
Factors Associated with Using Telemedicine in the Primary Care Clinics during the COVID-19 Pandemic in Israel

Abstract
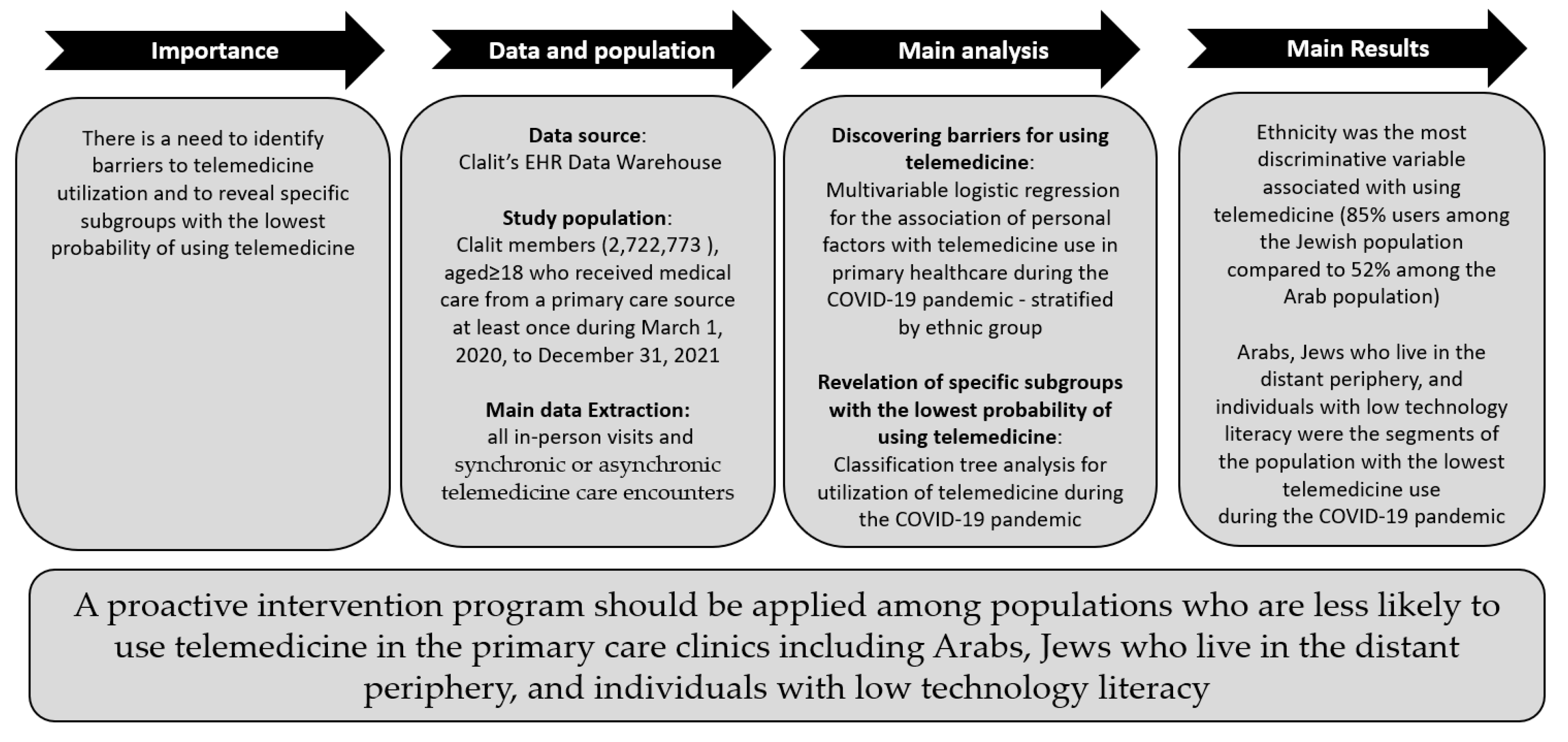
:1. Introduction
2. Methods
2.1. Data Source
2.2. Study Design
2.3. Study Population
2.4. Study Variables
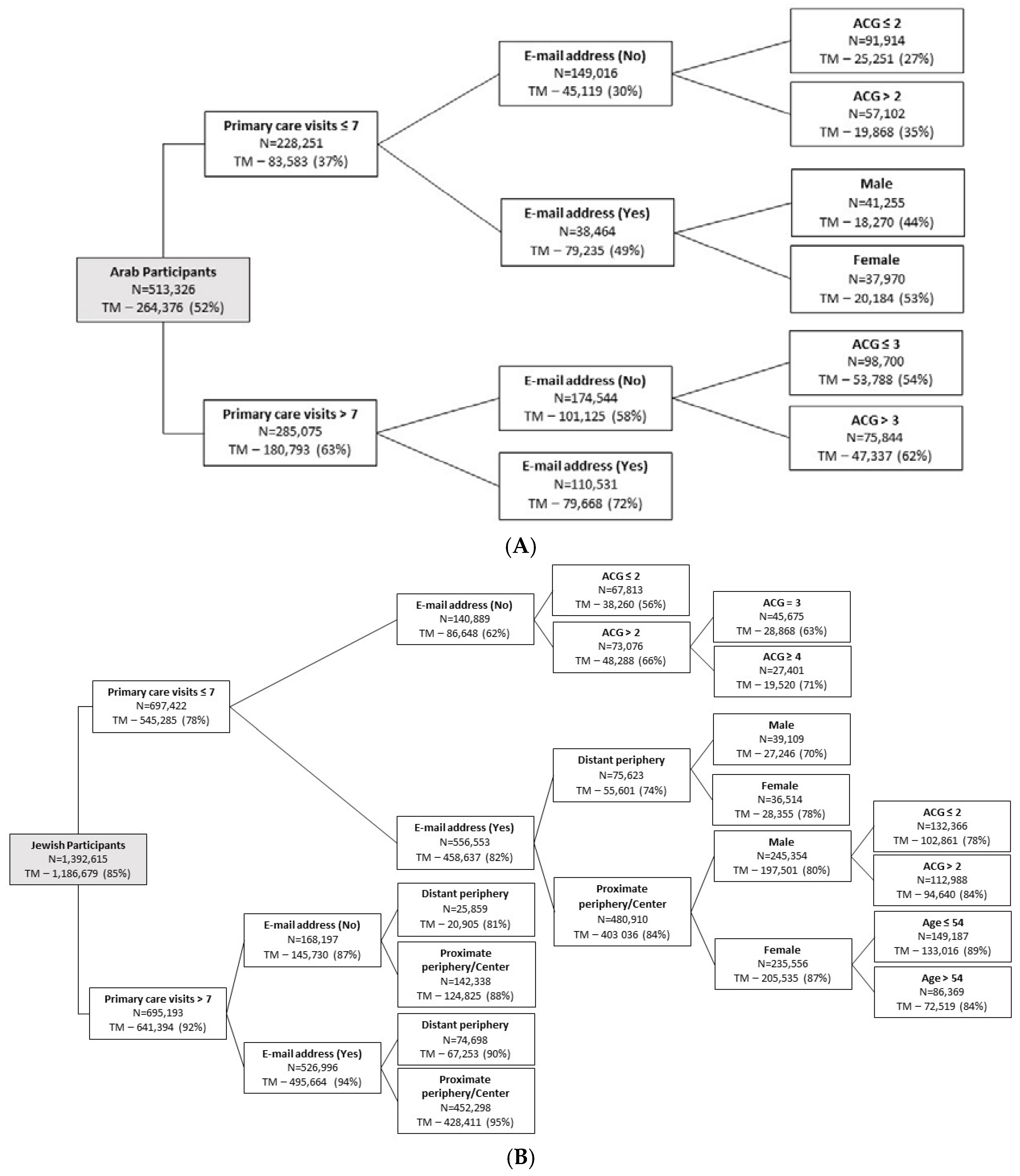
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Whaley, C.M.; Pera, M.F.; Cantor, J.; Chang, J.; Velasco, J.; Hagg, H.K.; Sood, N.; Bravata, D.M. Changes in Health Services Use among Commercially Insured US Populations During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2024984. [Google Scholar] [CrossRef] [PubMed]
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med. Inform. Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef]
- Lau, J.; Knudsen, J.; Jackson, H.; Wallach, A.B.; Bouton, M.; Natsui, S.; Philippou, C.; Karim, E.; Silvestri, D.M.; Avalone, L.; et al. Staying Connected in the COVID-19 Pandemic: Telehealth at the Largest Safety-Net System In The United States. Health Aff. 2020, 39, 1437–1442. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.Y.; Mehrotra, A.; Huskamp, H.A.; Uscher-Pines, L.; Ganguli, I.; Barnett, M.L. Variation in Telemedicine Use and Outpatient Care during the COVID-19 Pandemic in the United States. Health Aff. 2021, 40, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Colbert, G.B.; Venegas-Vera, A.V.; Lerma, E.V. Utility of telemedicine in the COVID-19 era. Rev. Cardiovasc. Med. 2020, 21, 583–587. [Google Scholar] [CrossRef]
- Cantor, J.H.; McBain, R.K.; Pera, M.F.; Bravata, D.M.; Whaley, C.M. Who Is (and Is Not) Receiving Telemedicine Care during the COVID-19 Pandemic. Am. J. Prev. Med. 2021, 61, 434–438. [Google Scholar] [CrossRef]
- Lavie, G.; Weinstein, O.; Segal, Y.; Davidson, E. Adapting to change: Clalit’s response to the COVID-19 pandemic. Isr. J. Health Policy Res. 2021, 10, 68. [Google Scholar] [CrossRef] [PubMed]
- Miron, O.; Sagy, Y.W.; Yaron, S.; Ramot, N.; Lavie, G. Trends in the Volume and Types of Primary Care Visits during the Two Years of the COVID-19 Pandemic in Israel. Int. J. Environ. Res. Public Health 2022, 19, 10601. [Google Scholar] [CrossRef]
- Khairat, S.; Haithcoat, T.; Liu, S.; Zaman, T.; Edson, B.; Gianforcaro, R.; Shyu, C.-R. Advancing health equity and access using telemedicine: A geospatial assessment. J. Am. Med. Inform. Assoc. 2019, 26, 796–805. [Google Scholar] [CrossRef]
- Nouri, S.; Khoong, E.C.; Lyles, C.R.; Karliner, L. Addressing equity in telemedicine for chronic disease management during the COVID-19 pandemic. NEJM Catal. Innov. Care Deliv. 2020, 1, 1–13. [Google Scholar]
- Luo, J.; Tong, L.; Crotty, B.H.; Somai, M.; Taylor, B.; Osinski, K.; George, B. Telemedicine Adoption during the COVID-19 Pandemic: Gaps and Inequalities. Appl. Clin. Inform. 2021, 12, 836–844. [Google Scholar] [CrossRef]
- Center for Connected Health Policy State Telehealth Laws and Medicaid Program Policies Spring. 2022. Available online: https://www.cchpca.org/resources/state-telehealth-laws-and-reimbursement-policies-report-spring-2022/ (accessed on 18 August 2022).
- Centers for Medicare & Medicaid Services. Coronavirus Waivers & Flexibilities. Baltimore: U.S. Centers for Medicare & Medicaid Services. Updated 30 April 2020. Available online: https://www.cms.gov/about-cms/emergency-preparedness-response-operations/current-emergencies/coronavirus-waivers (accessed on 18 August 2022).
- Pierce, R.P.; Stevermer, J.J. Disparities in use of telehealth at the onset of the COVID-19 public health emergency. J. Telemed. Telecare 2020. [Google Scholar] [CrossRef]
- Adepoju, O.E.; Chae, M.; Ojinnaka, C.O.; Shetty, S.; Angelocci, T. Utilization Gaps during the COVID-19 Pandemic: Racial and Ethnic Disparities in Telemedicine Uptake in Federally Qualified Health Center Clinics. J. Gen. Intern. Med. 2022, 37, 1191–1197. [Google Scholar] [CrossRef]
- Jaffe, D.H.; Lee, L.; Huynh, S.; Haskell, T.P. Health Inequalities in the Use of Telehealth in the United States in the Lens of COVID-19. Popul. Health Manag. 2020, 23, 368–377. [Google Scholar] [CrossRef] [PubMed]
- López, L.; Green, A.R.; Tan-McGrory, A.; King, R.S.; Betancourt, J.R. Bridging the Digital Divide in Health Care: The Role of Health Information Technology in Addressing Racial and Ethnic Disparities. Jt. Comm. J. Qual. Patient Saf. 2011, 37, 437–445. [Google Scholar] [CrossRef] [Green Version]
- Roberts, E.T.; Mehrotra, A. Assessment of Disparities in Digital Access Among Medicare Beneficiaries and Implications for Telemedicine. JAMA Intern. Med. 2020, 180, 1386. [Google Scholar] [CrossRef] [PubMed]
- Lam, K.; Lu, A.D.; Shi, Y.; Covinsky, K.E. Assessing Telemedicine Unreadiness Among Older Adults in the United States during the COVID-19 Pandemic. JAMA Intern. Med. 2020, 180, 1389. [Google Scholar] [CrossRef] [PubMed]
- Benis, A.; Banker, M.; Pinkasovich, D.; Kirin, M.; Yoshai, B.-E.; Benchoam-Ravid, R.; Ashkenazi, S.; Seidmann, A. Reasons for Utilizing Telemedicine during and after the COVID-19 Pandemic: An Internet-Based International Study. J. Clin. Med. 2021, 10, 5519. [Google Scholar] [CrossRef]
- Central Bureau of Statistics Israel. Characterization and Classification of Geographical Units by the Socio-Economic Level of the Population 2008; Central Bureau of Statistics Israel: Jerusalem, Israel, 2013.
- Points Location Intelligence. 2019. Available online: http://www.points.co.il/?lang=en (accessed on 25 August 2022).
- Central Bureau of Statistics–Statistical Methodology Department–Natalia Tsibel. Peripherality Index of Local Authorities in Israel: Combination of Potential Accessibility Index with Proximity to the Tel Aviv District; Working paper series No.45; Central Bureau of Statistics: Jerusalem, Israel, 2009.
- Johns Hopkins Bloomberg School of Public Health. The Johns Hopkins ACG ® System Version 11.0 Applications Guide; Johns Hopkins Bloomberg School of Public Health: Baltimore, MD, USA, 2014. [Google Scholar]
- Mitchell, U.A.; Chebli, P.G.; Ruggiero, L.; Muramatsu, N. The digital divide in health-related technology use: The significance of race/ethnicity. Gerontologist 2019, 59, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Daoud, N.; Soskolne, V.; Mindell, J.S.; Roth, M.A.; Manor, O. Ethnic inequalities in health between Arabs and Jews in Israel: The relative contribution of individual-level factors and the living environment. Int. J. Public Health 2017, 63, 313–323. [Google Scholar] [CrossRef]
- Vilchinsky, N.; Reges, O.; Leibowitz, M.; Khaskia, A.; Mosseri, M.; Kark, J.D. Symptoms of Depression and Anxiety as Barriers to Participation in Cardiac Rehabilitation Programs Among Arab and Jewish Patients in Israel. J. Cardiopulm. Rehabil. Prev. 2018, 38, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Campos-Castillo, C.; Anthony, D. Racial and ethnic differences in self-reported telehealth use during the COVID-19 pandemic: A secondary analysis of a US survey of internet users from late March. J. Am. Med. Inform. Assoc. 2021, 28, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Dopelt, K.; Avni, N.; Haimov-Sadikov, Y.; Golan, I.; Davidovitch, N. Telemedicine and eHealth Literacy in the Era of COVID-19: A Cross-Sectional Study in a Peripheral Clinic in Israel. Int. J. Environ. Res. Public Health 2021, 18, 9556. [Google Scholar] [CrossRef] [PubMed]
- Tinmaz, H.; Lee, Y.-T.; Fanea-Ivanovici, M.; Baber, H. A systematic review on digital literacy. Smart Learn. Environ. 2022, 9, 21. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Jewish | Arabs | ||
|---|---|---|---|---|
| n = 2,722,773 | n = 1,990,049 | n = 732,724 | ||
| Sex | ||||
| Male | n (%) | 1,276,981 (46.9%) | 922,694 (46.4%) | 354,287 (48.4%) |
| Female | n (%) | 1,445,792 (53.1%) | 1,067,355 (53.6%) | 378,437 (51.6%) |
| Age | ||||
| Years | Mean (SD) | 46.8 (18.4) | 49.4 (18.5) | 39.7 (16.3) |
| 18–24 | n (%) | 294,793 (10.8%) | 138,633 (7.0%) | 156,160 (21.3%) |
| 25–44 | n (%) | 1,103,065 (40.5%) | 787,219 (39.6%) | 315,846 (43.1%) |
| 45–64 | n (%) | 754,296 (27.7%) | 558,906 (28.1%) | 195,390 (26.7%) |
| 65–74 | n (%) | 343,734 (12.6%) | 301,296 (15.1%) | 42,438 (5.8%) |
| ≥75 | n (%) | 226,885 (8.3%) | 203,995 (10.3%) | 22,890 (3.1%) |
| Socio-economic status | ||||
| Level | Mean (SD) | 5.34 (2.08) | 6.09 (1.79) | 3.27 (1.26) |
| 1–3 | n (%) | 689,683 (25.3%) | 191,052 (9.6%) | 498,631 (68.1%) |
| 4–5 | n (%) | 731,923 (26.9%) | 543,824 (27.3%) | 188,099 (25.7%) |
| 6–7 | n (%) | 807,750 (29.7%) | 768,017 (38.6%) | 39,733 (5.4%) |
| 8–10 | n (%) | 493,417 (18.1%) | 487,156 (24.5%) | 6,261 (0.9%) |
| Birthplace | ||||
| Israel | n (%) | 2,053,293 (75.4%) | 1,335,968 (67.1%) | 717,325 (97.9%) |
| Other | n (%) | 669,480 (24.6%) | 654,081 (32.9%) | 15,399 (2.1%) |
| Children | ||||
| Number | Mean (SD) | 0.86 (1.43) | 0.78 (1.36) | 1.11 (1.56) |
| 0 | n (%) | 1,757,101 (64.5%) | 1,345,735 (67.6%) | 411,366 (56.1%) |
| 1–2 | n (%) | 568,934 (20.9%) | 387,863 (19.5%) | 181,071 (24.7%) |
| 3–4 | n (%) | 327,503 (12.0%) | 214,355 (10.8%) | 113,148 (15.4%) |
| ≥5 | n (%) | 69,235 (2.5%) | 42,096 (2.1%) | 27,139 (3.7%) |
| Peripherality index | ||||
| Distant periphery (1–4) | n (%) | 533,160 (19.6%) | 281,677 (14.2%) | 251,483 (34.3%) |
| Proximate periphery (5–7) | n (%) | 1,239,005 (45.5%) | 898,034 (45.1%) | 340,971 (46.5%) |
| Central (8–10) | n (%) | 950,608 (34.9%) | 810,338 (40.7%) | 140,270 (19.1%) |
| Residence in an urban area | ||||
| No | n (%) | 809,988 (29.7%) | 428,781 (21.5%) | 381,207 (52.0%) |
| Yes | n (%) | 1,912,785 (70.3%) | 1,561,268 (78.5%) | 351,517 (48.0%) |
| ACG Comorbidity Score | ||||
| Level | Mean (SD) | 3.07 (1.11) | 3.15 (1.11) | 2.87 (1.09) |
| 1–2 | n (%) | 932,464 (34.2%) | 632,895 (31.8%) | 299,569 (40.9%) |
| 3 | n (%) | 855,588 (31.4%) | 622,940 (31.3%) | 232,648 (31.8%) |
| 4 | n (%) | 650,732 (23.9%) | 502,875 (25.3%) | 147,857 (20.2%) |
| 5–6 | n (%) | 283,989 (10.4%) | 231,339 (11.6%) | 52,650 (7.2%) |
| Home confinement | ||||
| No | n (%) | 2,125,820 (97.6%) | 1,606,635 (97.4%) | 519,185 (98.1%) |
| Yes | n (%) | 52,386 (2.4%) | 42,368 (2.6%) | 10,018 (1.9%) |
| E-mail address | ||||
| Yes | n (%) | 1,819,024 (66.8%) | 1,548,243 (77.8%) | 270,781 (37.0%) |
| No | n (%) | 903,749 (33.2%) | 441,806 (22.2%) | 461,943 (63.0%) |
| Primary care visits | ||||
| Number of visits | Mean (SD) | 10.67 (10.15) | 10.17 (9.46) | 12.05 (11.72) |
| Telemedicine utilization | ||||
| ≥1 Telemedicine care service | n (%) | 2,073,584 (76%) | 1,696,225 (85%) | 377,359 (52%) |
| Jewish n = 1,990,049 | Arabs n = 732,724 | |
|---|---|---|
| Predictor | OR (95% CI) | OR (95% CI) |
| Sex | ||
| Male (Ref. group) | 1.00 | 1.00 |
| Female | 1.39 (1.39–1.39) | 1.28 (1.28–1.28) |
| Age (years) | ||
| 18–24 | 1.14 (1.14–1.14) | 0.93 (0.93–0.93) |
| 25–44 | 1.28 (1.28–1.28) | 1.06 (1.06–1.06) |
| 45–64 (Ref. group) | 1.00 | 1.00 |
| 65–74 | 0.89 (0.89–0.89) | 0.94 (0.94–0.94) |
| ≥75 | 0.97 (0.97–0.97) | 1.17 (1.17–1.17) |
| Socio-economic status | ||
| 1–3 (Ref. group) | 1.00 | 1.00 |
| 4–5 | 1.10 (1.10–1.10) | 1.03 (1.03–1.03) |
| 6–7 | 1.23 (1.23–1.23) | 1.62 (1.62–1.62) |
| 8–10 | 1.27 (1.27–1.27) | 1.30 (1.30–1.30) |
| Birthplace | ||
| Israel | 1.31 (1.31–1.31) | N/A |
| Other (Ref. group) | 1.00 | |
| Children | ||
| 0 (Ref. group) | 1.00 | 1.00 |
| 1–2 | 1.09 (1.09–1.09) | 1.05 (1.05–1.05) |
| 3–4 | 1.07 (1.07–1.07) | 1.05 (1.05–1.05) |
| ≥5 | 1.12 (1.12–1.12) | 1.18 (1.18–1.18) |
| Peripherality index | ||
| Distant periphery (1–4) (Ref. group) | 1.00 | 1.00 |
| Proximate periphery (5–7) | 1.56 (1.56–1.56) | 1.08 (1.08–1.08) |
| Central (8–10) | 1.72 (1.72–1.72) | 0.98 (0.98–0.98) |
| Residence in an urban area | ||
| No (Ref. group) | 1.00 | 1.00 |
| Yes | 1.40 (1.40–1.40) | 1.19 (1.19–1.19) |
| ACG Comorbidity Score | ||
| 1–2 (Ref. group) | 1.00 | 1.00 |
| 3 | 1.28 (1.28–1.28) | 1.16 (1.16–1.16) |
| 4 | 1.58 (1.58–1.58) | 1.27 (1.27–1.27) |
| 5–6 | 1.64 (1.64–1.64) | 1.28 (1.28–1.28) |
| Home confinement | ||
| No (Ref. group) | 1.00 | 1.00 |
| Yes | 1.96 (1.96–1.96) | 1.42 (1.42–1.42) |
| E-mail address | ||
| No (Ref. group) | 1.00 | 1.00 |
| Yes | 2.49 (2.49–2.49) | 2.01 (2.01–2.01) |
| Primary care visits | ||
| Number of visits | 1.11 (1.11–1.11) | 1.06 (1.06–1.06) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reges, O.; Feldhamer, I.; Wolff Sagy, Y.; Lavie, G. Factors Associated with Using Telemedicine in the Primary Care Clinics during the COVID-19 Pandemic in Israel. Int. J. Environ. Res. Public Health 2022, 19, 13207. https://doi.org/10.3390/ijerph192013207
Reges O, Feldhamer I, Wolff Sagy Y, Lavie G. Factors Associated with Using Telemedicine in the Primary Care Clinics during the COVID-19 Pandemic in Israel. International Journal of Environmental Research and Public Health. 2022; 19(20):13207. https://doi.org/10.3390/ijerph192013207
Chicago/Turabian StyleReges, Orna, Ilan Feldhamer, Yael Wolff Sagy, and Gil Lavie. 2022. "Factors Associated with Using Telemedicine in the Primary Care Clinics during the COVID-19 Pandemic in Israel" International Journal of Environmental Research and Public Health 19, no. 20: 13207. https://doi.org/10.3390/ijerph192013207