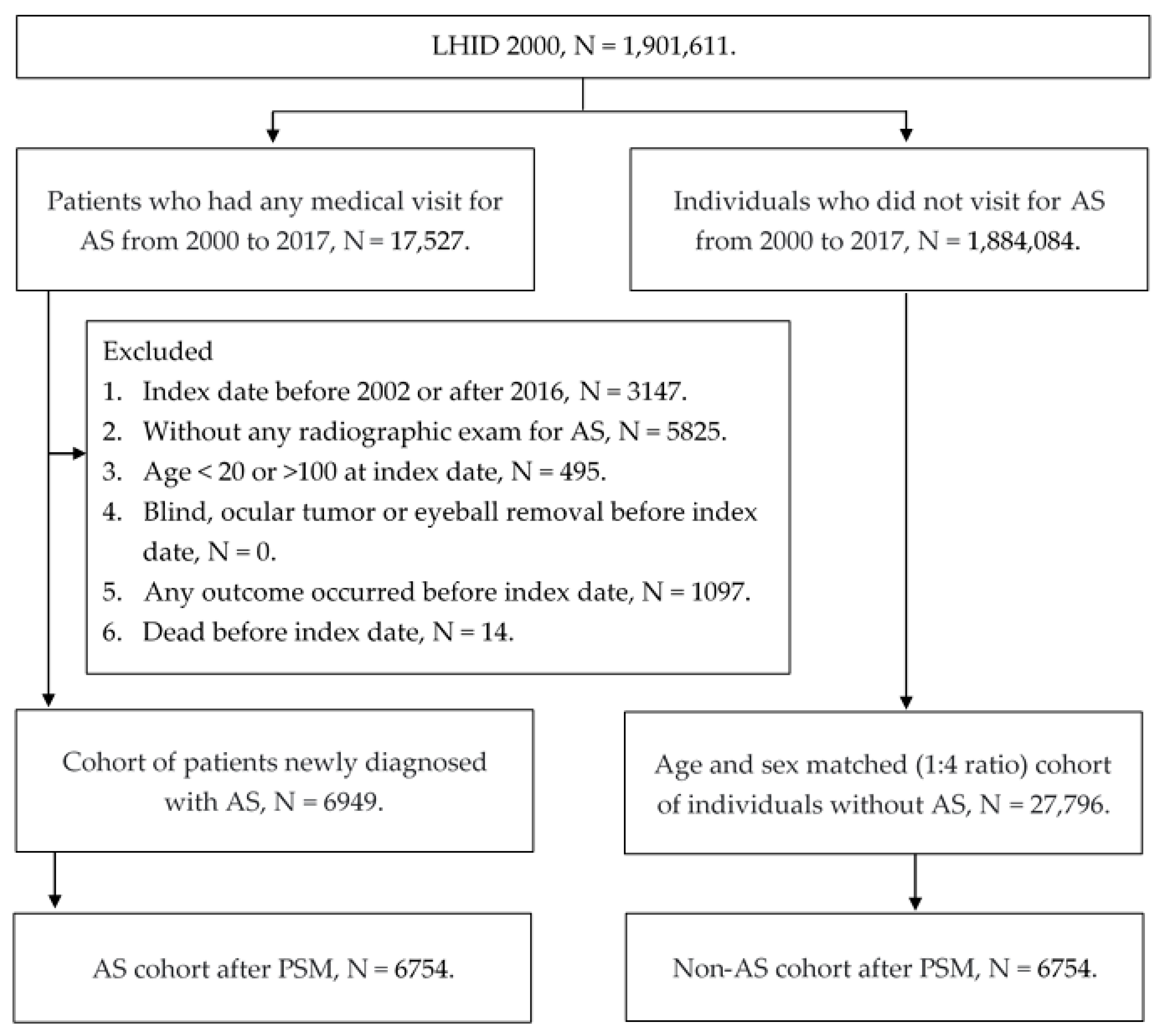
2.2. Participant Selection
2.3. Main Outcome Definition
2.4. Demographic Variables and Comorbidities
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mauro, D.; Thomas, R.; Guggino, G.; Lories, R.; Brown, M.A.; Ciccia, F. Ankylosing spondylitis: An autoimmune or autoinflammatory disease? Nat. Rev. Rheumatol. 2021, 17, 387–404. [Google Scholar] [CrossRef] [PubMed]
- Taurog, J.D.; Chhabra, A.; Colbert, R.A. Ankylosing Spondylitis and Axial Spondyloarthritis. N. Engl. J. Med. 2016, 374, 2563–2574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.A. Update on ankylosing spondylitis: Current concepts in pathogenesis. Curr. Allergy Asthma Rep. 2015, 15, 489. [Google Scholar] [CrossRef]
- Golder, V.; Schachna, L. Ankylosing spondylitis: An update. Aust. Fam. Physician 2013, 42, 780–784. [Google Scholar]
- Hanson, A.; Brown, M.A. Genetics and the Causes of Ankylosing Spondylitis. Rheum. Dis. Clin. N. Am. 2017, 43, 401–414. [Google Scholar] [CrossRef] [PubMed]
- Sieper, J.; Poddubnyy, D. Axial spondyloarthritis. Lancet 2017, 390, 73–84. [Google Scholar] [CrossRef]
- Kemeny-Beke, A.; Szodoray, P. Ocular manifestations of rheumatic diseases. Int. Ophthalmol. 2020, 40, 503–510. [Google Scholar] [CrossRef] [Green Version]
- Gouveia, E.B.; Elmann, D.; Morales, M.S. Ankylosing spondylitis and uveitis: Overview. Rev. Bras. De Reumatol. 2012, 52, 742–756. [Google Scholar]
- Bisht, A.; Shrestha, S.; Bajgai, P.; Khadka, M.; Koirala, P.; Bhattarai, K. Uveitis in Patients with Ankylosing Spondylitis. J. Nepal Health Res. Counc. 2021, 19, 97–100. [Google Scholar] [CrossRef]
- Ebrahimiadib, N.; Berijani, S.; Ghahari, M.; Pahlaviani, F.G. Ankylosing Spondylitis. J. Ophthalmic Vis. Res. 2021, 16, 462–469. [Google Scholar] [CrossRef]
- Rodriguez, A.; Akova, Y.A.; Pedroza-Seres, M.; Foster, C.S. Posterior segment ocular manifestations in patients with HLA-B27-associated uveitis. Ophthalmology 1994, 101, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- van Bentum, R.E.; Baniaamam, M.; Kinaci-Tas, B.; van de Kreeke, J.A.; Kocyigit, M.; Tomassen, J.; den Braber, A.; Visser, P.J.; Ter Wee, M.M.; Serné, E.H.; et al. Microvascular changes of the retina in ankylosing spondylitis, and the association with cardiovascular disease—The eye for a heart study. Semin. Arthritis Rheum. 2020, 50, 1535–1541. [Google Scholar] [CrossRef] [PubMed]
- Cabuk, K.S.; Üstün, E.I.; Atalay, K.; Kirgiz, A.; Aydin, R. Corneal biomechanical features in patients with ankylosing spondylitis. Arq. Bras. De Oftalmol. 2017, 80, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.I.; Rauz, S. The eye and inflammatory rheumatic diseases: The eye and rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis. Best Pract. Res. Clin. Rheumatol. 2016, 30, 802–825. [Google Scholar] [CrossRef] [PubMed]
- Perez, V.L.; Stern, M.E.; Pflugfelder, S.C. Inflammatory basis for dry eye disease flares. Exp. Eye Res. 2020, 201, 108294. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S. Keratitis. Biosci. Rep. 2001, 21, 419–444. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Montoya, L.; Gul, H.; Emery, P. Recent advances in ankylosing spondylitis: Understanding the disease and management. F1000Research 2018, 7. [Google Scholar] [CrossRef] [Green Version]
- Hwang, M.C.; Ridley, L.; Reveille, J.D. Ankylosing spondylitis risk factors: A systematic literature review. Clin. Rheumatol. 2021, 40, 3079–3093. [Google Scholar] [CrossRef]
- Ranganathan, V.; Gracey, E.; Brown, M.A.; Inman, R.D.; Haroon, N. Pathogenesis of ankylosing spondylitis—Recent advances and future directions. Nat. Rev. Rheumatol. 2017, 13, 359–367. [Google Scholar] [CrossRef]
- Fiorillo, M.T.; Haroon, N.; Ciccia, F.; Breban, M. Editorial: Ankylosing Spondylitis and Related Immune-Mediated Disorders. Front. Immunol. 2019, 10, 1232. [Google Scholar] [CrossRef]
- Thulasi, P.; Djalilian, A.R. Update in Current Diagnostics and Therapeutics of Dry Eye Disease. Ophthalmology 2017, 124, S27–S33. [Google Scholar] [CrossRef]
- O’Neil, E.C.; Henderson, M.; Massaro-Giordano, M.; Bunya, V.Y. Advances in dry eye disease treatment. Curr. Opin. Ophthalmol. 2019, 30, 166–178. [Google Scholar] [CrossRef]
- Buckley, R.J. Assessment and management of dry eye disease. Eye 2018, 32, 200–203. [Google Scholar] [CrossRef] [Green Version]
- Roussel, T.; Grutzmacher, R.; Coster, D. Patterns of superficial keratopathy. Aust. J. Ophthalmol. 1984, 12, 301–316. [Google Scholar] [CrossRef]
- Farahani, M.; Patel, R.; Dwarakanathan, S. Infectious corneal ulcers. Disease-a-Month 2017, 63, 33–37. [Google Scholar] [CrossRef]
- Austin, A.; Lietman, T.; Rose-Nussbaumer, J. Update on the Management of Infectious Keratitis. Ophthalmology 2017, 124, 1678–1689. [Google Scholar] [CrossRef]
- Wang, F.; Yang, C.; Ye, J. Severe Hypopyon Uveitis in the Right Eye of Ankylosing Spondylitis. J. Rheumatol. 2021, 48, 147–148. [Google Scholar] [CrossRef]
- Bond, D. Ankylosing spondylitis: Diagnosis and management. Nurs. Stand. 2013, 28, 52–59. [Google Scholar] [CrossRef]
- Hogan, M.J.; Crawford, J.W. Epidemic Keratoconjunctivitis: (Superficial Punctate Keratitis, Keratitis Subepithelialis, Keratitis Maculosa, Keratitis Nummularis) with a Review of the Literature and a Report of 125 Cases. Am. J. Ophthalmol. 2018, 190, 1059–1078. [Google Scholar] [CrossRef]
- Wang, R.; Ward, M.M. Epidemiology of axial spondyloarthritis: An update. Curr. Opin. Rheumatol. 2018, 30, 137–143. [Google Scholar] [CrossRef]
- Tiskaoglu, N.S.; Yazıcı, A.; Karlıdere, T.; Sari, E.; Oguz, E.Y.; Musaoglu, M.; Aslan, S.; Samet Ermiş, S. Dry Eye Disease in Patients with Newly Diagnosed Depressive Disorder. Curr. Eye Res. 2017, 42, 672–676. [Google Scholar] [CrossRef]
- Gau, S.Y.; Lee, Y.H.; Tsou, H.K.; Huang, J.Y.; Chen, X.; Ye, Z.; Wei, J.C. Patients With Ankylosing Spondylitis Are Associated With High Risk of Fibromyalgia: A Nationwide Population-Based Cohort Study. Front. Med. 2021, 8, 618594. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Non-AS Group N = 6754 | AS Group N = 6754 | ASD |
|---|---|---|---|
| Year of index | 0.0000 | ||
| 2002–2006 | 2992 (44.30%) | 2966 (43.91%) | |
| 2007–2011 | 1959 (29.01%) | 1989 (29.45%) | |
| 2012–2017 | 1803 (26.70%) | 1799 (26.64%) | |
| Sex | 0.0000 | ||
| Male | 4427 (65.55%) | 4427 (65.55%) | |
| Female | 2327 (34.45%) | 2327 (34.45%) | |
| Age at index | 0.0000 | ||
| 20–30 | 1786 (26.44%) | 1748 (25.88%) | |
| 30–39 | 1551 (22.96%) | 1545 (22.88%) | |
| 40–49 | 1377 (20.39%) | 1359 (20.12%) | |
| 50–59 | 1074 (15.90%) | 1082 (16.02%) | |
| 60–69 | 547 (8.10%) | 561 (8.31%) | |
| 70–100 | 419 (6.20%) | 459 (6.80%) | |
| Urbanization | 0.0219 | ||
| Urban | 4000 (59.22%) | 3948 (58.45%) | |
| Sub-urban | 2186 (32.37%) | 2216 (32.81%) | |
| Rural | 568 (8.41%) | 590 (8.74%) | |
| Education | 0.0000 | ||
| Elementary school or below | 1763 (26.10%) | 1759 (26.04%) | |
| Junior high school | 1152 (17.06%) | 1181 (17.49%) | |
| Senior high school | 2982 (44.15%) | 2953 (43.72%) | |
| University or above | 857 (12.69%) | 861 (12.75%) | |
| Co-morbidities | |||
| Hypertension | 978 (14.48%) | 1019 (15.09%) | 0.0171 |
| DM | 338 (5.00%) | 398 (5.89%) | 0.0391 |
| ESRD | 39 (0.58%) | 41 (0.61%) | 0.0039 |
| Ischemic heart diseases | 161 (2.38%) | 211 (3.12%) | 0.0452 |
| Cerebrovascular disease | 65 (0.96%) | 87 (1.29%) | 0.0309 |
| Rheumatoid arthritis | 14 (0.21%) | 10 (0.15%) | 0.0141 |
| Systemic lupus erythematous | 49 (0.18%) | 10 (0.14%) | 0.0024 |
| Other inflammatory diseases | 60 (0.89%) | 60 (0.89%) | 0.0000 |
| Event | Non-AS N = 6754 | AS N = 6754 | p Value |
|---|---|---|---|
| Any outcome | |||
| Follow up person months | 696,943 | 666,896 | |
| New case | 408 | 709 | |
| Incidence rate † (95% CI) | 0.59 (0.53–0.65) | 1.06 (0.99–1.14) | |
| Crude Relative risk (95% CI) | Reference | 1.802 (1.595–2.035) | |
| AHR (95% CI) | Reference | 1.826 (1.616–2.063) | <0.0001 * |
| Dry eye | |||
| Follow up person months | 710,667 | 685,762 | |
| New case | 267 | 504 | |
| Incidence rate † (95% CI) | 0.38 (0.33–0.42) | 0.73 (0.67–0.80) | |
| Crude Relative risk (95% CI) | Reference | 1.947 (1.678–2.258) | |
| AHR (95% CI) | Reference | 1.973 (1.701–2.290) | <0.0001 * |
| Keratopathy | |||
| Follow up person months | 712,411 | 697,502 | |
| New case | 225 | 351 | |
| Incidence rate † (95% CI) | 0.32 (0.28–0.36) | 0.50 (0.45–0.56) | |
| Crude Relative risk (95% CI) | Reference | 1.586 (1.341–1.875) | |
| AHR (95% CI) | Reference | 1.593 (1.347–1.883) | <0.0001 * |
| Corneal ulcer | |||
| Follow up person months | 729,389 | 726,261 | |
| New case | 42 | 34 | |
| Incidence rate † (95% CI) | 0.06 (0.04–0.08) | 0.05 (0.03–0.07) | |
| Crude Relative risk (95% CI) | Reference | 0.813 (0.517–1.278) | |
| AHR (95% CI) | Reference | 0.805 (0.512–1.266) | 0.4598 |
| Parameters (AHR ± 95% CI) | Any Event | DED | Keratopathy | Corneal Ulcer |
|---|---|---|---|---|
| Age | ||||
| 20–30 | 1.340 (1.045–1.719) | 1.618 (1.122–2.333) | 1.262 (0.929–1.715) | 0.571 (0.248–1.314) |
| 30–39 | 1.857 (1.492–2.312) | 2.064 (1.561–2.728) | 1.555 (1.157–2.090) | 0.784 (0.327–1.881) |
| 40–49 | 1.900 (1.566–2.305) | 2.051 (1.636–2.571) | 1.647 (1.247–2.175) | 0.681 (0.264–1.757) |
| 50–59 | 2.053 (1.725–2.443) | 2.204 (1.811–2.681) | 1.844 (1.428–2.382) | 0.809 (0.323–2.024) |
| 60–69 | 1.632 (1.308–2.038) | 1.458 (1.117–1.904) | 1.464 (1.064–2.015) | 1.746 (0.756–4.030) |
| 70–100 | 1.068 (0.779–1.464) | 1.387 (0.961–2.001) | 0.836 (0.536–1.306) | 1.204 (0.348–4.163) |
| p for interaction | 0.0030 | 0.0386 | 0.0997 | 0.4130 |
| Sex | ||||
| Male | 1.737 (1.530–1.972) | 1.956 (1.667–2.294) | 1.466 (1.232–1.744) | 0.975 (0.617–1.540) |
| Female | 1.711 (1.515–1.933) | 1.812 (1.572–2.089) | 1.519 (1.277–1.809) | 0.702 (0.379–1.301) |
| p for interaction | 0.9468 | 0.6222 | 0.8149 | 0.3192 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-Y.; Chen, H.-C.; Huang, J.-Y.; Yen, C.-H.; Hwang, Y.-S.; Chang, C.-K.; Yang, S.-F. The Presence of Ankylosing Spondylitis and the Incidence of Subsequent External Eye Diseases: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 16296. https://doi.org/10.3390/ijerph192316296
Lee C-Y, Chen H-C, Huang J-Y, Yen C-H, Hwang Y-S, Chang C-K, Yang S-F. The Presence of Ankylosing Spondylitis and the Incidence of Subsequent External Eye Diseases: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(23):16296. https://doi.org/10.3390/ijerph192316296
Chicago/Turabian StyleLee, Chia-Yi, Hung-Chi Chen, Jing-Yang Huang, Chieh-Hung Yen, Yih-Shiou Hwang, Chao-Kai Chang, and Shun-Fa Yang. 2022. "The Presence of Ankylosing Spondylitis and the Incidence of Subsequent External Eye Diseases: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 19, no. 23: 16296. https://doi.org/10.3390/ijerph192316296