
The Use of Mobile Health Interventions for Outcomes among Middle-Aged and Elderly Patients with Prediabetes: A Systematic Review
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Research Sample
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
2.6. Data Synthesis
3. Results
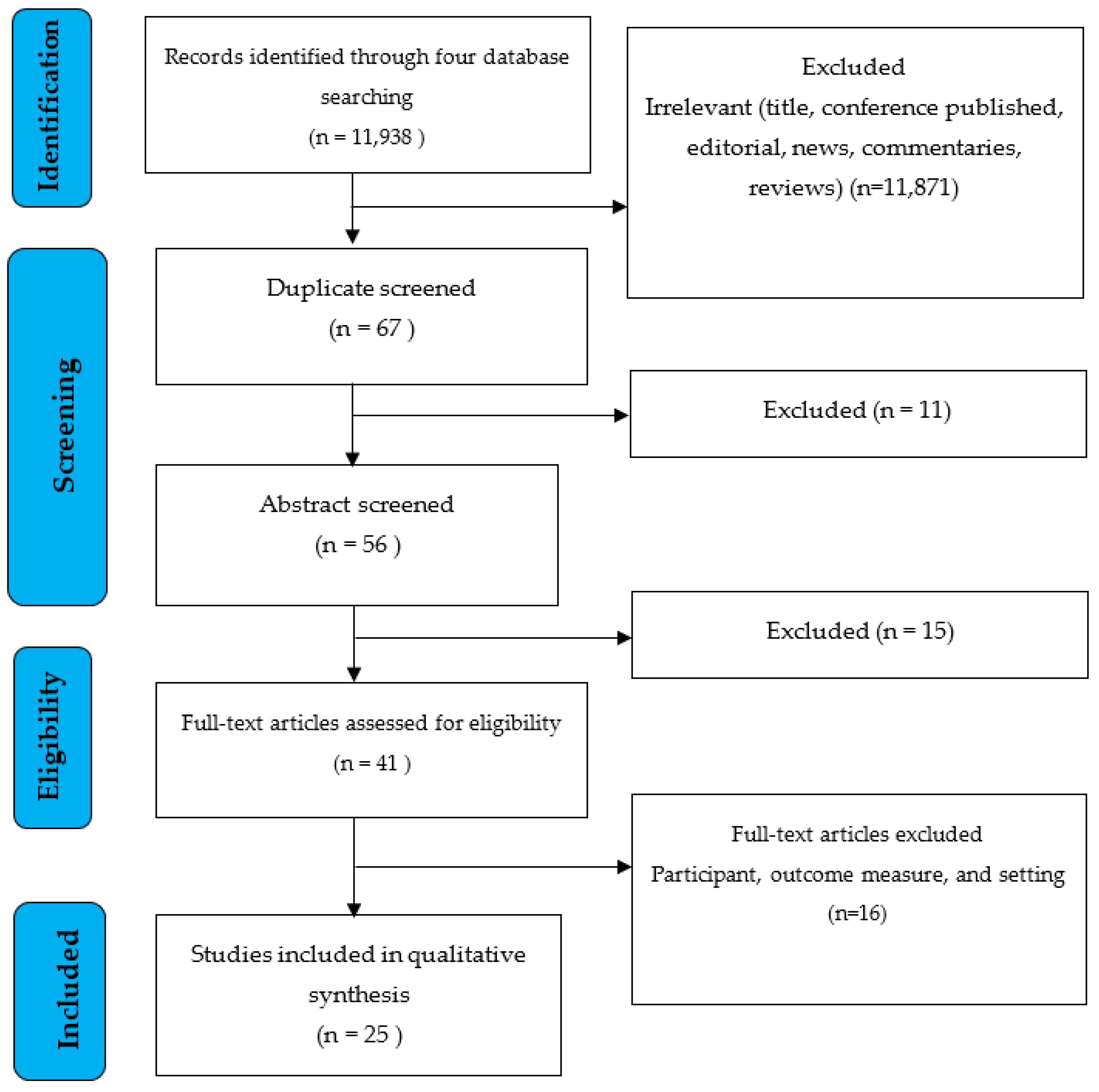
3.1. Search Results
3.2. Characteristics of the Studies
3.3. Quality Assessment

{kind=link}
| Author, Year | Subject Criteria | Number of Subjects | Duration of Intervention and Study Location | Type of Mobile Health | Functions Used | Methods | Outcome Measures | Measurement Methods Detail |
|---|---|---|---|---|---|---|---|---|
| Ramachandran et al., 2013 [36] | Impaired glucose tolerance (OGTT: 140–199 mg/dL) Age: 35–55 years BMI: ≥23 kg/m² or more. Sex: Male | Randomized Participants: 537 Analyzed Participants: 537 Completed: 527 | 24 months Southeast India | Text message based: Short message Service (SMS), Text Message based on the transtheoretical model stage | Encouraged lifestyle change could reduce incident type 2 diabetes | RCT (prospective,2-arm parallel-group) | Primary Outcome
| Primary Outcome Incident T2DM: The estimated cumulative incidence of T2DM was calculated using unadjusted Cox regression analysis. Secondary Outcome Body Mass Index (BMI), Waist circumference, and Blood Pressure (systolic and diastolic): Mean of two readings obtained at each visit using standardized methods. Physical activity evaluation using a questionnaire Total dietary intake: dietary intake as determined by a 24-h recall Lipid profile (total cholesterol, triglycerides (TG), and HDL): fasting venous plasma sampling HOMA-IR: ([fasting insulin (mU/L) × fasting glucose (mmol/L)] formula/22·5) |
| Chen et al., 2014 [55] | Impaired Fasting Glucose (FG:100–125 mg/dL) Age: 40–70 years BMI: Not Reported Sex: Male and Female | Eligibility Participant: 253 Analyzed Participant: 231 Completed: 231 | 6 months Lu’an Anhui, China | Website Based: SWAP-DM2 | Risk scoring and personalized counseling lifestyle management | Quasi-Experimental Mixed Methods |
| not reported in detail |
| Block et al., 2015 [37] | Impaired Fasting Glucose (FG: 100–125 mg/dL) and or Prediabetes (A1c: 5.7–6.4%) Age: 30–69 years BMI: ≥ 27 kg/m (BMI ≥25 kg/m for Asian participants) Sex: Male and Female | Randomized Participants: 340 Analyzed Participants: 339 Completed: 292 | 6 months Berkeley USA | “Hybrid” Mobile phone apps and Website Based: The Alive-PD | To improve glycemic control and reduce diabetes risk through lasting changes in physical activity and eating habits | RCT (wait-list controlled Trial) | Primary Outcome
| not reported in detail |
| Fukuoka et al., 2015 [38] | Impaired Fasting Glucose (FG: 100–125 mg/dL) and or Prediabetes (A1c: 5.7–6.4%) Age: ≥35 years BMI: BMI of at least 25 kg/m (BMI > 23 kg/m for Asian-Pacific Islanders participants) Sex: Male and Female | Randomized Participants: 61 Analyzed Participant: 61 Completed: 56 | 5 months San Francisco and Berkeley, CA, USA | Mobile phone apps based: The mDPP trial app | to supplement the in-person sessions and was intended to enhance their effect. Electronic diaries for self-monitoring of weight, activity, and caloric intake, daily reminders. | RCT (2-arm, parallel groups) | Primary Outcome
| All outcomes are objectively measured and reported by participants. but not in detail |
| Fischer et al., 2016 [39] | Prediabetes (HbA1c from 5.7–6.4%) and Obesity (BMI 25–50 kg/m2) Age: ≥18 years BMI: 25–50 kg/m2 Sex: Male and Female | Randomized Participants: 163 Analyzed Participants: 157 Completed Participants: 157 | 12 months Denver, Colorado, USA | Text message based: Text message using the National DPP (Diabetes Prevention Program) curriculum content (SMS4PreDM) | To support weight loss | RCT (parallel groups) | Primary Outcome
| not reported in detail |
| Bender et al., 2018 [40] | Prediabetes (HbA1c from >5.6%) or Impaired Fasting Glucose (FG; 100–125 mg/dL) Or Impaired glucose tolerance (OGTT: 140–199 mg/dL) Age: ≥18 years BMI: >23 kg/m2 Sex: Male and Female Notes: Self-identified as Filipino | Randomized Participants: 67 Analyzed Participants: 61 Completed Participants: 61 | 6 months San Francisco, USA | Mobile phone apps based: (Fit and Trim) App Plus Wearable Devices (Fitbit Devices) | Weight loss lifestyle intervention including virtual social support | RCT (2-arm, wait-list controlled Trial) | Primary outcome:
| not reported in detail |
| Sharit et al., 2018 [56] | Prediabetes (HbA1c from 5.7–6.4%) or Impaired Fasting Glucose (FG: 100–125 mg/dL) Or Impaired glucose tolerance (OGTT: 140–199 mg/dL) Age: ≥20 years BMI: 25–42 kg/m2 Sex: Male and Female | Eligibility Participant: 38 Analyzed Participants: 38 Completed Participants: 38 | 13 weeks A large city in the USA | Website based: Practice on use of Track Health (TH) Journals and Vitals + Readings features as a basis for promoting positive Physical Activity (PA) and dietary lifestyles | Promoting positive Physical Activity (PA) and dietary lifestyles | Quasi-Experimental (pilot 3 month clinical trial pre-post design) | Primary outcome:
| not reported in detail |
| Griauzde et al., 2019 [41] | Prediabetes (HbA1c from 5.7–6.4%) Age: >18 years old BMI: Not Reported Sex: Male and Female | Randomized Participants: 69 Analyzed Participants: 55 Completed Participants: 55 | 12 weeks Ann Arbor, MI, USA | Mobile phone apps based: App-Only And App-Plus Wearable device (Fitbit Devices) | To help individuals gain awareness of and control over the factors that influence their health behaviors (Sleep; Presence; Activity; Creativity; Eating) (S.P.A.C.E). | RCT (parallel, 3-arm) Mixed Methods |
| not reported in detail |
| Fischer et al., 2019 [57] | Prediabetes (HbA1c from 5.7 06.4%) Age: > 18 years old BMI: Not Reported | Eligibility Participant: 1.518 Analyzed Participants: 1.518 Completed Participants: 1.492 | 12 months Denver, Colorado, USA | Text message based: Text message using the National DPP (Diabetes Prevention Program) curriculum content (SMS4PreDM) | To support weight loss | Pragmatic trial |
| For SMS4PreDM participants, a repeating measure analysis used all weights available in the EHR from routine healthcare visits within a year of the individual’s start date, or matched identification dates for controls. |
| Ramos et al., 2020 [42] | Prediabetes (HbA1c from 5.7–6.4% within 3 months before study enrollment) Age: >18 years old BMI: NA Sex: Male and Female Notes: referral from the patient’s physician | Eligibility Participant: 1.513 Randomized Participants: 202 Analyzed Participants: 202 Completed Participants: 155 | 12 months New York, NY, USA | Mobile phone apps based: Noom’s App With the National DPP (Diabetes Prevention Program) curriculum content | To support weight loss | RCT (two-arm, parallel RCT) | Primary outcome:
Program engagement
| The DCA Vantage (Siemens) point-of-care (POC) HbA1c machine was used in primary care and endocrinology clinics. |
| Nandhita et al., 2020 [43] | Prediabetes (HbA1c from 6.0–6.4%) Age: 35–55 years (India) 40–74 years (UK) BMI: ≥23 kg/m2 (India) Sex: Male and Female Notes: Pre-screening: having three or more risk factors, including age 35–55 years, BMI ≥ 23 kg/m2, waist circumference ≥90 cm in men and ≥80 cm in women, first-degree family history of type 2 diabetes, history of hypertension or prediabetes, or habitual sedentary behavior | Randomized Participants: 2062 Analyzed Participants: 2062 Completed Participants: 1.763 | 24 months UK and India | Text message based: Short message Service (SMS), Text Message based on the transtheoretical model stage | To provide additional education and motivation. The messages provided tips, suggestions, and positive reinforcement for healthy behaviors including goal setting, physical activity, dietary planning, and personal strategies for a lifestyle change. | RCT (two-arm, parallel RCT) | Primary outcome:
| HbA1c international criteria for fasting plasma glucose or HbA1c at any study review visit or in any healthcare setting (UK); incident type 2 diabetes determined solely by HbA1c (India) Body Mass Index (BMI), Waist Circumference, and Blood Pressure (Systolic and Diastolic): the average of two readings taken by standard procedures at each visit. The serum lipid profile (total cholesterol, low-density lipoprotein, HDL-cholesterol, and triacylglycerols) and HbA1c were measured using standard enzymatic procedures with quality control. |
| Mcleod et al., 2020 [44] | Prediabetes (HbA1c from 5.9–6.6% current or tested in preceding 3 months) Age: 18–75 years BMI: ≥20–40 kg/m2 Sex: Male and Female Notes: participant included diabetes | Randomized Participants: 225 Analyzed Participants: 201 Completed Participants: 201 | 12 month The greater Wellington and Waikato regions of the North Island of New Zealand, | Mobile phone apps based: BetaMe/Melon App | a structured, in-person lifestyle modification program focused on weight reduction | RCT (parallel-group 2-arm single-blinded superiority trial) | Primary outcome:
| The Protocol describes standardized measurement procedures. |
| Muralidharan et al., 2020 [45] | Prediabetes Impaired Fasting Glucose (FG 100–125 mg/dL) Age: 20–65 years BMI: ≥25 kg/m2 Sex: Male andFemale | Randomized Participants: 741 Analyzed Participants: 561 Completed Participants: 561 | 4 month Chennai, Bangalore and New Delhi, India. | Mobile phone apps based: mDiab | To support Diabetes prevention program (DPP) and culturally modified it to suit the Indian population | RCT (parallel-group two-arm) |
| Omron HBF-306 Body Fat Monitor was used to calculate the percentage of body fat. Every day, the waist circumference was measured with a standard, non-stretchable, 1-inch tape measure that was calibrated. While calibrating, it was ensured that the difference between the two readings was no greater than 0.2 cm. If the measuring tape was damaged, whether stretched or twisted, or if graduations had been erased, it was replaced with a new one. The study participants were instructed to stand with their feet together and their arms by their sides, palms facing inward. The technician then determined the midpoint by locating the inferior margin of the last rib and the crest of the ileum. After ensuring the proper placement of the tape around the waist, a measurement to the nearest 0.1 cm was taken. Two measurements were taken, and the average of the two was taken. |
| Xu et al., 2020 [46] | Prediabetes (High risk for diabetes, measured by the American Diabetes Association (ADA) screening tool (score of ≥5 or) Age: ≥18 years BMI: NA Sex: Male and Female Notes: access to WeChat | Randomized Participants: 81 Analyzed Participants: 76 Completed Participants: 76 | 6 month Beijing, China | Mobile phone apps based: DHealthBar | improving eating habits and physical activity, | RCT (A pragmatic, parallel-group, 2-arm) | Primary Outcome:
| Participants filled out self-reported questionnaires. |
| Staite et al., 2020 [47] | Prediabetes (HbA1c from 5.7–6.4%) Age: 18–65 years BMI: ≥25 kg/m² (≥23 kg/m² if of Asian ethnicity) Sex: Male and Female Notes: being ambulatory | Randomized Participants: 200 Analyzed Participants: 156 Completed Participants: 156 | 12 month London, United Kingdom. | “Tribrid” Mobile phone Apps based & Web-based & Text Messages based: the wristband and the associated study-specific smartphone app (Buddi wristband) | to support participants in forming healthy intentions, encourage self-monitoring of lifestyle behaviors, and promoting social support | RCT (two-arm, parallel, single-blind) | Primary outcome:
| Using a stadiometer, weight was measured in light clothing, without shoes, to 0.01 kg, and height was measured to 0.1 cm (Class 3 Tanita SC240). BMI (kg/m2) was calculated based on weight and height measurements. Using a non-extensible steel tape against the bare abdomen, the waist circumference (cm) was measured horizontally halfway between the lowest rib and the upper prominence of the pelvis. The waist-to-hip ratio was also calculated by measuring hip circumference. Diastolic and systolic blood pressure (BP), as well as resting heart rate, were measured using digital Omron BP monitors (Omron M7) and standardized procedures for the average of two readings taken one minute apart while seated. |
| Francis et al., 2021 [48] | Prediabetes (HbA1c from 5.7–6.4%) And ≥25 kg/m2 Or Person with ≥30 kg/m2 Only Age: >18 years old BMI: ≥25 kg/m2 Sex: Male and Female | Randomized Participants: 430 Analyzed Participants: 388 Completed Participants: 388 | 6 months Iowa City, IA, USA | Mobile phone apps based: MapTrek-Plus Fitbit Devices | To promotes walking | RCT (two-arm, parallel) | Primary outcome:
| The Fitbit Zip activity monitor objectively measures the number of daily steps. |
| Hamdan et al., 2021 [49] | Prediabetes (HbA1c from 5.6–6.9%) Age: 18–60 years BMI: ≥25 kg/m2 Sex: Female Notes: active users of android or IOS-based | Cluster Randomized: 3 primary care Randomized Participants:110 Analyzed Participants: 110 Completed Participants: 483 | 6 months Riyadh, SA | Mobile phone apps based: Al-Nahdi Mobile App And Social Media | Lifestyle modifications emphasizing the importance of weight loss, healthy diet and physical activity. | RCT (multicenter, 3-arm cluster randomized, Multi-intervention) | Primary outcome:
| Anthropometric measurements were taken at baseline and after 6 months in all three arms of the study. Height (to the nearest cm) and weight (to the nearest 100 g) were measured in light clothing without shoes on calibrated scales. Waist circumference (cm) was measured at the umbilical level without clothing after exhaling in a relaxed standing position. The traditional mercurial sphygmomanometer was used to measure blood pressure (mmHg) after a sufficient rest at each visit, and the average was recorded. Body mass index (BMI) is calculated by dividing weight in kg by height in meters squared (kg/m2). All measurements were taken by trained and licensed nurses and dietitians. |
| Summers et al., 2021 [58] | Prediabetes (HbA1c from 5.6–6.9%) Age: ≥18 years BMI: Not reported Sex: Male and Female Notes: Diabetes and prediabetes | Eligibility Participant: 27 Analyzed Participants: 27 Completed Participants: 21 | 12 months Norwood Surgery in Southport, United Kingdom. | Mobile phone apps based: The Low Carb Program App | Educates and supports sustainable dietary changes focused on carbohydrate restriction | Single-Arm Prospective Study | Primary outcome:
| not reported in detail |
| Khunti et al., 2021 [50] | Prediabetes (HbA1c from 6–6.4% within the last 5 years.) or Impaired Fasting Glucose (FG 100–125 mg/dL) Or Impaired glucose tolerance (OGTT: 140–199 mg/dL) Age: 40–74 years, or 25–74 years if they were South Asian BMI: Not Reported Sex: Male and Female | Randomized Participants: 1366 Analyzed Participants: 1366 Completed Participants: 986 | 48 month Leicester, United Kingdom. | Mobile phone apps based: an integrated mobile health | to support the maintenance of behavior change within Walking Away | RCT (three-arm, parallel-group, pragmatic, superiority) | Primary outcome:
| Estimated conversion rate at the lower level reported for traditionally defined prediabetes Height, body weight, body fat percentage, and waist circumference were all measured to the nearest 0.5 cm, 0.1 kg, 0.5%, and 0.1 cm, respectively. The waist circumference was measured with a soft tape measure halfway between the lowest rib and the iliac crest. When the participant was seated, the arterial blood pressure was taken from the right arm. Venous sampling was used to assess standard biomedical outcomes such as HbA1c, a lipid profile (triglycerides, HDL, LDL, and total cholesterol), urea and electrolytes (sodium, potassium, urea, and creatinine), and liver function tests (albumin, total bilirubin, alkaline phosphatase, and alanine transaminase). |
| Katula et al., 2022 [51] | Prediabetes (HbA1c from 5.7–6.4%) Age: ≥19 years BMI: ≥25 kg/m2 (≥22 kg/m2 if participant self-identified as Asian) Sex: Male and Female | Randomized Participants: 599 Analyzed Participants: 599 Completed Participants: 483 | 12 months Omaha, Nebraska., USA | Mobile phone apps based: App-Plus Wearable Devices | To support weight loss | RCT (two-rm, parallel single-blind) | Primary outcome:
| All study measures were collected at the University of Nebraska Medical Center in a 4-week assessment window by staff who were blinded to study group assignment at each assessment point (baseline, 4 months, and 12 months). Sociodemographic data and health literacy were only collected at the start of the study. HbA1c levels were determined using nonfasting blood samples. Blood was drawn via venipuncture and processed at the University of Nebraska Medical Center’s central diagnostic testing laboratory for cardiovascular disease (lipid panels) using the boronate affinity analytical technique. Weight was measured in stocking feet on a calibrated medical-grade scale with the participant fasting. |
| Stewart et al., 2022 [59] | Prediabetes (HbA1c from 5.7–6.4%) Age: Not Reported BMI: Not Reported Sex: Male and Female Notes: One method of participant recruitment from primary care manager (PCM) referral | Eligibility Participant: 33 Analyzed Participants: 33 | 12 month Augusta, Georgia, USA | “Hybrid” Mobile phone apps and text message-based: Mobile phone App Plus Wearable Devices (FitBit) And The combination of the daily text messages of DPP content | to support participants in losing weight (5–7%) and being active (150 physical activity minutes/week) | Quasi-experimental (pre/post design) |
| Baseline biometric/survey measures and the electronic medical record Physical activity as self-reported |
| Lim et al., 2022 [52] | Prediabetes (HbA1c from 6–6.4%) or Impaired Fasting Glucose (fasting glucose 100–125 mg/dL) Or Impaired glucose tolerance (oral glucose tolerance test: 140–199 mg/dL) Age: 21–75 years BMI: ≥23 kg/m2 Sex: Male and Female | Participant Eligible: 217 Randomized Participants: 148 Analyzed Participants: 148 Completed Participants: 140 | 6 month Singapore | Mobile phone apps based: the nBuddy Diabetes app | To empower individuals through prompts and cues and achieve clinically meaningful weight loss of >5% | RCT (multicenter concurrent parallel RCTs) | Primary outcome:
Secondary outcome:
| Body weight was measured in the clinic by research staff using a standard digital weighing scale (Omron HN-289, Japan) after an overnight fast, with participants dressed lightly and without shoes. To calculate BMI, height was measured without shoes to the nearest centimeter. Venous blood samples were collected after 8–12 h of overnight fasting and processed at CAP-accredited laboratories (National University Hospital Department of Laboratory Medicine or National Healthcare Group Diagnostics). Plasma glucose was determined using a photometric assay using the hexokinase method, and HbA1c was measured using high-performance liquid chromatography. An enzymatic colorimetric assay was used to determine serum lipids and creatinine levels. Self-reported questionnaires were used to collect participants’ physical activity levels in minutes per week at baseline, 3 months, and 6 months. At the baseline, 3-, and 6-month visits, dietary intake was collected using a 2-day food diary and analyzed using the nBuddy Dashboard’s nutrient analysis platform, which includes over 14,000 food items and incorporates the Singapore energy and nutrient composition of food, Malaysian Food Composition, and USDA food databases, as well as nutritional information from food packaging and nutrient analysis of recipes. |
| Sevilla et al., 2022 [60] | Prediabetes (HbA1c from 6–6.4%) or Impaired Fasting Glucose (FG 100–125 mg/dL) Or Impaired glucose tolerance (OGTT: 140–199 mg/dL) Age: 18–65 years BMI: ≥20–40 kg/m2 Sex: Male and Female Notes: Some participants were randomly prescribed 750 mg extended release metformin every 12 h to evaluate the “medication” module of the web platform | Eligibility Participant: 122 Randomized Participants: 77 Analyzed Participants: 77 Completed Participants: 77 | 3 month Mexico City, Mexico | Web-based: Vida Sana | Lifestyle modification counseling with the goal of reaching a weight loss of >3%. | Prospective Interventional Study |
| Dual-energy X-ray absorptiometry is used to determine body composition. Waist and hip circumferences (to the nearest 0.5 cm) were measured at the midpoint between the lower ribs and the iliac crest and at the level of the trochanter major, respectively. Participants who met the inclusion criteria were invited back the following week for an intervention visit. Using colorimetric enzymatic methods, measurements from the oral glucose tolerance test included glucose levels, insulin levels, and lipid profiles (Unicel DxC 600). Beckman Coulter Synchron Clinical System. A chemiluminescence assay was used to measure insulin levels (Access 2, Beckman Coulter). HbA1c was measured using a Variant II Turbo system (BIORAD) and a 4-mL peripheral blood sample was drawn via venipuncture using the standardized technique. Diet and physical activity questionnaires were administered. |
| Moravcova et al., 2022 [53] | Prediabetes (HbA1c from 6–6.4%) or Impaired Fasting Glucose (FG 100–125 mg/dL) Or Impaired glucose tolerance (OGTT: 140–199 mg/dL) Or Insulin resistance (IR) (HOMA-IR > 2.7) Age: 18–60 years BMI: ≥30 kg/m2 Sex: Male and Female Notes: participant included diabetes | Randomized Participants: 100 Analyzed Participants: 78 (3 months) 51 (6 months) Completed Participants: 78 (3 months) 51 (6 months) | 6 month Mexico City, Mexico | Mobile phone apps based: Vitadio application | to provide individualized support in lifestyle modification and self-management | RCT (prospective, double-armed) | primary outcome:
only the 3-month laboratory measurement is evaluated in this paper. The 6-month attrition rate was higher dropout were associated with the COVID-19 pandemic. | The study procedure includes four visits: at baseline, three months later, six months later, and twelve months later, with anthropometric and laboratory examinations performed at each visit. Blood samples were collected after a 12- to 14-h fast. A glucose hexokinase method was used to measure glucose. An enzymatic colorimetric test was used to examine lipids. A two-step sandwich enzyme immunoassay using monoclonal antibodies was used to measure serum insulin. Matthews’ formula was used to calculate HOMA-IR. Body composition was determined using bioelectrical impedance analysis with the InBody 370 and 15 impedance measurements at 5 body segments, as well as a tetrapolar 8-point tactile electrode system. |
| Kondo et al., 2022 [54] | Prediabetes Impaired Fasting Glucose (FG: 100–125 mg/dL) Age: 40–75 years BMI: ≥25 kg/m2 Sex: Male and Female Notes: participant has metabolic syndrome | Randomized Participants: 122 Analyzed Participants: 75 Completed Participants: 74 | 3 months Tokyo, Japan. | Mobile phone apps based: DialBeticsLite | Daily recording of several physical parameters, in addition to tracking lifestyle behavior, that is, diet and exercise | RCT (open-label, 2-arm, parallel-design | Primary Outcome:
| VFA was calculated by distinguishing visceral fat from abdominal subcutaneous fat using current flow from two different routes (DU-ALSCAN, HDS-2000, Fukuda Colin). The HDS-2000 underestimates VFA when compared to computed tomography scans, but the correlation was very strong (r = 0.89). Because of its simplicity and noninvasiveness, the HDS-2000 can be a good option for evaluating VFA. To avoid variation in measurement procedures across raters, the VFA of all participants was measured by the same individual with sufficient experience. The person was able to see again after the group intervened. Secondary outcomes included changes in physical and metabolic parameters from baseline to the 3-month follow-up. Physical parameters included BW, WC, BMI, and BP. Blood tests were used to determine metabolic parameters such as cholesterol, triglyceride, fasting plasma glucose, and HbA1c levels. |
| Results | Chen et al., 2014 [55] | Fischer et al., 2019 [57] | Sevilla et al., 2022 [60] | Sharit et al., 2018 [56] | Stewart et al., 2022 [59] | Summers et al., 2021 [58] | Bender et al., 2019 [40] | Block et al., 2015 [37] | Fischer et al., 2016 [39] | Francis et al., 2021 [48] | Fukuoka et al., 2015 [38] | Griauzde et al., 2019 [41] | Hamdan et al., 2021 [49] | Katula et al., 2022 [51] | Khunti et al., 2021 [50] | Kondo et al., 2022 [54] | Lim et al., 2022 [52] | Mcleod et al., 2020 [44] | Moravcova et al., 2022 [53] | Muralidharan et al., 2020 [45] | Nandhita et al., 2020 [43] | Ramachandran et al., 2013 [36] | Ramos et al., 2020 [42] | Staite et al., 2020 [47] | Xu et al., 2020 [46] | ||
| Type of Trial | Non-Randomized Intervention Trial | Randomized Trial | |||||||||||||||||||||||||
| Number of Samples Included | <100 participant | 77 | 38 | 33 | 27 | 67 | 61 | 69 | 90 | ||||||||||||||||||
| 100–500 participant | 253 | 340 | 163 | 430 | 253 | 122 | 148 | 225 | 100 | 202 | 208 | ||||||||||||||||
| 501–1000 participant | 599 | 833 | 537 | ||||||||||||||||||||||||
| >1000 participant | 1518 | 1366 | 2062 | ||||||||||||||||||||||||
| SEX | Both | Both | Both | Both | Both | Both | Both | Both | Both | Both | Both | Both | Female | Both | Both | Both | Both | Both | Both | Both | Both | Male | Both | Both | Both | ||
| Mean AGE (years) ** | Range: 50–70 | IG: 45.5 (12.2); CG: 48.4 (14.6) | IG: 48 ± 12.0; CG: 48.4 ± 10.8 | 57.7 ± 7.7 | 44 ± 8.5 | 52.42 ± 13.43 | IG: 42.1 ± 12.2; CG: 41.3 ± 12.1 | 55 ± 8.9 range: 31–70 | IG: 47.7 ± 12.4; CG: 45.2 ± 10.6 | IG: 46.9 ± 13.2; CG: 45.8 ± 13.8 | 55.2 ± 9.0 | IG: 52.1 ± 12.0; IG- plus 51.6 ± 11.1; CG: 51.3 ± 11.0 | IG: 43.7 8.1 CG positive: 42.9–12.2: CG negative: 50.9–7.1 | IG: 55.3 ± 12.9; CG: 55.6 ± 12.6 | IG: 59.3 ± 9.1; CG positive: 59.4 ± 9.4; CG negative: 59.4 ± 8.8 | IG: 49.3 ± 6.1; CG: 48.5 (5.3) | IG: 51.9 ± 8.7; CG: 54.3 (9.9) | IG: 61.8 ± 9.5; CG: 62.4 ± 8.7 | IG: 43.3 ± 10.5; CG: 43.3 ± 8.4 | IG: 37.8 ± 9.2; CG: 37.8 ± 9.6 | CG: 52.0 ± 10.2; IG: 52.1 ± 10.3 | IG: 46.1 ± 4.6; CG: 45.9 ± 4.8 | IG: 55.7; CG: 57.5 | IG: 51.76 ± 7.68; CG: 52.78 ± 8.20 | IG: 46.0; CG: 47.5 | ||
| Mean AGE (years) ** | MIDDLE AGE (40–60) | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||
| ELDERLY (>60) | √ | √ | √ | ||||||||||||||||||||||||
| Mean BMI (kg/m2) ** | IG: 24.80 ± 3.21; CG: 23.36 ± 2.95 | Not Reported | IG: 30.8 ± 16.5 CG: 30.6 ± 4.2 | 33.6 ± 3.9 | Pre:38.8 ± 1.8; Post: 37.6 ± 1.9 | Not Reported | IG30.5(±3.9) CG 30.5(±4.9) | 31.1 ± 4.4 | Not Reported | IG: 36.4 ± 6.2; CG: 37.0 ± 6.8 | 33.3 ± 6.0 | IG only: 33.0 ± 10.4; IG plus 30.7 ± 9.3; CG: 33.4 ± 7.8 | IG: 30 ± 5.1; CG Positive: 34.8 ± 9.0; CG Negative: 31.6 ± 5.8 | IG: 35.8 ± 6.1; CG: 35.8 ± 6.1 | IG: 28.4 CG Positive: 28.2; CG negative: 28.5 | IG: 27.4 3.0Con: 26.6 (2.2) | IG: 29.8 ± 4.2; CG: 29.8 ± 3.9 | IG: 33.5 ± 7.7; CG: 33.1 ± 7.1 | IG: 40.5 ± 7.1 CG: 39.7 ± 5.1 | IG: 29.4 ± 3.8; CG: 29.3 ± 4.2 | IG: 28.7 ± 4.7CG: 28.9 ± 4.8 | IG 25.8 ± 3.0; CG: 25.8 ± 3.3 | IG: 31.25 ± 6.43; CG: 30.94 ± 7.23 | Not Reported | IG: 25.3; CG: 24.7 | ||
| Diagnostic Criteria | HbA1c | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||
| HbA1c Only | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||||||||
| OGGT | √ | √ | √ | √ | √ | √ | √ | ||||||||||||||||||||
| OGGT Only | √ | ||||||||||||||||||||||||||
| FG | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||||||||
| FG Only | √ | √ | √ | ||||||||||||||||||||||||
| Combination | √ | √ | √ | √ | √ | √ | √ | * | |||||||||||||||||||
| Duration of study | <6 month | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||||||||||||
| 6–12 month | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||||
| 13–24 month | |||||||||||||||||||||||||||
| >24 month | √ | √ | √ | ||||||||||||||||||||||||
| Type of mobile health | Text Message-Based | √ | √ | √ | √ | √ | √ | ||||||||||||||||||||
| Web Based | √ | √ | √ | √ | √ | ||||||||||||||||||||||
| Mobile Phone Apps | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||
| Combination (Hybrid or Tribrid) | √ | √ | √ | ||||||||||||||||||||||||
| Wearable Devices | √ | √ | √ | √ | √ | √ | |||||||||||||||||||||
| Outcome Measures | Incidence | √ | √ | √ | |||||||||||||||||||||||
| Anthropometric Measures | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||
| Laboratory Parameters | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||
| Physical Activity | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||||||
| Dietary Behavior | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||||||||||
 : Non-Randomized Interventional Trial.
: Non-Randomized Interventional Trial.  : Randomized Trial. *: Diagnosed by American Diabetes Association (ADA) screening tool (score of ≥ 5 or). **: Age (years) by mean ± SD or range age of participants. IG: Intervention Group; CG: Control Group.
: Randomized Trial. *: Diagnosed by American Diabetes Association (ADA) screening tool (score of ≥ 5 or). **: Age (years) by mean ± SD or range age of participants. IG: Intervention Group; CG: Control Group.| METHODOLOGICAL FEATURE | ITEM | ANSWER | SCORE |
|---|---|---|---|
| Randomization | Was the study described as randomized? | Yes | 1 |
| No | 0 | ||
| Was the method used to generate the sequence of randomization described and appropriate? | Yes | 1 | |
| No | 0 | ||
| Described and inappropriate | −1 | ||
| Blinding | Was the study described as double-blind? | Yes | 1 |
| No | 0 | ||
| Was the method of double blinding described and appropriate? | Yes | 1 | |
| No | 0 | ||
| Described and inappropriate | −1 | ||
| withdrawals and dropouts | Was there a description of withdrawals and dropouts? | Yes | 1 |
| No | 0 |
| Author, Year | Ramachandran et al., 2013 [36] | Chen et al., 2014 [55] | Block et al., 2015 [37] | Fukuoka et al., 2015 [38] | Fischer et al., 2016 [39] | Bender et al., 2019 [40] | Sharit et al., 2018 [56] | Griauzde et al., 2019 [41] | Fischer et al., 2019 [57] | Ramos et al., 2020 [42] | Nandhita et al., 2020 [43] | Mcleod et al., 2020 [44] | Muralidharan et al., 2020 [45] | Xu et al., 2020 [46] | Staite et al., 2020 [47] | Francis et al., 2021 [48] | Hamdan et al., 2021 [49] | Summers et al., 2021 [58] | Khunti et al., 2021 [50] | Katula et al., 2022 [51] | Stewart et al., 2022 [59] | Lim et al., 2022 [52] | Sevilla et al., 2022 [60] | Moravcova et al., 2022 [53] | Kondo et al., 2022 [54] |
| Randomization | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 |
| 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | |
| Blinding | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 |
| 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Withdrawals and Dropouts | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Total Score | 3 | 1 | 4 | 4 | 3 | 4 | 1 | 3 | 1 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 1 | 4 | 4 | 1 | 4 | 1 | 4 | 4 |
3.4. Mobile Health Interventions
3.5. Outcomes Reported
3.5.1. Incidence of T2DM
3.5.2. Anthropometric Measures
| Results of Intervention Outcome | Chen et al., 2014 [55] | Fischer et al., 2019 [57] | Sevilla et al., 2022 [60] | Sharit et al., 2018 [56] | Stewart et al., 2022 [59] | Summers et al., 2021 [58] | Bender et al., 2019 [40] | Block et al., 2015 [37] | Fischer et al., 2016 [39] | Francis et al., 2021 [48] | Fukuoka et al., 2015 [38] | Griauzde et al., 2019 [41] | Hamdan et al., 2021 [49] | Katula et al., 2022 [51] | Khunti et al., 2021 [50] | Kondo et al., 2022 [54] | Lim et al., 2022 [52] | Mcleod et al., 2020 [44] | Moravcova et al., 2022 [53] | Muralidharan et al., 2020 [45] | Nandhita et al., 2020 [43] | Ramachandran et al., 2013 [36] | Ramos et al., 2020 [42] | Staite et al., 2020 [47] | Xu et al., 2020 [46] | |
| Type of Trial | Non-Randomized Interventional Study | Randomized Trial | ||||||||||||||||||||||||
| Incidence of type 2 DM | 0 | 0 | 1 | |||||||||||||||||||||||
| anthropometry measures | Weight Change | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | |||||
| Achieving ≥ 3% Weight loss | 0 | 1 | ||||||||||||||||||||||||
| Achieving ≥ 5% | 1 | 0 | 1 | 1 | ||||||||||||||||||||||
| BMI Change | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | |||||||||
| Waist circumference | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | |||||||||||
| Physical Activity | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | |||||||||||||||
| Dietary Behavior | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | ||||||||||||||||||
| Laboratory measures | HbA1C Reduction | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | |||||||||
| Blood Glucose Level Reduction | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | ||||||||||||||||||
| Fasting Plasma Glucose | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | ||||||||||||||||||
| OGGT | 1 | 0 | 0 | |||||||||||||||||||||||
| Blood Lipid Level Reduction | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||||||||||||||||
 : Not observed in the study.
: Not observed in the study.  : Results were statistically significant.
: Results were statistically significant.  : Results were not statistically significant.
: Results were not statistically significant. 3.5.3. Physical Activity
3.5.4. Dietary Behaviors
3.5.5. Laboratory Measures
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Introduction: Standards of medical care in diabetes-2018. Diabetes Care 2018, 41, S1–S2. [CrossRef] [Green Version]
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Richter, B.; Hemmingsen, B.; Metzendorf, M.-I.; Takwoingi, Y. Development of type 2 diabetes mellitus in people with intermediate hyperglycaemia. Cochrane Database Syst. Rev. 2018, 10, CD012661. [Google Scholar] [CrossRef] [PubMed]
- Rooney, M.R.; Rawlings, A.M.; Pankow, J.S.; Echouffo Tcheugui, J.B.; Coresh, J.; Sharrett, A.R.; Selvin, E. Risk of Progression to Diabetes Among Older Adults With Prediabetes. JAMA Intern. Med. 2021, 181, 511–519. [Google Scholar] [CrossRef]
- Anothaisintawee, T.; Sansanayudh, N.; Thamakaison, S.; Lertrattananon, D.; Thakkinstian, A. Neck Circumference as an Anthropometric Indicator of Central Obesity in Patients with Prediabetes: A Cross-Sectional Study. BioMed Res. Int. 2019, 2019, 4808541. [Google Scholar] [CrossRef] [Green Version]
- Grundy, S.M. Pre-diabetes, metabolic syndrome, and cardiovascular risk. J. Am. Coll. Cardiol. 2012, 59, 635–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmingsen, B.; Sonne, D.P.; Metzendorf, M.-I.; Richter, B. Insulin secretagogues for prevention or delay of type 2 diabetes mellitus and its associated complications in persons at increased risk for the development of type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2016, 10, CD012151. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Guo, X.; Zhang, Z. The efficacy of mobile phone apps for lifestyle modification in diabetes: Systematic review and meta-analysis. JMIR mHealth uHealth 2019, 7, e12297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Center, P.R. Older Adults and Technology Use. PEW Research Center. 2014. Available online: http://www.pewinternet.org/2014/04/03/older-adults-andtechnology-%0Ause/%0A (accessed on 25 September 2022).
- Carroll, J.K.; Moorhead, A.; Bond, R.; LeBlanc, W.G.; Petrella, R.J.; Fiscella, K. Who uses mobile phone health apps and does use matter? A secondary data analytics approach. J. Med. Internet Res. 2017, 19, e125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, C.; Carter, B.; Hewitt, J.; Francisa, T.; Mayor, S. Do mobile phone applications improve glycemic control (HbA1c) in the self-management of diabetes? A systematic review, meta-analysis, and GRADE of 14 randomized trials. Diabetes Care 2016, 39, 2089–2095. [Google Scholar] [CrossRef]
- Ang, S.M.; Chen, J.; Liew, J.H.; Johal, J.; Dan, Y.Y.; Allman-Farinelli, M.; Lim, S.L. Efficacy of interventions that incorporate mobile apps in facilitating weight loss and health behavior change in the asian population: Systematic review and meta-analysis. J. Med. Internet Res. 2021, 23, e28185. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Wang, Q.; Yang, X.; Cao, J.; Chen, J.; Mo, X.; Huang, J.; Wang, L.; Gu, D. Effect of mobile phone intervention for diabetes on glycaemic control: A meta-analysis. Diabet. Med. 2011, 28, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Fakih El Khoury, C.; Karavetian, M.; Halfens, R.J.G.; Crutzen, R.; Khoja, L.; Schols, J.M.G.A. The Effects of Dietary Mobile Apps on Nutritional Outcomes in Adults with Chronic Diseases: A Systematic Review and Meta-Analysis. J. Acad. Nutr. Diet. 2019, 119, 626–651. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Min, J.; Khuri, J.; Xue, H.; Xie, B.; Kaminsky, L.A.; Cheskin, L.J. Effectiveness of Mobile Health Interventions on Diabetes and Obesity Treatment and Management: Systematic Review of Systematic Reviews. JMIR mHealth uHealth 2020, 8, e15400. [Google Scholar] [CrossRef] [PubMed]
- Kitsiou, S.; Paré, G.; Jaana, M.; Gerber, B. Effectiveness of mHealth interventions for patients with diabetes: An overview of systematic reviews. PLoS ONE 2017, 12, e0173160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villinger, K.; Wahl, D.R.; Boeing, H.; Schupp, H.T.; Renner, B. The effectiveness of app-based mobile interventions on nutrition behaviours and nutrition-related health outcomes: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 1465–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dounavi, K.; Tsoumani, O. Mobile Health Applications in Weight Management: A Systematic Literature Review. Am. J. Prev. Med. 2019, 56, 894–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Shu, W.; Du, J.; Du, M.; Wang, P.; Xue, M.; Zheng, H.; Jiang, Y.; Yin, S.; Liang, D.; et al. Mobile health in the management of type 1 diabetes: A systematic review and meta-analysis. BMC Endocr. Disord. 2019, 19, 21. [Google Scholar] [CrossRef]
- Dobson, R.; Whittaker, R.; Pfaeffli Dale, L.; Maddison, R. The effectiveness of text message-based self-management interventions for poorly-controlled diabetes: A systematic review. Digit. Health 2017, 3, 2055207617740315. [Google Scholar] [CrossRef]
- Marcolino, M.S.; Oliveira, J.A.Q.; D’Agostino, M.; Ribeiro, A.L.; Alkmim, M.B.M.; Novillo-Ortiz, D. The Impact of mHealth Interventions: Systematic Review of Systematic Reviews. JMIR mHealth uHealth 2018, 6, e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotter, A.P.; Durant, N.; Agne, A.A.; Cherrington, A.L. Internet interventions to support lifestyle modification for diabetes management: A systematic review of the evidence. J. Diabetes Complicat. 2014, 28, 243–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorig, K.; Ritter, P.L.; Laurent, D.D.; Plant, K.; Green, M.; Jernigan, V.B.B.; Case, S. Online diabetes self-management program: A randomized study. Diabetes Care 2010, 33, 1275–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, C.R.; Mehari, K.S.; McIntyre, L.G.; Janney, A.W.; Fortlage, L.A.; Sen, A.; Strecher, V.J.; Piette, J.D. A randomized trial comparing structured and lifestyle goals in an internet-mediated walking program for people with type 2 diabetes. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, T.; Spruijt-Metz, D.; Wen, C.K.F.; Hingle, M.D. Prevention and treatment of pediatric obesity using mobile and wireless technologies: A systematic review. Pediatr. Obes. 2015, 10, 403–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron, J.; McBain, H.; Newman, S. The impact of mobile monitoring technologies on glycosylated hemoglobin in diabetes: A systematic review. J. Diabetes Sci. Technol. 2012, 6, 1185–1196. [Google Scholar] [CrossRef] [Green Version]
- Bloomfield, G.S.; Vedanthan, R.; Vasudevan, L.; Kithei, A.; Were, M.; Velazquez, E.J. Mobile health for non-communicable diseases in Sub-Saharan Africa: A systematic review of the literature and strategic framework for research. Global. Health 2014, 10, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barengo, N.C.; Diaz Valencia, P.A.; Apolina, L.M.; Estrada Cruz, N.A.; Fernández Garate, J.E.; Correa González, R.A.; Cinco Gonzalez, C.A.; Gómez Rodriguez, J.A.; González, N.C. Mobile Health Technology in the Primary Prevention of Type 2 Diabetes: A Systematic Review. Curr. Diabetes Rep. 2022, 22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Van Rhoon, L.; Byrne, M.; Morrissey, E.; Murphy, J.; McSharry, J. A systematic review of the behaviour change techniques and digital features in technology-driven type 2 diabetes prevention interventions. Digit. Health 2020, 6, 2055207620914427. [Google Scholar] [CrossRef]
- Elavsky, S.; Knapova, L.; Klocek, A.; Smahel, D. Mobile health interventions for physical activity, sedentary behavior, and sleep in adults aged 50 years and older: A systematic literature review. J. Aging Phys. Act. 2019, 27, 565–593. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Macaskill, P.; Gatsonis, C.; Deeks, J.; Harbord, R.; Takwoingi, Y. Chapter 10 Analysing and Presenting Results. In Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy; 2010; pp. 1–61. Available online: http://srdta.cochrane.org/handbook-dta-reviews (accessed on 25 September 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA 2009 Flow Diagram. Prism. Statement 2009, 6, 1000097. [Google Scholar]
- Ramachandran, A.; Snehalatha, C.; Ram, J.; Selvam, S.; Simon, M.; Nanditha, A.; Shetty, A.S.; Godsland, I.F.; Chaturvedi, N.; Majeed, A.; et al. Effectiveness of mobile phone messaging in prevention of type 2 diabetes by lifestyle modification in men in India: A prospective, parallel-group, randomised controlled trial. Lancet Diabetes Endocrinol. 2013, 1, 191–198. [Google Scholar] [CrossRef]
- Block, G.; Azar, K.M.J.; Romanelli, R.J.; Block, T.J.; Hopkins, D.; Carpenter, H.A.; Dolginsky, M.S.; Hudes, M.L.; Palaniappan, L.P.; Block, C.H. Diabetes prevention and weight loss with a fully automated behavioral intervention by email, web, and mobile phone: A randomized controlled trial among persons with prediabetes. J. Med. Internet Res. 2015, 17, e240. [Google Scholar] [CrossRef]
- Xu, Z.; Geng, J.; Zhang, S.; Zhang, K.; Yang, L.; Li, J.; Li, J. A Mobile-Based Intervention for Dietary Behavior and Physical Activity Change in Individuals at High Risk for Type 2 Diabetes Mellitus: Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e19869. [Google Scholar] [CrossRef]
- Staite, E.; Bayley, A.; Al-Ozairi, E.; Stewart, K.; Hopkins, D.; Rundle, J.; Basudev, N.; Mohamedali, Z.; Ismail, K. A Wearable Technology Delivering a Web-Based Diabetes Prevention Program to People at High Risk of Type 2 Diabetes: Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e15448. [Google Scholar] [CrossRef]
- Francis, S.L.; Simmering, J.E.; Polgreen, L.A.; Evans, N.J.; Hosteng, K.R.; Carr, L.J.; Cremer, J.F.; Coe, S.; Cavanaugh, J.E.; Segre, A.M.; et al. Gamifying accelerometer use increases physical activity levels of individuals pre-disposed to type II diabetes. Prev. Med. Rep. 2021, 23, 101426. [Google Scholar] [CrossRef]
- Al-Hamdan, R.; Avery, A.; Al-Disi, D.; Sabico, S.; Al-Daghri, N.M.; McCullough, F. Efficacy of lifestyle intervention program for Arab women with prediabetes using social media as an alternative platform of delivery. J. Diabetes Investig. 2021, 12, 1872–1880. [Google Scholar] [CrossRef]
- Khunti, K.; Griffin, S.; Brennan, A.; Dallosso, H.; Davies, M.; Eborall, H.; Edwardson, C.; Gray, L.; Hardeman, W.; Heathcote, L.; et al. Behavioural interventions to promote physical activity in a multiethnic population at high risk of diabetes: PROPELS three-arm RCT. Health Technol. Assess. 2021, 25, 1–190. [Google Scholar] [CrossRef]
- Katula, J.A.; Dressler, E.V.; Kittel, C.A.; Harvin, L.N.; Almeida, F.A.; Wilson, K.E.; Michaud, T.L.; Porter, G.C.; Brito, F.A.; Goessl, C.L.; et al. Effects of a Digital Diabetes Prevention Program: An RCT. Am. J. Prev. Med. 2022, 62, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.L.; Ong, K.W.; Johal, J.; Han, C.Y.; Yap, Q.V.; Chan, Y.H.; Zhang, Z.P.; Chandra, C.C.; Thiagarajah, A.G.; Khoo, C.M. A Smartphone App-Based Lifestyle Change Program for Prediabetes (D’LITE Study) in a Multiethnic Asian Population: A Randomized Controlled Trial. Front. Nutr. 2021, 8, 780567. [Google Scholar] [CrossRef] [PubMed]
- Moravcová, K.; Karbanová, M.; Bretschneider, M.P.; Sovová, M.; Ožana, J.; Sovová, E. Comparing Digital Therapeutic Intervention with an Intensive Obesity Management Program: Randomized Controlled Trial. Nutrients 2022, 14, 2005. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.; Okitsu, T.; Waki, K.; Yamauchi, T.; Nangaku, M.; Ohe, K. Effect of Information and Communication Technology-Based Self-management System DialBeticsLite on Treating Abdominal Obesity in the Specific Health Guidance in Japan: Randomized Controlled Trial. JMIR Form. Res. 2022, 6, e33852. [Google Scholar] [CrossRef] [PubMed]
- Fukuoka, Y.; Gay, C.L.; Joiner, K.L.; Vittinghoff, E. A Novel Diabetes Prevention Intervention Using a Mobile App: A Randomized Controlled Trial with Overweight Adults at Risk. Am. J. Prev. Med. 2015, 49, 223–237. [Google Scholar] [CrossRef] [Green Version]
- Fischer, H.H.; Fischer, I.P.; Pereira, R.I.; Furniss, A.L.; Rozwadowski, J.M.; Moore, S.L.; Durfee, M.J.; Raghunath, S.G.; Tsai, A.G.; Havranek, E.P. Text Message Support for Weight Loss in Patients with Prediabetes: A Randomized Clinical Trial. Diabetes Care 2016, 39, 1364–1370. [Google Scholar] [CrossRef] [Green Version]
- Bender, M.S.; Cooper, B.A.; Flowers, E.; Ma, R.; Arai, S. Filipinos Fit and Trim—A feasible and efficacious DPP-based intervention trial. Contemp. Clin. Trials Commun. 2018, 12, 76–84. [Google Scholar] [CrossRef]
- Griauzde, D.; Kullgren, J.T.; Liestenfeltz, B.; Ansari, T.; Johnson, E.H.; Fedewa, A.; Saslow, L.R.; Richardson, C.; Heisler, M. A Mobile Phone-Based Program to Promote Healthy Behaviors Among Adults with Prediabetes Who Declined Participation in Free Diabetes Prevention Programs: Mixed-Methods Pilot Randomized Controlled Trial. JMIR mHealth uHealth 2019, 7, e11267. [Google Scholar] [CrossRef] [Green Version]
- Toro-Ramos, T.; Michaelides, A.; Anton, M.; Karim, Z.; Kang-Oh, L.; Argyrou, C.; Loukaidou, E.; Charitou, M.M.; Sze, W.; Miller, J.D. Mobile Delivery of the Diabetes Prevention Program in People with Prediabetes: Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e17842. [Google Scholar] [CrossRef]
- Nanditha, A.; Thomson, H.; Susairaj, P.; Srivanichakorn, W.; Oliver, N.; Godsland, I.F.; Majeed, A.; Darzi, A.; Satheesh, K.; Simon, M.; et al. A pragmatic and scalable strategy using mobile technology to promote sustained lifestyle changes to prevent type 2 diabetes in India and the UK: A randomised controlled trial. Diabetologia 2020, 63, 486–496. [Google Scholar] [CrossRef] [Green Version]
- McLeod, M.; Stanley, J.; Signal, V.; Stairmand, J.; Thompson, D.; Henderson, K.; Davies, C.; Krebs, J.; Dowell, A.; Grainger, R.; et al. Impact of a comprehensive digital health programme on HbA1c and weight after 12 months for people with diabetes and prediabetes: A randomised controlled trial. Diabetologia 2020, 63, 2559–2570. [Google Scholar] [CrossRef]
- Muralidharan, S.; Ranjani, H.; Anjana, R.M.; Gupta, Y.; Ambekar, S.; Koppikar, V.; Jagannathan, N.; Jena, S.; Tandon, N.; Allender, S.; et al. Change in cardiometabolic risk factors among Asian Indian adults recruited in a mHealth-based diabetes prevention trial. Digit. Health 2021, 7, 20552076211039030. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Chai, J.; Cheng, J.; Li, K.; Xie, S.; Liang, H.; Shen, X.; Feng, R.; Wang, D. A smart web aid for preventing diabetes in rural China: Preliminary findings and lessons. J. Med. Internet Res. 2014, 16, e98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharit, J.; Idrees, T.; Andrade, A.D.; Anam, R.; Karanam, C.; Valencia, W.; Florez, H.; Ruiz, J.G. Use of an online personal health record’s Track Health function to promote positive lifestyle behaviors in Veterans with prediabetes. J. Health Psychol. 2018, 23, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Fischer, H.H.; Durfee, M.J.; Raghunath, S.G.; Ritchie, N.D. Short message service text message support for weight loss in patients with prediabetes: Pragmatic trial. JMIR Diabetes 2019, 4, e12985. [Google Scholar] [CrossRef] [Green Version]
- Summers, C.; Tobin, S.; Unwin, D. Evaluation of the Low Carb Program Digital Intervention for the Self-Management of Type 2 Diabetes and Prediabetes in an NHS England General Practice: Single-Arm Prospective Study. JMIR Diabetes 2021, 6, e25751. [Google Scholar] [CrossRef]
- Stewart, J.L.; Hatzigeorgiou, C.; Davis, C.L.; Ledford, C.J.W. DPPFit: Developing and Testing a Technology-Based Adaptation of the Diabetes Prevention Program (DPP) to Address Prediabetes in a Primary Care Setting. J. Am. Board Fam. Med. 2022, 35, 548–558. [Google Scholar] [CrossRef]
- Sevilla-Gonzalez, M.D.R.; Bourguet-Ramirez, B.; Lazaro-Carrera, L.S.; Martagon-Rosado, A.J.; Gomez-Velasco, D.V.; Viveros-Ruiz, T.L. Evaluation of a Web Platform to Record Lifestyle Habits in Subjects at Risk of Developing Type 2 Diabetes in a Middle-Income Population: Prospective Interventional Study. JMIR Diabetes 2022, 7, e25105. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Gillies, C.L.; Taub, N.A.; Mostafa, S.A.; Hiles, S.L.; Abrams, K.R.; Davies, M.J. A comparison of cost per case detected of screening strategies for Type 2 diabetes and impaired glucose regulation: Modelling study. Diabetes Res. Clin. Pract. 2012, 97, 505–513. [Google Scholar] [CrossRef]
- Berger, V.W.; Alperson, S.Y. A general framework for the evaluation of clinical trial quality. Rev. Recent Clin. Trials 2009, 4, 79–88. [Google Scholar] [CrossRef] [Green Version]
- Dany, F.; Kusumawardani, N.; Pradono, J.; Kristianto, Y.; Delima, D. Faktor Risiko Prediabetes: Isolated Impaired Fasting Glucose (i-IFG), Isolated Impaired Glucose Tolerance (i-IGT) dan Kombinasi IFG-IGT (Analisis Lanjut Riskesdas 2013). Bul. Penelit. Kesehat. 2017, 45, 113–124. [Google Scholar] [CrossRef]
- Xiao, L.; Yank, V.; Wilson, S.R.; Lavori, P.W.; Ma, J. Two-year weight-loss maintenance in primary care-based Diabetes Prevention Program lifestyle interventions. Nutr. Diabetes 2013, 3, 17–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muralidharan, S.; Ranjani, H.; Anjana, R.; Allender, S.; Mohan, V. Mobile health technology in the prevention and management of Type 2 diabetes. Indian J. Endocrinol. Metab. 2017, 21, 334–340. [Google Scholar] [CrossRef] [Green Version]
- Lee, J. Hype or hope for diabetes mobile health applications? Diabetes Res. Clin. Pract. 2014, 106, 390–392. [Google Scholar] [CrossRef] [PubMed]
- Gossain, V.V.; Aldasouqi, S. The challenge of undiagnosed pre-diabetes, diabetes and associated cardiovascular disease. Int. J. Diabetes Mellit. 2010, 2, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Seo, D.C.; Niu, J. Evaluation of internet-based interventions on waist circumference reduction: A meta-analysis. J. Med. Internet Res. 2015, 17, e181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.K.; Menon, A.; Brashear, M.; Johnson, W.D. Prediabetes: Prevalence, pathogenesis, and recognition of enhanced risk. In Nutritional and Therapeutic Interventions for Diabetes and Metabolic Syndrome, 2nd ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2018; pp. 15–32. ISBN 9780128120194. [Google Scholar]
- Anderson, K.; Burford, O.; Emmerton, L. Mobile health apps to facilitate self-care: A qualitative study of user experiences. PLoS ONE 2016, 11, e0156164. [Google Scholar] [CrossRef] [Green Version]
- Kannisto, K.A.; Koivunen, M.H.; Välimäki, M.A. Use of mobile phone text message reminders in health care services: A narrative literature review. J. Med. Internet Res. 2014, 16, e222. [Google Scholar] [CrossRef] [PubMed]
- Strandbygaard, U.; Thomsen, S.F.; Backer, V. A daily SMS reminder increases adherence to asthma treatment: A three-month follow-up study. Respir. Med. 2010, 104, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Prochaska, J.J.; Coughlin, S.S.; Lyons, E.J. Social media and mobile technology for cancer prevention and treatment. Am. Soc. Clin. Oncol. Educ. Book 2017, 37, 128–137. [Google Scholar] [CrossRef]
- Lupton, D. Apps as Artefacts: Towards a Critical Perspective on Mobile Health and Medical Apps. Societies 2014, 4, 606–622. [Google Scholar] [CrossRef]
- MacPherson, M.; Merry, K.; Locke, S.; Jung, M. Developing Mobile Health Interventions with Implementation in Mind: Application of the Multiphase Optimization Strategy (MOST) Preparation Phase to Diabetes Prevention Programming. JMIR Form. Res. 2022, 6, e36143. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeem, Y.A.; Andriani, R.N.; Nabila, R.; Emelia, D.D.; Lazuardi, L.; Koesnanto, H. The Use of Mobile Health Interventions for Outcomes among Middle-Aged and Elderly Patients with Prediabetes: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 13638. https://doi.org/10.3390/ijerph192013638
Jeem YA, Andriani RN, Nabila R, Emelia DD, Lazuardi L, Koesnanto H. The Use of Mobile Health Interventions for Outcomes among Middle-Aged and Elderly Patients with Prediabetes: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(20):13638. https://doi.org/10.3390/ijerph192013638
Chicago/Turabian StyleJeem, Yaltafit Abror, Russy Novita Andriani, Refa Nabila, Dwi Ditha Emelia, Lutfan Lazuardi, and Hari Koesnanto. 2022. "The Use of Mobile Health Interventions for Outcomes among Middle-Aged and Elderly Patients with Prediabetes: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 20: 13638. https://doi.org/10.3390/ijerph192013638