

Effectiveness of Rehabilitation Exercise in Improving Physical Function of Stroke Patients: A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Systematic Data Resource
2.2. Eligibility and Exclusion Criteria
- Patients (P): Patients with a stroke (except where a person without disabilities acts as a person with disabilities)
- Interventions (I): Rehabilitation, exercise, and/or treatment for stroke survivors
- Comparisons (C): No rehabilitation or other intervention
- Outcomes (O): The results after intervention regarding functional improvement, pain reduction, and effectiveness of treatment
2.3. Screening, Selection, and Exrtraction Process
2.4. Assessment of Quality
3. Results
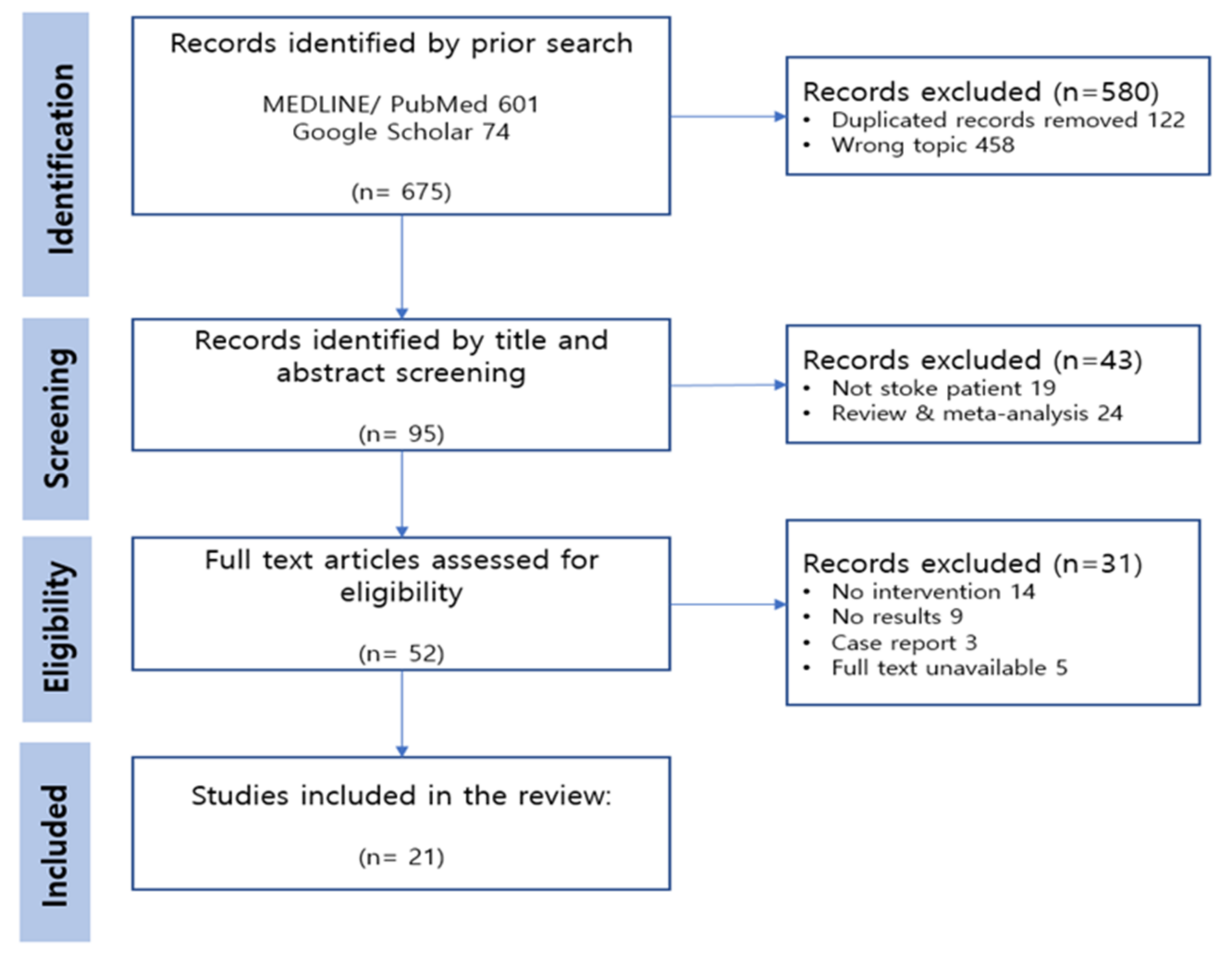
3.1. Study Selection
3.2. Quality Assessment and Risk of Bias
3.3. Study Characteristics
3.4. Exercise Type
3.5. Exercise Type Based on the Stage of Stroke
4. Discussion
4.1. Exercise Type
4.2. Exercise Type Based on the Stage of Stroke
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Selected Paper | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 10 |
| 2 | Yes | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | 8 |
| 3 | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 10 |
| 4 | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| 5 | Yes | No | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6 |
| 6 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 11 |
| 7 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 11 |
| 8 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 11 |
| 9 | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 9 |
| 10 | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 9 |
| 11 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 11 |
| 12 | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 7 |
| 13 | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | 10 |
| 14 | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | 7 |
| 15 | Yes | Yes | No | No | No | Yes | No | Yes | Yes | Yes | Yes | 6 |
| 16 | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | 8 |
| 17 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 11 |
| 18 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 11 |
| 19 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 11 |
| 20 | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 8 |
| 21 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | 10 |
References
- Sharp, S.A.; Brouwer, B.J. Isokinetic strength training of the hemiparetic knee: Effects on function and spasticity. Arch. Phys. Med. Rehabil. 1997, 78, 1231–1236. [Google Scholar] [CrossRef]
- Duncan, P.W.; Horner, R.D.; Reker, D.M.; Samsa, G.P.; Hoenig, H.; Hamilton, B.; LaClair, B.J.; Dudley, T.K. Adherence to Postacute Rehabilitation Guidelines Is Associated With Functional Recovery in Stroke. Stroke 2002, 33, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Hochstenbach, J.; Prigatano, G.; Mulder, T. Patients’ and Relatives’ Reports of Disturbances 9 Months After Stroke: Subjective Changes in Physical Functioning, Cognition, Emotion, and Behavior. Arch. Phys. Med. Rehabil. 2005, 86, 1587–1593. [Google Scholar] [CrossRef]
- Wolf, S.L.; Catlin, P.A.; Ellis, M.; Archer, A.L.; Morgan, B.; Piacentino, A. Assessing Wolf Motor Function Test as Outcome Measure for Research in Patients After Stroke. Stroke 2001, 32, 1635–1639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dijkerman, H.C.; Ietswaart, M.; Johnston, M.; MacWalter, R.S. Does motor imagery training improve hand function in chronic stroke patients? A pilot study. Clin. Rehabil. 2004, 18, 538–549. [Google Scholar] [CrossRef] [PubMed]
- Cifu, D.; Stewart, D.G. Factors affecting functional outcome after stroke: A critical review of rehabilitation interventions. Arch. Phys. Med. Rehabil. 1999, 80, S35–S39. [Google Scholar] [CrossRef]
- Ottenbacher, K.J.; Jannell, S. The Results of Clinical Trials in Stroke Rehabilitation Research. Arch. Neurol. 1993, 50, 37–44. [Google Scholar] [CrossRef]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Kang, S.-M.; Kim, S.-H.; Han, K.-D.; Paik, N.-J.; Kim, W.-S. Physical activity after ischemic stroke and its association with adverse outcomes: A nationwide population-based cohort study. Top. Stroke Rehabil. 2020, 28, 170–180. [Google Scholar] [CrossRef]
- Ivey, F.M.; Hafer-Macko, C.E.; Macko, R.F. Exercise rehabilitation after stroke. NeuroRX 2006, 3, 439–450. [Google Scholar] [CrossRef]
- Blum, L.; Korner-Bitensky, N. Usefulness of the Berg Balance Scale in Stroke Rehabilitation: A Systematic Review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef]
- Teasell, R.; Foley, N.; Salter, K.; Bhogal, S.; Jutai, J.; Speechley, M. Evidence-Based Review of Stroke Rehabilitation: Executive Summary. Top. Stroke Rehabil. 2009, 16, 463–488. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Bovonsunthonchai, S.; Aung, N.; Hiengkaew, V.; Tretriluxana, J. A randomized controlled trial of motor imagery combined with structured progressive circuit class therapy on gait in stroke survivors. Sci. Rep. 2020, 10, 6945. [Google Scholar] [CrossRef] [Green Version]
- Stuart, M.; Dromerick, A.W.; Macko, R.; Benvenuti, F.; Beamer, B.; Sorkin, J.; Chard, S.; Weinrich, M. Adaptive Physical Activity for Stroke: An Early-Stage Randomized Controlled Trial in the United States. Neurorehabil. Neural Repair 2019, 33, 668–680. [Google Scholar] [CrossRef]
- Ribeiro, T.S.; Regalado, I.C.R.; da Silva, S.T.; de Oliveira Sousa, C.; de Figueiredo, K.M.O.B.; Lindquist, A.R.R. Effects of Load Addition During Gait Training on Weight-Bearing and Temporal Asymmetry After Stroke: A Randomized Clinical Trial. Am. J. Phys. Med. Rehabil. 2020, 99, 250–256. [Google Scholar] [CrossRef]
- Manji, A.; Amimoto, K.; Matsuda, T.; Wada, Y.; Inaba, A.; Ko, S. Effects of transcranial direct current stimulation over the supplementary motor area body weight-supported treadmill gait training in hemiparetic patients after stroke. Neurosci. Lett. 2018, 662, 302–305. [Google Scholar] [CrossRef]
- Cecchi, F.; Germanotta, M.; Macchi, C.; Montesano, A.; Galeri, S.; Diverio, M.; Falsini, C.; Martini, M.; Mosca, R.; Langone, E.; et al. Age is negatively associated with upper limb recovery after conventional but not robotic rehabilitation in patients with stroke: A secondary analysis of a randomized-controlled trial. J. Neurol. 2020, 268, 474–483. [Google Scholar] [CrossRef]
- Shimodozono, M.; Noma, T.; Nomoto, Y.; Hisamatsu, N.; Kamada, K.; Miyata, R.; Kawahira, K. Benefits of a repetitive facilitative exercise program for the upper paretic extremity after subacute stroke: A randomized controlled trial. Neurorehabil. Neural Repair 2013, 27, 296–305. [Google Scholar] [CrossRef]
- Marzolini, S.; Brooks, D.; Oh, P.; Jagroop, D.; MacIntosh, B.J.; Anderson, N.D.; Alter, D.; Corbett, D. Aerobic with Resistance Training or Aerobic Training Alone Poststroke: A Secondary Analysis From a Randomized Clinical Trial. Neurorehabil. Neural Repair 2018, 32, 209–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jong, L.D.; Dijkstra, P.U.; Gerritsen, J.; Geurts, A.C.; Postema, K. Combined arm stretch positioning and neuromuscular electrical stimulation during rehabilitation does not improve range of motion, shoulder pain or function in patients after stroke: A randomised trial. J. Physiother. 2013, 59, 245–254. [Google Scholar] [CrossRef] [Green Version]
- Hung, C.S.; Hsieh, Y.W.; Wu, C.Y.; Lin, K.C.; Lin, J.C.; Yeh, L.M.; Yin, H.P. Comparative assessment of two robot-assisted therapies for the upper extremity in people with chronic stroke. Am. J. Occup. Ther. 2019, 73, 7301205010p1–7301205010p9. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-W.; Lin, K.-C.; Wu, C.-Y.; Shih, T.-Y.; Li, M.-W.; Chen, C.-L. Comparison of proximal versus distal upper-limb robotic rehabilitation on motor performance after stroke: A cluster controlled trial. Sci. Rep. 2018, 8, 2091. [Google Scholar] [CrossRef] [Green Version]
- Patten, C.; Condliffe, E.G.; A Dairaghi, C.; Lum, P.S. Concurrent neuromechanical and functional gains following upper-extremity power training post-stroke. J. Neuroeng. Rehabil. 2013, 10, 1. [Google Scholar] [CrossRef] [Green Version]
- Chae, S.H.; Kim, Y.; Lee, K.-S.; Park, H.-S. Development and Clinical Evaluation of a Web-Based Upper Limb Home Rehabilitation System Using a Smartwatch and Machine Learning Model for Chronic Stroke Survivors: Prospective Comparative Study. JMIR mHealth uHealth 2020, 8, e17216. [Google Scholar] [CrossRef]
- Corti, M.; McGuirk, T.E.; Wu, S.S.; Patten, C. Differential Effects of Power Training Versus Functional Task Practice on Compensation and Restoration of Arm Function After Stroke. Neurorehabilit. Neural Repair 2012, 26, 842–854. [Google Scholar] [CrossRef]
- Annino, G.; Alashram, A.R.; Alghwiri, A.A.; Romagnoli, C.; Messina, G.; Tancredi, V.; Mercuri, N.B. Effect of segmental muscle vibration on upper extremity functional ability poststroke: A randomized controlled trial. Medicine 2019, 98, e14444. [Google Scholar] [CrossRef]
- Han, C.; Wang, Q.; Meng, P.-P.; Qi, M.-Z. Effects of intensity of arm training on hemiplegic upper extremity motor recovery in stroke patients: A randomized controlled trial. Clin. Rehabil. 2012, 27, 75–81. [Google Scholar] [CrossRef]
- Linder, S.M.; Davidson, S.; Rosenfeldt, A.; Lee, J.; Koop, M.M.; Bethoux, F.; Alberts, J.L. Forced and Voluntary Aerobic Cycling Interventions Improve Walking Capacity in Individuals With Chronic Stroke. Arch. Phys. Med. Rehabil. 2020, 102, 1–8. [Google Scholar] [CrossRef]
- Emmerson, K.B.; Harding, K.E.; Taylor, N.F. Home exercise programmes supported by video and automated reminders compared with standard paper-based home exercise programmes in patients with stroke: A randomized controlled trial. Clin. Rehabil. 2016, 31, 1068–1077. [Google Scholar] [CrossRef]
- Topcuoglu, A.; Gokkaya, N.K.O.; Ucan, H.; Karakuş, D. The effect of upper-extremity aerobic exercise on complex regional pain syndrome type I: A randomized controlled study on subacute stroke. Top. Stroke Rehabil. 2015, 22, 253–261. [Google Scholar] [CrossRef]
- Jung, K.M.; Choi, J.D. The Effects of Active Shoulder Exercise with a Sling Suspension System on Shoulder Subluxation, Proprioception, and Upper Extremity Function in Patients with Acute Stroke. Med. Sci. Monit. 2019, 25, 4849–4855. [Google Scholar] [CrossRef]
- Kerimov, K.; Benlidayi, I.C.; Ozdemir, C.; Gunasti, O. The Effects of Upper Extremity Isokinetic Strengthening in Post-Stroke Hemiplegia: A Randomized Controlled Trial. J. Stroke Cerebrovasc. Dis. 2021, 30, 105729. [Google Scholar] [CrossRef]
- Pinheiro, D.R.d.R.; Cabeleira, M.E.P.; da Campo, L.A.; Gattino, L.A.F.; de Souza, K.S.; Burg, L.D.S.; Blauth, A.H.E.G.; Corrêa, P.S.; Cechetti, F. Upper limbs cycle ergometer increases muscle strength, trunk control and independence of acute stroke subjects: A randomized clinical trial. NeuroRehabilitation 2021, 48, 533–542. [Google Scholar] [CrossRef]
- Winters, C.; Kwakkel, G.; van Wegen, E.E.; Nijland, R.H.; Veerbeek, J.M.; Meskers, C.G. Moving stroke rehabilitation forward: The need to change research. NeuroRehabilitation 2018, 43, 19–30. [Google Scholar] [CrossRef]
- Aidar, F.J.; Oliveira, R.; Silva, A.; De Matos, D.G.; Filho, M.L.M.; Hickner, R.; Reis, V.M. The Influence of Resistance Exercise Training on the Levels of Anxiety in Ischemic Stroke. Stroke Res. Treat. 2012, 2012, 298375. [Google Scholar] [CrossRef] [Green Version]
- Veerbeek, J.M.; van Wegen, E.; van Peppen, R.; van der Wees, P.J.; Hendriks, E.; Rietberg, M.; Kwakkel, G. What is the evidence for physical therapy poststroke? A systematic review and meta-analysis. PloS ONE 2014, 9, e87987. [Google Scholar] [CrossRef] [Green Version]
- Hebert, D.; Lindsay, M.P.; McIntyre, A.; Kirton, A.; Rumney, P.G.; Bagg, S.; Bayley, M.; Dowlatshahi, D.; Dukelow, S.; Garnhum, M.; et al. Canadian stroke best practice recommendations: Stroke rehabilitation practice guidelines, update 2015. Int. J. Stroke 2016, 11, 459–484. [Google Scholar] [CrossRef] [Green Version]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Zorowitz, R.D. Guidelines for adult stroke rehabilitation and recovery: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef]
- Chang, W.H.; Kim, Y.-H. Robot-assisted Therapy in Stroke Rehabilitation. J. Stroke 2013, 15, 174–181. [Google Scholar] [CrossRef]
- Laver, K.; George, S.; Thomas, S.; Deutsch, J.E.; Crotty, M. Virtual Reality for Stroke Rehabilitation. Stroke 2012, 43. [Google Scholar] [CrossRef]
- Pennycott, A.; Wyss, D.; Vallery, H.; Klamroth-Marganska, V.; Riener, R. Towards more effective robotic gait training for stroke rehabilitation: A review. J. Neuro Eng. Rehabil. 2012, 9, 65. [Google Scholar] [CrossRef] [Green Version]
- Gresham, G.E.; Stason, W.B.; Duncan, P.W. Post-Stroke Rehabilitation; Diane Publishing: Collingdale, PA, USA, 2004; Volume 95, p. 662. [Google Scholar]
- Kim, Y.-H.; Han, T.R.; Jung, H.Y.; Chun, M.H.; Lee, J.; Kim, D.Y.; Paik, N.-J.; Park, S.-W.; Kim, M.-W.; Pyun, S.-B.; et al. Clinical Practice Guideline for Stroke Rehabilitation in Korea. Brain Neurorehabil. 2009, 2, 1–38. [Google Scholar] [CrossRef] [Green Version]
- Laver, K.; Ratcliffe, J.; George, S.; Lester, L.; Walker, R.; Burgess, L.; Crotty, M. Early rehabilitation management after stroke: What do stroke patients prefer? J. Rehabil. Med. 2011, 43, 354–358. [Google Scholar] [CrossRef] [Green Version]
- Askim, T.; Bernhardt, J.; Salvesen, Ø.; Indredavik, B. Physical activity early after stroke and its association to functional outcome 3 months later. J. Stroke Cerebrovasc. Dis. 2014, 23, e305–e312. [Google Scholar] [CrossRef]
- Kendall, B.J.; Gothe, N.P. Effect of aerobic exercise interventions on mobility among stroke patients: A systematic review. Am. J. Phys. Med. Rehabil. 2016, 95, 214–224. [Google Scholar] [CrossRef]
- Stoller, O.; de Bruin, E.D.; Knols, R.H.; Hunt, K.J. Effects of cardiovascular exercise early after stroke: Systematic review and meta-analysis. BMC Neurol. 2012, 12, 45. [Google Scholar] [CrossRef] [Green Version]
- Chi, N.-F.; Huang, Y.-C.; Chiu, H.-Y.; Chang, H.-J.; Huang, H.-C. Systematic Review and Meta-Analysis of Home-Based Rehabilitation on Improving Physical Function Among Home-Dwelling Patients With a Stroke. Arch. Phys. Med. Rehabil. 2019, 101, 359–373. [Google Scholar] [CrossRef]
- D’alisa, S.; Baudo, S.; Mauro, A.; Miscio, G. How does stroke restrict participation in long-term post-stroke survivors? Acta Neurol. Scand. 2005, 112, 157–162. [Google Scholar] [CrossRef]
- Nam, H.S.; Park, E.; Heo, J.H. Facilitating Stroke Management using Modern Information Technology. J. Stroke 2013, 15, 135–143. [Google Scholar] [CrossRef] [PubMed]

| Study ID | Participants (Number, Intervention, Control) | Intervention | Exercise Type | Control | Assessment | Results |
|---|---|---|---|---|---|---|
| Bovonsunthonchai et al. (2020) [15] | 40 participants (20, 20) Age: 49.9 Time since stroke : 3–12 months | Structured Progressive Circuit Class Therapy (SPCCT) + MI (Motor imagery) Duration: 90 min Frequency: 3 times/week (4 weeks) | Functional Aerobic | SPCCT + Health Education Duration: 90 min Frequency: 3 times/week (4 weeks) | Temporo-spatial gait: FDM Strength: dynamometer Step length, time: SI | Temporo-spatial gait: + (p < 0.05), except for the step length of the unaffected limb (p = 0.063). Step length: + (p < 0.001) Step time: X (p > 0.05) Hip flexor: + (p = 0.002) Knee extensor: + (p = 0.014) |
| Stuart et al. (2019) [16] | 76 participants (43, 33) Age: 63.9 Time since stroke : 5.1 years | APA-Strokes (progressive exercise with gait, standing and seated coordination exercises) Duration: 60 min Frequency: 3 times/week (6 weeks) | Aerobic | Sittercise (performed in a seated position) Duration: 60 min Frequency: 3 times/week (6 weeks) | Gait velocity: 6 MWT BBS (Berg balance scale), SPPB (Short Physical Performance Battery), the 30-foot timed walk, the Stroke Impact Scale (SIS) | Gait speed: + (p = 0.004) 30-foot walk: + (p = 0.02) SPPB: X (p = 0.54) BBS: X (p = 0.23) SIS: X (p = 0.90) |
| Ribeiro et al. (2020) [17] | 38 participants (19, 19) Age: 57 Time since stroke : 3 months | Constraint-induced movement therapy (CIMT): treadmill training with load (5% of body weight) on the nonparetic limb Duration: 30 min Frequency: 2 times/week (9 sessions) | Aerobic | Treadmill training without load Duration: 30 min Frequency: 2 times/week (9 sessions) | Ground reaction force (GRF) from static and dynamic trials Swing time symmetry ratio | Static GRF of the paretic limb: + (p = 0.037) Control group’s dynamic GRF: + (p = 0.021) Swing time: X (p = 0.190) |
| Manji et al. (2018) [18] | 30 participants (15, 15) Age: 62.2 Time since stroke : at least 4 months | Transcranial direct current stimulation (tDCS) + body weight-supported treadmill training (BWSTT) → Sham stim + body weight-supported treadmill training (BWSTT) Duration: 20 min Frequency: 7 times/week (2 sessions) | Aerobic | * Crossover design G1: tDCS + BWSTT → Sham stim + BWSTT G2: Sham stim + BWSTT → tDCS + BWSTT | Gait speed: 10 MWT Walking ability: Timed Up and Go (TUG) Lower limb: FMA-LE, TCT, POMA | G1′s Gait speed: + (p < 0.005) G1′s Walking ability: + (p < 0.005) Effect with the groups or interaction: X |
| Cecchi et al. (2021) [19] | 224 participants (113, 111) Age: 68.5 Time since stroke : 46.5 days | Robotic rehabilitation + conventional physiotherapy (6 times/week) Duration: 45 min Frequency: 5 days/week (30sessions) | Functional (passive) | Task-oriented exercises) + Conventional physiotherapy (6 times/week) | FMA-UE | Age-FMA-UE: X (p = 0.603) * Age is associated with the outcome after conventional but not robotic rehabilitation. |
| Shimodozono et al. (2012) [20] | 49rticipants (26, 23) Age: 65 Time since stroke : 6.8 weeks | Repetitive facilitative exercise (elicit movement of the shoulder, elbow, wrist, and fingers + passive stretching) + dexterity-related training (30 min) Duration: 40 min Frequency: 5 days/week (20 sessions) | Functional (passive) | Conventional upper-extremity rehabilitation program | ARAT(Action Research Arm Test) FMA | ARAT: + (p = 0.009) FMA: + (p = 0.019) |
| Marzolini et al. (2018) [21] | 68 participants (35, 33) Age: 63.7 Time since stroke : 11.5 months | Aerobic and resistance training (AT + RT) Duration: 20–60 min Frequency:5 times/wk (6 months) (duration or intensity was increased)-2 sessions (AT) 8weeks-2 sessions (RT) (1 to 2 sets of 10 to 11 exercises) | Aerobic Resistance (isotonic) | AT | Cardiorespiratory Fitness, Body Composition and Dietary Assessment. Maximal Isometric Strength 6 MWT, Sit-to-Stand and Stair Climb Performance Exercise Logs, Adherence to Exercise, Exercise Performance, and Adverse Event Reporting | Body lean mass: + (p = 0.039) Predominantly trunk: + (p = 0.02) affected-side limbs: + (p = 0.04), VO2VT: + (p = 0.046) Muscular strength: + (p < 0.03) Both groups yielded similar and significant improvements: 6 MWT: X (p = 0.8) VO2peak: X (p = 0.9) Sit-to-stand time: X (p = 0.05), Stair climb performance: X (p = 0.97) |
| Jong et al. (2013) [22] | 46 participants (23, 23) Age: 57.2 Time since stroke : 43 days | Multidisciplinary stroke rehabilitation (Cyclic neuromuscular electrical stimulation (NMES)) Duration: 45 min Frequency: 2 times/wk (16 sessions) | Functional (passive) | Sham stretch positioning procedure + simultaneous sham conventional TENS | ROM Pain in the hemiplegic shoulder: Shoulder Q | Passive range of motion: X (p = 0.217) No significant difference between the groups (r2 = 1.53, p = 0.217 |
| Hung et al. (2019) [23] | 68 participants (20, 10) Age: 55.54 Time since stroke : 23 months | Robot-assisted therapy (RT) BMT robot vs. IMT robot Duration: 90–100 min Frequency: 5 times/wk (20 sessions) | Functional (passive) | Individualized occupational therapy | FMA-UE Muscle spasticity: MAS Quality of movement: MAL Muscle strength of the affected arm: MRC | FMA-UE: IMT > BMT (p < 0.01) MAS: IMT + (p = 0.01), BMT X (p = 0.55) CT X (p = 0.44) MAL: IMT + (p = 0.01) BMT X (p = 0.55) CT X (p = 0.44) MRC: IMT X (p = 0.27) BMT + (p = 0.01) CT: X (p = 0.3) |
| Hsieh et al. (2018) [24] | 44 participants (32, 12) Age: 54 Time since stroke : 21 months | Robot-assisted therapy (RT) P-IMT vs. D-IMT Duration: 90–100 min Frequency: 5 times/wk (20 sessions) | Functional (passive) | Conventional rehabilitation +FTP | FMA-UE Muscle spasticity: MAS Quality of movement: MAL Muscle strength of the affected arm: MRC Wrist-worn accelerometers | Total MRC: D-IMT > P-IMT, CT (p = 0.04, p = 0.04) FMA:X (p = 0.77), proximal FMA: X (p = 0.97), proximal MRC: X (p = 0.12) * Distal upper-limb robotic rehabilitation using the D-IMT had superior effects on distal muscle strengthen |
| Patten et al. (2013) [25] | 19 participants (9, 10) Age: 68 Time since stroke : 12 months | HYBRID (combined Functional Training Practice + Power training) Duration: 75 min Frequency: 5 times/wk (24 sessions) | Resistance (isokinetic) Functional | * Crossover design G1: FTP→HYBRID G2: HYBRID→FTP | FMA-UE the Ashworth Scale WMFT-FAS Functional Independence Measure: FIM | WMFT-FAS: HYBRID > FTP (p < 0.05) Treatment order: X (p = 0.43) FMA: X (p > 0.05) FIM: + (HYB > FTP, p < 0.05) Ashworth score: X (p > 0.05) |
| Chae et al. (2020) [26] | 23 participants (17, 6) Age: 61.4 Time since stroke : at least 6 months | Smart watch based Home-based rehabilitation Duration: 30 min Frequency: 12 weeks | Functional | Tele-rehabilitation service | FMA-UE WMFT-FAS Grip power ROM BDI: Beck Depression Inventory | WMAFT: + (p = 0.02) Grip power: X (p = 0.46) FMA-UE: X (p = 0.34) ROM: flexion: + (p < 0.001) Extension: X (p = 0.16) Internal rotation: + (p = 0.001) External rotation: X (p = 0.2) |
| Corti et al. (2012) [27] | 14 participants (14) Age: 59.8 Time since stroke : 15 weeks | Dynamic resistance training (POWER) vs. Functional task practice (FTP) Duration: 90 min Frequency: 3 days/wk (30 sessions) | Resistance (isokinetic) Functional | * Crossover design (10 week+10 week) Order1: FTP→POWER Order2: POWER→FTP | UEFMMS the Ashworth Scale European Stroke Scale CMHAI Kinematics of functional reach to grasp | Treatment effect (FTP vs. POWER): X (both groups improved without differential treatment effects) Treatment order: X (p > 0.05) Period effect: X (p > 0.05) Kinematic: Treatment effect: POWER > FTP Treatment order: G2 > G1 |
| Annino et al. (2019) [28] | 37 participants (19, 18) Age: 68.6 Time since stroke : null | Supervised physical therapy + Segmental muscle vibration (SPT-SMV) Duration: 30 min Frequency: 3 days/wk (24 sessions) | Functional (passive) | Supervised physical therapy (SPT) | Barthel index (BI) the Ashworth Scale (MAS) Manual muscle testing (MMT) ROM | Both groups improved in BI, Elbow ROM, Elbow muscles strength Muscle tone in elbow joint improved only in SPT-SMV (p = 0.008) |
| Han et al. (2012) [29] | 32 participants (11, 10, 11) Age: 50.2 Time since stroke : 38–42 days | Different intensities of arm rehabilitation training (correct positioning and carrying of the arm; passive, assisted and active movements; strength training; practice of functional activities) Duration: G1: 1 h/G2: 2 h/G3: 3 h Frequency: 5 days/wk (30 sessions) | Resistance (isotonic) Functional (passive) | 1 h (group A) 2 h (group B) 3 h (group C) | FMA-UE ARAT (Action Research Arm Test) Barthel index (BI) | FMA and ARAT: Group C > A, B (p < 0.05) BI: X (p > 0.05). |
| Linder et al. (2020) [30] | 43 participants (16, 14, 13) Age: 56 Time since stroke : 13 months | G1: Forced aerobic exercise (60% to 80% of their heartrate reserve) + repetitive task practice (FE + RTP) G2: Voluntary aerobic exercise + RTP (VE + RTP) Duration: 90 min Frequency: 3 times/wk (24 sessions) | Aerobic Functional (passive) | G3: RTP only | 6 MWT | 6 MWT: G1: + (p < 0.001) G2: + (p < 0.001) G3: X (p = 0.21) |
| Emmerson et al. (2017) [31] | 62 participants (30, 32) Age: 66 Time since stroke : 4 months | Home exercise video on smart technology and automated reminders (stretching, strengthening, fine motor/coordination) Duration & Frequency depended on the participants (average 38 min/day) | Functional (passive) | Paper-based home exercise program | Adherence WMFT Satisfaction | Adherence: X (p > 0.05) WMFT: X (p > 0.05) Satisfaction: X (p > 0.05) * smart technology was not superior to standard paper-based |
| Topcuoglu et al. (2015) [32] | 40 participants (20, 20) Age: 65.95 Time since stroke : 3.5 months | Upper extremity aerobic exercise (UEAE) (arm crank ergometry) Duration: 30 min Frequency: 5 days/wk (20 sessions) | Aerobic | Conventional physiotherapy | CPRS clinical determinants Functional independence measure (FIM) Nottingham Health Profile (NHP) Beck Depression Scale scores (BDS) | FIM sub scores (motor and cognitive): + (p > 0.05) NHP: + (p > 0.005) BDS: + (p = 0.005) Clinical determinants: significant pain relief and decline in signs and symptom |
| Jung et al. (2019) [33] | 36 participants (18, 18) Age: 58.5 Time since stroke : 28.65 days | Active shoulder exercise with a sling suspension system Duration: 40 min Frequency: 5 days/wk (20 sessions) | Resistance (isometric) | Bilateral arm training | Shoulder subluxation distance Shoulder proprioception FMA-UE the manual function test (MFT) | Subluxation: + (p = 0.001) Proprioception: + (p = 0.046) FMA: + (p = 0.002) MFT: + (p = 0.007) |
| Kerimov et al. (2021) [34] | 24 participants (12, 12) Age: 54.3 Time since stroke : at least 6 months | Isokinetic training in paretic upper extremity Duration: 40 min Frequency: 3 days/wk (12 sessions) | Resistance (isokinetic) | Tailored strengthening exercises with exercise bands | Isokinetic peak torque FMA-UE Stroke Impact Scale (SIS) Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire Grip strength Peak isometric strength | SIS: isokinetic group had higher scores on nearly every domain Extensor peak torque at 60°: + (p = 0.007) Extensor peak isometric muscle strength: + (p = 0.007) DASH after 4weeks after the end of treatment: + (p = 0.014) Grip strength: X (p > 0.05) |
| Pinheiro et al. (2021) [35] | 20 participants (10, 10) Age: 66.2 Time since stroke : null (Acute) | Upper limb cycle ergometer (ULCE) Duration: 20 min Frequency: 5 days/wk (20 sessions) | Aerobic | Conventional physiotherapy | Upper limb strength and grip Trunk impairment scale (TIS) Level of independence: Modified Rankin scale (MRS) | ULCE: all variables showed Superior (p = 0.005) TIS: + (p < 0.001) MRS: + (p < 0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.E.; Choi, M.; Jeoung, B. Effectiveness of Rehabilitation Exercise in Improving Physical Function of Stroke Patients: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 12739. https://doi.org/10.3390/ijerph191912739
Lee KE, Choi M, Jeoung B. Effectiveness of Rehabilitation Exercise in Improving Physical Function of Stroke Patients: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(19):12739. https://doi.org/10.3390/ijerph191912739
Chicago/Turabian StyleLee, Kyung Eun, Muncheong Choi, and Bogja Jeoung. 2022. "Effectiveness of Rehabilitation Exercise in Improving Physical Function of Stroke Patients: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 19: 12739. https://doi.org/10.3390/ijerph191912739