
Relationship between Oxygen Uptake Reserve and Heart Rate Reserve in Young Male Tennis Players: Implications for Physical Fitness Monitoring

Abstract
:1. Introduction
2. Materials and Methods
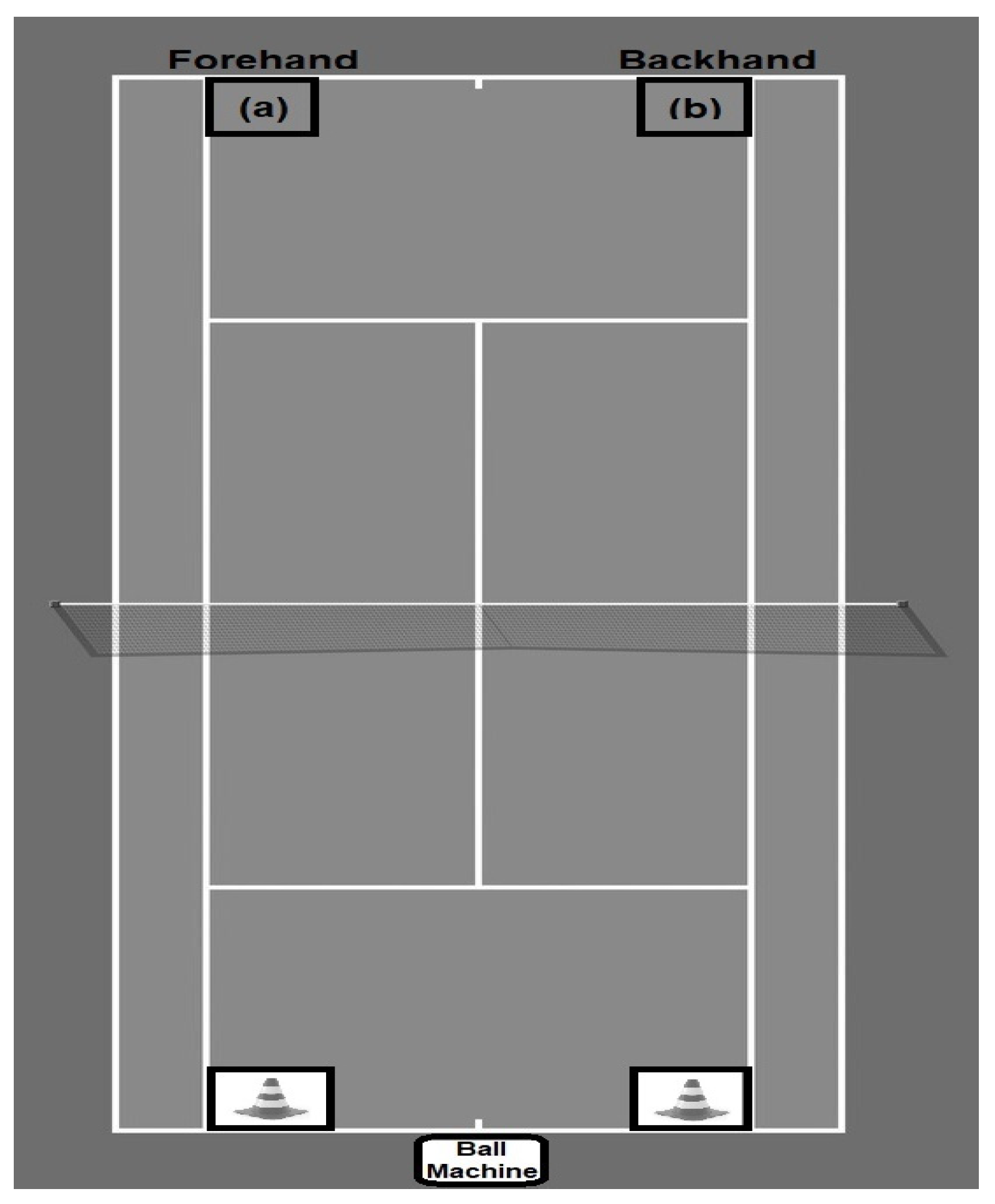
2.1. Experimental Protocol
2.2. Data Collection
2.3. Statistical Analysis
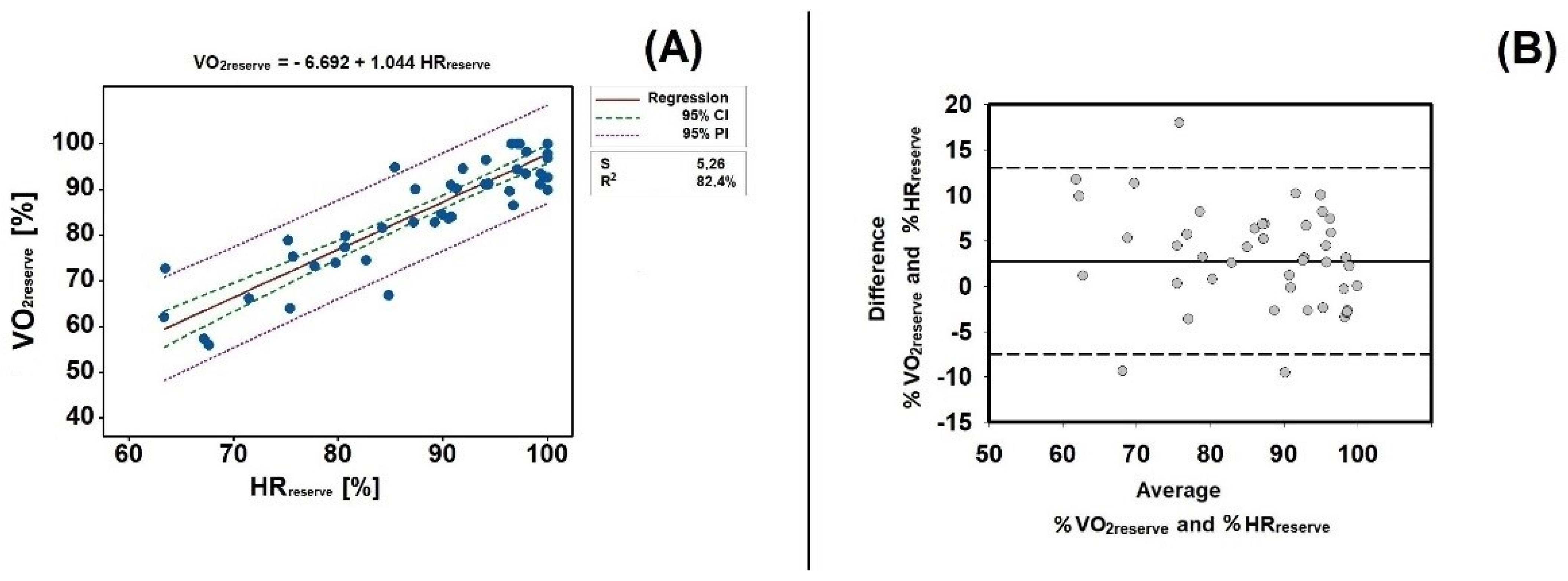
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schoeller, D.A.; Racette, S. A Review of Field Techniques for the Assessment of Energy Expenditure. J. Nutr. 1990, 120, 1492–1495. [Google Scholar] [CrossRef] [PubMed]
- MacInnis, M.J.; Gibala, M.J. Physiological adaptations to interval training and the role of exercise intensity. J. Physiol. 2017, 595, 2915–2930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achten, J.; Jeukendrup, A.E. Heart Rate Monitoring. Sport. Med. 2003, 33, 517–538. [Google Scholar] [CrossRef]
- Schneider, C.; Hanakam, F.; Wiewelhove, S.S.T.; Döweling, A.; Kellmann, M.; Meyer, T.; Pfeiffer, M.; Ferrauti, A. Heart Rate Monitoring in Team Sports—A Conceptual Framework for Contextualizing Heart Rate Measures for Training and Recovery Prescription. Front. Physiol. 2018, 9, 639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaminsky, L. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription; CQUniversity: Sydney, Australia, 2006; ISBN 0-7817-4591-8. [Google Scholar]
- Bell, P.G.; Furber, M.J.W.; Van Someren, K.A.; Antón-Solanas, A.; Swart, J. The Physiological Profile of a Multiple Tour de France Winning Cyclist. Med. Sci. Sports Exerc. 2017, 49, 115–123. [Google Scholar] [CrossRef]
- Baiget, E.; Iglesias, X.; Fuentes, J.P.; Rodríguez, F.A. New Approaches for On-court Endurance Testing and Conditioning in Competitive Tennis Players. Strength Cond. J. 2019, 41, 9–16. [Google Scholar] [CrossRef]
- Bartolomeu, R.F.; Barbosa, T.M.; Morais, J.E.; Lopes, V.P.; Bragada, J.A.; Costa, M.J. The aging influence on cardiorespiratory, metabolic, and energy expenditure adaptations in head-out aquatic exercises: Differences between young and elderly women. Women Health 2016, 57, 377–391. [Google Scholar] [CrossRef]
- Andrade, L.S.; Botton, C.E.; David, G.B.; Pinto, S.S.; Häfele, M.S.; Alberton, C.L. Cardiorespiratory Parameters Comparison Between Incremental Protocols Performed in Aquatic and Land Environments by Healthy Individuals: A Systematic Review and Meta-Analysis. Sports Med. 2022, 52, 2247–2270. [Google Scholar] [CrossRef] [PubMed]
- Swain, D.P.; Leutholtz, B.C.; King, M.E.; Haas, L.A.; Branch, J.D. Relationship between% heart rate reserve and%??VO2reserve in treadmill exercise. Med. Sci. Sports Exerc. 1998, 30, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Solheim, T.J.; Keller, B.G.; Fountaine, C.J. VO2 Reserve vs. Heart Rate Reserve During Moderate Intensity Treadmill Exercise. Int. J. Exerc. Sci. 2014, 7, 311–317. [Google Scholar]
- Lounana, J.; Campion, F.; Noakes, T.D.; Medelli, J. Relationship Between% HRmax,% HR Reserve,% VO2max, And% VO2 Reserve in Elite Cyclists. Med. Sci. Sport. Exerc. 2007, 39, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Morais, J.E.; A Bragada, J.; Silva, R.; Nevill, A.M.; Nakamura, F.Y.; A Marinho, D. Analysis of the physiological response in junior tennis players during short-term recovery: Understanding the magnitude of recovery until and after the 25 seconds rule. Int. J. Sports Sci. Coach. 2022, 0. [Google Scholar] [CrossRef]
- Pialoux, V.; Genevois, C.; Capoen, A.; Forbes, S.C.; Thomas, J.; Rogowski, I. Playing vs. Nonplaying Aerobic Training in Tennis: Physiological and Performance Outcomes. PLoS ONE 2015, 10, e0122718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brechbuhl, C.; Girard, O.; Millet, G.P.; Schmitt, L. On the Use of a Test to Exhaustion Specific to Tennis (TEST) with Ball Hitting by Elite Players. PLoS ONE 2016, 11, e0152389. [Google Scholar] [CrossRef] [PubMed]
- Kilit, B.; Arslan, E. Effects of High-Intensity Interval Training vs. on-Court Tennis Training in Young Tennis Players. J. Strength Cond. Res. 2019, 33, 188–196. [Google Scholar] [CrossRef]
- Beltz, N.M.; Gibson, A.L.; Janot, J.M.; Kravitz, L.; Mermier, C.M.; Dalleck, L.C. Graded Exercise Testing Protocols for the Determination of VO2max: Historical Perspectives, Progress, and Future Considerations. J. Sport. Med. 2016, 2016, 3968393. [Google Scholar] [CrossRef] [Green Version]
- Durmić, T.; Ðjelić, M.; Gavrilović, T.; Antić, M.; Jeremić, R.; Vujović, A.; Mihailović, Z.; Zdravkovic, M. Usefulness of heart rate recovery parameters to monitor cardiovascular adaptation in elite athletes: The impact of the type of sport. Physiol. Int. 2019, 106, 81–94. [Google Scholar] [CrossRef]
- Lazic, J.S.; Dekleva, M.; Soldatovic, I.; Leischik, R.; Suzic, S.; Radovanovic, D.; Djuric, B.; Nesic, D.; Lazic, M.; Mazic, S. Heart rate recovery in elite athletes: The impact of age and exercise capacity. Clin. Physiol. Funct. Imaging 2015, 37, 117–123. [Google Scholar] [CrossRef]
- Bragada, J.A.; Bartolomeu, R.F.; Rodrigues, P.M.; Magalhães, P.M.; Bragada, J.P.; Morais, J.E. Validation of StepTest4all for Assessing Cardiovascular Capacity in Young Adults. Int. J. Environ. Res. Public Health 2022, 19, 11274. [Google Scholar] [CrossRef]
- Djurić, B.; Suzić, S. Heart Rate Recovery: Short Review of Methodology. Med. Podml. 2016, 67, 48–50. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Fernandez, J.; García-Tormo, V.; Santos-Rosa, F.J.; Teixeira, A.S.; Nakamura, F.Y.; Granacher, U.; Sanz-Rivas, D. The Effect of a Neuromuscular vs. Dynamic Warm-up on Physical Performance in Young Tennis Players. J. Strength Cond. Res. 2020, 34, 2776–2784. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; ISBN 1-4698-2666-6. [Google Scholar]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-Predicted Maximal Heart Rate Revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [Green Version]
- Micklewright, D.; Gibson, A.S.C.; Gladwell, V.; Al Salman, A. Development and Validity of the Rating-of-Fatigue Scale. Sports Med. 2017, 47, 2375–2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seiler, S.; Tønnessen, E. Intervals, Thresholds, and Long Slow Distance: The Role of Intensity and Duration in Endurance Training. Sportscience 2009, 13, 32–53. [Google Scholar]
- Ferguson, C.J. An effect size primer: A guide for clinicians and researchers. Prof. Psychol. Res. Pract. 2009, 40, 532–538. [Google Scholar] [CrossRef] [Green Version]
- Morais, J.E.; Sanders, R.H.; Papic, C.; Barbosa, T.M.; Marinho, D.A. The Influence of the Frontal Surface Area and Swim Velocity Variation in Front Crawl Active Drag. Med. Sci. Sports Exerc. 2020, 52, 2357–2364. [Google Scholar] [CrossRef]
- Barbosa, T.M.; Morais, J.E.; Forte, P.; Neiva, H.; Garrido, N.D.; Marinho, D.A. A Comparison of Experimental and Analytical Procedures to Measure Passive Drag in Human Swimming. PLoS ONE 2015, 10, e0130868. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Dalleck, L.C.; Kravitz, L. Relationship Between %Heart Rate Reserve And %VO2 Reserve During Elliptical Crosstrainer Exercise. J. Sports Sci. Med. 2006, 5, 662–671. [Google Scholar]
- Daniels, J.T.; Yarbrough, R.; Foster, C. Changes in $$\dot V $$ O2 Max and Running Performance with Training. Eur. J. Appl. Physiol. Occup. Physiol. 1978, 39, 249–254. [Google Scholar] [CrossRef]
- Butts, N.K.; A Henry, B.; McLean, D. Correlations between VO2max and performance times of recreational triathletes. J. Sports Med. Phys. Fit. 1991, 31, 339–344. [Google Scholar]
- Mahon, A.D.; Anderson, C.S.; Hipp, M.J.; Hunt, K.A. Heart Rate Recovery from Submaximal Exercise in Boys and Girls. Med. Sci. Sports Exerc. 2003, 35, 2093–2097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaafar, Z.; Lim, Y.Z. A comparison of low and high dose of moderate intensity aerobic exercise on heart rate recovery of the sedentary adults: A pragmatic randomised controlled trial. J. Sports Med. Phys. Fit. 2022. [Google Scholar] [CrossRef] [PubMed]
- Daanen, H.A.; Lamberts, R.P.; Kallen, V.L.; Jin, A.; Van Meeteren, N.L. A Systematic Review on Heart-Rate Recovery to Monitor Changes in Training Status in Athletes. Int. J. Sports Physiol. Perform. 2012, 7, 251–260. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Machine Stage | Mean ± 1SD | |
|---|---|---|
| HRreserve (beats/min) | VO2reserve (mL/kg/min) | |
| 1 | 106.3 ± 16.3 | 27.8 ± 5.9 |
| 2 | 117.7 ± 19.8 | 32.0 ± 8.7 |
| 3 | 126.5 ± 15.4 | 34.7 ± 7.6 |
| 4 | 135.1 ± 11.4 | 36.7 ± 6.3 |
| 5 | 140.3 ± 9.2 | 38.5 ± 5.5 |
| Average | 126.0 ± 18.6 | 34.2 ± 7.6 |
| Mean ± 1SD | ||||
|---|---|---|---|---|
| VO2max (mL/kg/min) | VO2reserve (mL/kg/min) | HRmax (beats/min) | HRreserve (beats/min) | |
| Level #1—VO2reserve < 80% | 29.0 ± 5.6 | 25.5 ± 5.6 | 157.9 ± 13.7 | 102.5 ± 13.1 |
| Level #2—81% < VO2reserve ≤ 93% | 38.1 ± 4.6 | 34.6 ± 4.6 | 186.7 ± 12.0 | 131.3 ± 11.0 |
| Level #3—VO2reserve > 93% | 43.0 ± 4.8 | 39.5 ± 4.8 | 192.7 ± 11.5 | 137.5 ± 10.4 |
| VO2 Level #1 | VO2 Level #2 | VO2 Level #3 | |
|---|---|---|---|
| HRrecovery(30s) level #1 | 30.14 ± 9.13rs = 0.343 (p = 0.230) | ||
| HRrecovery(30s) level #2 | 26.17 ± 8.20rs = −0.068 (p = 0.810) | ||
| HRrecovery(30s) level #3 | 21.91 ± 6.42rs = 0.468 (p = 0.028) |
| HRreserve | HRmax | Difference (beats/min) | ||
|---|---|---|---|---|
| HRreserve (beats/min) | HRtarget (beats/min) | HRtarget (beats/min) | ||
| HRreserve < 80% | <120 | <170 | <160 | 10 |
| HRreserve (80%–93%) | (120–140) | (170–190) | (160–186) | 10–4 |
| HRreserve > 93% | >140 | >190 | >186 | >4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morais, J.E.; Bragada, J.A. Relationship between Oxygen Uptake Reserve and Heart Rate Reserve in Young Male Tennis Players: Implications for Physical Fitness Monitoring. Int. J. Environ. Res. Public Health 2022, 19, 15780. https://doi.org/10.3390/ijerph192315780
Morais JE, Bragada JA. Relationship between Oxygen Uptake Reserve and Heart Rate Reserve in Young Male Tennis Players: Implications for Physical Fitness Monitoring. International Journal of Environmental Research and Public Health. 2022; 19(23):15780. https://doi.org/10.3390/ijerph192315780
Chicago/Turabian StyleMorais, Jorge E., and José A. Bragada. 2022. "Relationship between Oxygen Uptake Reserve and Heart Rate Reserve in Young Male Tennis Players: Implications for Physical Fitness Monitoring" International Journal of Environmental Research and Public Health 19, no. 23: 15780. https://doi.org/10.3390/ijerph192315780