
The Social Distance Impacts from COVID-19 Pandemic on the Development of Two Orders of a Concurrent Training Programme for Morbidly Obese Patients

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
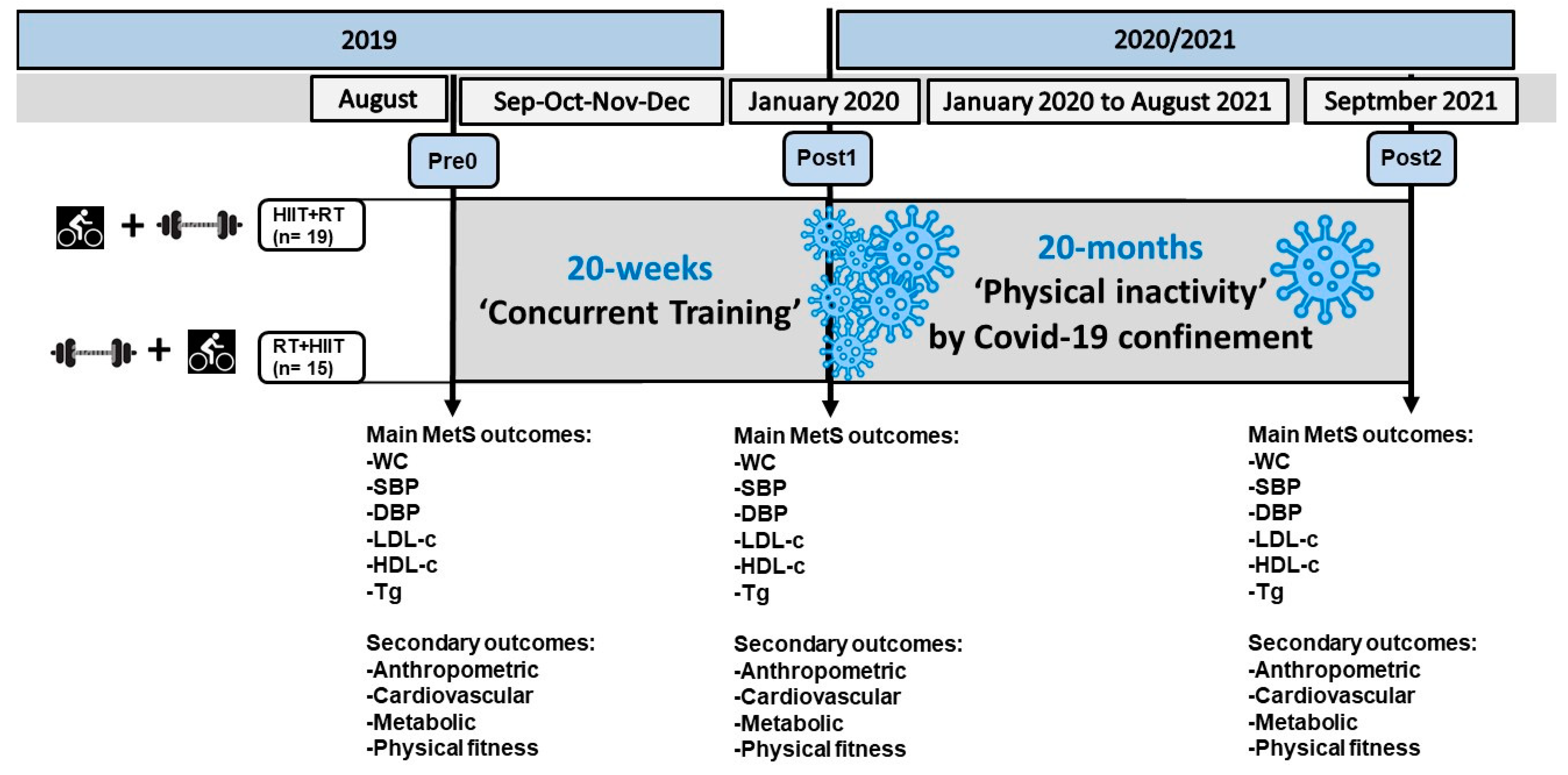
2. Materials and Methods
2.1. Participants
2.2. Metabolic Syndrome Outcomes
2.3. Body Composition and Anthropometric Parameters
2.4. Six-Minute Walking Test
2.5. Handgrip Strength
2.6. Concurrent Training Intervention
2.7. Statistical Analyses
3. Results
3.1. Anthropometry and Body Composition (Secondary Outcomes)
3.2. Training-Induced Effects on Anthropometrics, Body Composition, Cardiovascular, Metabolic, and Physical Fitness (Secondary Outcomes)
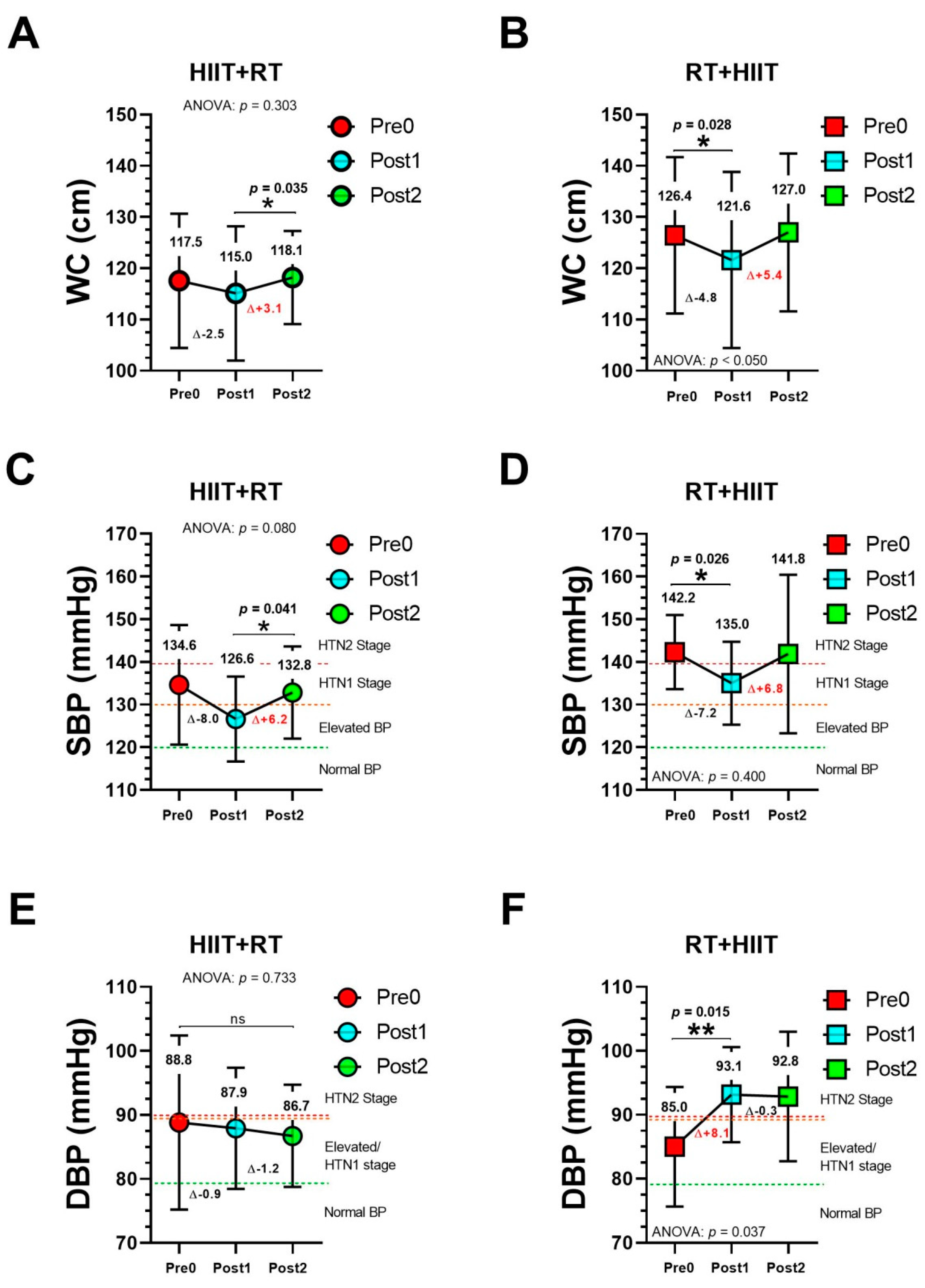
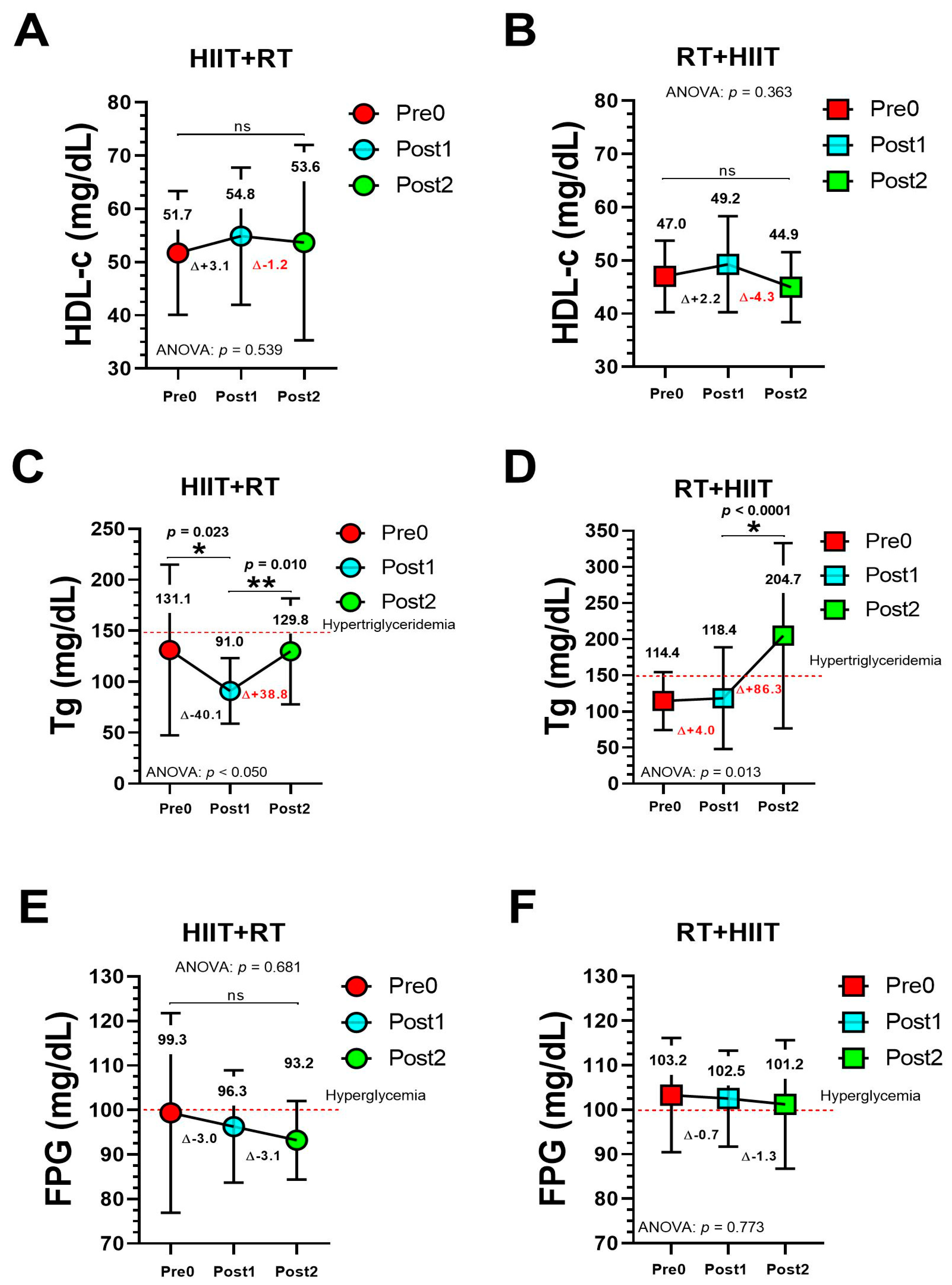
3.3. Training-Induced Effects on Metabolic Syndrome Outcomes (Main Outcomes)
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143. [Google Scholar]
- WHO. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Katzmarzyk, P.T.; Friedenreich, C.; Shiroma, E.J.; Lee, I.-M. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br. J. Sports Med. 2022, 56, 101–106. [Google Scholar] [CrossRef]
- Reyes-Olavarría, D.; Latorre-Román, P.Á.; Guzmán-Guzmán, I.P.; Jerez-Mayorga, D.; Caamaño-Navarrete, F.; Delgado-Floody, P. Positive and negative changes in food habits, physical activity patterns, and weight status during COVID-19 confinement: Associated factors in the Chilean population. Int. J. Environ. Res. Public Health 2020, 17, 5431. [Google Scholar] [CrossRef]
- Caprara, G. Mediterranean-Type Dietary Pattern and Physical Activity: The Winning Combination to Counteract the Rising Burden of Non-Communicable Diseases (NCDs). Nutrients 2021, 13, 429. [Google Scholar] [CrossRef]
- Katsoulis, M.; Pasea, L.; Lai, A.G.; Dobson, R.J.; Denaxas, S.; Hemingway, H.; Banerjee, A. Obesity during the COVID-19 pandemic: Both cause of high risk and potential effect of lockdown? A population-based electronic health record study. Public Health 2021, 191, 41–47. [Google Scholar] [CrossRef]
- Melamed, O.C.; Selby, P.; Taylor, V.H. Mental Health and Obesity During the COVID-19 Pandemic. Curr. Obes. Rep. 2022, 11, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Fernández, P.; González-Santos, J.; Santamaría-Peláez, M.; Soto-Cámara, R.; Sánchez-González, E.; González-Bernal, J.J. Psychological Effects of Home Confinement and Social Distancing Derived from COVID-19 in the General Population—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6528. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Ruíz-Roso, M.B.; de Carvalho Padilha, P.; Matilla-Escalante, D.C.; Brun, P.; Ulloa, N.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Rangel Bousquet Carrilho, T.; de Oliveira Cardoso, L.; et al. Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during COVID-19 Pandemic: An Observational Study. Nutrients 2020, 12, 2289. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, A.V.; Sciomer, S.; Cocchi, C.; Maffei, S.; Gallina, S. Quarantine during COVID-19 outbreak: Changes in diet and physical activity increase the risk of cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1409–1417. [Google Scholar] [CrossRef]
- Joseph, R.P.; Pituch, K.A.; Guest, M.A.; Maxfield, M.; Peckham, A.; Coon, D.W.; Kim, W.; Langer, S.L. Physical activity among predominantly white middle-aged and older US adults during the SARS-CoV-2 pandemic: Results from a national longitudinal survey. Front. Public Health 2021, 9, 291. [Google Scholar] [CrossRef] [PubMed]
- Janssen, M.; Chang, B.P.; Hristov, H.; Pravst, I.; Profeta, A.; Millard, J. Changes in food consumption during the COVID-19 pandemic: Analysis of consumer survey data from the first lockdown period in Denmark, Germany, and Slovenia. Front. Nutr. 2021, 8, 60. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, J.E. Food supply chains during the COVID-19 pandemic. Can. J. Agric. Econ./Rev. Can. D’Agroecon. 2020, 68, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Strotmann, C.; Baur, V.; Börnert, N.; Gerwin, P. Generation and prevention of food waste in the German food service sector in the COVID-19 pandemic—Digital approaches to encounter the pandemic related crisis. Socio-Econ. Plan. Sci. 2021, 82, 101104. [Google Scholar] [CrossRef]
- Chen, L.; Li, J.; Xia, T.; Matthews, T.A.; Tseng, T.-S.; Shi, L.; Zhang, D.; Chen, Z.; Han, X.; Li, Y.; et al. Changes of Exercise, Screen Time, Fast Food Consumption, Alcohol, and Cigarette Smoking during the COVID-19 Pandemic among Adults in the United States. Nutrients 2021, 13, 3359. [Google Scholar] [CrossRef] [PubMed]
- Biamonte, E.; Pegoraro, F.; Carrone, F.; Facchi, I.; Favacchio, G.; Lania, A.G.; Mazziotti, G.; Mirani, M. Weight change and glycemic control in type 2 diabetes patients during COVID-19 pandemic: The lockdown effect. Endocrine 2021, 72, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Maffoni, S.; Brazzo, S.; De Giuseppe, R.; Biino, G.; Vietti, I.; Pallavicini, C.; Cena, H. Lifestyle Changes and Body Mass Index during COVID-19 Pandemic Lockdown: An Italian Online-Survey. Nutrients 2021, 13, 1117. [Google Scholar] [CrossRef] [PubMed]
- Laffin, L.J.; Kaufman, H.W.; Chen, Z.; Niles, J.K.; Arellano, A.R.; Bare, L.A.; Hazen, S.L. Rise in Blood Pressure Observed Among US Adults During the COVID-19 Pandemic. Circulation 2022, 145, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Celik, M.; Yilmaz, Y.; Karagoz, A.; Kahyaoglu, M.; Cakmak, E.O.; Kup, A.; Celik, F.B.; Karaduman, A.; Kulahcioglu, S.; Izci, S. Anxiety disorder associated with the COVID-19 pandemic causes deterioration of blood pressure control in primary hypertensive patients. Medeni. Med. J. 2021, 36, 83. [Google Scholar]
- Rezaei, A.; Neshat, S.; Heshmat-Ghahdarijani, K. Alterations of lipid profile in COVID-19: A narrative review. Curr. Probl. Cardiol. 2021, 47, 100907. [Google Scholar] [CrossRef] [PubMed]
- Biancalana, E.; Parolini, F.; Mengozzi, A.; Solini, A. Short-term impact of COVID-19 lockdown on metabolic control of patients with well-controlled type 2 diabetes: A single-centre observational study. Acta Diabetol. 2021, 58, 431–436. [Google Scholar] [CrossRef]
- Auriemma, R.S.; Pirchio, R.; Liccardi, A.; Scairati, R.; Del Vecchio, G.; Pivonello, R.; Colao, A. Metabolic syndrome in the era of COVID-19 outbreak: Impact of lockdown on cardiometabolic health. J. Endocrinol. Investig. 2021, 44, 2845–2847. [Google Scholar] [CrossRef]
- Gjaka, M.; Feka, K.; Bianco, A.; Tishukaj, F.; Giustino, V.; Parroco, A.M.; Palma, A.; Battaglia, G. The effect of COVID-19 lockdown measures on physical activity levels and sedentary behaviour in a relatively young population living in Kosovo. J. Clin. Med. 2021, 10, 763. [Google Scholar] [CrossRef] [PubMed]
- Mauro, M.; Toselli, S.; Bonazzi, S.; Grigoletto, A.; Cataldi, S.; Greco, G.; Latessa, P.M. Effects of quarantine on Physical Activity prevalence in Italian Adults: A pilot study. PeerJ 2022, 10, e14123. [Google Scholar] [CrossRef] [PubMed]
- Halpern, B.; Louzada, M.L.d.C.; Aschner, P.; Gerchman, F.; Brajkovich, I.; Faria-Neto, J.R.; Polanco, F.E.; Montero, J.; Juliá, S.M.M.; Lotufo, P.A. Obesity and COVID-19 in Latin America: A tragedy of two pandemics—Official document of the Latin American Federation of Obesity Societies. Obes. Rev. 2021, 22, e13165. [Google Scholar] [CrossRef]
- Polero, P.; Rebollo-Seco, C.; Adsuar, J.C.; Pérez-Gómez, J.; Rojo-Ramos, J.; Manzano-Redondo, F.; Garcia-Gordillo, M.Á.; Carlos-Vivas, J. Physical Activity Recommendations during COVID-19, Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 65. [Google Scholar] [CrossRef]
- Bentlage, E.; Ammar, A.; How, D.; Ahmed, M.; Trabelsi, K.; Chtourou, H.; Brach, M. Practical Recommendations for Maintaining Active Lifestyle during the COVID-19 Pandemic: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 6265. [Google Scholar] [CrossRef]
- Chen, Y.; Ma, L.; Ma, Y.; Wang, H.; Luo, J.; Zhang, X.; Luo, C.; Wang, H.; Zhao, H.; Pan, D.; et al. A national school-based health lifestyles interventions among Chinese children and adolescents against obesity: Rationale, design and methodology of a randomized controlled trial in China. BMC Public Health 2015, 15, 210. [Google Scholar] [CrossRef] [Green Version]
- Arena, R.; Lavie, C.J.; Hivert, M.-F.; Williams, M.A.; Briggs, P.D.; Guazzi, M. Who will deliver comprehensive healthy lifestyle interventions to combat non-communicable disease? Introducing the healthy lifestyle practitioner discipline. Expert Rev. Cardiovasc. Ther. 2016, 14, 15–22. [Google Scholar] [CrossRef]
- Marcon, E.R.; Baglioni, S.; Bittencourt, L.; Lopes, C.; Neumann, C.; Trindade, M. What is the best treatment before bariatric surgery? Exercise, exercise and group therapy, or conventional waiting: A randomized controlled trial. Obes. Surg. 2017, 27, 763–773. [Google Scholar] [CrossRef]
- Delgado-Floody, P.; Soriano-Maldonado, A.; Rodríguez-Pérez, M.A.; Latorre-Román, P.Á.; Martínez-Salazar, C.; Vargas, C.A.; Caamaño-Navarrete, F.; Jerez-Mayorga, D.; Álvarez, C. The Effects of Two Different Concurrent Training Configurations on Markers of Metabolic Syndrome and Fitness in Women with Severe/Morbid Obesity: A Randomised Controlled Trial. Front. Physiol. 2021, 12, 1160. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Floody, P.; Latorre-Román, P.Á.; Jerez-Mayorga, D.; Caamaño-Navarrete, F.; Cano-Montoya, J.; Laredo-Aguilera, J.A.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; Pozuelo-Carrascosa, D.P.; Álvarez, C. Poor sleep quality decreases concurrent training benefits in markers of metabolic syndrome and quality of life of morbidly obese patients. Int. J. Environ. Res. Public Health 2020, 17, 6804. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed] [Green Version]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A. 2013 ESH/ESC practice guidelines for the management of arterial hypertension: ESH-ESC the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood Press. 2014, 23, 3–16. [Google Scholar] [CrossRef]
- North American Association for the Study of Obesity, National Heart, Lung, Blood Institute; NHLBI Obesity Education Initiative. The Practical Guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults; National Institutes of Health, National Heart, Lung, and Blood Institute, NHLBI Obesity Education Initiative, North American Association for the Study of Obesity: Bethesda, MA, USA, 2000.
- Sturm, R. Increases in morbid obesity in the USA. 2000–2005. Public Health 2007, 121, 492–496. [Google Scholar] [CrossRef] [Green Version]
- De Souza, S.A.F.; Faintuch, J.; Fabris, S.M.; Nampo, F.K.; Luz, C.; Fabio, T.L.; Sitta, I.S.; de Batista Fonseca, I.C. Six-minute walk test: Functional capacity of severely obese before and after bariatric surgery. Surg. Obes. Relat. Dis. 2009, 5, 540–543. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Gonzalez, M.C.; Schulzke, J.-D.; Pirlich, M. Hand grip strength: Outcome predictor and marker of nutritional status. Clin. Nutr. 2011, 30, 135–142. [Google Scholar] [CrossRef]
- Delgado-Floody, P.; Alvarez, C.; Lusa Cadore, E.; Flores-Opazo, M.; Caamano-Navarrete, F.; Izquierdo, M. Preventing metabolic syndrome in morbid obesity with resistance training: Reporting interindividual variability. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1368–1381. [Google Scholar] [CrossRef]
- Álvarez, C.; Ramírez-Campillo, R.; Lucia, A.; Ramírez-Vélez, R.; Izquierdo, M. Concurrent exercise training on hyperglycemia and comorbidities associated: Non-responders using clinical cutoff points. Scand. J. Med. Sci. Sports 2019, 29, 952–967. [Google Scholar] [CrossRef]
- Brzycki, M. Strength testing—Predicting a one-rep max from reps-to-fatigue. J. Phys. Educ. Recreat. Danc. 1993, 64, 88–90. [Google Scholar] [CrossRef]
- Guzik, T.J.; Mohiddin, S.A.; Dimarco, A.; Patel, V.; Savvatis, K.; Marelli-Berg, F.M.; Madhur, M.S.; Tomaszewski, M.; Maffia, P.; D’acquisto, F. COVID-19 and the cardiovascular system: Implications for risk assessment, diagnosis, and treatment options. Cardiovasc. Res. 2020, 116, 1666–1687. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Quintana, E.; del Carmen Vega-Acedo, L.; Santana-Herrera, D.; Pérez-Acosta, C.; Medina-Gil, J.M.; Muñoz-Díaz, E.; Rodríguez-González, F. Mental well-being among patients with congenital heart disease and heart failure during the COVID-19 pandemic. Am. J. Cardiovasc. Dis. 2021, 11, 618. [Google Scholar] [PubMed]
- Sohn, M.; Koo, B.K.; Yoon, H.I.; Song, K.-H.; Kim, E.S.; Kim, H.B.; Lim, S. Impact of COVID-19 and Associated Preventive Measures on Cardiometabolic Risk Factors in South Korea. J. Obes. Metab. Syndr. 2021, 30, 248. [Google Scholar] [CrossRef] [PubMed]
- Kaufman-Shriqui, V.; Navarro, D.A.; Raz, O.; Boaz, M. Multinational dietary changes and anxiety during the coronavirus pandemic-findings from Israel. Isr. J. Health Policy Res. 2021, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Narici, M.; Vito, G.D.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur. J. Sport Sci. 2021, 21, 614–635. [Google Scholar] [CrossRef]
- Timmons, J.F.; Griffin, C.; Cogan, K.E.; Matthews, J.; Egan, B. Exercise maintenance in older adults 1 year after completion of a supervised training intervention. J. Am. Geriatr. Soc. 2020, 68, 163–169. [Google Scholar] [CrossRef]
- Leitão, L.; Marocolo, M.; de Souza, H.L.; Arriel, R.A.; Campos, Y.; Mazini, M.; Junior, R.P.; Figueiredo, T.; Louro, H.; Pereira, A. Three-Month vs. One-Year Detraining Effects after Multicomponent Exercise Program in Hypertensive Older Women. Int. J. Environ. Res. Public Health 2022, 19, 2871. [Google Scholar] [CrossRef]
- Flanagan, E.W.; Beyl, R.A.; Fearnbach, S.N.; Altazan, A.D.; Martin, C.K.; Redman, L.M. The impact of COVID-19 stay-at-home orders on health behaviors in adults. Obesity 2021, 29, 438–445. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Chourdakis, M. Impact of the first COVID-19 lockdown on body weight: A combined systematic review and a meta-analysis. Clin. Nutr. 2021; in press. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M. Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of the ECLB-COVID19 international online survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Kriaucioniene, V.; Bagdonaviciene, L.; Rodríguez-Pérez, C.; Petkeviciene, J. Associations between changes in health behaviours and body weight during the COVID-19 quarantine in Lithuania: The Lithuanian COVIDiet study. Nutrients 2020, 12, 3119. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity, eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Li, H.; Tao, X.; Fan, Y.; Gao, Q.; Yang, J. Optimised anthropometric indices as predictive screening tools for metabolic syndrome in adults: A cross-sectional study. BMJ Open 2021, 11, e043952. [Google Scholar] [CrossRef] [PubMed]
- Ramírez Manent, J.I.; Altisench Jané, B.; Sanchís Cortés, P.; Busquets-Cortés, C.; Arroyo Bote, S.; Masmiquel Comas, L.; López González, Á.A. Impact of COVID-19 lockdown on anthropometric variables, blood pressure, and glucose and lipid profile in healthy adults: A before and after pandemic lockdown longitudinal study. Nutrients 2022, 14, 1237. [Google Scholar] [CrossRef] [PubMed]
- Bogataj Jontez, N.; Novak, K.; Kenig, S.; Petelin, A.; Jenko Pražnikar, Z.; Mohorko, N. The Impact of COVID-19-Related Lockdown on Diet and Serum Markers in Healthy Adults. Nutrients 2021, 13, 1082. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Ferran, M.; de la Guía-Galipienso, F.; Sanchis-Gomar, F.; Pareja-Galeano, H. Metabolic impacts of confinement during the COVID-19 pandemic due to modified diet and physical activity habits. Nutrients 2020, 12, 1549. [Google Scholar] [CrossRef]
- Aajal, A.; El Boussaadani, B.; Hara, L.; Benajiba, C.; Boukouk, O.; Benali, M.; Ouadfel, O.; Bendoudouch, H.; Zergoune, N.; Alkattan, D. The consequences of the lockdown on cardiovascular diseases. J. Am. Coll. Cardiol. 2021, 77, 3136. [Google Scholar] [CrossRef]
- Fosco, M.J.; Silva, P.; Taborda, G.A.; Ahumada, L. Asociación entre aislamiento social preventivo obligatorio por COVID-19 e Hipertensión Arterial Grave. MEDICINA 2020, 80, 25–29. [Google Scholar]
- Giralt-Herrera, A.; Rojas-Velázquez, J.M.; Leiva-Enríquez, J. Relación entre COVID-19 e hipertensión arterial. Rev. Habanera De Cienc. Méd. 2020, 19, e_3246. [Google Scholar]
- Saklayen, M.G. The global epidemic of the metabolic syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Time | HIIT + RT | RT + HIIT | Baseline p-Value | |
|---|---|---|---|---|
| Age (y) | 45.0 ± 8.9 | 35.5 ± 14.7 | p = 0.108 | |
| Anthropometric | ||||
| Body mass (kg) | Pre0 | 104.4 ± 20.3 | 120.1 ± 21.8 | p = 0.132 |
| Post1 | 102.7 ± 20.6 | 115.1 ± 20.8 ¥ | ||
| Post2 | 109.2 ± 19.3 † | 121.8 ± 266 *† | ||
| BMI (kg/m2) | Pre0 | 42.1 ± 6.6 | 47.5 ± 8.4 | p = 0.153 |
| Post1 | 41.4 ± 6.4 | 45.6 ± 8.3 | ||
| Post2 | 44.1 ± 6.5 | 47.6 ± 10.3 † | ||
| Body composition | ||||
| Body fat (%) | Pre0 | 48.2 ± 4.2 | 50.6 ± 3.7 | p = 0.222 |
| Post1 | 48.0 ± 3.8 | 50.7 ± 4.8 | ||
| Post2 | 49.7 ± 3.2 *† | 48.4 ± 4.3 | ||
| Body fat (kg) | Pre0 | 50.8 ± 13.6 | 61.4 ± 15.9 | p = 0.164 |
| Post1 | 49.9 ± 13.5 | 59.3 ± 16.3 | ||
| Post2 | 54.8 ± 12.9 *† | 59.7 ± 18 | ||
| Lean mass (kg) | Pre0 | 53.2 ± 7.1 | 58.5 ± 6.6 | p = 0.0.47 |
| Post1 | 52.6 ± 7.3 | 56.2 ± 4.2 | ||
| Post2 | 54.3 ± 6.7 † | 62.0 ± 10.3 *† | ||
| Skeletal muscle mass (kg) | Pre0 | 50.5 ± 6.8 | 55.6 ± 6.2 | p = 0.129 |
| Post1 | 50.0 ± 6.9 | 53.3 ± 4.0 | ||
| Post2 | 51.5 ± 6.4 † | 58.8 ± 9.8 *† | ||
| Bone mass (kg) | Pre0 | 2.7 ± 0.3 | 2.9 ± 0.3 | p = 0.157 |
| Post1 | 2.6 ± 0.3 | 2.8 ± 0.1 | ||
| Post2 | 2.7 ± 0.3 | 3.1 ± 0.4 *† | ||
| Total body water (%) | Pre0 | 38.7 ± 5.9 | 41.8 ± 4.5 | p = 0.259 |
| Post1 | 37.3 ± 5.4 | 40.2 ± 4.4 | ||
| Post2 | 39.7 ± 5.6 | 46.5 ± 9.4 *† | ||
| Basal metabolic rate (kcal) | Pre0 | 1688.0 ± 251.0 | 1897.0 ± 230.0 | p = 0.094 |
| Post1 | 1670.0 ± 255.1 | 1818.0 ± 175.8 | ||
| Post2 | 1727.0 ± 237.8 † | 1985.0 ± 349.0 *† |
| Time | HIIT + RT | RT + HIIT | p-Value | |
|---|---|---|---|---|
| Cardiovascular | ||||
| Heart rate resting (beats/min) | Pre0 | 85.2 ± 17.8 | 78.6 ± 10.1 | p = 0.257 |
| Post1 | 86.9 ± 16.9 | 92.9 ± 17.8 ¥ | ||
| Post2 | 85.2 ± 10.8 | 84.2 ± 16.1 | ||
| Metabolic | ||||
| Total cholesterol (mg/dL) | Pre0 | 177.6 ± 33.7 | 191.6 ± 23.5 | p = 0.356 |
| Post1 | 180.6 ± 34.2 | 170.5 ± 26.9 | ||
| Post2 | 180.5 ± 38.6 | 178.3 ± 19.6 | ||
| LDL cholesterol (mg/dL) | Pre0 | 116.8 ± 39.1 | 124.6 ± 17.2 | p = 0.630 |
| Post1 | 116.6 ± 20.9 | 112.7 ± 22.8 | ||
| Post2 | 123.5 ± 35.8 | 125.0 ± 20.1 | ||
| Physical fitness | ||||
| 6 Mwt (m) | Pre0 | 540.9 ± 117.1 | 531.4 ± 51.7 | p = 0.843 |
| Post1 | 660.9 ± 104.3 | 585.0 ± 65.9 | ||
| Post2 | 504.5 ± 119.9 *† | 541.4 ± 94.0 | ||
| Handgrip strength dominant (kg) | Pre0 | 29.1 ± 6.5 | 32.2 ± 9.6 | p = 0.425 |
| Post1 | 31.6 ± 6.4 | 33.5 ± 4.9 | ||
| Post2 | 28.5 ± 7.1 | 33.8 ± 7.3 | ||
| Handgrip strength non-dominant (kg) | Pre0 | 26.5 ± 6.3 | 29.5 ± 9.3 | p = 0.425 |
| Post1 | 29.8 ± 6.7 | 31.2 ± 5.9 | ||
| Post2 | 27.7 ± 7.2 | 35.2 ± 9.2 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delgado-Floody, P.; Chirosa-Ríos, L.; Guzmán-Guzmán, I.P.; Vargas, C.A.; Sandoval-Aguilera, K.; Caamaño-Navarrete, F.; Guede-Rojas, F.; Alvarez, C. The Social Distance Impacts from COVID-19 Pandemic on the Development of Two Orders of a Concurrent Training Programme for Morbidly Obese Patients. Int. J. Environ. Res. Public Health 2022, 19, 13408. https://doi.org/10.3390/ijerph192013408
Delgado-Floody P, Chirosa-Ríos L, Guzmán-Guzmán IP, Vargas CA, Sandoval-Aguilera K, Caamaño-Navarrete F, Guede-Rojas F, Alvarez C. The Social Distance Impacts from COVID-19 Pandemic on the Development of Two Orders of a Concurrent Training Programme for Morbidly Obese Patients. International Journal of Environmental Research and Public Health. 2022; 19(20):13408. https://doi.org/10.3390/ijerph192013408
Chicago/Turabian StyleDelgado-Floody, Pedro, Luis Chirosa-Ríos, Iris Paola Guzmán-Guzmán, Claudia Andrea Vargas, Karina Sandoval-Aguilera, Felipe Caamaño-Navarrete, Francisco Guede-Rojas, and Cristian Alvarez. 2022. "The Social Distance Impacts from COVID-19 Pandemic on the Development of Two Orders of a Concurrent Training Programme for Morbidly Obese Patients" International Journal of Environmental Research and Public Health 19, no. 20: 13408. https://doi.org/10.3390/ijerph192013408