
Physical Therapy Interventions in Patients with Anorexia Nervosa: A Systematic Review



Abstract
:1. Introduction
2. Methodology
2.1. Inclusion Criteria
2.2. Literature Search and Study Selection
2.3. Data Extraction and Risk-of-Bias Assessment
2.4. Certainty of Evidence
3. Results
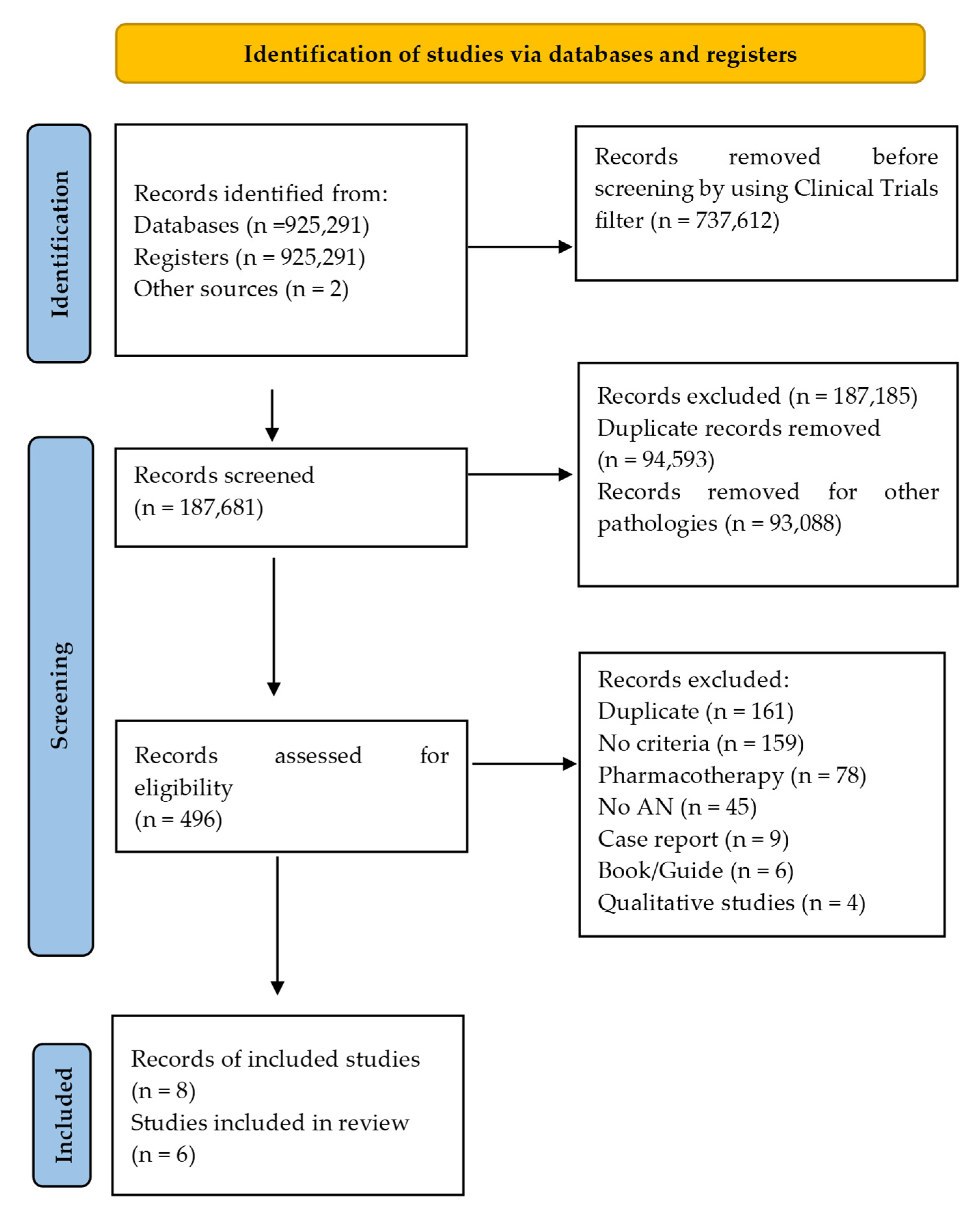
3.1. Search Results
3.2. Study Characteristics
3.3. Physiological and Muscular Effects
3.4. Psychological and Cognitive Effects
3.5. Behavioural Effects
3.6. Effects on Quality of Life
3.7. Risk of Bias and Certainty of Evidence
4. Discussion
4.1. Implications for Rehabilitation
4.2. Strengths and Limits
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mehler, P.S.; Brown, C. Anorexia nervosa–medical complications. J. Eat. Disord. 2015, 3, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, C.; Mehler, P.S. Medical complications of anorexia nervosa and their treatments: An update on some critical aspects. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2015, 20, 419–425. [Google Scholar] [CrossRef]
- Roux, H.; Chapelon, E.; Godart, N. Epidemiology of anorexia nervosa: A review. L’Encéphale 2013, 39, 85–93. [Google Scholar] [CrossRef] [PubMed]
- van Eeden, A.E.; van Hoeken, D.; Hoek, H.W. Incidence, prevalence and mortality of anorexia nervosa and bulimia nervosa. Curr. Opin. Psychiatry 2021, 34, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Franko, D.L.; Keshaviah, A.; Eddy, K.T.; Krishna, M.; Davis, M.C.; Keel, P.K.; Herzog, D.B. A Longitudinal Investigation of Mortality in Anorexia Nervosa and Bulimia Nervosa. Am. J. Psychiatry 2013, 170, 917–925. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch. Gen. Psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckert, E.D.; Halmi, K.A.; Marchi, P.; Grove, W.; Crosby, R. Ten-year follow-up of anorexia nervosa: Clinical course and outcome. Psychol. Med. 1995, 25, 143–156. [Google Scholar] [CrossRef]
- Vancampfort, D.; Vanderlinden, J.; De Hert, M.; Soundy, A.; Adámkova, M.; Skjaerven, L.H.; Catalán-Matamoros, D.; Gyl-lensten, A.L.; Gómez-Conesa, A.; Probst, M. A systematic review of physical therapy interventions for patients with anorexia and bulemia nervosa. Disabil. Rehabil. 2014, 36, 628–634. [Google Scholar] [CrossRef]
- Rizk, M.; Mattar, L.; Kern, L.; Berthoz, S.; Duclos, J.; Viltart, O.; Godart, N. Physical Activity in Eating Disorders: A Systematic Review. Nutrients 2020, 12, 183. [Google Scholar] [CrossRef] [Green Version]
- Stice, E. Risk and maintenance factors for eating pathology: A meta-analytic review. Psychol. Bull. 2002, 128, 825–848. [Google Scholar] [CrossRef]
- Cook, B.; Engel, S.; Crosby, R.; Hausenblas, H.; Wonderlich, S.; Mitchell, J. Pathological motivations for exercise and eating disorder specific health-related quality of life. Int. J. Eat. Disord. 2014, 47, 268–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achamrah, N.; Coëffier, M.; Déchelotte, P. Physical activity in patients with anorexia nervosa. Nutr. Rev. 2016, 74, 301–311. [Google Scholar] [CrossRef]
- Gümmer, R.; Giel, K.E.; Schag, K.; Resmark, G.; Junne, F.P.; Becker, S.; Zipfel, S.; Teufel, M. High Levels of Physical Activity in Anorexia Nervosa: A Systematic Review. Eur. Eat. Disord. Rev. 2015, 23, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Woodside, B.D.; Staab, R. Management of psychiatric comorbidity in anorexia nervosa and bulimia nervosa. CNS Drugs 2006, 20, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Agras, W.S. The Consequences and Costs of the Eating Disorders. Psychiatr. Clin. N. Am. 2001, 24, 371–379. [Google Scholar] [CrossRef]
- Schalla, M.A.; Stengel, A. Gastrointestinal alterations in anorexia nervosa-A systematic review. Eur. Eat. Disord. Rev. 2019, 27, 447–461. [Google Scholar] [CrossRef]
- Bemer, P.; di Lodovico, L.; Haykanush, O.; Théodon, H.; Briot, K.; Carlier, R.; Dicembre, M.; Duquesnoy, M.; Melchior, J.; Hanachi, M. Bone mineral density at extremely low weight in patients with anorexia nervosa. Clin. Endocrinol. 2021, 95, 423–429. [Google Scholar] [CrossRef]
- Gosseaume, C.; Dicembre, M.; Bemer, P.; Melchior, J.-C.; Hanachi, M. Somatic complications and nutritional management of anorexia nervosa. Clin. Nutr. Exp. 2019, 28, 2–10. [Google Scholar] [CrossRef] [Green Version]
- Fichter, M.M.; Quadflieg, N.; Crosby, R.D.; Koch, S. Long-term outcome of anorexia nervosa: Results from a large clinical longitudinal study. Int. J. Eat. Disord. 2017, 50, 1018–1030. [Google Scholar] [CrossRef]
- Soundy, A.; Stubbs, B.; Probst, M.; Gyllensten, A.L.; Skjaerven, L.H.; Catalan-Matamoros, D.; Vancampfort, D. Considering the Role of Physical Therapists Within the Treatment and Rehabilitation of Individuals With Eating Disorders: An International Survey of Expert Clinicians. Physiother. Res. Int. 2016, 21, 237–246. [Google Scholar] [CrossRef]
- Ziora, K.; Ziora, D.; Oswiecimska, J.; WRoczniak, W.; Machura, E.; Dworniczak, S.; Tomalak, W.; Dyduch, A. Spirometric parameters in malnourished girls with anorexia nervosa. J. Physiol. Pharmacol. 2008, 59 (Suppl. S6), 801–807. [Google Scholar] [PubMed]
- Probst, M.; Majeweski, M.L.; Albertsen, M.N.; Catalan-Matamoros, D.; Danielsen, M.; de Herdt, A.; Duskova Zakova, H.; Fabricius, S.; Joern, C.; Kjölstad, G.; et al. Physiotherapy for patients with anorexia nervosa. Adv. Eat. Disord. 2013, 1, 224–238. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems Tenth Revision, 2nd ed.; World Health Organization, Ed.; WHO Library: Geneva, Switzerland, 2004. [Google Scholar]
- MeSH. National Library of Medicine. In Physical Therapy Modalities; Rockville Pike, MD, USA 2006. Available online: https://www.ncbi.nlm.nih.gov/mesh/68026741 (accessed on 3 August 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 10, 89. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J. Chapter 8: Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.0, 2019th ed.; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2019. [Google Scholar]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; deBeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Thien, V.; Thomas, A.; Markin, D.; Birmingham, C.L. Pilot study of a graded exercise program for the treatment of anorexia nervosa. Int. J. Eat. Disord. 2000, 28, 101–106. [Google Scholar] [CrossRef]
- Hart, S.; Field, T.; Hernandez-Reif, M.; Nearing, G.; Shaw, S.; Schanberg, S.; Kuhn, C. Anorexia nervosa symptoms are reduced by massage therapy. Eat. Disord. 2001, 9, 289–299. [Google Scholar] [CrossRef]
- del Valle, M.F.; Pérez, M.; Santana-Sosa, E.; Fiuza-Luces, C.; Bustamante-Ara, N.; Gallardo, C.; Villaseñor, A.; Graell, M.; Morandé, G.; Romo, G.R.; et al. Does Resistance Training Improve the Functional Capacity and Well Being of Very Young Anorexic Patients? A Randomized Controlled Trial. J. Adolesc. Health 2010, 46, 352–358. [Google Scholar] [CrossRef]
- Catalan-Matamoros, D.; Helvik-Skjaerven, L.; Labajos-Manzanares, M.T.; Martínez-De-Salazar-Arboleas, A.; Sánchez-Guerrero, E. A pilot study on the effect of Basic Body Awareness Therapy in patients with eating disorders: A ran-domized controlled trial. Clin. Rehabil. 2011, 25, 617–626. [Google Scholar] [CrossRef]
- Fernández-Del-Valle, M.; Larumbe-Zabala, E.; Morande-Lavin, G.; Perez Ruiz, M. Muscle function and body composition profile in adolescents with restrictive anorexia nervosa: Does resistance training help? Disabil. Rehabil. 2016, 38, 346–353. [Google Scholar] [CrossRef]
- Fernandez-del-Valle, M.; Larumbe-Zabala, E.; Graell-Berna, M.; Perez-Ruiz, M. Anthropometric changes in adolescents with anorexia nervosa in response to resistance training. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2015, 20, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Del-Valle, M.; Larumbe-Zabala, E.; Villaseñor-Montarroso, A.; Cardona Gonzalez, C.; Diez-Vega, I.; Lopez Mo-jares, L.M.; Perez Ruiz, M. Resistance training enhances muscular performance in patients with anorexia nervosa: A rando-mized controlled trial. Int. J. Eat. Disord. 2014, 47, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Hay, P.; Touyz, S.; Arcelus, J.; Pike, K.; Attia, E.; Crosby, R.D.; Madden, S.; Wales, J.; la Puma, M.; Heriseanu, A.I.; et al. A randomized controlled trial of the compuLsive Exercise Activity TheraPy (LEAP): A new approach to compulsive exercise in anorexia nervosa. Int. J. Eat. Disord. 2018, 51, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Ng, L.W.; Ng, D.P.; Wong, W. Is supervised exercise training safe in patients with anorexia nervosa? A meta-analysis. Physiotherapy 2013, 99, 1–11. [Google Scholar] [CrossRef]
- Quiles Marcos, Y.; León Zarceño, E.; López López, J.A. Effectiveness of exercise-based interventions in patients with anorexia nervosa: A systematic review. Eur. Eat. Disord. Rev. 2021, 29, 3–19. [Google Scholar] [CrossRef]
- Moola, F.J.; Gairdner, S.; Amara, C. Exercise in the care of patients with anorexia nervosa: A systematic review of the literature. Ment. Health Phys. Act. 2013, 6, 59–68. [Google Scholar] [CrossRef]


{kind=link}
| Scheme. | Participants N and Diagnosis; n Females/Males; (% Female); Mean Age (Years Treatment/Control) | Treatment (Numbers) [Control (Numbers)] | Duration; Frequency (Sessions/wk); min/Session; [Training: Individual, Group, or Unspecified] | Co-Interventions | Outcome Measures | Results Treatment vs. Control (from Baseline to Post-Test) | Adverse Effects |
|---|---|---|---|---|---|---|---|
| Thien et al., 2000 [30] | 16 AN; 15/ 1; 93.75%; 29/36.1 | Stretching, isometrics, cardiovascular, resistive stretching, increase weekly (n = 8) [Standard Care and Limit exercise (n = 8)] | 3 months; 3/wk [Training: unspecified] | Standard Care: Psychiatric follow-up | BMI BF QOL: SF-36 | ≠BMI (from 20.26 ± 1.8 vs. 17.2 ± 1.6 at baseline; to increase 1.0 ± 1.3 vs. increase 0.8 ± 1.1 at 3 months; p = 0.37) ≠BF (from 21.0 ± 2.9 vs. 16.7 ± 4.9 at baseline; to increase 0.9 ± 2.1 vs. increase 0.5 ± 2.6 at 3 months; p = 0.39) ↑ SF-36 (from 58.8 ± 13.9 vs. 53.3 ± 14.5 at baseline; to increase 6.6 ± 7.0 vs. increase −12.0 ± 25.5 at 3 months; p = 0.07) | Not reported |
| Hart et al., 2001 [31] | 19 AN; 19/0; 100%; 24.9/26.3 | Full body massage Instruction to relax and discourage her from talking (n = 10) [Standard Care n = 9] | 5 weeks; 2/wk; 30 min. [Training: unspecified] | Standard Care: Psychiatric and nutritional follow-up Engaged other activities, such as movement therapies | Anxiety: STAI Mood States: POMS Eating Disorders: EDI | ↑ STAI (from 52.3/40.1 vs. 50.2/46.5 at baseline; to 47.3/37.0 vs. 48.8/46.1 at 5 wk; p < 0.01) ↑ POMS (from 39.5/28.5 vs. 32.8/31.7 at baseline; to 30.0/20.2 vs. 29.1/25.0 at 5 wk; p < 0.05) ↑ EDI (from 88.8 vs. 83.1 at baseline; to 66.0 vs. 80.5 at 5 wk; p < 0.05) | Not reported |
| Fernandez-Del-Valle et al., 2010 [32] | 22 AN; 20/2; 90.90%; 14.7 ± 0.6/14.2 ± 1.2 | Strength training, Isometric contraction with their body weight or barbells of 1–3 kg (n = 11) [Standard Care Control and maintain physical activity level n = 11] | 12 weeks; 2/wk; 60–70 min. [Training: individual] | Standard Care: Psychotherapy Dietary counseling | BMI BF Muscle strength: 6RM | ≠BMI (from 18.7 ± 1.7 vs. 18.2 ± 1.5 at baseline; to 18.2 ± 2.2 vs. 18.3 ± 1.6 at 12 wk; p = 0.543) ≠BF (from 14.8 ± 2.9 vs. 13.8 ± 2.6 at baseline; to 13.7 ± 3.3 vs. 13.9 ± 2.4 at 12 wk; p = 0.247) ↑ 6RM (from 45.4 ± 5.7 vs. 46.0 ± 11.8 at baseline; to 59.0 ± 13.7 vs. 46.9 ± 11.3 at 12 wk; p = 0.009) | Program well tolerated |
| Catalan-Matamoros et al., 2011 [33] | 8 AN; 10 BN; 3 atypical AN; 1 atypical BN 6 non-detailed diagnosis (28) 26/2; 92.85%; 29.5/25.2 | Basic Body Awareness Therapy (n = 14) [Standard Care Control n = 8] | 7 weeks; 1/wk; 1 h. (during 2 wk); 2/wk; 1.5 h. [Total 12 sessions/patient] [Training: individual and group] | Standard care: Psychotherapy and Psychiatric follow-up | Eating Disorder: EDI Body Attitude: BAT Eating Attitude: EAT-40 | ↑ EDI (33.6 ± 32.0EG vs. 7.3 ± 13.7CG at 7 wk; p = 0.015) ↑ BAT (24.7 ± 26.4 EG vs. −8.3 ± 28.4CG at 7 wk; p = 0.012) ↑ EAT-40 (14.8 ± 21.8 EG vs. 1.2 ± 4.1 CG at 7 wk; p = 0.039) | Not reported |
| Fernandez-Del-Valle et al., 2014; 2015; 2016 [34,35,36] | 44 AN-R; 44/0; 100%; 12.61/13.0 | High intensity resistance program: Isometrics and stretching (n = 18) [Standard Care Control n = 18] | 8 weeks; 3 /wk; 50–60 min. [follow-up 4 wk] [Training: individual] | Standard Care: Psychological therapy and control calorie intake | BMI BF Muscle strength: Bench press; Leg press; Lateral row Muscular areas: AMA; MTMA Relative strength: Strength to BW; Strength to SMM | ≠BMI (from 17.28 ± 2.55 vs. 18.12 ± 2.11 at baseline; to 17.82 ± 2.50 vs. 18.50 ± 2.10 at 8 wk; p=0.242) ≠BF (from 25% vs. 26% at baseline; to 24% vs. 27% at 8 wk; p = 0.075) ↑ Bench press IG 41% (mean dif. –1.65) at 8 wk; p < 0.001 ↑ Leg press IG 52% (mean dif. 3.80) at 8 wk; p < 0.001 ↑ Lateral row IG 37% (mean dif. –2.27) at 8 wk; p < 0.001 ↑ AMA (from 21.3 ± 5.2 vs. 25.5 ± 5.6 at baseline to 23.3 ± 5.7 vs. 24.1 ± 5.1 at 8 wk; p = 0.030 ↑ MTMA (from 122.99 ± 19.4 vs. 137.63 ± 20.3 at baseline to 128.00 ± 20.8 vs. 133.74 ± 17.4 at 8 wk; p = 0.061) Strength to BW at 8 wk: ↑ Bench press 32.97% (27.14%–49.29%); p < 0.001 ↑ Leg press 49.59% (32.93%–66.24%); p < 0.001 ↑ Lateral row 38.22% (22.53%–43.40%); p < 0.001 Strength to SMM at 8 wk: ↑ Bench press 37.11% (28.20%–46.01%); p < 0.001 ↑ Leg press 49.11% (31.79%–66.43%); p < 0.001 ↑ Lateral row 32.56% (21.39%–43.72%); p < 0.001 Strength to BW follow-up 4 wk: ↑ Bench press (mean dif. –0.23 vs. −0.01); p < 0.001 ↑ Lateral row (mean dif. –0.15 vs. −8.8); p = 0.014 Strength to SMM follow-up 4 wk: ↑ Bench press (mean dif. –0.68 vs. −0.04); p < 0.001 ↑ Leg press (mean dif. −0.79 vs. –0.13); p = 0.039 ↑ Lateral row (mean dif. –0.44 vs. −0.27); p = 0.005 | No adverse effects or health problems |
| Hay et al., 2018 [37] | 78 AN; 74/4; 94.87%; 26.1/28.6 | Compulsive Exercise Activity Therapy (LEAP) (n = 39) [CBT-AN Control n = 39] | 8.5 months; 2/wk (during 4 wk); 1/wk; 50 min. [Intervention 8 LEAP sessions and 26 CBT-AN sessions; Control 34 CBT-AN sessions] [Training: individual] | CBT-AN | BMI Eating Disorder: EDE-Q Behavior to Physical Exercise: EBQ; CET; CES Depression and anxiety: K-10 Motivation to change: ANSOCQ QOL: EDQOL; HRQOL-12 | ↑ BMI (16.58 ± 1.04 vs. 16.47 ± 1.2 at baseline; to 16.99 ± 4.04 vs. 18.49 ± 2.9 at 34 wk; p = 0.01) ≠EDE (from 3.54 ± 1.29 vs. 3.18 ± 1.29 at baseline; to 2.28 ± 1.32 vs. 2.16 ± 1.42 at 34 wk) ≠EBQ (from 45.6 ± 21.2 vs. 46.0 ± 24.3 at baseline; to 27.1 ± 21.1 vs. 40.0 ± 27.5 at 34 wk) ↑ CET (from 15.7 ± 4.3 vs. 16.8 ± 4.5 at baseline; to 11.9 ± 5.5 vs. 14.1 ± 4.8 at 34 wk; p < 0.06) ≠CES (from 60.8 ± 27.9 vs. 70.1 ± 26.7 at baseline; to 36.8 ± 26.5 vs. 47.8 ± 30.4 at 34 wk) ≠K-10 (from 31.5 ± 9.2 vs. 30.4 ± 9.9 at baseline; to 24.3 ± 8.4 vs. 22.3 ± 9.8 at 34 wk) ≠ANSOCQ (from 2.4 ± 0.6 vs. 2.4 ± 0.6 at baseline; to 3.0 ± 0.9 vs. 3.3 ± 1.0 at 34 wk) ↑ EDQOL (from 1.6 ± 0.6 vs. 1.8 ± 0.8 at baseline; to 1.1 ± 0.8 vs. 1.0 ± 1.0 at 34 wk; p < 0.05) ≠HRQoL (from 28.7 ± 10.9 vs. 29.5 ± 13.0 at baseline; to 35.6 ± 10.0 vs. 39.1 ± 11.4 at 34 wk) | Not reported |
| Study | Sequence | Allocation | Blinding1 | Blinding2 | Outcome1 | Outcome2 | Other |
|---|---|---|---|---|---|---|---|
| Thien V et al., 2000 [30] | (+) | (+) | (-) | (-) | (+) | (+) | (+) |
| Hart S et al., 2001 [31] | (+) | (+) | (-) | (-) | (-) | (-) | (+) |
| Del Valle MF et al., 2010 [32] | (+) | (+) | (-) | (-) | (+) | (+) | (+) |
| Catalan-Matamoros D et al., 2011 [33] | (+) | (+) | (-) | (-) | (+) | (+) | (+) |
| Fernandez-Del-Valle M et al., 2014; 2015; 2016 [34,35,36] | (+) | (-) | (-) | (-) | (+) | (+) | (+) |
| Hay P et al., 2018 [37] | (+) | (+) | (+) | (+) | (+) | (+) | (-) |
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirect Evidence * | Inaccuracy | Publication Bias ** | Impact | Quality | Importance *** |
|---|---|---|---|---|---|---|---|---|---|
| Physiological and muscular effects (measured with BMI) (Follow-up 8 weeks–8.5 months) | |||||||||
| 4 [30,32,34,35,36,37] | randomized trials | serious a | serious b | no serious | serious c | no serious | serious c | ⊕⊕⊕⊝ MODERATE | 4/9 |
| Physiological and muscular effects (measured with muscle strength) (Follow-up 8–12 weeks) | |||||||||
| 2 [32,34,35,36] | randomized trials | serious a | no serious d | no serious | no serious d | no serious | no serious d | ⊕⊕⊕⊝ MODERATE | 5/9 |
| Physiological and muscular effects (measured with BF) (Follow-up 8–12 weeks) | |||||||||
| 3 [30,32,34,35,36] | randomized trials | serious a | serious e | no serious | serious e | no serious | serious e | ⊕⊕⊝⊝ LOW | 2/9 |
| Physiological and muscular effects (measured with AMA and MTMA) (Follow-up 8 weeks) | |||||||||
| 1 [34,35,36] | randomized trial | serious a | no serious f | no serious | no serious f | no serious | no serious f | ⊕⊕⊝⊝ LOW | 3/9 |
| Psychological effects (depression and anxiety measured with K-10 and STAI) (Follow-up 5 weeks–8.5 months) | |||||||||
| 2 [31,37] | randomized trials | serious a | serious g | no serious | serious g | no serious | no serious g | ⊕⊕⊝⊝ LOW | 3/9 |
| Cognitive effects (mood measured with POMS) (Follow-up 5 weeks) | |||||||||
| 1 [31] | randomized trial | serious a | no serious h | no serious | no serious h | no serious | no serious h | ⊕⊕⊕⊝ MODERATE | 4/9 |
| Cognitive effects (attitude measured with BAT and EAT-40) (Follow-up 7 weeks) | |||||||||
| 1 [33] | randomized trial | serious a | no serious i | no serious | no serious i | no serious | no serious i | ⊕⊕⊕⊝ MODERATE | 4/9 |
| Behavioral effects (eating measured with EDI, ANSOQ and EDE-Q) (Follow-up 5 weeks–8.5 months) | |||||||||
| 3 [31,33,37] | randomized trials | serious a | no serious j | no serious | no serious j | no serious | no serious j | ⊕⊕⊕⊝ MODERATE | 4/9 |
| Behavioral effects (impulse control measured with CET) (Follow-up 8.5 months) | |||||||||
| 1 [37] | randomized trial | no serious | no serious k | no serious | no serious k | no serious | no serious k | ⊕⊕⊝⊝ LOW | 2/9 |
| Quality of life effects (measured with SF-36, EDQOL and HRQOL-12) (Follow-up 12 weeks–8.5 months) | |||||||||
| 2 [30,37] | randomized trials | serious a | no serious l | no serious | no serious l | no serious | no serious l | ⊕⊕⊕⊝ MODERATE | 4/9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minano-Garrido, E.J.; Catalan-Matamoros, D.; Gómez-Conesa, A. Physical Therapy Interventions in Patients with Anorexia Nervosa: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 13921. https://doi.org/10.3390/ijerph192113921
Minano-Garrido EJ, Catalan-Matamoros D, Gómez-Conesa A. Physical Therapy Interventions in Patients with Anorexia Nervosa: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(21):13921. https://doi.org/10.3390/ijerph192113921
Chicago/Turabian StyleMinano-Garrido, Emilio Jose, Daniel Catalan-Matamoros, and Antonia Gómez-Conesa. 2022. "Physical Therapy Interventions in Patients with Anorexia Nervosa: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 21: 13921. https://doi.org/10.3390/ijerph192113921