
Feasibility of Patient Reported Outcome Measures in Psychosocial Palliative Care: Observational Cohort Study of Hospice Day Care and Social Support Groups

Abstract
:1. Introduction
Aim
2. Materials and Methods
2.1. Study Design
2.2. Settings
2.3. Participants
2.4. Recruitment
2.5. Sample Size
2.6. Data Collection
2.6.1. Perceived Social Support
2.6.2. Loneliness
2.6.3. Depression
2.6.4. Quality of Life
2.7. Analysis
3. Results
3.1. Participants
3.2. Recruitment
3.3. Data Collection
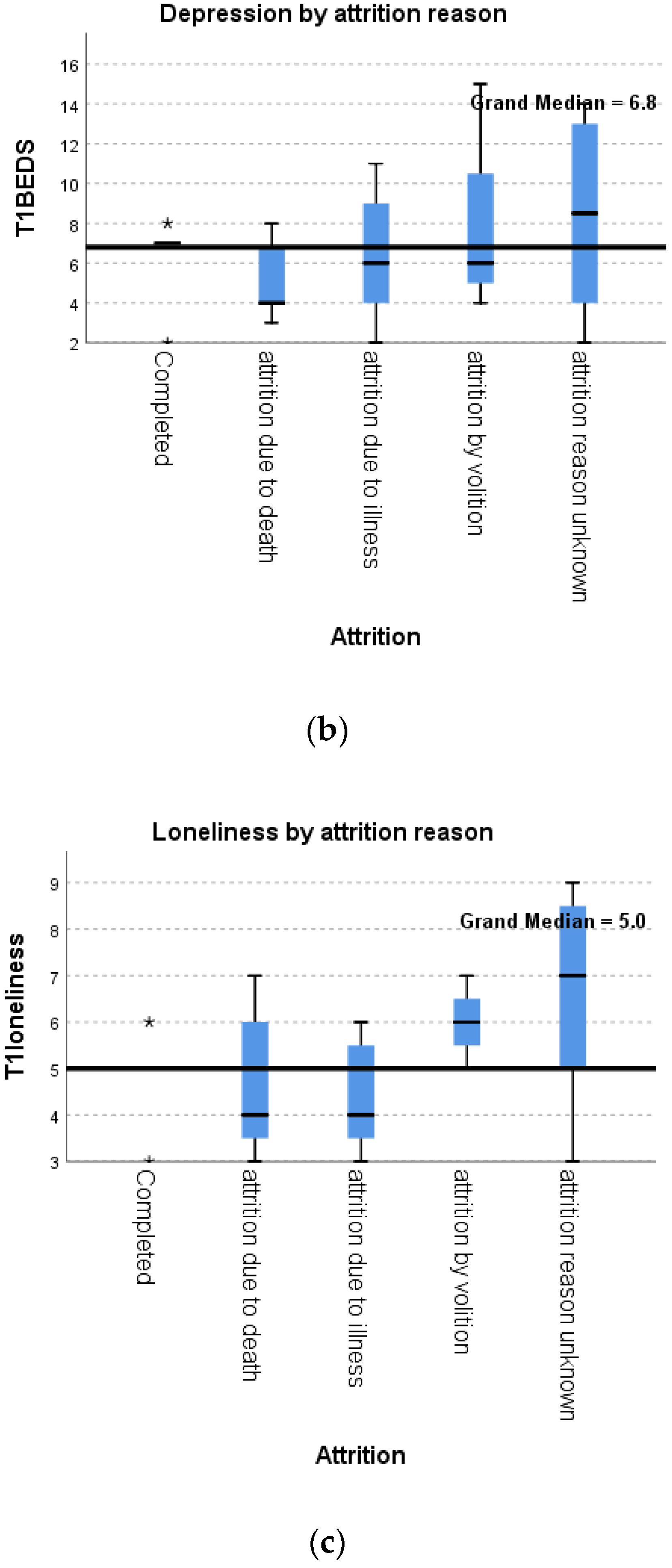
3.4. Reasons for Attrition
3.5. Quality of Life (EQ-5D-5L)
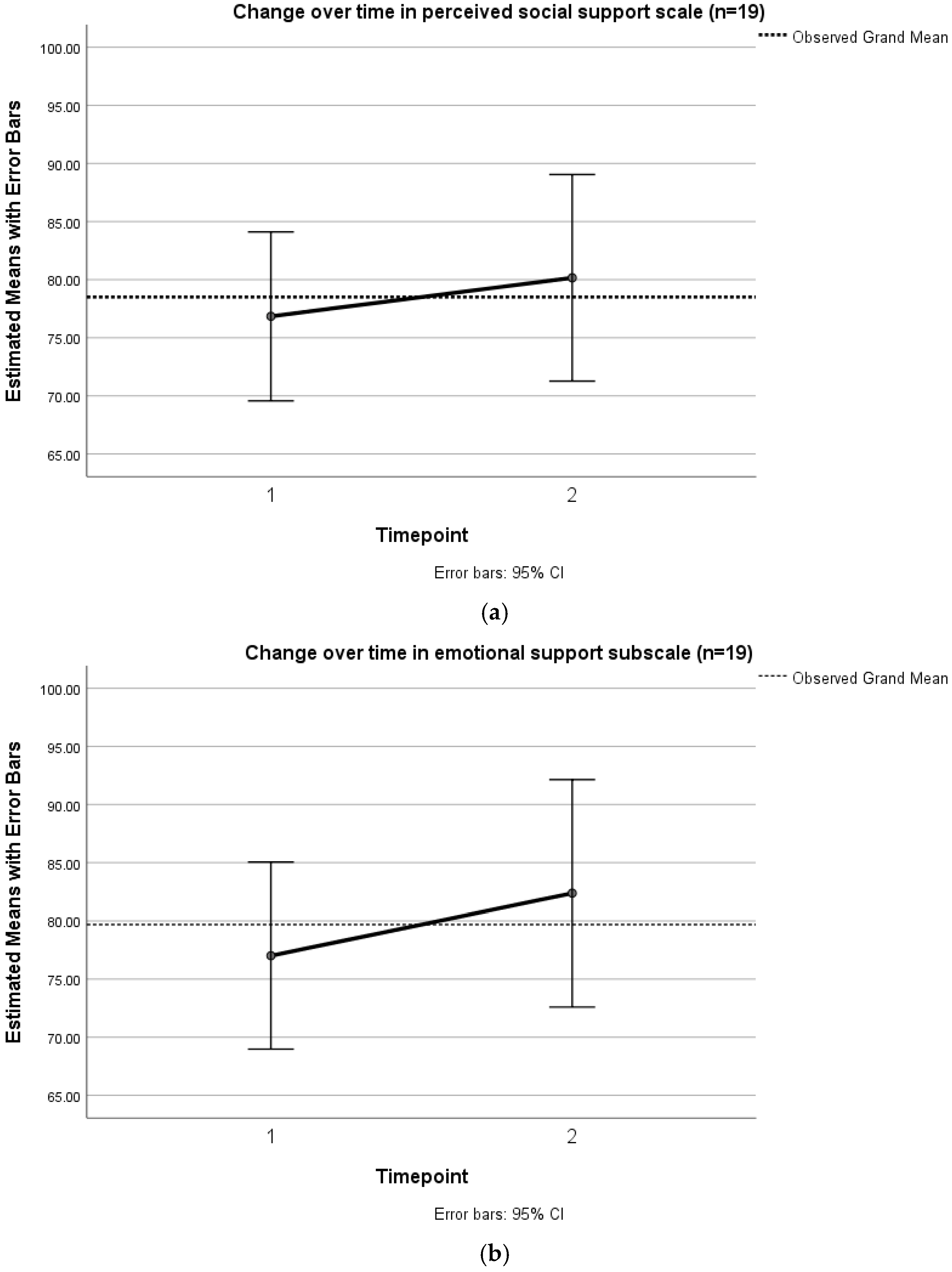
3.6. Perceived Social Support (MOS-SS)
3.7. Loneliness (UCLA)
3.8. Depression (BEDS)
3.9. Research Location
3.10. Patient Context
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lloyd, A.; Kendall, M.; Starr, J.M.; A Murray, S. Physical, social, psychological and existential trajectories of loss and adaptation towards the end of life for older people living with frailty: A serial interview study. BMC Geriatr. 2016, 16, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krikorian, A.; Limonero, J.T.; Maté, J. Suffering and distress at the end-of-life. Psycho-Oncology 2011, 21, 799–808. [Google Scholar] [CrossRef]
- Hospice UK. Hospice Accounts Report; Hospice UK: London, UK, 2018. [Google Scholar]
- Bradley, N.; Dowrick, C.; Lloyd-Williams, M. A survey of hospice day services in the United Kingdom & Republic of Ireland: How did hospices offer social support to palliative care patients, pre-pandemic? BMC Palliat. Care 2022, 21, 170. [Google Scholar] [CrossRef]
- Bradley, N.; Lloyd-Williams, M.; Dowrick, C. Effectiveness of palliative care interventions offering social support to people with life-limiting illness-A systematic review. Eur. J. Cancer Care 2018, 27, e12837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodwin, D.M.; Higginson, I.J.; Myers, K.; Douglas, H.-R.; Normand, C.E. What is palliative day care? Support Care Cancer 2002, 10, 556–562. [Google Scholar] [CrossRef]
- Holt-Lunstad, J. Why Social Relationships Are Important for Physical Health: A Systems Approach to Understanding and Modifying Risk and Protection. Annu. Rev. Psychol. 2018, 69, 437–458. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Cacioppo, S. Social Relationships and Health: The Toxic Effects of Perceived Social Isolation. Soc. Pers. Psychol. Compass 2014, 8, 58–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social Relationships and Mortality Risk: A Meta-analytic Review. PLOS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and Social Isolation as Risk Factors for Mortality. Perspect. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [Green Version]
- Lim, M.H.; Eres, R.; Vasan, S. Understanding loneliness in the twenty-first century: An update on correlates, risk factors, and potential solutions. Soc. Psychiatry 2020, 55, 793–810. [Google Scholar] [CrossRef] [PubMed]
- Jaremka, L.M.; Fagundes, C.P.; Glaser, R.; Bennett, J.M.; Malarkey, W.B.; Kiecolt-Glaser, J.K. Loneliness predicts pain, depression, and fatigue: Understanding the role of immune dysregulation. Psychoneuroendocrinology 2013, 38, 1310–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nummela, O.; Seppänen, M.; Uutela, A. The effect of loneliness and change in loneliness on self-rated health (SRH): A longitudinal study among aging people. Arch. Gerontol. Geriatr. 2011, 53, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Courtin, E.; Knapp, M. Social isolation, loneliness and health in old age: A scoping review. Health Soc. Care Community 2017, 25, 799–812. [Google Scholar] [CrossRef] [PubMed]
- Arabyat, R.M.; Raisch, D.W. Relationships Between Social/Emotional Support and Quality of Life, Depression and Disability in Patients With Chronic Obstructive Pulmonary Disease: An Analysis Based on Propensity Score Matching. Ann. Behav. Med. 2019, 53, 918–927. [Google Scholar] [CrossRef] [PubMed]
- Teo, A.R.; Marsh, H.E.; Forsberg, C.W.; Nicolaidis, C.; Chen, J.I.; Newsom, J.; Saha, S.; Dobscha, S.K. Loneliness is closely associated with depression outcomes and suicidal ideation among military veterans in primary care. J. Affect. Disord. 2018, 230, 42–49. [Google Scholar] [CrossRef]
- Sorato, D.B.; Osório, F.L. Coping, psychopathology, and quality of life in cancer patients under palliative care. Palliat. Support. Care 2014, 13, 517–525. [Google Scholar] [CrossRef]
- Fivecoat, H.C.; Sayers, S.L.; Riegel, B. Social support predicts self-care confidence in patients with heart failure. Eur. J. Cardiovasc. Nurs. 2018, 17, 598–604. [Google Scholar] [CrossRef] [Green Version]
- Svidén, G.A.; Fürst, C.; von Koch, L.; Borell, L. Palliative day care—A study of well-being and health-related quality of life. Palliat. Med. 2009, 23, 441–447. [Google Scholar] [CrossRef]
- Leppert, W.; Zdun-Ryżewska, A.; Forycka, M.; Mess, E.; Majkowicz, M. Quality of life assessment in advanced cancer patients treated at home, an inpatient unit, and a day care center. OncoTargets Ther. 2014, 7, 687–695. [Google Scholar] [CrossRef] [Green Version]
- Guy, M.P.; Higginson, I.J.; Amesbury, B.D. The effect of Palliative Daycare on Hope: A comparison of Daycare Patients with Two Control Groups. J. Palliat. Care 2011, 27, 216–223. [Google Scholar] [CrossRef]
- Lloyd-Williams, M.; Cobb, M.; O’Connor, C.; Dunn, L.; Shiels, C. A pilot randomised controlled trial to reduce suffering and emotional distress in patients with advanced cancer. J. Affect. Disord. 2013, 148, 141–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloyd-Williams, M.; Shiels, C.; Ellis, J.; Abba, K.; Gaynor, E.; Wilson, K.; Dowrick, C. Pilot randomised controlled trial of focused narrative intervention for moderate to severe depression in palliative care patients: DISCERN trial. Palliat. Med. 2017, 32, 206–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walshe, C.; Roberts, D.; Appleton, L.; Calman, L.; Large, P.; Lloyd-Williams, M.; Grande, G. Coping Well with Advanced Cancer: A Serial Qualitative Interview Study with Patients and Family Carers. PLoS ONE 2017, 12, e0169071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrop, E.; Noble, S.; Edwards, M.; Sivell, S.; Moore, B.; Nelson, A. Managing, making sense of and finding meaning in advanced illness: A qualitative exploration of the coping and wellbeing experiences of patients with lung cancer. Sociol. Health Illn. 2017, 39, 1448–1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, A.; Coroiu, A.; Korner, A. One-to-one peer support in cancer care: A review of scholarship published between 2007 and 2014. Eur. J. Cancer Care 2014, 24, 299–312. [Google Scholar] [CrossRef]
- I Van Dongen, S.; De Nooijer, K.; Cramm, J.M.; Francke, A.L.; Oldenmenger, W.H.; Korfage, I.J.; E Witkamp, F.; Stoevelaar, R.; Van Der Heide, A.; Rietjens, J.A. Self-management of patients with advanced cancer: A systematic review of experiences and attitudes. Palliat. Med. 2020, 34, 160–178. [Google Scholar] [CrossRef] [Green Version]
- Walshe, C.; Roberts, D.; Calman, L.; Appleton, L.; Croft, R.; Skevington, S.; Lloyd-Williams, M.; Grande, G.; Algorta, G.P. Peer support to maintain psychological wellbeing in people with advanced cancer: Findings from a feasibility study for a randomised controlled trial. BMC Palliat. Care 2020, 19, 129. [Google Scholar] [CrossRef]
- Walshe, C.; Roberts, D. Peer support for people with advanced cancer: A systematically constructed scoping review of quantitative and qualitative evidence. Curr. Opin. Support. Palliat. Care 2018, 12, 308–322. [Google Scholar] [CrossRef]
- E Bradley, S.; Frizelle, D.; Johnson, M. Patients’ psychosocial experiences of attending Specialist Palliative Day Care: A systematic review. Palliat. Med. 2011, 25, 210–228. [Google Scholar] [CrossRef]
- Stevens, E.; Martin, C.R.; A White, C. The outcomes of palliative care day services: A systematic review. Palliat. Med. 2010, 25, 153–169. [Google Scholar] [CrossRef]
- Brereton, L.; Clark, J.; Ingleton, C.; Gardiner, C.; Preston, L.; Ryan, T.; Goyder, E. What do we know about different models of providing palliative care? Findings from a systematic review of reviews. Palliat. Med. 2017, 31, 781–797. [Google Scholar] [CrossRef] [PubMed]
- Higginson, I.J.; Evans, C.J.; Grande, G.; Preston, N.; Morgan, M.; McCrone, P.; Lewis, P.; Fayers, P.; Harding, R.; Hotopf, M.; et al. Evaluating complex interventions in End of Life Care: The MORECare Statement on good practice generated by a synthesis of transparent expert consultations and systematic reviews. BMC Med. 2013, 11, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Hussain, J.; White, I.R.; Johnson, M.J.; Byrne, A.; Preston, N.J.; Haines, A.; Seddon, K.; Peters, T.J. Development of guidelines to reduce, handle and report missing data in palliative care trials: A multi-stakeholder modified nominal group technique. Palliat. Med. 2022, 36, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Hussain, J.A.; White, I.R.; Langan, D.; Johnson, M.J.; Currow, D.C.; Torgerson, D.J.; Bland, M. Missing data in randomized controlled trials testing palliative interventions pose a significant risk of bias and loss of power: A systematic review and meta-analyses. J. Clin. Epidemiol. 2015, 74, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Cacioppo, J.T. A Short Scale for Measuring Loneliness in Large Surveys. Res. Aging 2004, 26, 655–672. [Google Scholar] [CrossRef]
- Lloyd-Williams, M.; Shiels, C.; Dowrick, C. The development of the Brief Edinburgh Depression Scale (BEDS) to screen for depression in patients with advanced cancer. J. Affect. Disord. 2007, 99, 259–264. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Gąsiorowski, J.; Rudowicz, E. Functional Social Support for Hypertensive Patients in Primary Care Setting in Poland: What Is Expected and What Is Received? Value Health Reg. Issues 2017, 13, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Priede, A.; Andreu, Y.; Martínez, P.; Conchado, A.; Ruiz-Torres, M.; González-Blanch, C. The factor structure of the Medical Outcomes Study–Social Support Survey: A comparison of different models in a sample of recently diagnosed cancer patients. J. Psychosom. Res. 2018, 108, 32–38. [Google Scholar] [CrossRef]
- Valtorta, N.K.; Kanaan, M.; Gilbody, S.; Hanratty, B. Loneliness, social isolation and social relationships: What are we measuring? A novel framework for classifying and comparing tools. BMJ Open 2016, 6, e010799. [Google Scholar] [CrossRef] [Green Version]
- De Jong Gierveld, J.; van Tilburg, T. A 6-Item Scale for Overall, Emotional, and Social Loneliness. Res. Aging 2006, 28, 582–598. [Google Scholar] [CrossRef] [Green Version]
- Russell, D.; Peplau, L.A.; Cutrona, C.E. The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. J. Pers. Soc. Psychol. 1980, 39, 472–480. [Google Scholar] [CrossRef]
- Hughes, S.; Jaremka, L.M.; Alfano, C.M.; Glaser, R.; Povoski, S.P.; Lipari, A.M.; Agnese, D.; Farrar, W.B.; Yee, L.D.; Carson, I.W.E.; et al. Social support predicts inflammation, pain, and depressive symptoms: Longitudinal relationships among breast cancer survivors. Psychoneuroendocrinology 2014, 42, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Lie, H.; Hjermstad, M.; Fayers, P.; Finset, A.; Kaasa, S.; Loge, J. Depression in advanced cancer—Assessment challenges and associations with disease load. J. Affect. Disord. 2015, 173, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Plumb, M.M.; Holland, J. Comparative Studies of Psychological Function in Patients with Advanced Cancer—I. Self-Reported Depressive Symptoms. Psychosom. Med. 1977, 39, 264–276. [Google Scholar] [CrossRef]
- Lloyd-Williams, M. Screening for depression in palliative care patients: A review. Eur. J. Cancer Care 2001, 10, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Tordrup, D.; Mossman, J.; Kanavos, P. Responsiveness of the EQ-5D to clinical change: Is the patient experience adequately represented? Int. J. Technol. Assess. Health Care 2014, 30, 10–19. [Google Scholar] [CrossRef]
- Janssen, M.F.; Pickard, A.S.; Golicki, D.; Gudex, C.; Niewada, M.; Scalone, L.; Swinburn, P.; Busschbach, J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Qual. Life Res. 2012, 22, 1717–1727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolan, C.M.; Longworth, L.; Lord, J.; Canavan, J.L.; E Jones, S.; Kon, S.; Man, W.D.-C. The EQ-5D-5L health status questionnaire in COPD: Validity, responsiveness and minimum important difference. Thorax 2016, 71, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.-W.; Sun, H.-P.; Wang, X.; Ma, Q.; Xu, Y.; Luo, N.; Wang, P. The EQ-5D-5L index score is more discriminative than the EQ-5D-3L index score in diabetes patients. Qual. Life Res. 2014, 24, 1767–1774. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.M.; Coast, J.; Myring, G.; Ricciardi, F.; Vickerstaff, V.; Jones, L.; Zafar, S.; Cudmore, S.; Jordan, J.; McKibben, L.; et al. Exploring the costs, consequences and efficiency of three types of palliative care day services in the UK: A pragmatic before-and-after descriptive cohort study. BMC Palliat. Care 2020, 19, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Nipp, R.D.; El-Jawahri, A.; Ba, J.N.F.; Ba, J.E.; Stagl, J.M.; Rn, E.R.G.; Park, E.R.; Jackson, V.A.; Pirl, W.; Greer, J.A.; et al. The relationship between coping strategies, quality of life, and mood in patients with incurable cancer. Cancer 2016, 122, 2110–2116. [Google Scholar] [CrossRef]
- Johns, S.A.; Beck-Coon, K.; Stutz, P.V.; Talib, T.L.; Chinh, K.; Cottingham, A.H.; Schmidt, K.; Shields, C.; Stout, M.E.; Stump, T.E.; et al. Mindfulness Training Supports Quality of Life and Advance Care Planning in Adults With Metastatic Cancer and Their Caregivers: Results of a Pilot Study. Am. J. Hosp. Palliat. Med. 2019, 37, 88–99. [Google Scholar] [CrossRef]
- Pappa, K.; Doty, T.; Taff, S.D.; Kniepmann, K.; Foster, E.R. Self-Management Program Participation and Social Support in Parkinson’s Disease: Mixed Methods Evaluation. Phys. Occup. Ther. Geriatr. 2017, 35, 81–98. [Google Scholar] [CrossRef] [Green Version]
- Feldstain, A.; Macdonald, N.; Bhargava, R.; Chasen, M. Reported distress in patients living with advanced cancer: Changes pre-post interdisciplinary palliative rehabilitation. Support. Care Cancer 2017, 25, 3191–3197. [Google Scholar] [CrossRef]
- Rutkowski, N.A.; Lebel, S.; Richardson, K.; Mutsaers, B.; Chasen, M.; Feldstain, A. A Little Help from My Friends: Social Support in Palliative Rehabilitation. Curr. Oncol. 2018, 25, 358–365. [Google Scholar] [CrossRef] [Green Version]
- Nottelmann, L.; Grønvold, M.; Petersen, M.A.; Vejlgaard, T.; Jensen, L.H. A single-center randomized clinical trial of palliative rehabilitation versus standard care alone in patients with newly diagnosed non-resectable cancer. J. Clin. Oncol. 2018, 36, 75. [Google Scholar] [CrossRef]
- Lloyd-Williams, M.; Shiels, C.; Dowrick, C.; Kissane, D. Socio-Economic Deprivation and Symptom Burden in UK Hospice Patients with Advanced Cancer—Findings from a Longitudinal Study. Cancers 2021, 13, 2537. [Google Scholar] [CrossRef]
- Perissinotto, C.; Holt-Lunstad, J.; Periyakoil, V.S.; Covinsky, K. A Practical Approach to Assessing and Mitigating Loneliness and Isolation in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 657–662. [Google Scholar] [CrossRef]
- Köhler, M.; Steinmann, E.; Mehdorn, H.M.; Pedersen, A.; Goebel, S. The importance of social relationships for brain tumor patients’ quality of life: A case for the inclusion of the concept of disclosure in psycho-oncological care. J. Psychosoc. Oncol. 2019, 38, 310–327. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Uchino, B.N. Uchino. Social Ambivalence and Disease (SAD): A Theoretical Model Aimed at Understanding the Health Implications of Ambivalent Relationships. Psychol. Sci. 2019, 14, 941–966. [Google Scholar] [CrossRef]
- Rivers, A.S.; Sanford, K. When we say “perceived support,” what do we mean? Contexts and components of support among people with serious medical conditions. J. Soc. Pers. Relatsh. 2020, 37, 2758–2778. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Recruitment Dates | Region of England | Index of Multiple Deprivation (0–10, 10 = Least Deprived) | Urban or Rural Hospice Location | Hospice Services (Intervention Description) |
|---|---|---|---|---|---|
| 1 | December 2018–March 2019 | North-West | 5 | Urban city and town | Traditional day care with clinical input & facilitated discussions. Specified day to attend. Transport provided. |
| 2 | August 2018–March 2019 | South-West | 9 | Rural village | Traditional day care with spirituality, art, and nature. Transport provided. Stepdown programme in operation. |
| 3 | February 2019–April 2019 | South-East | 5 | Urban major conurbation | Rehabilitative exercise group, plus social & therapeutic programme. Open access social space. Limited transport provision. |
| 4 | October 2018–April 2019 | South Coast | 5 | Urban city and town | Open access art, exercise, & wellbeing groups. Clinical input & transport by appointment. |
| Domain. | Measure | Description | Reason for Selection |
|---|---|---|---|
| Perceived social support | MOS-SS | 19 questions, inc. emotional, informational, tangible, affectionate, and interactional support | Questions about perception of different types of support, including outside of the family unit, and so reflects goals of intervention. |
| Loneliness | UCLA 3-item | 3 indirect questions on loneliness, distinct from functional support and depressive symptomology | Brief measure of perception of relevant negative social experiences reflecting loneliness, without using word ‘lonely’. |
| Depression | BEDS | 6 questions, based on cognitive and affective depressive symptoms | Brief measure suitable for advanced illness and validated for use in palliative care. |
| Quality of life | EQ-5D-5L | 5 questions-mobility, self-care, usual activities, pain, anxiety/depression-plus visual analogue scale | 5 domains commonly used in practice so familiar to participants, 5 L could be more sensitive to change than 3 L version. |
| Site 1 | Site 2 | Site 3 | Site 4 | Total | |
|---|---|---|---|---|---|
| N | 8 | 6 | 10 | 6 | 30 |
| Age | |||||
| Range | 58–77 | 56–87 | 56–91 | 59–84 | 56–91 |
| Mean (standard error) | 69.38 (2.764) | 70.5 (5.542) | 68.5 (3.769) | 78.17 (3.894) | 71.07 (1.999) |
| 95% confidence interval | 62.84–75.91 | 56.25–84.75 | 59.97–77.03 | 68.16–88.18 | 66.98–75.15 |
| Gender | |||||
| Male | 5 | 0 | 7 | 3 | 15 |
| Female | 3 | 6 | 3 | 3 | 15 |
| Ethnicity | |||||
| White British | 8 | 5 | 9 | 6 | 28 |
| Asian Ugandan | 0 | 1 | 0 | 0 | 1 |
| Black Caribbean | 0 | 0 | 1 | 0 | 1 |
| Diagnosis | |||||
| Cancer | 2 | 4 | 7 | 3 | 16 |
| Noncancer | 2 | 0 | 1 | 3 | 6 |
| Multimorbidity inc cancer | 4 | 2 | 1 | 0 | 7 |
| Living alone | 1 | 1 | 4 | 2 | 8 |
| Dimension. | T1 (n = 30) | T2 (n = 19) | Significance |
|---|---|---|---|
| Mobility | |||
| 1 | 13.3% | 5.3% | 0.248 |
| 2 | 10% | 15.8% | |
| 3 | 53.3% | 42.1% | |
| 4 | 20% | 36.8% | |
| 5 | 3.3% | 0% | |
| Self-care | |||
| 1 | 40% | 26.3% | 0.012 |
| 2 | 23.3% | 21.1% | |
| 3 | 20% | 42.1% | |
| 4 | 13.3% | 5.3% | |
| 5 | 3.3% | 5.3% | |
| Usual activities | |||
| 1 | 13.3% | 5.3% | 0.273 |
| 2 | 10% | 15.8% | |
| 3 | 36.7% | 31.6% | |
| 4 | 26.7% | 21.1% | |
| 5 | 13.3% | 26.3% | |
| Pain/discomfort | |||
| 1 | 13.3% | 10.5% | 0.248 |
| 2 | 6.7% | 26.3% | |
| 3 | 63.3% | 47.4% | |
| 4 | 16.7% | 15.8% | |
| 5 | 0% | 0% | |
| Anxiety/Depression | |||
| 1 | 43.3% | 42.1% | 0.357 |
| 2 | 30% | 26.3% | |
| 3 | 23.3% | 31.6% | |
| 4 | 3.3% | 0% | |
| 5 | 0% | 0% | |
| Overall health (VAS 0-100) | (n = 28) | (n = 19) | |
| Median | 56 | 60 | 0.420 |
| Mean | 54.18 | 55.63 | |
| Standard deviation | 16.678 | 20.421 |
| Mean Change | Standard Deviation | Standard Error of Mean | 95% Confidence Interval of the Difference | T Value | p Value (2 Tailed) | Wilcoxon Signed Rank Test | ||
|---|---|---|---|---|---|---|---|---|
| Overall social support | 3.316 | 16.082 | 3.689 | −0.435 | 11.067 | 0.899 | 0.381 | 0.267 |
| Emotional | 5.357 | 16.114 | 3.697 | −0.410 | 13.124 | 1.449 | 0.165 | 0.114 |
| Tangible | 5.263 | 24.970 | 5.729 | −0.772 | 17.299 | 0.919 | 0.370 | 0.189 |
| Affectionate | −0.351 | 13.050 | 2.994 | −0.641 | 5.940 | −0.117 | 0.908 | 0.904 |
| Interaction | 4.211 | 18.485 | 4.241 | −0.699 | 13.120 | 0.993 | 0.334 | 0.268 |
| Mean Change | Standard Deviation | Standard Error of Mean | 95% Confidence Interval of The Difference | T Value | p Value (2 Tailed) | Wilcoxon Signed Rank Test | ||
|---|---|---|---|---|---|---|---|---|
| Loneliness | −0.421 | 1.071 | 0.246 | −0.937 | 0.95 | −0.714 | 0.104 | 0.104 |
| Depression | −0.632 | 2.985 | 0.685 | −0.070 | 0.807 | −0.922 | 0.369 | 0.528 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bradley, N.; Dowrick, C.; Lloyd-Williams, M. Feasibility of Patient Reported Outcome Measures in Psychosocial Palliative Care: Observational Cohort Study of Hospice Day Care and Social Support Groups. Int. J. Environ. Res. Public Health 2022, 19, 13258. https://doi.org/10.3390/ijerph192013258
Bradley N, Dowrick C, Lloyd-Williams M. Feasibility of Patient Reported Outcome Measures in Psychosocial Palliative Care: Observational Cohort Study of Hospice Day Care and Social Support Groups. International Journal of Environmental Research and Public Health. 2022; 19(20):13258. https://doi.org/10.3390/ijerph192013258
Chicago/Turabian StyleBradley, Natasha, Christopher Dowrick, and Mari Lloyd-Williams. 2022. "Feasibility of Patient Reported Outcome Measures in Psychosocial Palliative Care: Observational Cohort Study of Hospice Day Care and Social Support Groups" International Journal of Environmental Research and Public Health 19, no. 20: 13258. https://doi.org/10.3390/ijerph192013258