
Correlation between Component Factors of Non-Alcoholic Fatty Liver Disease and Metabolic Syndrome in Nurses: An Observational and Cross-Sectional Study

Abstract
:1. Introduction

2. Materials and Methods
2.1. Participants and Sampling
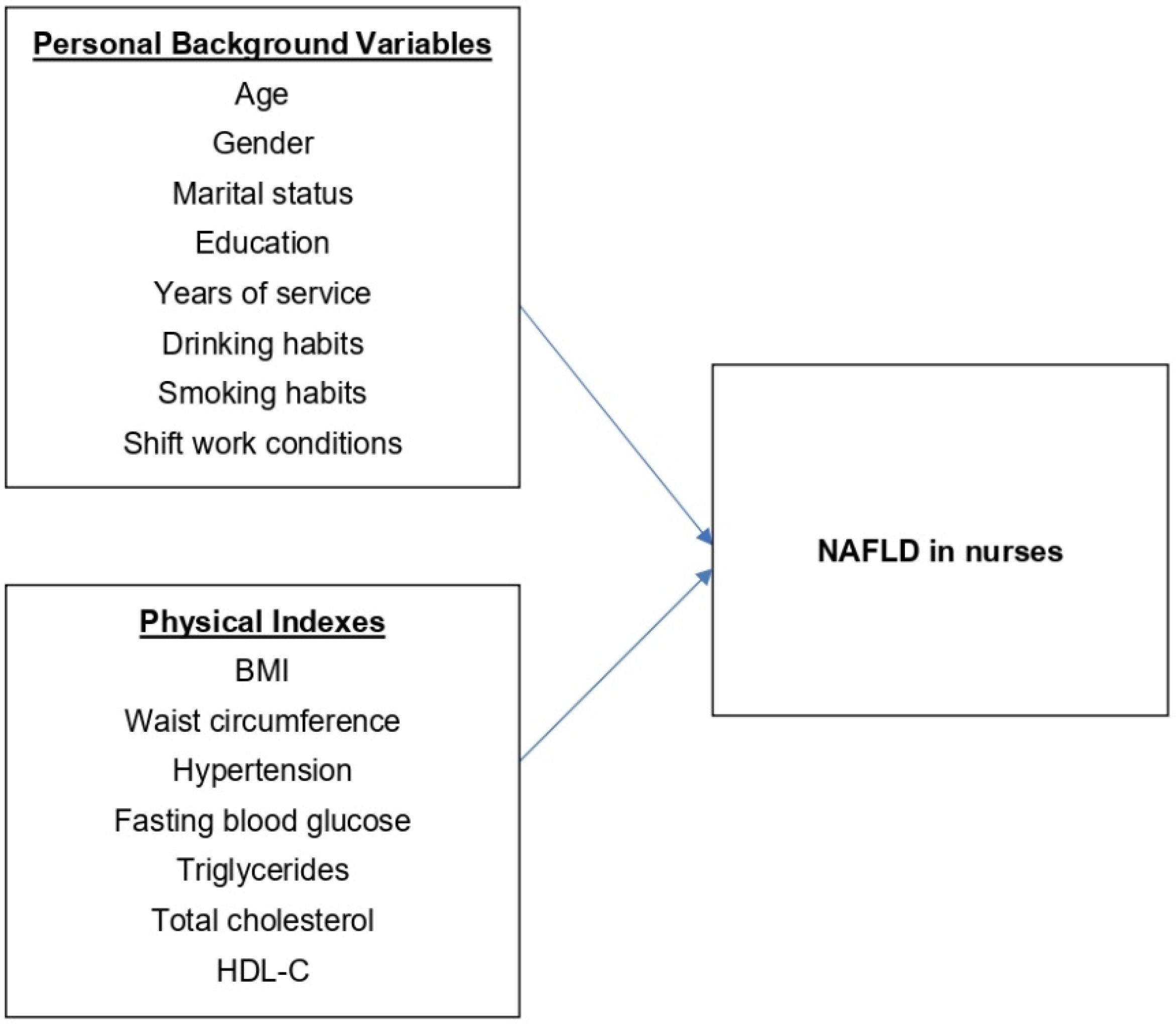
2.2. Design
2.3. Statistical Methods
3. Results
3.1. Prevalence of NAFLD among Nurses and Basic Information Analysis
3.2. Primary Influencing Factors of NAFLD in Nurses
3.3. Comparison of Primary Factors Influencing the Severity of NAFLD in Nurses
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ross, A.; Bevans, M.; Brooks, A.T.; Gibbons, S.; Wallen, G.R. Nurses and health-promoting behaviors: Knowledge may not translate into self-care. AORN J. 2017, 105, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, H.; Dan, H.; Pang, Y.; Kim, B.; Jeong, H.; Lee, J.E.; Kim, O. Association between dietary habits, shift work, and the metabolic syndrome: The Korea nurses’ health study. Int. J. Environ. Res. Public Health 2020, 17, 7697. [Google Scholar] [CrossRef] [PubMed]
- Idalsoaga, F.; Kulkarni, A.V.; Mousa, O.Y.; Arrese, M.; Arab, J.P. Non-alcoholic fatty liver disease and alcohol-related liver disease: Two intertwined entities. Front. Med. 2020, 7, 448. [Google Scholar] [CrossRef] [PubMed]
- Araújo, A.R.; Rosso, N.; Bedogni, G.; Tiribelli, C.; Bellentani, S. Global epidemiology of non-alcoholic fatty liver disease/non-alcoholic steatohepatitis: What we need in the future. Liver Int. 2018, 38, 47–51. [Google Scholar] [CrossRef] [Green Version]
- Chalasani, N.; Youmossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 142, 1592–1609. [Google Scholar]
- Abd El-Kader, S.M.; El-Den Ashmawy, E.M. Non-alcoholic fatty liver disease: The diagnosis and management. World J. Hepatol. 2015, 7, 846–858. [Google Scholar] [CrossRef]
- Flisiak-Jackiewicz, M.; Bobrus-Chociej, A.; Wasilewska, N.; Lebensztejn, D.M. From nonalcoholic fatty liver disease (NAFLD) to metabolic dysfunction-associated fatty liver disease (MAFLD)-New terminology in pediatric patients as a step in good scientific direction? J. Clin. Med. 2021, 10, 924. [Google Scholar] [CrossRef]
- Paudel, M.S.; Tiwari, A.; Mandal, A.; Shrestha, B.; Kafle, P.; Chaulagai, B.; Kc, S. Metabolic syndrome in patients with non-alcoholic fatty liver disease: A community based cross-sectional study. Cureus 2019, 11, e4099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, E.J. Nonalcoholic fatty liver disease and diabetes: An epidemiological perspective. Endocrinol. Metab. 2019, 34, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Caruso, C.C.; Baldwin, C.M.; Berger, A.; Chasens, E.R.; Edmonson, J.C.; Gobel, B.H.; Landis, C.A.; Patrician, P.A.; Redeker, N.S.; Scott, L.D.; et al. Policy brief: Nurse fatigue, sleep, and health, and ensuring patient and public safety. Nurs. Outlook 2019, 67, 615–619. [Google Scholar] [CrossRef] [Green Version]
- Health Promotion Administration; Ministry of Health and Welfare. Health 99 Education Resource. Available online: http://health99.hpa.gov.tw/en (accessed on 19 January 2020).
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Ferraioli, G.; Soares Monteiro, L.B. Ultrasound-based techniques for the diagnosis of liver steatosis. World J. Gastroenterol. 2019, 25, 6053–6062. [Google Scholar] [CrossRef] [PubMed]
- Farrell, G.C.; Wong, V.W.; Chitturi, S. NAFLD in Asia—As common and important as in the West. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; De, A.; Chowdhury, A. Epidemiology of non-alcoholic and alcoholic fatty liver diseases. Transl. Gastroenterol. Hepatol. 2020, 5, 16. [Google Scholar] [CrossRef] [PubMed]
- Schwenger, K.J.; Allard, J.P. Clinical approaches to non-alcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 1712–1723. [Google Scholar] [CrossRef] [PubMed]
- Saran, A.R.; Dave, S.; Zarrinpar, A. Circadian rhythms in the pathogenesis and treatment of fatty liver disease. Gastroenterology 2020, 158, 1948–1966.e1. [Google Scholar] [CrossRef]
- Yasutake, K.; Kohjima, M.; Kotoh, K.; Nakashima, M.; Nakamuta, M.; Enjoji, M. Dietary habits and behaviors associated with nonalcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 1756–1767. [Google Scholar] [CrossRef]
- Alqahtani, S.A.; Schattenberg, J.M. NAFLD in the elderly. Clin. Interv. Aging 2021, 16, 1633–1649. [Google Scholar] [CrossRef]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Lonardo, A. NAFLD as a sexual dimorphic disease: Role of gender and reproductive status in the development and progression of nonalcoholic fatty liver disease and inherent cardiovascular risk. Adv. Ther. 2017, 34, 1291–1326. [Google Scholar] [CrossRef]
- Sayiner, M.; Koenig, A.; Henry, L.; Younossi, Z.M. Epidemiology of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis in the United States and the rest of the world. Clin. Liver Dis. 2016, 20, 205–214. [Google Scholar] [CrossRef]
- Du, S.; Zhang, H.; Wu, H.; Ye, S.; Li, W.; Su, Q. Prevalence and gender differences of metabolic syndrome in young ketosis-prone type 2 diabetic individuals: A retrospective study. Diabetes Metab. Syndr. Obes. 2020, 13, 2719–2727. [Google Scholar] [CrossRef] [PubMed]
- Khan, Y.; Lalchandani, A.; Gupta, A.C.; Khadanga, S.; Kumar, S. Prevalence of metabolic syndrome crossing 40% in Northern India: Time to act fast before it runs out of proportions. J. Family Med. Prim. Care 2018, 7, 118–123. [Google Scholar] [PubMed]
- Lee, J.; Cho, Y.K.; Kang, Y.M.; Kim, H.S.; Jung, C.H.; Kim, H.K.; Park, J.Y.; Lee, W.J. The impact of NAFLD and waist circumference changes on diabetes development in prediabetes subjects. Sci. Rep. 2019, 9, 17258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuel, V.T.; Shulman, G.I. Nonalcoholic fatty liver disease as a nexus of metabolic and hepatic diseases. Cell Metab. 2018, 27, 22–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarghamravanbakhsh, P.; Frenkel, M.; Poretsky, L. Metabolic causes and consequences of nonalcoholic fatty liver disease (NAFLD). Metab. Open 2021, 12, 100149. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.W.; Chen, Y.S.; Chen, P.J.; Yeh, S.H. Androgen receptor functions in pericentral hepatocytes to decrease gluconeogenesis and avoid hyperglycemia and obesity in male mice. Metabolism 2022, 135, 155269. [Google Scholar] [CrossRef] [PubMed]
- Yeh, W.C.; Chuang, H.H.; Lu, M.C.; Tzeng, I.S.; Chen, J.Y. Prevalence of metabolic syndrome among employees of a Taiwanese hospital varies according to profession. Medicine 2018, 97, e11664. [Google Scholar] [CrossRef]
- Alshammari, G.M.; Balakrishnan, A.; Chinnasamy, T. Butein protects the nonalcoholic fatty liver through mitochondrial reactive oxygen species attenuation in rats. BioFactors 2018, 44, 289–298. [Google Scholar] [CrossRef]
- Yang, J.; Fernández-Galilea, M.; Martínez-Fernández, L.; González-Muniesa, P.; Pérez-Chávez, A.; Martínez, J.A.; Moreno-Aliaga, M.J. Oxidative stress and non-alcoholic fatty liver disease: Effects of omega-3 fatty acid supplementation. Nutrients 2019, 11, 872. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.C.; Chou, S.C.; Huang, P.T.; Chiou, H.Y. Risk factors and predictors of non-alcoholic fatty liver disease in Taiwan. Ann. Hepatol. 2011, 10, 125–132. [Google Scholar] [CrossRef]
- Masarone, M.; Rosato, V.; Dallio, M.; Gravina, A.G.; Aglitti, A.; Loguercio, C.; Federico, A.; Persico, M. Role of oxidative stress in pathophysiology of nonalcoholic fatty liver disease. Oxid. Med. Cell. Longev. 2018, 2018, 9547613. [Google Scholar] [CrossRef] [PubMed]
- Verwer, B.J.; Scheffer, P.G.; Vermue, R.P.; Pouwels, P.J.; Diamant, M.; Tushuizen, M.E. NAFLD is related to post-prandial triglyceride-enrichment of HDL particles in association with endothelial and HDL dysfunction. Liver Int. 2020, 40, 2439–2444. [Google Scholar] [CrossRef] [PubMed]
- Godoy-Matos, A.F.; Silva Júnior, W.S.; Valerio, C.M. NAFLD as a continuum: From obesity to metabolic syndrome and diabetes. Diabetol. Metab. Syndr. 2020, 12, 60. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | All n = 706 | Without NAFLD n = 446 | With NAFLD n = 260 | p |
|---|---|---|---|---|
| No. (%) | No. (%) | No. (%) | ||
| Gender | 0.713 | |||
| Male | 30 (4.2) | 18 (4.0) | 12 (4.6) | |
| Female | 676 (95.8) | 428 (96.0) | 248 (95.4) | |
| Marital status | 0.564 | |||
| Living with spouse or partner | 136 (19.3) | 83 (18.6) | 53 (20.4) | |
| Not living with spouse or partner | 570 (80.7) | 363 (81.4) | 207 (79.6) | |
| Education | 0.910 | |||
| Junior college | 250 (35.4) | 155 (34.8) | 95 (36.6) | |
| University | 420 (59.5) | 272 (61.0) | 148 (56.9) | |
| Graduate school | 36 (5.1) | 19 (4.2) | 17 (6.5) | |
| Drinking | 0.559 | |||
| Yes (including occasionally or only when entertaining) | 286 (40.5) | 177 (39.7) | 109 (41.9) | |
| No | 420 (59.5) | 269 (60.3) | 151 (58.1) | |
| Smoking | 0.503 | |||
| Yes | 32 (4.5) | 22 (4.9) | 10 (3.8) | |
| No | 674 (95.5) | 424 (95.1) | 250 (96.2) | |
| Shift work | 0.037 | |||
| Yes | 531 (75.2) | 347 (77.8) | 184 (70.8) | |
| No | 175 (24.8) | 99 (22.2) | 76 (29.2) | |
| BMI | <0.001 | |||
| Normal | 478 (67.7) | 398 (89.2) | 80 (30.8) | |
| Overweight | 95 (13.5) | 41 (9.2) | 54 (20.8) | |
| Obese | 133 (18.8) | 7 (1.6) | 126 (48.5) | |
| Waist circumference | <0.001 | |||
| Normal | 171 (69.3) | 396 (88.8) | 93 (35.8) | |
| Exceeding standard | 217 (30.7) | 50 (11.2) | 167 (64.2) | |
| Hypertension | 0.031 | |||
| Yes | 16 (2.3) | 6 (1.3) | 10 (3.8) | |
| No | 690 (97.7) | 440 (98.7) | 250 (96.2) | |
| Fasting blood glucose (mg/dL) | <0.001 | |||
| <100 | 669 (94.8) | 438 (98.2) | 231 (88.8) | |
| 100–125 | 26 (3.7) | 6 (1.3) | 20 (7.7) | |
| ≥126 | 11 (1.6) | 2 (0.4) | 9 (3.5) | |
| Triglycerides (mg/dL) | 0.001 | |||
| <150 | 670 (94.9) | 433 (97.1) | 237 (91.2) | |
| ≥150 | 36 (5.1) | 13 (2.9) | 23 (8.8) | |
| Total cholesterol (mg/dL) | 0.131 | |||
| <200 | 507 (71.8) | 329 (73.8) | 178 (68.5) | |
| ≥200 | 199 (28.2) | 117 (26.2) | 82 (31.5) | |
| HDL-C (mg/dL) | <0.001 | |||
| Normal | 597 (84.6) | 411 (92.2) | 186 (71.5) | |
| Overly low | 109 (15.4) | 35 (7.8) | 74 (28.5) | |
| NAFLD | ||||
| No | 446 (63.2) | - | - | |
| Mild | 188 (26.6) | - | - | |
| Moderate/severe | 72 (10.2) | - | - | |
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| Age (years) | 29.39 (7.06) | 28.44 (6.60) | 31.02 (7.53) | <0.001 |
| Years of service (years) | 6.15 (5.52) | 5.49 (5.19) | 7.28 (5.88) | <0.001 |
| Predictors | NAFLD n = 260 (36.8%) | |
|---|---|---|
| OR [95% CI] | p | |
| Age (Years) | 1.07 [1.00, 1.15] | 0.044 |
| Gender (Male vs. Female) | 0.87 [0.31, 2.49] | 0.798 |
| Marital status (Living with vs. Not living with spouse or partner) | 0.71 [0.38, 1.32] | 0.281 |
| Education | ||
| Graduate school vs. Junior college | 0.45 [0.15, 1.39] | 0.166 |
| University vs. Junior college | 0.78 [0.50, 1.23] | 0.283 |
| Years of service | 0.99 [0.90,1.08] | 0.751 |
| Drinking (Yes vs. No) | 1.29 [0.83, 2.00] | 0.262 |
| Smoking (Yes vs. No) | 0.70 [0.26, 1.86] | 0.471 |
| Shift work (Yes vs. No) | 1.21 [0.68, 2.16] | 0.525 |
| BMI | ||
| Obese vs. Normal | 38.29 [14.74, 99.46] | <0.001 |
| Overweight vs. Normal | 4.12 [2.31, 7.32] | <0.001 |
| Waist circumference (Exceeding standard vs. Normal) | 2.27 [1.25, 4.14] | 0.007 |
| Hypertension (Yes vs. No) | 0.35 [0.06, 2.13] | 0.257 |
| Fasting blood glucose (mg/dL) | ||
| >126 vs. <100 | 3.91 [0.51, 30.01] | 0.191 |
| 100–125 vs. <100 | 4.66 [1.42, 15.26] | 0.011 |
| Triglycerides (≥150 vs. <150) (mg/dL) | 0.90 [0.33, 2.47] | 0.832 |
| Total cholesterol (≥200 vs. <200) (mg/dL) | 1.25 [0.78, 2.01] | 0.347 |
| HDL-C (Overly low vs. Normal) | 2.10 [1.11, 3.97] | 0.022 |
| Predictors | NAFLD | |||
|---|---|---|---|---|
| Mild n = 188 (26.6%) | Moderate/Severe n = 72 (10.2%) | |||
| OR [95% CI] | p | OR [95% CI] | p | |
| Age (Years) | 1.08 [1.01, 1.16] | 0.037 | 1.05 [0.94, 1.18] | 0.398 |
| Gender (Male vs. Female) | 0.67 [0.21, 2.19] | 0.510 | 6.42 [1.07, 38.70] | 0.043 |
| Marital status (Living with vs. Not living with spouse or partner) | 0.71 [0.38, 1.32] | 0.278 | 0.61 [0.20, 1.86] | 0.380 |
| Education | ||||
| Graduate school vs. Junior college | 0.40 [0.12, 1.32] | 0.132 | 0.47 [0.08, 2.79] | 0.407 |
| University vs. Junior college | 0.79 [0.50, 1.24] | 0.296 | 0.58 [0.26, 1.30] | 0.186 |
| Years of service | 0.99 [0.90, 1.08] | 0.760 | 1.02 [0.89, 1.17] | 0.782 |
| Drinking (Yes vs. No) | 1.31 [0.84, 2.05] | 0.230 | 0.99 [0.45, 2.18] | 0.977 |
| Smoking (Yes vs. No) | 0.65 [0.24, 1.82] | 0.416 | 1.67 [0.27, 10.34] | 0.579 |
| Shift work (Yes vs. No) | 1.25 [0.70, 2.26] | 0.453 | 0.88 [0.32, 2.41] | 0.798 |
| BMI | ||||
| Obese vs. Normal | 23.30 [8.88, 61.10] | <0.001 | 409.63 [61.59, 2724.38] | <0.001 |
| Overweight vs. Normal | 3.89 [2.15, 7.04] | <0.001 | 13.50 [2.35, 77.50] | 0.004 |
| Waist circumference (Exceeding standard vs. Normal) | 2.10 [1.14, 3.87] | 0.017 | 9.33 [2.30, 37.98] | 0.002 |
| Hypertension (Yes vs. No) | 0.16 [0.02, 1.52] | 0.110 | 0.65 [0.07, 5.82] | 0.697 |
| Fasting blood glucose (mg/dL) | ||||
| >126 vs. <100 | 3.55 [0.43, 29.44] | 0.240 | 2.98 [0.22, 40.11] | 0.411 |
| 100–125 vs. <100 | 4.09 [1.19, 14.03] | 0.025 | 11.74 [2.22, 62.27] | 0.004 |
| Triglycerides (≥150 vs. <150) (mg/dL) | 0.57 [0.18, 1.80] | 0.337 | 5.63 [1.35, 23.49] | 0.018 |
| Total cholesterol (≥200 vs. <200) (mg/dL) | 1.29 [0.80, 2.07] | 0.295 | 0.87 [0.36, 2.14] | 0.767 |
| HDL-C (Overly low vs. Normal) | 2.01 [1.05, 3.85] | 0.036 | 2.60 [1.03, 6.58] | 0.044 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, W.-P.; Chang, Y.-P. Correlation between Component Factors of Non-Alcoholic Fatty Liver Disease and Metabolic Syndrome in Nurses: An Observational and Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 16294. https://doi.org/10.3390/ijerph192316294
Chang W-P, Chang Y-P. Correlation between Component Factors of Non-Alcoholic Fatty Liver Disease and Metabolic Syndrome in Nurses: An Observational and Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(23):16294. https://doi.org/10.3390/ijerph192316294
Chicago/Turabian StyleChang, Wen-Pei, and Yu-Pei Chang. 2022. "Correlation between Component Factors of Non-Alcoholic Fatty Liver Disease and Metabolic Syndrome in Nurses: An Observational and Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 23: 16294. https://doi.org/10.3390/ijerph192316294