
Using a Taxonomy to Systematically Identify and Describe Self-Management Interventions Components in Randomized Trials for COPD
 , , , , , , ,
, , , , , , ,  , , , , , , , add
Show full author list
, , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Literature Search
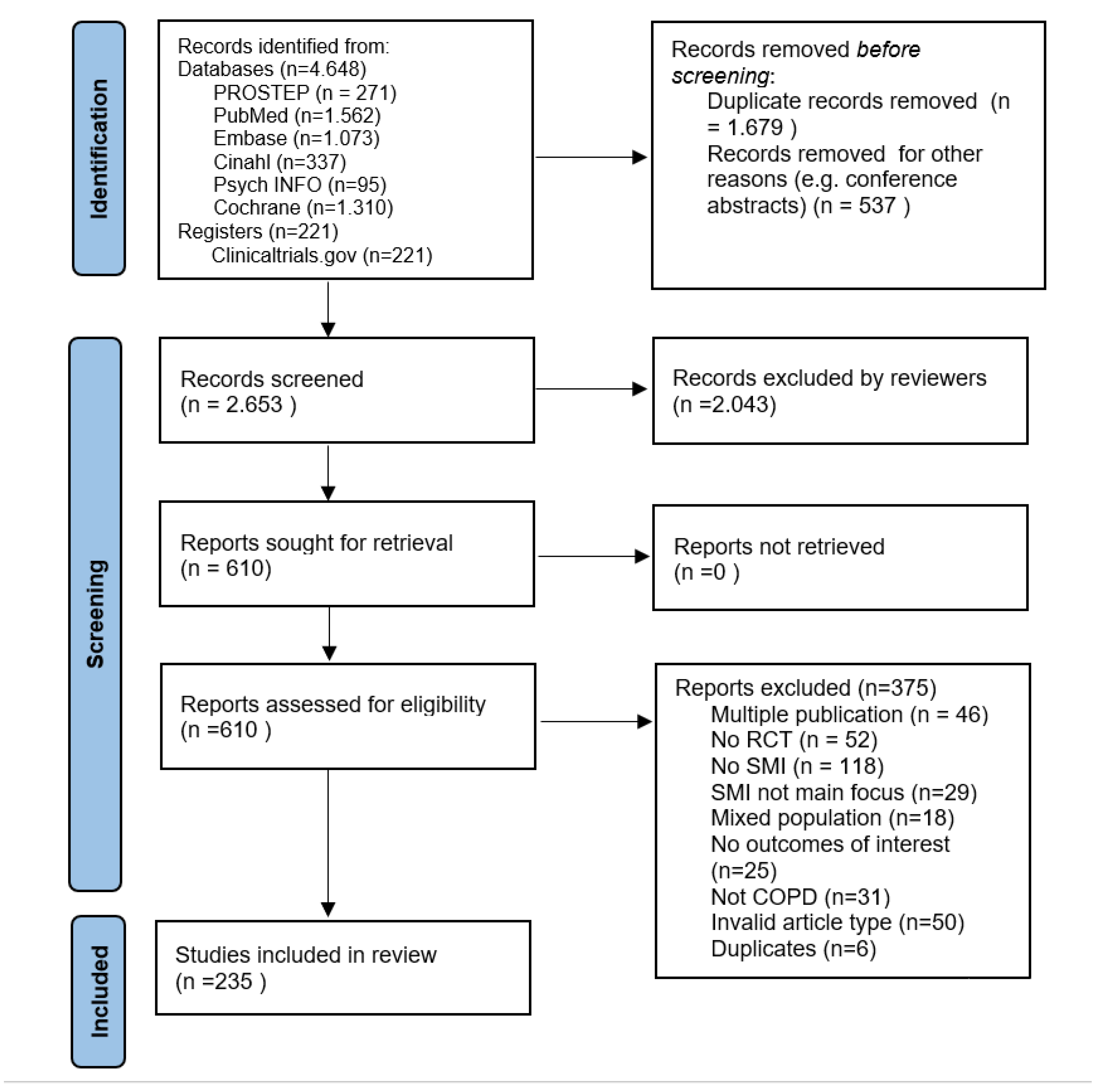
2.2. Screening and Selection Process
2.3. Data Extraction and Synthesis
2.4. Data Analysis
3. Results
3.1. Included Studies
3.2. Key Characteristics of Included Studies
3.3. Usual Care Arms
3.4. Intervention Arms
3.4.1. Expected Patient or Carer Self-Management Behaviours
3.4.2. Reported Intervention Characteristics
- Self-management support techniques
- Mode of delivery and setting
- Duration, intensity, and follow-up
3.4.3. Outcomes
3.4.4. Target Population Characteristics
3.4.5. Risk of Bias in Included Studies
4. Discussion
4.1. Summary of Evidence
4.2. Limitations and Strengths
4.3. Our results in the Context of Previous Research
4.4. Implications for Practice and Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Search | Query | Items found |
| #3 | #1 AND #2 AND #3 Filters: Publication date from 2010/01/01 | 1562 |
| #4 | #1 AND #2 AND #3 | 2787 |
| #3 | (“Clinical Trials as Topic”[Mesh] OR “Randomized Controlled Trial” [pt] OR “Controlled Clinical Trial” [pt] OR randomized [tiab] OR randomly[tiab] OR placebo[tiab] OR trial[ti]) NOT (animals[mh] NOT humans[mh]) | 1,167,356 |
| #2 | “Self Care”[Mesh] OR “Self-Management”[Mesh] OR “Power (Psychology)”[Mesh] OR “Health Education”[Mesh] OR “Patient Participation”[Mesh] OR “Decision Making”[Mesh] OR “Telemedicine”[Mesh] OR self-administration*[tiab] OR self-care[tiab] OR self efficac*[tiab] OR self-manag*[tiab] OR selfmanag*[tiab] OR self-monitor*[tiab] OR selfmonitor*[tiab] OR self-diagnos*[tiab] OR selfdiagnos*[tiab] OR self-assess*[tiab] OR selfassess*[tiab] OR self-direct*[tiab] OR selfdirect*[tiab] OR self-help*[tiab] OR empower*[tiab] OR enablement[tiab] OR health education[tiab] OR patient education[tiab] OR patient participation[tiab] OR coach*[tiab] OR health promot*[tiab] OR ((community[tiab] OR peer[tiab]) AND (support*[tiab] OR advice*[tiab] OR monitor*[tiab] OR train*[tiab] OR instruction*[tiab] OR intervention*[tiab] OR consult*[tiab] OR assist*[tiab] OR educat*[tiab] OR information*[tiab] OR skill*[tiab])) OR group support*[tiab] OR group intervention*[tiab] OR group advice*[tiab] OR group monitor*[tiab] OR group train*[tiab] OR training group*[tiab] OR group instruct*[tiab] OR group assist*[tiab] OR group educat*[tiab] OR group inform*[tiab] OR group skill*[tiab] OR ((patient[tiab] OR patients[tiab]) AND (centered[tiab] OR centred[tiab] OR focus*[tiab] of directed[tiab] OR coach*[tiab] OR engage*[tiab] OR involve*[tiab] OR orient*[tiab] OR participat*[tiab])) OR ((patient[tiab] OR patients[tiab]) AND (educat*[tiab] OR train*[tiab] OR instruct*[tiab] OR teach*[tiab])) OR (management*[tiab] AND (plan[tiab] OR program*[tiab] OR disease[tiab])) OR (symptom*[tiab] AND (management[tiab] OR directed[tiab] OR focus*[tiab])) OR ((personalized[tiab] OR personalized[tiab]) AND care[tiab]) OR telemedicine[tiab] OR eHealth[tiab] OR e-Health[tiab] OR mHealth[tiab] OR m-Health[tiab] OR shared decision*[tiab] OR sharing decision*[tiab] OR informed decision*[tiab] OR informed choice*[tiab] or decision aid*[tiab] OR ((share*[ti] OR sharing*[ti] OR informed*[ti]) AND (decision*[ti] OR deciding*[ti] OR choice*[ti])) | 1,904,809 |
| #1 | “Pulmonary Disease, Chronic Obstructive”[Mesh] OR COPD[tiab] OR obstructive lung disease*[tiab] OR obstructive pulmonary disease*[tiab] OR acute exacerbation*[tiab] OR AECB[tiab] OR restrictive lung disease*[tiab] OR chronic pulmonary obstructive disease*[tiab] OR COAD[tiab] OR chronic obstructive airway disease*[tiab] | 85,951 |
| Search | Query | Items found |
| #6 | #5 NOT (‘chapter’/it OR ‘conference abstract’/it OR ‘conference review’/it OR ‘editorial’/it OR ‘letter’/it OR ‘note’/it OR ‘short survey’/it) | 1073 |
| #5 | #1 AND #2 AND #3 AND [2010–2019]/py | 1494 |
| #4 | #1 AND #2 AND #3 | 1995 |
| #3 | (‘clinical trial (topic)’/exp OR randomized:ab,ti,kw OR randomly:ab,ti,kw OR placebo:ab,ti,kw OR trial:ti) NOT ([animals]/lim NOT [humans]/lim) | 1,267,704 |
| #2 | ‘self care’/exp OR ‘coping behaviour’/exp OR ‘drug self administration’/exp OR ‘self monitoring’/exp OR ‘empowerment’/exp OR ‘health education’/exp OR ‘patient participation’/exp OR ‘shared decision making’/exp OR ‘telehealth’/exp OR ‘self administration*’:ab,ti,kw OR ‘self care’:ab,ti,kw OR ‘self efficac*’:ab,ti,kw OR ‘self manag*’:ab,ti,kw OR selfmanag*:ab,ti,kw OR ‘self monitor*’:ab,ti,kw OR selfmonitor*:ab,ti,kw OR ‘self diagnos*’:ab,ti,kw OR selfdiagnos*:ab,ti,kw OR ‘self assess*’:ab,ti,kw OR selfassess*:ab,ti,kw OR ‘self direct*’:ab,ti,kw OR selfdirect*:ab,ti,kw OR ‘self help*’:ab,ti,kw OR empower*:ab,ti,kw OR enablement:ab,ti,kw OR ‘health education’:ab,ti,kw OR ‘patient education’:ab,ti,kw OR ‘patient participation’:ab,ti,kw OR coach*:ab,ti,kw OR ‘health promot*’:ab,ti,kw OR (((group OR peer) NEAR/3 (support* OR advice* OR monitor* OR intervention* OR train* OR instruction* OR consult* OR assist* OR educat* OR information* OR skill*)):ab,ti,kw) OR (((patient OR patients) NEAR/3 (centered OR centred OR focus* OR directed OR coach* OR engage* OR involve* OR orient* OR participat*)):ab,ti,kw) OR (((patient OR patients) NEAR/3 (educat* OR train* OR instruct* OR teach*)):ab,ti,kw) OR ((management* NEAR/3 (plan OR program* OR disease)):ab,ti,kw) OR ((symptom* NEAR/3 (management OR directed OR focus*)):ab,ti,kw) OR (((personalized OR personalized) NEAR/3 care):ab,ti,kw) OR telemedicine:ab,ti,kw OR ehealth:ab,ti,kw OR ‘e health’:ab,ti,kw OR mhealth:ab,ti,kw OR ‘m health’:ab,ti,kw OR ‘shared decision*’:ab,ti,kw OR ‘sharing decision*’:ab,ti,kw OR ‘informed decision*’:ab,ti,kw OR ‘informed choice*’:ab,ti,kw OR ‘decision aid*’:ab,ti,kw OR (((share* OR sharing* OR informed*) NEAR/3 (decision* OR deciding* OR choice*)):ab,ti,kw) | 972,108 |
| #1 | ‘chronic obstructive lung disease’/exp OR (obstructive NEAR/3 (lung OR pulmonary OR airway) NEAR/3 disease*):ab,ti,kw OR ‘acute exacerbation*’:ab,ti,kw OR AECB:ab,ti,kw OR ‘restrictive lung disease*’:ab,ti,kw OR COAD:ab,ti,kw | 136,078 |
| Search | Query | Items found |
| S5 | S1 AND S2 AND S3 Limiters—Publication Year: 2010–2018 | 95 |
| S4 | S1 AND S2 AND S3 | 153 |
| S3 | DE “Clinical Trials” OR TI (randomized OR randomly OR placebo OR trial) OR AB (randomized OR randomly OR placebo) OR KW (randomized OR randomly OR placebo OR trial) NOT (PO Animal NOT PO Human) | 165,282 |
| S2 | DE (“Self-Care Skills” OR “Self-Efficacy” OR “Drug Self Administration” OR “Coping Behavior” OR “Empowerment” OR “Telemedicine” OR “Health Education” OR “Health Promotion” OR “Client Participation”) OR TI (“self administration*” OR “self care” OR “self efficac*” OR “self manag*” OR selfmanag* OR “self monitor*” OR selfmonitor* OR “self diagnos*” OR selfdiagnos* OR “self assess*” OR selfassess* OR “self direct*” OR selfdirect* OR “self help*” OR empower* OR enablement OR “health education” OR “patient education” OR “patient participation” OR coach* OR “health promot*” OR (((group OR peer) N3 (support* OR advice* OR monitor* OR intervention* OR train* OR instruction* OR consult* OR assist* OR educat* OR information* OR skill*))) OR (((patient OR patients) N3 (centered OR centred OR focus* OR directed OR coach* OR engage* OR involve* OR orient* OR participat*))) OR (((patient OR patients) N3 (educat* OR train* OR instruct* OR teach*))) OR ((management* N3 (plan OR program* OR disease))) OR ((symptom* N3 (management OR directed OR focus*))) OR (((personalized OR personalized) N3 care)) OR telemedicine OR ehealth OR “e health” OR mhealth OR “m health” OR “shared decision*” OR “sharing decision*” OR “informed decision*” OR “informed choice*” OR “decision aid*” OR (((share* OR sharing* OR informed*) N3 (decision* OR deciding* OR choice*))) OR AB (“self administration*” OR “self care” OR “self efficac*” OR “self manag*” OR selfmanag* OR “self monitor*” OR selfmonitor* OR “self diagnos*” OR selfdiagnos* OR “self assess*” OR selfassess* OR “self direct*” OR selfdirect* OR “self help*” OR empower* OR enablement OR “health education” OR “patient education” OR “patient participation” OR coach* OR “health promot*” OR (((group OR peer) N3 (support* OR advice* OR monitor* OR intervention* OR train* OR instruction* OR consult* OR assist* OR educat* OR information* OR skill*))) OR (((patient OR patients) N3 (centered OR centred OR focus* OR directed OR coach* OR engage* OR involve* OR orient* OR participat*))) OR (((patient OR patients) N3 (educat* OR train* OR instruct* OR teach*))) OR ((management* N3 (plan OR program* OR disease))) OR ((symptom* N3 (management OR directed OR focus*))) OR (((personalized OR personalized) N3 care)) OR telemedicine OR ehealth OR “e health” OR mhealth OR “m health” OR “shared decision*” OR “sharing decision*” OR “informed decision*” OR “informed choice*” OR “decision aid*” OR (((share* OR sharing* OR informed*) N3 (decision* OR deciding* OR choice*))) OR KW (“self administration*” OR “self care” OR “self efficac*” OR “self manag*” OR selfmanag* OR “self monitor*” OR selfmonitor* OR “self diagnos*” OR selfdiagnos* OR “self assess*” OR selfassess* OR “self direct*” OR selfdirect* OR “self help*” OR empower* OR enablement OR “health education” OR “patient education” OR “patient participation” OR coach* OR “health promot*” OR (((group OR peer) N3 (support* OR advice* OR monitor* OR intervention* OR train* OR instruction* OR consult* OR assist* OR educat* OR information* OR skill*))) OR (((patient OR patients) N3 (centered OR centred OR focus* OR directed OR coach* OR engage* OR involve* OR orient* OR participat*))) OR (((patient OR patients) N3 (educat* OR train* OR instruct* OR teach*))) OR ((management* N3 (plan OR program* OR disease))) OR ((symptom* N3 (management OR directed OR focus*))) OR (((personalized OR personalized) N3 care)) OR telemedicine OR ehealth OR “e health” OR mhealth OR “m health” OR “shared decision*” OR “sharing decision*” OR “informed decision*” OR “informed choice*” OR “decision aid*” OR (((share* OR sharing* OR informed*) N3 (decision* OR deciding* OR choice*))) | 410,566 |
| S1 | DE “Chronic Obstructive Pulmonary Disease” OR TI (obstructive N3 (lung OR pulmonary OR airway) N3 disease*) OR “acute exacerbation*” OR AECB OR “restrictive lung disease*” OR COAD) OR AB (obstructive N3 (lung OR pulmonary OR airway) N3 disease*) OR “acute exacerbation*” OR AECB OR “restrictive lung disease*” OR COAD) OR KW (obstructive N3 (lung OR pulmonary OR airway) N3 disease*) OR “acute exacerbation*” OR AECB OR “restrictive lung disease*” OR COAD) | 2794 |
| Search | Query | Items found |
| S5 | S1 AND S2 AND S3 Limiters—Publication Year: 2010–2018, academic journals | 337 |
| S4 | S1 AND S2 AND S3 | 668 |
| S3 | MH “Clinical Trials+” OR TI (randomized OR randomly OR placebo OR trial) OR AB (randomized OR randomly OR placebo) NOT (MH “Animals” NOT MH “Human) | 377,931 |
| S2 | MH (“Self Care+” OR “Self-Efficacy” OR “Coping” OR”Empowerment” OR “Telehealth+”) OR “Health Education” OR “Consumer Participation”) OR TI (“self administration*” OR “self care” OR “self efficac*” OR “self manag*” OR selfmanag* OR “self monitor*” OR selfmonitor* OR “self diagnos*” OR selfdiagnos* OR “self assess*” OR selfassess* OR “self direct*” OR selfdirect* OR “self help*” OR empower* OR enablement OR “health education” OR “patient education” OR “patient participation” OR coach* OR “health promot*” OR (((group OR peer) N3 (support* OR advice* OR monitor* OR intervention* OR train* OR instruction* OR consult* OR assist* OR educat* OR information* OR skill*))) OR (((patient OR patients) N3 (centered OR centred OR focus* OR directed OR coach* OR engage* OR involve* OR orient* OR participat*))) OR (((patient OR patients) N3 (educat* OR train* OR instruct* OR teach*))) OR ((management* N3 (plan OR program* OR disease))) OR ((symptom* N3 (management OR directed OR focus*))) OR (((personalized OR personalized) N3 care)) OR telemedicine OR ehealth OR “e health” OR mhealth OR “m health” OR “shared decision*” OR “sharing decision*” OR “informed decision*” OR “informed choice*” OR “decision aid*” OR (((share* OR sharing* OR informed*) N3 (decision* OR deciding* OR choice*))) OR AB (“self administration*” OR “self care” OR “self efficac*” OR “self manag*” OR selfmanag* OR “self monitor*” OR selfmonitor* OR “self diagnos*” OR selfdiagnos* OR “self assess*” OR selfassess* OR “self direct*” OR selfdirect* OR “self help*” OR empower* OR enablement OR “health education” OR “patient education” OR “patient participation” OR coach* OR “health promot*” OR (((group OR peer) N3 (support* OR advice* OR monitor* OR intervention* OR train* OR instruction* OR consult* OR assist* OR educat* OR information* OR skill*))) OR (((patient OR patients) N3 (centered OR centred OR focus* OR directed OR coach* OR engage* OR involve* OR orient* OR participat*))) OR (((patient OR patients) N3 (educat* OR train* OR instruct* OR teach*))) OR ((management* N3 (plan OR program* OR disease))) OR ((symptom* N3 (management OR directed OR focus*))) OR (((personalized OR personalized) N3 care)) OR telemedicine OR ehealth OR “e health” OR mhealth OR “m health” OR “shared decision*” OR “sharing decision*” OR “informed decision*” OR “informed choice*” OR “decision aid*” OR (((share* OR sharing* OR informed*) N3 (decision* OR deciding* OR choice*))) | 473,148 |
| S1 | (MH “Pulmonary Disease, Chronic Obstructive+”) OR TI (obstructive N3 (lung OR pulmonary OR airway) N3 disease*) OR “acute exacerbation*” OR AECB OR “restrictive lung disease*” OR COAD) OR AB (obstructive N3 (lung OR pulmonary OR airway) N3 disease*) OR “acute exacerbation*” OR AECB OR “restrictive lung disease*” OR COAD) | 22,225 |
| Search | Query | Items found |
| #4 | #3 Limits Publication Year from 2010 to 2018, with Cochrane Library publication date from Jan 2010 to Dec 2018, | 1531 |
| #3 | #1 AND #2 | 2379 |
| #2 | (self NEXT administration* OR self NEXT care OR self NEXT efficac* OR self NEXT manag* OR selfmanag* OR self NEXT monitor* OR selfmonitor* OR self NEXT diagnos* OR selfdiagnos* OR self NEXT assess* OR selfassess* OR self NEXT direct* OR selfdirect* OR self NEXT help* OR empower* OR enablement OR health NEXT education OR patient NEXT education OR patient NEXT participation OR coach* OR health NEXT promot*):ti,ab,kw OR ((group OR peer) NEAR/3 (support* OR advice* OR monitor* OR intervention* OR train* OR instruction* OR consult* OR assist* OR educat* OR information* OR skill*)):ti,ab,kw OR ((patient OR patients) NEAR/3 (centered OR centred OR focus* OR directed OR coach* OR engage* OR involve* OR orient* OR participat*)):ti,ab,kw OR ((patient OR patients) NEAR/3 (educat* OR train* OR instruct* OR teach*)):ti,ab,kw OR (management* NEAR/3 (plan OR program* OR disease)):ti,ab,kw OR (symptom* NEAR/3 (management OR directed OR focus*)):ti,ab,kw OR ((personalized OR personalized) NEAR/3 care):ti,ab,kw OR (telemedicine OR ehealth OR “e-health” OR mhealth OR “m-health” OR shared NEXT decision* OR sharing NEXT decision* OR informed NEXT decision* OR informed NEXT choice* OR decision NEXT aid*):ti,ab,kw OR ((share* OR sharing* OR informed*) NEAR/3 (decision* OR deciding* OR choice*)):ti,ab,kw OR (self NEXT administration* OR self NEXT care OR self NEXT efficac* OR self NEXT manag* OR selfmanag* OR self NEXT monitor* OR selfmonitor* OR self NEXT diagnos* OR selfdiagnos* OR self NEXT assess* OR selfassess* OR self NEXT direct* OR selfdirect* OR self NEXT help* OR empower* OR enablement OR health NEXT education OR patient NEXT education OR patient NEXT participation OR coach* OR health NEXT promot*):ti,ab,kw OR ((group OR peer) NEAR/3 (support* OR advice* OR monitor* OR intervention* OR train* OR instruction* OR consult* OR assist* OR educat* OR information* OR skill*)):ti,ab,kw OR ((patient OR patients) NEAR/3 (centered OR centred OR focus* OR directed OR coach* OR engage* OR involve* OR orient* OR participat*)):ti,ab,kw OR ((patient OR patients) NEAR/3 (educat* OR train* OR instruct* OR teach*)):ti,ab,kw OR (management* NEAR/3 (plan OR program* OR disease)):ti,ab,kw OR (symptom* NEAR/3 (management OR directed OR focus*)):ti,ab,kw OR ((personalized OR personalized) NEAR/3 care):ti,ab,kw OR (telemedicine OR ehealth OR “e-health” OR mhealth OR “m-health” OR shared NEXT decision* OR sharing NEXT decision* OR informed NEXT decision* OR informed NEXT choice* OR decision NEXT aid*):ti,ab,kw OR ((share* OR sharing* OR informed*) NEAR/3 (decision* OR deciding* OR choice*)):ti,ab,kw | 120,972 |
| #1 | (obstructive NEAR/3 (lung OR pulmonary OR airway) NEAR/3 disease*) OR acute NEXT exacerbation* OR AECB OR restrictive NEXT lung NEXT disease* OR COAD:ti,ab,kw | 13,914 |
Appendix B
| Inclusion Criteria | Considerations |
| The article should be written in English or Spanish. Invalid article types such as study proposals or designs as well as dissertations should be excluded. |
| If at the full-text assessment or data extraction phase you encounter a study labelled as quasi-random, quasi-randomized, or quasi-experimental, please:
|
| |
| At least 80% of the sample should have one of these diagnoses. In case of mixed populations: If the study population is mixed, outcomes should be reported by disease and not for the mixed population only. Pregnant women are excluded |
| |
Self-management is defined as “what individuals, families and communities do with the intention to promote, maintain, or restore health and to cope with illness and disability with or without the support of health professionals. It includes but is not limited to self-prevention, self-diagnosis, self-medication and self-management of illness and disability...”.). Self-management interventions SMIs are systematically provided by healthcare staff or other patients or lay persons to increase patients’ skills and confidence in managing their chronic condition. SMIs aim to equip patients (and their informal caregivers whenever appropriate) to actively participate in the management of their chronic condition. | |
| If the self-management intervention is not the more central component, it is just one of many other components → exclude study. For example, if an intervention is introducing a disease management program, which includes elements of SMI but has stronger component of organizational change, it should be EXCLUDED. If the self-management intervention is compared with other components but outcomes are reported separately, it should be included. For example, if in a case of disease management program the authors independently analyse the effectiveness of the SM components, the study can be included. |
|
Appendix C

{kind=link}
{kind=link}
{kind=link}
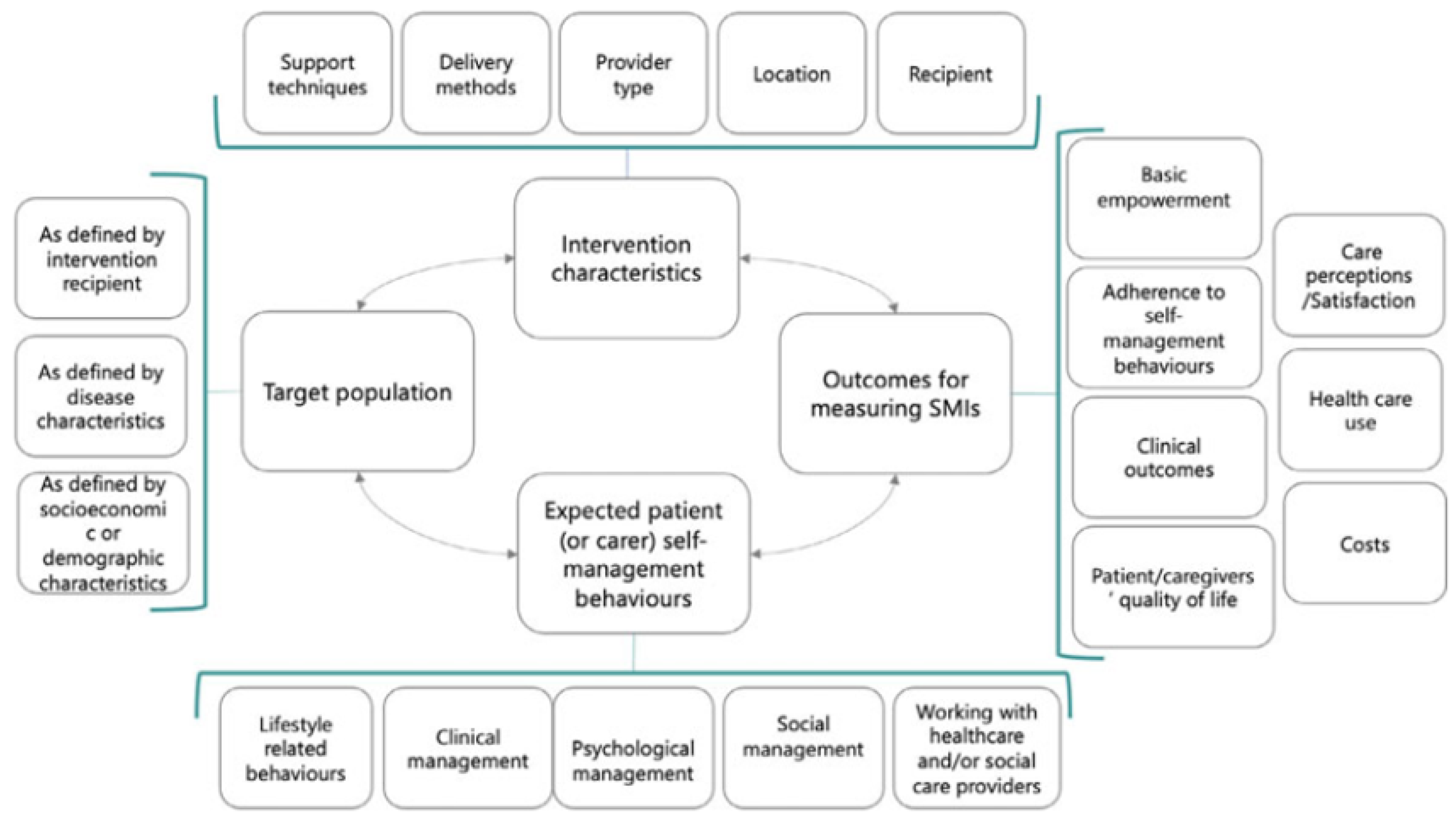
| Domain 1: Self-Management Intervention Characteristics | |
|---|---|
| Subdomains | Ingredients |
| 1.1 Support techniques | Sharing information, Skills training, Stress and/or emotional management, Shared decision-making, Goal setting and action planning, Enhancing problem solving skills, Self-monitoring training and feedback, Using prompts and reminders, Encouraging use of services, Providing equipment, Social support, Coaching, and motivational interviewing |
| 1.2 Support delivery methods | Set of five subdomains |
| 1.2.1 Type of encounter | Clinical visit, Support session, Self-guided intervention |
| 1.2.2 Support delivery mode | Face-to-face intervention, Distance/remote intervention, Phone (calls only), Smartphone, Internet, Specific devices |
| 1.2.3 Time of communication | Synchronous–Asynchronous |
| 1.2.4 Recipient | Individual, Group, Specific population |
| 1.2.5 Type of provider | Physician–Nurse–Pharmacist–Physiotherapist–Occupational therapist–Social worker–Psychologist -Dietician/nutritionist–Healthcare Assistant–Peer-Lay Person–Service |
| 1.3 Location | Hospital, Long-term care centre/nursing home, Community-based care, Home, Primary care centre, Outpatient Setting, Workplace |
| Domain 2: Expected patient (or caregiver) self-management behaviours | |
| 2.1 Lifestyle-related behaviours | Eating behaviours, Physical activity/exercise, Smoking cessation or reduction, Cessation or reduction of the consumption of alcohol or other harmful substances, Healthy sleep habits |
| 2.2 Clinical management | Disease-specific behaviours, Self-monitoring, Medication use and adherence, Early recognition of symptoms, Asking for professional help or emergency care when needed, Device Management, Physical management |
| 2.3 Psychological management | Handling/managing emotions |
| 2.4 Social Management | Fitting in at work, Social Roles, Being able to work |
| 2.5 Working with healthcare and/or social care providers | Communicating with healthcare and/or social care providers |
| Domain 3: Outcomes to measure the effect of a self-management intervention | |
| 3.1 Basic empowerment components | Level of knowledge, Level of health literacy, Level of skill acquisition, Level of self-efficacy, Level of patient activation |
| 3.2 Level of adherence to expected self-management behaviours | Lifestyle-related behaviours, Clinical self-management behaviours, Psychological self-management behaviours, Social self-management behaviours, Interactions and communication with healthcare and/or social care providers |
| 3.3 Clinical outcomes | Disease progression (clinical markers, symptoms), Complications, Adverse Events, Mortality |
| 3.4 Patient and informal caregivers’ quality of life | Overall quality of life, Physical functioning, Psychological and emotional role functioning, Social functioning, Sexual functioning, Burden of treatment |
| 3.5 Perceptions of and/or satisfaction with care | Overall satisfaction with self-management intervention, Perception of being well and sufficiently informed (quality of information provision), Perception of patient–provider relationship, Personalized care |
| 3.6 Healthcare use | Type and number of visits, hospital admissions and readmissions, emergency care |
| 3.7 Cost | Healthcare costs for patient, healthcare costs, direct non-medical costs, societal costs |
| Domain 4: Target population | |
| 4.1 As defined by intervention recipient | Patients, informal caregivers, or family caregivers |
| 4.2 As defined by disease-related characteristics | Time since diagnosis, disease severity, comorbidity, and multimorbidity |
| 4.3 As defined by socioeconomic or demographic characteristics | Socioeconomic status, cultural group, health literacy, digital literacy, biological sex or gender, age, living situation |
Appendix D
| Outcome (COS) | Definition |
| Knowledge | Relates to knowledge about COPD in general and COPD self-management, or the way care for COPD is organized and this both for patients and their social network. |
| Self-efficacy | A person’s belief that s/he is capable of doing something, often related to a specific goal s/he wants to achieve; feeling of confidence and of being in control. |
| Patient activation | The knowledge, skills, and confidence a person has on managing their own health and healthcare, including a feeling of being responsible for taking care of their own health. |
| Lung function | FEV1 |
| Mortality | |
| Taking medication or other treatment as advised (adherence) and adherence to regular visits | The extent to which a patient follows the prescribed treatment, such as taking medication as advised and following lifestyle advice, and extent of attending scheduled visits. |
| Smoking cessation | Stopping smoking (and/or smoking less). |
| COPD symptoms (short-term) | Extent of symptoms relief (in the short-term, including cough; breathlessness, among others). |
| Physical activity—muscle strength | Referral/participation in a pulmonary rehabilitation program: physical activity, physical activities, muscle strength linked with exercise capacity plus an overall support. |
| Sleep quality | Sleep quality contains interrupted sleep, sleep problems, sleep quality (as overall), and sleepiness. |
| Exacerbation | Increased breathlessness, mucus/phlegm/sputum production, and change in color of sputum and feeling out of breath. |
| Caregiver quality of life (including burden) | Caregiver quality of life and the burden that he/she feels from the caregiver’s tasks. |
| Activities of daily living: including sex life, social activities, and work (usual activities) | Being able to do usual activities, such as personal hygiene, housework, sex, managing finances, social activities, and work. |
| Coping with the disease, including depression and anxiety | How well a person feels able to cope/manage with stress or other difficulties caused by the disease, including depression and anxiety. |
| Number of emergency room visits and admissions | Number of visits to emergency department visits and hospital admissions. |
References
- GOLD. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease, 2020 Report. Available online: http://goldcopd.org/gold-reports/ (accessed on 3 July 2022).
- Brussele, G.J.; Joos, G.F.; Bracke, K.R. New insights into the immunology of chronic obstructive pulmonary disease. Lancet 2011, 378, 1015–1026. [Google Scholar] [CrossRef]
- WHO. Global Health Estimates 2020: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2019; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- López-Campos, J.L.; Tan, W.; Soriano, J.B. Global burden of COPD. Respirology 2016, 21, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Salvi, S.S.; Barnes, P.J. Chronic obstructive pulmonary disease non-smokers. Lancet 2009, 374, 733–743. [Google Scholar] [CrossRef]
- Wagg, K. Unravelling self-management for COPD: What next? Chron. Respir. Dis. 2012, 9, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Rogliani, P.; Ora, J.; Puxeddu, E.; Matera, M.G.; Cazzola, M. Adherence to COPD treatment: Myth and reality. Respir. Med. 2017, 129, 117–123. [Google Scholar] [CrossRef]
- Bryant, J.; McDonald, V.M.; Boyes, A.; Sanson-Fisher, R.; Paul, C.; Melville, J. Improving medication adherence in chronic obstructive pulmonary disease: A systematic review. Respir. Res. 2013, 14, 109. [Google Scholar] [CrossRef] [Green Version]
- Sriram, K.B.; Percival, M. Suboptimal inhaler medication adherence and incorrect technique are common among chronic obstructive pulmonary disease patients. Chron. Respir. Dis. 2016, 13, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Effing, T.W.; Vercoulen, J.H.; Bourbeau, J.; Trappenburg, J.; Lenferink, A.; Cafarella, P.; Coultas, D.; Meek, P.; Van Der Valk, P.; Bischoff, E.W. Definition of a COPD self-management intervention: International Expert Group consensus. Eur. Respir. J. 2016, 48, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Jonkman, N.H.; Westland, H.; Trappenburg, J.C.; Groenwold, R.H.H.; Bischoff, E.W.; Bourbeau, J.; Bucknall, C.E.; Coultas,, D.; Effing, T.W.; Epton, M.J.; et al. Do self-management interventions in COPD patients work and which patients benefit most? An individual patient data meta-analysis. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 2063–2074. [Google Scholar] [CrossRef] [Green Version]
- Effing, T.W.; Bourbeau, J.; Vercoulen, J.; Apter, A.J.; Coultas, D.; Meek, P.; Valk, P.V.; Partridge, M.R.; Palen, J.V. Self-management programmes for COPD: Moving forward. Chron Respir Dis. 2012, 9, 27–35. [Google Scholar]
- Van Hooft, S.M.; Been-Dahmen, J.M.J.; Ista, E.; van Staa, A.; Boeije, H.R. A realist review: What do nurse-led self-management interventions achieve for outpatients with a chronic condition? J. Adv. Nurs. 2017, 73, 1255–1271. [Google Scholar] [CrossRef] [PubMed]
- Newham, J.J.; Presseau, J.; Heslop-Marshall, K.; Russell, S.; Ogunbayo, O.J.; Netts, P.; Hanratty, B.; Kaner, E. Features of self-management interventions for people with COPD associated with improved health-related quality of life and reduced emergency department visits: A systematic review and meta-analysis. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 1705–1720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonsdottir, H. Self-management programmes for people living with chronic obstructive pulmonary disease: A call for a reconceptualization. J. Clin. Nurs. 2013, 22, 621–637. [Google Scholar] [CrossRef] [PubMed]
- Zwerink, M.; Brusse-Keizer, M.; van der Valk, P.D.; Zielhuis, G.A.; Monninkhof, E.M.; van der Palen, J.; Frith, P.A.; Effing, T. Self management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014, 3, CD002990. [Google Scholar] [CrossRef]
- Glasziou, P.; Chalmers, I.; Green, S.; Michie, S. Intervention synthesis: A missing link between a systematic review and practical treatment(s). PLoS Med. 2014, 11, e1001690. [Google Scholar] [CrossRef]
- Bastian, H.; Glasziou, P.; Chalmers, I. Seventy-five trials and eleven systematic reviews a day: How will we ever keep up? PLoS Med. 2010, 7, e1000326. [Google Scholar] [CrossRef]
- Glasziou, P.; Meats, E.; Heneghan, C.; Shepperd, S. What is missing from descriptions of treatment in trials and reviews? BMJ 2008, 336, 1472–1474. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, T.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, G.D.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.; Erueti, C.; Glasziou, P. Poor description of non-pharmacological interventions: Analysis of consecutive sample of randomized trials. BMJ 2013, 347, f3755. [Google Scholar] [CrossRef] [Green Version]
- Barlow, J.; Wright, C.; Sheasby, J.; Turner, A.; Hainsworth, J. Self-management approaches for people with chronic conditions: A review. Patient Educ. Couns. 2002, 48, 177–187. [Google Scholar] [CrossRef]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health. 2011, 26, 1479–1498. [Google Scholar] [CrossRef] [PubMed]
- Krumholz, H.M.; Currie, P.M.; Riegel, B.; Phillips, C.O.; Peterson, E.D.; Smith, R.; Yancy, C.W.; Faxon, D.P.; American Heart Association Disease Management Taxonomy Writing Group. A taxonomy for disease management: A scientific statement from the American Heart Association Disease Management Taxonomy Writing Group. Circulation 2006, 114, 1432–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; Whittington, C.; Hamoudi, Z.; Zarnani, F.; Tober, G.; West, R. Identification of behaviour change techniques to reduce excessive alcohol consumption. Addiction 2012, 107, 1431–1440. [Google Scholar] [CrossRef] [PubMed]
- Presseau, J.; Ivers, N.M.; Newham, J.J.; Knittle, K.; Danko, K.J.; Grimshaw, J.M. Using a behaviour change techniques taxonomy to identify active ingredients within trials of implementation interventions for diabetes care. Implement Sci. 2015, 10, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballester, M.; Orrego, C.; Heijmans, M.; Alonso-Coello, P.; Versteegh, M.M.; Mavridis, D.; Groene, O.; Immonen, K.; Wagner, C.; Canelo-Aybar, C.; et al. Comparing the effectiveness and cost-effectiveness of self-management interventions in four high-priority chronic conditions in Europe (COMPAR-EU): A research protocol. BMJ Open 2020, 10, e034680. [Google Scholar] [CrossRef] [Green Version]
- Orrego, C.; Ballester, M.; Heijmans, M.; Camus, E.; Groene, O.; Nino de Guzman, E.; Pardo-Hernandez, H.; Sunol, R.; COMPAR-EU Group. Talking the same language on patient empowerment: Development and content validation of a taxonomy of self-management interventions for chronic conditions. Health Expect. 2021, 24, 1626–1638. [Google Scholar] [CrossRef]
- Arritty, C.; Gartlehner, G.; Nussbaumer-Streit, B.; King, V.J.; Hamel, C.; Kamel, C.L.A.; Stevens, A. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J. Clin. Epidemiol. 2020, 14, S0895–S4356. [Google Scholar]
- Camus-Carcía, E.; González-González, A.I.; Heijmans, M.; de Guzmán, E.N.; Valli, C.; Beltran, J.; Pardo-Hernandez, H.; Ninov, L.; Strammiello, V.; Immonen, K.; et al. Self-management interventions for adults living with Chronic Obstructive Pulmonary Disease (COPD): The development of a Core Outcome Set for COMPAR-EU project. PLoS ONE 2021, 16, e0247522. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.J.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, l.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Yadav, U.N.; Lloyd, J.; Hosseinzadeh, H.; Prasd Batal, K.; Harris, M.F. Do Chronic Obstructive Pulmonary Diseases (COPD) Self-Management Interventions Consider Health Literacy and Patient Activation? A Systematic Review. J. Clin. Med. 2020, 9, 646. [Google Scholar] [CrossRef] [PubMed]
- Dineen-Griffin, S.; Garcia-Cardenas, V.; Williams, K.; Benrimoj, S.I. Helping patients help themselves: A systematic review of self-management support strategies in primary health care practice. PLoS ONE 2019, 14, e0220116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smalley, K.R.; Aufegger, L.; Flott, K.; Mayer, E.K.; Darzi, A. Can self-management programmes change healthcare utilization in COPD? A systematic review and framework analysis. Patient Educ. Couns. 2020, 104, 50–63. [Google Scholar] [CrossRef]
- Roberts, N.J.; Ghiani, R.; Patridge, M.R. Health Literacy in COPD. Int. J. COPD 2008, 3, 499–507. [Google Scholar]
- Heijmans, M.; Willems, A.; Scherpenzeel, A. Self-Management Regarding Illness and Health Care: Experiences of People with Chronic Lung Disease; Nivel: Utrecht, The Netherlands, 2022. [Google Scholar]
- Gilkes, A.; Ashworth, M.; Schofield, P.; Harries, T.H.; Durbaba, S.; Weston, C.; White, P. Does COPD risk vary by ethnicity? A retrospective cross-sectional study. Int. J. COPD 2016, 11, 739–746. [Google Scholar] [CrossRef] [Green Version]
- Aryal, S.; Diaz-Guzman, E.; Mannino, D.M. COPD and gender differences: An update. Transl. Res. 2013, 162, 208–218. [Google Scholar] [CrossRef]
- Pumar, M.I.; Gray, C.R.; Walsh, J.R.; Yang, I.A.; Rolls, T.A.; Ward, D.L. Anxiety and depression—Important psychological comorbidities of COPD. J. Thorac. Dis. 2014, 6, 1615–1631. [Google Scholar]
- Yadav, U.N.; Lloyd, J.; Baral, K.P.; Bhatta, N.; Mehta, S.; Harris, M.F. Using a co-design process to develop an integrated model of care for delivering self-management intervention to multi-morbid COPD people in rural Nepal. Health Res. Policy Syst. 2021, 19, 17. [Google Scholar] [CrossRef]
- Prestwich, A.; Sniehotta, F.F.; Whittington, C.; Dombrowski, S.U.; Rogers, L.; Michie, S. Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychol. 2014, 33, 465–474. [Google Scholar] [CrossRef]



| Intervention Arms | |
|---|---|
| n = 307 | |
| Median number of expected behaviours | 3.0 (2.0–5.0) |
| Lifestyle-related behaviours | |
| Physical activity | 207 (67.4%) |
| Healthy eating | 85 (27.7%) |
| Smoking reduction | 69 (22.5%) |
| Healthy sleep | 11 (3.6%) |
| Alcohol reduction | 5 (1.6%) |
| Clinical management | |
| Condition-specific behaviour (e.g., breathing exercise) | 195 (63.5%) |
| Self-monitoring | 156 (50.8%) |
| Medication use | 104 (33.9%) |
| Early recognition of symptoms | 71 (23.1%) |
| Managing devices (e.g., inhaler, oxygen) | 53 (17.3%) |
| Physical limitations management | 27 (8.8%) |
| Psychological management | |
| Handling emotions | 76 (24.8%) |
| Social management | |
| Combining COPD with social roles | 7 (2.3%) |
| Being fit enough for work | 2 (0.7%) |
| Being able to work | 1 (0.3%) |
| Working with healthcare/providers | |
| Communication with healthcare (providers) | 23 (7.5%) |
| Asking for professional help | 35 (11.4%) |
| Intervention Arms | |
|---|---|
| n = 307 | |
| Median number of support techniques | 4.0 (3.0–5.0) |
| Type of support technique | |
| Sharing information | 290 (94.5%) |
| Skills training | 212 (69.1%) |
| Self-monitoring | 144 (46.9%) |
| Goal setting | 110 (35.8%) |
| Equipment provision | 97 (31.6%) |
| Emotional management | 58 (18.9%) |
| Coaching | 55 (17.9%) |
| Enhancing problem solving | 40 (13.0%) |
| Social support | 33 (10.7%) |
| Prompts use | 32 (10.4%) |
| Services use | 30 (9.8%) |
| Shared decision-making | 7 (2.3%) |
| No specific self-management | 0 (0.0%) |
| n (%) | n (%) | ||
|---|---|---|---|
| Mode of delivery | Time of communication | ||
| Clinical visits | 30 (9.8%) | Synchronous | 231 (75.2%) |
| Support sessions | 172 (56.0%) | A-synchronous | 18 (5.9%) |
| Self-guided | 29 (9.4%) | Combination | 58 (18.9%) |
| Combination | 75 (24.4%) | Not reported | 0 (0.0%) |
| Not reported | 1 (0.0%) | ||
| n(%) | n(%) | ||
| Type of contact | Population | ||
| Face-to-Face | 152 (49.5%) | Groups | 83 (26.0%) |
| Remote | 42 (13.7%) | Individual | 224 (71.0%) |
| Combination | 109 (35.5%) | Combination | 9 (3%) |
| Not reported | 4 (1.3%) | Not reported | 0 (0%) |
| n(%) | n(%) | ||
| Location (Top 5) | Provider (Top 5) | ||
| Outpatient care | 176 (57.3%) | Nurse | 117 (38.1%) |
| Homecare | 138 (45.0%) | Physiotherapist | 84 (27.4%) |
| Hospital care | 31 (10.1%) | Physician | 53 (17.3%) |
| Virtual | 29 (9.4%) | Online service | 33(10.7%) |
| Community care | 12 (3.9%) | Educator | 26 (8.5%) |
| Total | |
|---|---|
| n = 235 n (%) | |
| Basic empowerment | |
| Self-efficacy | 31 (13.2%) |
| Knowledge | 12 (5.1%) |
| Patient activation | 4 (1.7%) |
| Adherence to SM-behaviours | |
| Physical activity/Muscle strength | 131 (55.7%) |
| Adherence to treatment and recommended visits | 13 (5.5%) |
| Smoking Cessation | 11 (4.7%) |
| Clinical outcomes | |
| COPD symptoms (short-term) | 101 (43.0%) |
| Lung Function | 56 (23.8%) |
| Mortality | 24 (10.2%) |
| Exacerbation | 22 (9.4%) |
| Patients/caregivers quality of life | |
| Quality of life | 154 (65.5%) |
| Coping with the disease, including depression and anxiety | 55 (23.4%) |
| Activities of daily living | 14 (6.0%) |
| Sleep Quality | 3 (1.3%) |
| Healthcare use | |
| Number of emergency room visits and admissions | 85 (36.2%) |
| Characteristic | Reported (n/%) | Used as Inclusion Criteria (n/%) |
|---|---|---|
| Sex | 222 (94.5%) | 4 (1.7%) |
| Age | 230 (97.9%) | 121 (51.1%) |
| Socio-economic status * | 4 (1.7%) | 0 (0.0%) |
| Cultural background * | 3 (1.3%) | 2 (0.9%) |
| Health Literacy level | 0 (0.0%) | 0 (0.0%) |
| Time since diagnosis | 39 (16.6%) | 2 (0.9%) |
| Comorbidities | 32 (13.6%) | 7 (3.0%) |
| Illness severity | 214 (91.1%) | 135 (57.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heijmans, M.; Poortvliet, R.; Van der Gaag, M.; González-González, A.I.; Beltran Puerta, J.; Canelo-Aybar, C.; Valli, C.; Ballester, M.; Rocha, C.; Garcia, M.L.; et al. Using a Taxonomy to Systematically Identify and Describe Self-Management Interventions Components in Randomized Trials for COPD. Int. J. Environ. Res. Public Health 2022, 19, 12685. https://doi.org/10.3390/ijerph191912685
Heijmans M, Poortvliet R, Van der Gaag M, González-González AI, Beltran Puerta J, Canelo-Aybar C, Valli C, Ballester M, Rocha C, Garcia ML, et al. Using a Taxonomy to Systematically Identify and Describe Self-Management Interventions Components in Randomized Trials for COPD. International Journal of Environmental Research and Public Health. 2022; 19(19):12685. https://doi.org/10.3390/ijerph191912685
Chicago/Turabian StyleHeijmans, Monique, Rune Poortvliet, Marieke Van der Gaag, Ana I. González-González, Jessica Beltran Puerta, Carlos Canelo-Aybar, Claudia Valli, Marta Ballester, Claudio Rocha, Montserrat León Garcia, and et al. 2022. "Using a Taxonomy to Systematically Identify and Describe Self-Management Interventions Components in Randomized Trials for COPD" International Journal of Environmental Research and Public Health 19, no. 19: 12685. https://doi.org/10.3390/ijerph191912685