
The Mediating Role of Healthy Lifestyle Behaviours on the Association between Perceived Stress and Self-Rated Health in People with Non-Communicable Disease

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Context
2.2. Sample
2.3. Data Collection
2.3.1. Dependent Variable
2.3.2. Independent Variable
2.3.3. Mediator Variables
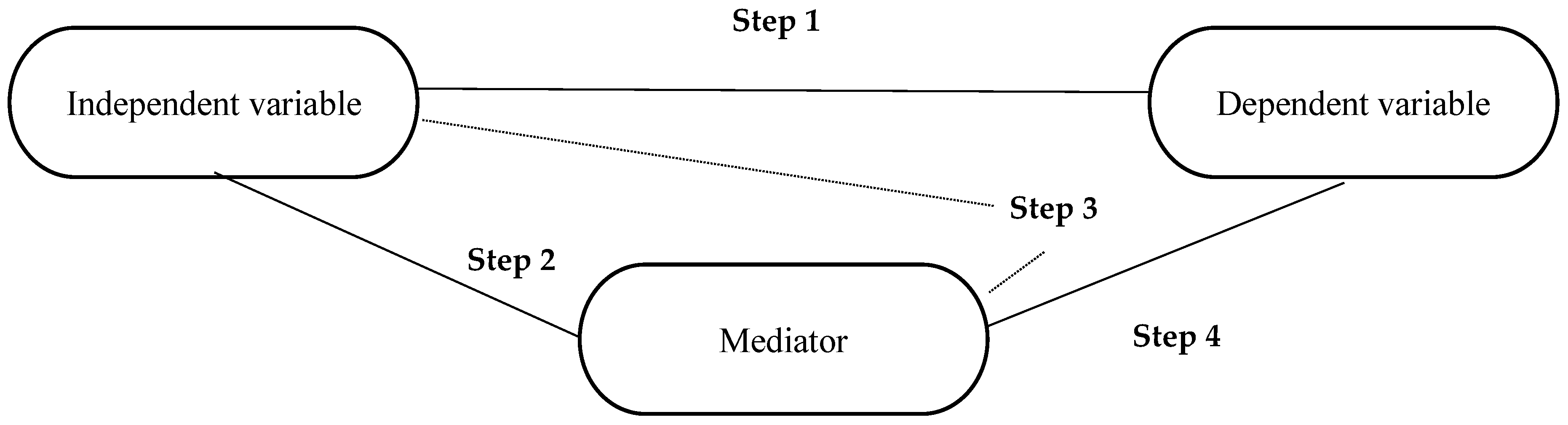
2.4. Data Management and Statistical Analyses
- The independent variable must be correlated with the dependent variable.
- The independent variable must be correlated with the mediator.
- The mediator must be correlated with the dependent variable when controlled for the independent variable.
- The effect of the mediator on the dependent variable is controlled. If the independent variable is no longer correlated with the dependent variable, there is a complete mediation. If the correlation between the independent variable and the dependent variable is reduced, there is a partial mediation. If the direct relationship of the independent variable to the dependent variable is less in the fourth regression than in the first, partial mediation is present, which, according to Baron and Kenny [32] is more realistic than perfect mediation.
3. Results
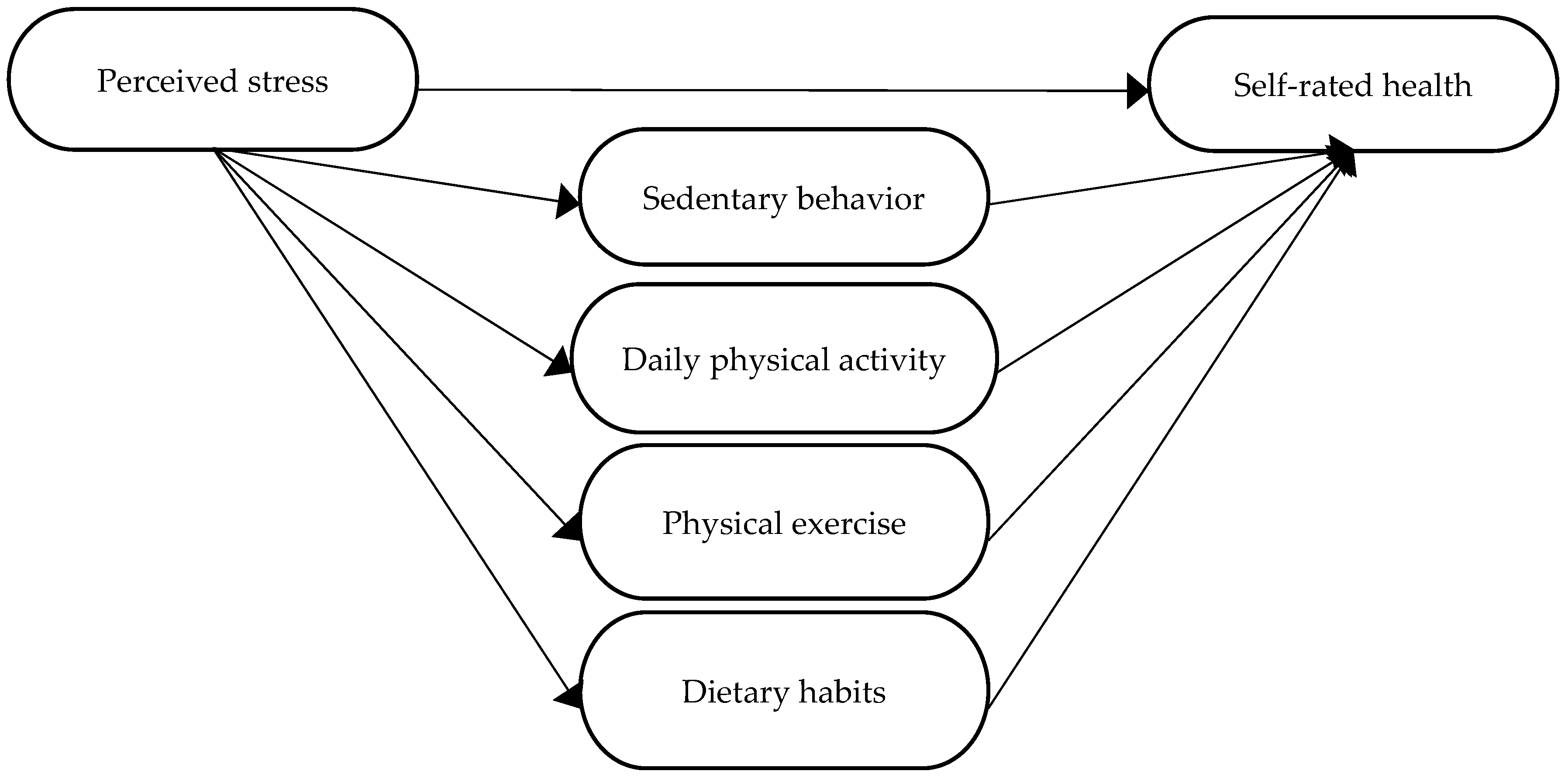
3.1. Model Testing and Mediation Model Analysis
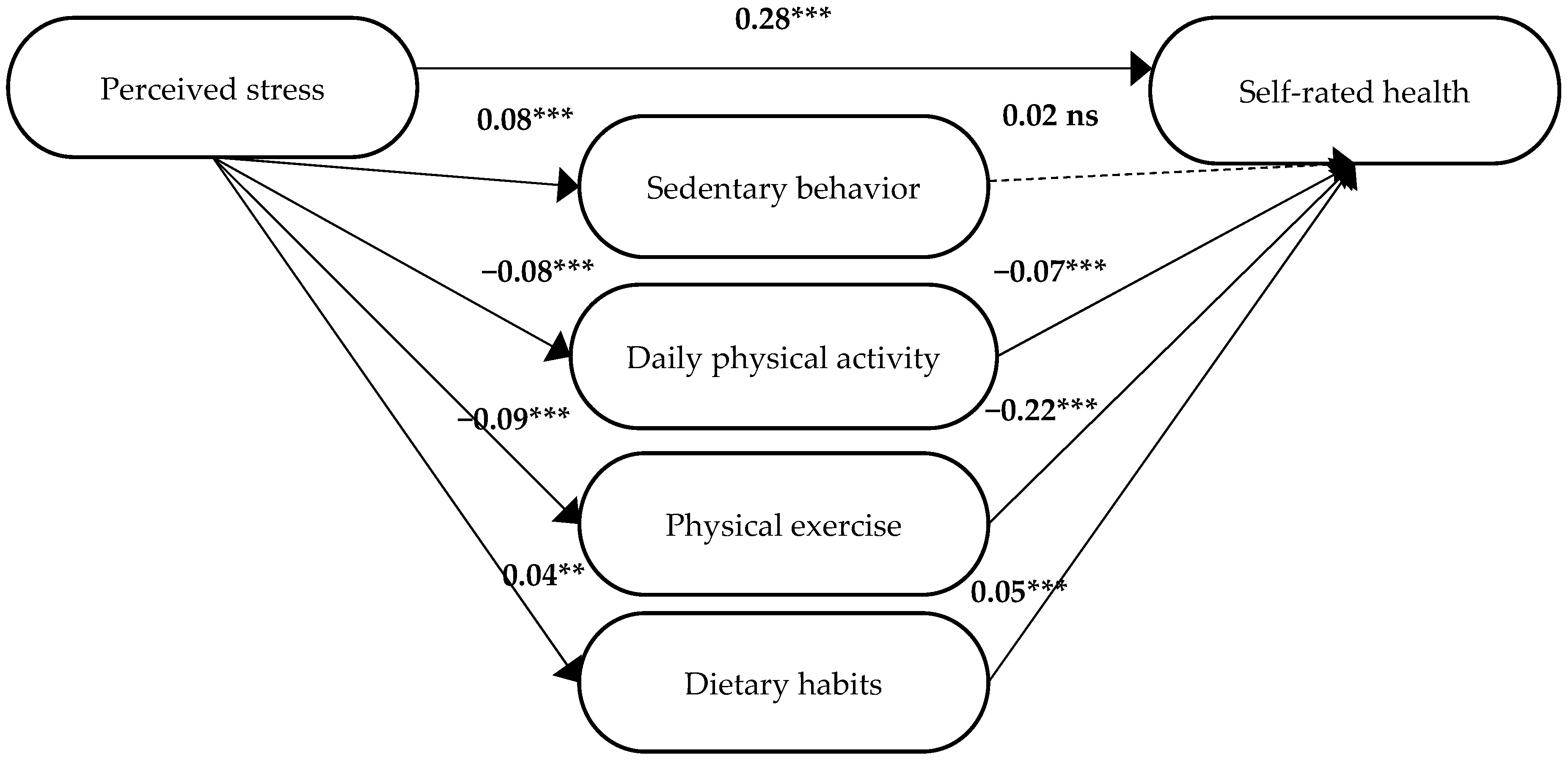
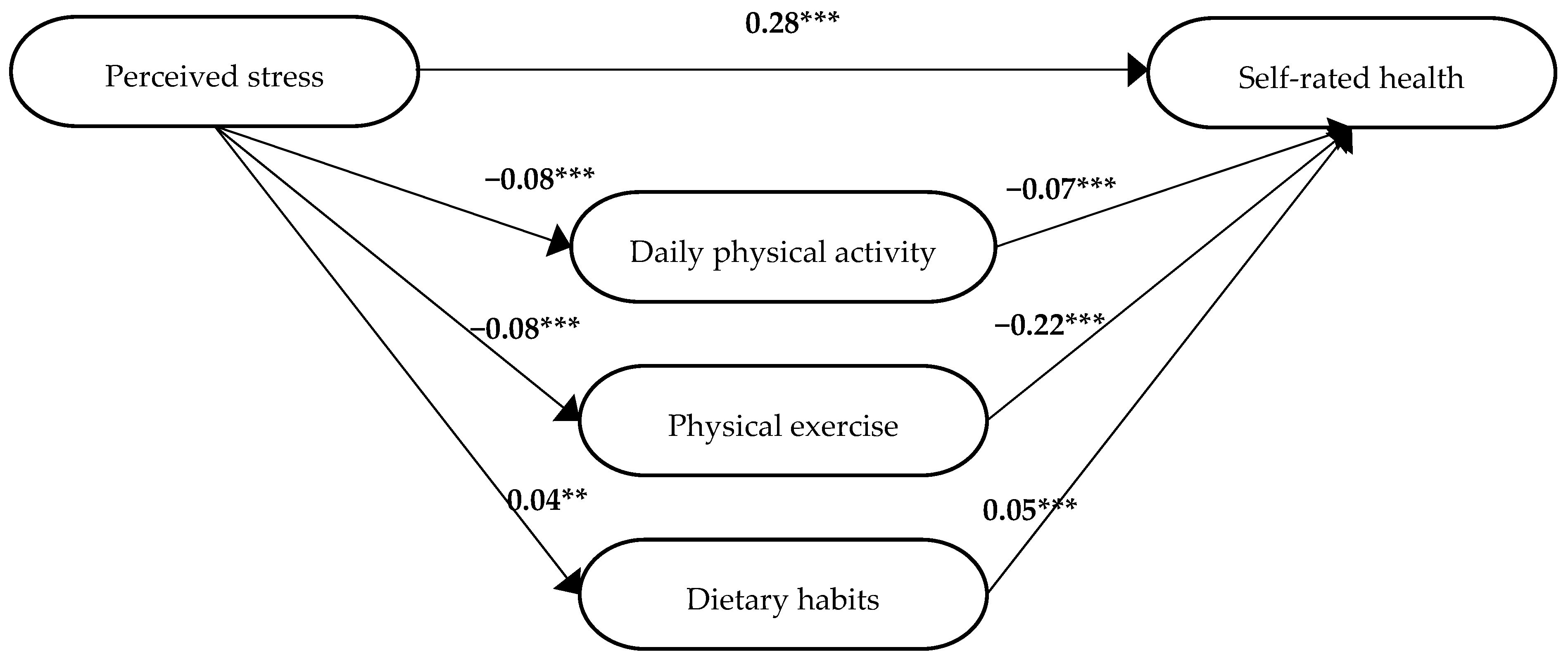
3.1.1. No Diagnosis
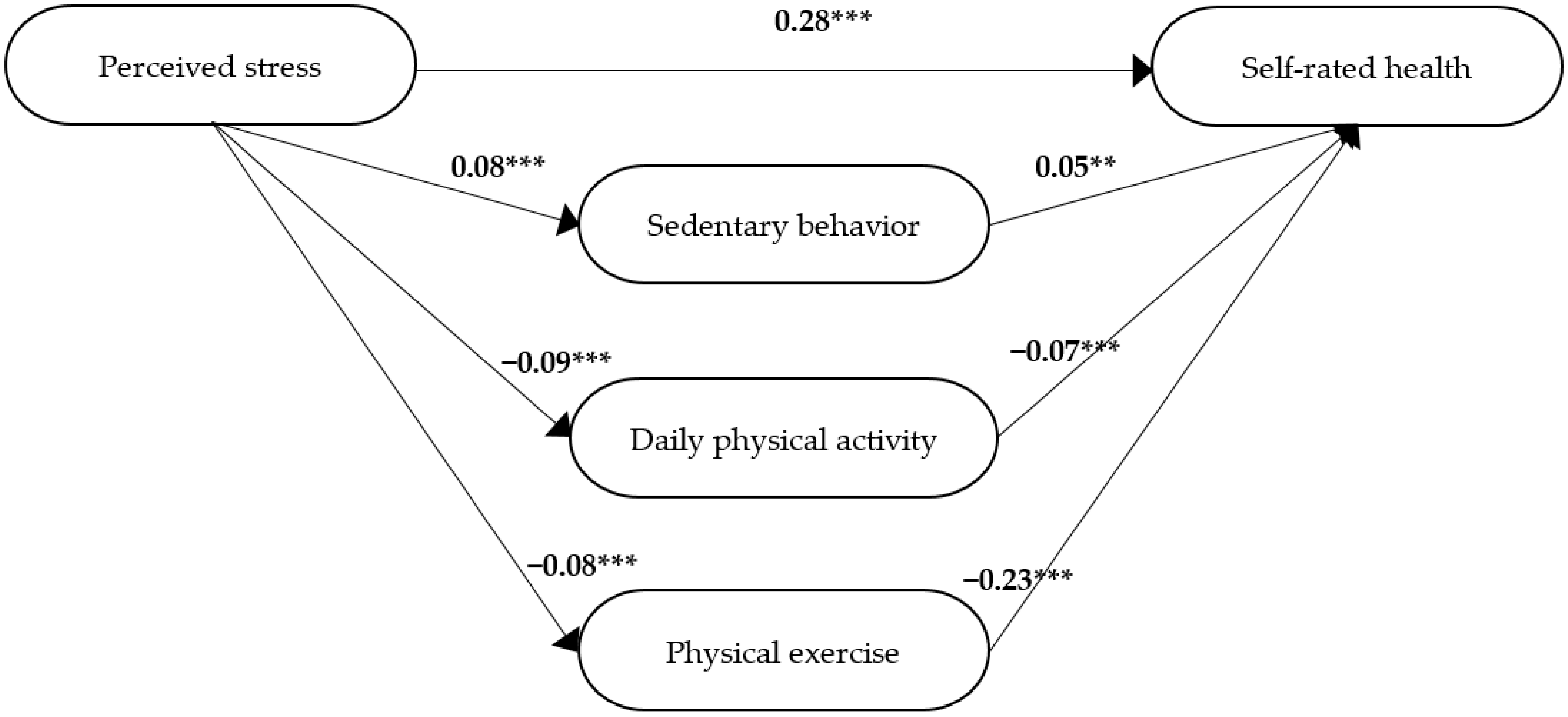
3.1.2. One Diagnosis
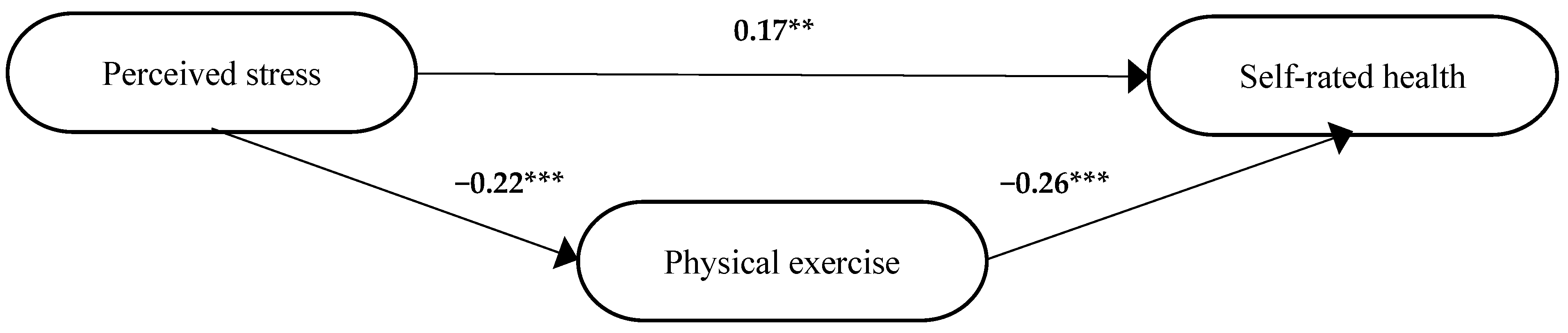
3.1.3. Two Diagnoses
3.1.4. Three or Four Diagnoses
4. Discussion
Methodological Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Connor, D.B.; Thayer, J.F.; Vedhara, K. Stress and Health: A Review of Psychobiological Processes. Annu. Rev. Psychol. 2021, 72, 663–688. [Google Scholar] [CrossRef] [PubMed]
- Mental Health Foundation. Stress: Mental Health Foundation. Available online: https://www.mentalhealth.org.uk/a-to-z/s/stress (accessed on 27 June 2022).
- Tomiyama, A.J. Stress and Obesity. Annu. Rev. Psychol. 2019, 70, 703–718. [Google Scholar] [CrossRef] [PubMed]
- Mavaddat, N.; Valderas, J.M.; Van Der Linde, R.; Khaw, K.T.; Kinmonth, A.L. Association of self-rated health with multimorbidity, chronic disease and psychosocial factors in a large middle-aged and older cohort from general practice: A cross-sectional study. BMC Fam. Pract. 2014, 15, 185. [Google Scholar] [CrossRef]
- Quiñones, A.R.; Valenzuela, S.H.; Huguet, N.; Ukhanova, M.; Marino, M.; Lucas, J.A.; O’Malley, J.; Schmidt, T.D.; Voss, R.; Peak, K.; et al. Prevalent Multimorbidity Combinations Among Middle-Aged and Older Adults Seen in Community Health Centers. J. Gen. Intern Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Badawi, G.; Gariépy, G.; Pagé, V.; Schmitz, N. Indicators of self-rated health in the Canadian population with diabetes. Diabet. Med. 2012, 29, 1021–1028. [Google Scholar] [CrossRef]
- Mozaffarian, D. Implications of the New Recommendation on Behavioral Counseling Interventions to Promote Healthy Eating and Physical Activity. JAMA 2022, 328, 334–335. [Google Scholar] [CrossRef]
- Sheffield, M.; Lewis, C. The joint effect of multiple health behaviors on odds of diabetes, depression. Prev. Med. Rep. 2022, 27, 101768. [Google Scholar] [CrossRef]
- Sarrafzadegan, N.; Mohammmadifard, N. Cardiovascular Disease in Iran in the Last 40 Years: Prevalence, Mortality, Morbidity, Challenges and Strategies for Cardiovascular Prevention. Arch. Iran. Med. 2019, 22, 204–210. [Google Scholar]
- American Diabetes Association. 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2020, 44, S53–S72. [Google Scholar] [CrossRef]
- Beatty, A.L.; Truong, M.; Schopfer, D.; Shen, H.; Bachmann, J.M.; Whooley, M.A. Geographic Variation in Cardiac Rehabilitation Participation in Medicare and Veterans Affairs Populations. Circulation 2018, 137, 1899–1908. [Google Scholar] [CrossRef]
- Kotseva, K.; Wood, D.; De Bacquer, D. Determinants of participation and risk factor control according to attendance in cardiac rehabilitation programmes in coronary patients in Europe: EUROASPIRE IV survey. Eur. J. Prev. Cardiol. 2020, 25, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- Sunamura, M.; Ter Hoeve, N.; Geleijnse, M.; Steenaard, R.; Berg-Emons, H.J.G.V.D.; Boersma, E.; Van Domburg, R.T. Cardiac rehabilitation in patients who underwent primary percutaneous coronary intervention for acute myocardial infarction: Determinants of programme participation and completion. Neth. Heart J. 2017, 25, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Cartagena, M.V.; Tort-Nasarre, G.; Arnaldo, E.R. Barriers and Facilitators for Physical Activity in Adults with Type 2 Diabetes Mellitus: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 5359. [Google Scholar] [CrossRef] [PubMed]
- Husdal, R.; Adolfsson, E.T.; Leksell, J.; Nordgren, L. Diabetes care provided by national standards can improve patients’ self-management skills: A qualitative study of how people with type 2 diabetes perceive primary diabetes care. Health Expect. 2021, 24, 1000–1008. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- The National Board of Health and Welfare. Bästa Möjliga Hälsa och En Hållbar Hälso- och Sjukvård: Med Fokus på Vården Vid Kroniska Sjukdomar: Lägesrapport 2018. [Best Possible Health and Sustainable Healthcare: With Focus on Chronic Disease Care: Progress Report 2018]. Available online: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2018-2-4.pdf (accessed on 17 August 2022).
- Blomstedt, Y.; Norberg, M.; Stenlund, H.; Nyström, L.; Lönnberg, G.; Boman, K.; Wall, S.; Weinehall, L. Impact of a combined community and primary care prevention strategy on all-cause and cardiovascular mortality: A cohort analysis based on 1 million person-years of follow-up in Västerbotten County, Sweden, during 1990–2006. BMJ Open 2015, 5, e009651. [Google Scholar] [CrossRef]
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Helping People Change, 3rd ed.; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Lindholm, L.; Stenling, A.; Norberg, M.; Stenlund, H.; Weinehall, L. A cost-effectiveness analysis of a community based CVD program in Sweden based on a retrospective register cohort. BMC Public Health 2018, 18, 452. [Google Scholar] [CrossRef]
- Eliasson, M.; Eriksson, M.; Lundqvist, R.; Wennberg, P.; Söderberg, S. Comparison of trends in cardiovascular risk factors between two regions with and without a community and primary care prevention programme. Eur. J. Prev. Cardiol. 2020, 25, 1765–1772. [Google Scholar] [CrossRef]
- Lingfors, H.; Persson, L.-G. All-cause mortality among young men 24–26 years after a lifestyle health dialogue in a Swedish primary care setting: A longitudinal follow-up register study. BMJ Open 2019, 9, e022474. [Google Scholar] [CrossRef]
- Mossberg, L.; Lundgren, U. Erfarenheter av hälsosamtalet i Sörmlands hälsoprogram: En intervjustudie utifrån de inbjudna deltagarnas perspektiv. [Experiences of Health Dialogues in Sörmland’s Health Programme: An Interview Study from the Perspective of the Invited Participants]. 2019. Available online: https://www.diva-portal.org/smash/record.jsf?pid=diva2:1373737 (accessed on 17 August 2022).
- Rosenstock, I.M. Understanding and Enhancing Patient Compliance with Diabetic Regimens. Diabetes Care 1985, 8, 610–616. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social Learning Theory and the Health Belief Model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Emmelin, M.; Weinehall, L.; Stegmayr, B.; Dahlgren, L.; Stenlund, H.; Wall, S. Self-rated ill-health strengthens the effect of biomedical risk factors in predicting stroke, especially for men-an incident case referent study. J. Hypertens. 2003, 21, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Norberg, M.; Wall, S.; Boman, K.; Weinehall, L. The Västerbotten Intervention Programme: Background, design and implications. Glob. Health Action 2010, 3. [Google Scholar] [CrossRef] [PubMed]
- Blomstedt, Y.; Emmelin, M.; Weinehall, L. What about healthy participants? The improvement and deterioration of self-reported health at a 10-year follow-up of the Västerbotten Intervention Programme. Glob. Health Action 2011, 4, 5435. [Google Scholar] [CrossRef]
- Lingfors, H.; Lindström, K.; Persson, L.-G.; Bengtsson, C.; Lissner, L. Lifestyle changes after a health dialogue. Results from the Live for Life health promotion programme. Scand. J. Prim. Health Care 2003, 21, 248–252. [Google Scholar] [CrossRef]
- Persson, L.-G.; Lingfors, H.; Nilsson, M.; Mölstad, S. The possibility of lifestyle and biological risk markers to predict morbidity and mortality in a cohort of young men after 26 years follow-up. BMJ Open 2015, 5, e006798. [Google Scholar] [CrossRef]
- Field, A.P. Discovering Statistics Using SPSS: And Sex and Drugs and Rock ‘N’ Roll; SAGE: London, UK; Los Angeles, CA, USA, 2009. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Warner, R.M. Applied Statistics: From Bivariate through Multivariate Techniques; SAGE Publications: Southend Oaks, CA, USA, 2012. [Google Scholar]
- Preacher, K.J.; Leonardelli, G.J. Calculation for the Sobel Test: An Interactive Calculation Tool for Mediation Tests. 2010. Available online: https://quantpsy.org/sobel/sobel.htm (accessed on 23 June 2021).
- Kenny, D.A. Mediation 2021. Available online: http://davidakenny.net/cm/mediate.htm#REF (accessed on 4 May 2021).
- Fatma, H.G.; Joan, V.A.; Ajabshir, S.; Gustavo, Z.G.; Exebio, J.; Dixon, Z. Perceived stress and self-rated health of Haitian and African Americans with and without Type 2 diabetes. J. Res. Med. Sci. 2013, 18, 198–204. [Google Scholar]
- Burke, K.E.; Schnittger, R.; O’Dea, B.; Buckley, V.; Wherton, J.P.; Lawlor, B.A. Factors associated with perceived health in older adult Irish population. Aging Ment. Health 2012, 16, 288–295. [Google Scholar] [CrossRef]
- Watson, J.M.; Logan, H.L.; Tomar, S.L. The influence of active coping and perceived stress on health disparities in a multi-ethnic low income sample. BMC Public Healh 2008, 8, 41. [Google Scholar] [CrossRef]
- Harvard Health. Exercising to Relax. Available online: https://www.health.harvard.edu/staying-healthy/exercising-to-relax (accessed on 21 September 2022).
- Mayo Clinic Staff. Exercise and Stress: Get Moving to Manage Stress. Available online: https://www.mayoclinic.org/healthy-lifestyle/stress-management/in-depth/exercise-and-stress/art-20044469 (accessed on 21 September 2022).
- Edholm, P.; Nilsson, A.; Kadi, F. Physical function in older adults: Impacts of past and present physical activity behaviors. Scand. J. Med. Sci. Sports 2019, 29, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Lentferink, A.J.; Oldenhuis, H.K.; De Groot, M.; Polstra, L.; Velthuijsen, H.; Van Gemert-Pijnen, J.E. Key Components in eHealth Interventions Combining Self-Tracking and Persuasive eCoaching to Promote a Healthier Lifestyle: A Scoping Review. J. Med. Internet Res. 2017, 19, e277. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Morrison, L.; Bradbury, K.; Muller, I. The Person-Based Approach to Intervention Development: Application to Digital Health-Related Behavior Change Interventions. J. Med. Internet Res. 2015, 17, e30. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, C.; Powell, J.; Payne, T.H.; Ainsworth, J.; Boyd, A.; Buchan, I. Active Assistance Technology for Health-Related Behavior Change: An Interdisciplinary Review. J. Med. Internet Res. 2012, 14, e80. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Sweden. Självskattat Allmänt Hälsotillstånd [Self-Rated Health]. Available online: https://www.folkhalsomyndigheten.se/fu-sjalvskattad-halsa (accessed on 16 August 2022).
- Statistics Sweden. Befolkning 2022 [Population 2022]. Available online: https://www.scb.se/hitta-statistik/statistik-efter-amne/befolkning/ (accessed on 16 August 2022).
- Swedish Agency for Health Technology Assessment and Assessment of Social Services. Statens Beredning för Medicinsk och Social Utvärdering. Måttligt Förhöjt Blodtryck: En Systematisk Litteraturöversikt: Uppdatering av SBU-Rapporten Måttligt Förhöjt Blodtryck (2004), nr 170/1; Statens Beredning för Medicinsk Utvärdering (SBU): Stockholm, Sweden, 2007. (In Swedish) [Google Scholar]
- The National Board of Health and Welfare. Nationella Riktlinjer för Diabetesvård: Stöd för Styrning och Ledning; Socialstyrelsen: Stockholm, Sweden, 2018. (In Swedish) [Google Scholar]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- DeSalvo, K.B.; Bloser, N.; Reynolds, K.; He, J.; Muntner, P. Mortality prediction with a single general self-rated health question. A meta-analysis. J. Gen. Intern. Med. 2006, 21, 267–275. [Google Scholar] [CrossRef]
- Nordgren, L.; Söderlund, A. Being on sick leave due to heart failure: Self-rated health, encounters with healthcare professionals and social insurance officers and self-estimated ability to return to work. Psychol. Health Med. 2014, 20, 582–593. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total; n (%) | 2016; n (%) | 2019; n (%) | p. |
|---|---|---|---|---|
| Sex | 0.162 | |||
| -male | 4868 (46.0) | 2695 (46.2) | 2173 (45.8) | |
| -female | 5593 (52.8) | 3020 (51.7) | 2573 (54.2) | |
| Age | 0.472 | |||
| -40 | 2900 (27.4) | 1574 (27.0) | 1326 (27.9) | |
| -50 | 3770 (35.6) | 2091 (35.8) | 1679 (35.4) | |
| -60 | 3800 (35.9) | 2059 (35.3) | 1741 (36.7) | |
| Country of birth | 0.002 | |||
| -Sweden | 8184 (77.3) | 4559 (78.1) | 3625 (76.4) | |
| -Nordic countries except Sweden | 441 (4.2) | 237 (4.1) | 204 (4.3) | |
| -Europe except Nordic countries | 400 (3.8) | 207 (3.5) | 193 (4.1) | |
| -outside Europe | 1440 (13.6) | 728 (12.5) | 712 (15.0) | |
| Education level | 0.004 | |||
| -elementary school | 1665 (15.7) | 946 (16.2) | 719 (15.1) | |
| -upper secondary school | 5149 (48.7) | 2859 (49.0) | 2290 (48.3) | |
| -higher education | 3579 (33.8) | 1880 (32.2) | 1699 (35.8) | |
| Employment status | 0.017 | |||
| -employed | 7418 (70.1) | 4023 (68.9) | 3395 (71.5) | |
| -self-employed | 946 (8.9) | 545 (9.3) | 401 (8.4) | |
| -unemployed | 499 (4.7) | 300 (5.1) | 199 (4.2) | |
| -sickness benefit/sickness or activity compensation | 565 (5.3) | 329 (5.6) | 236 (5.0) | |
| -other | 1155 (10.9) | 640 (11.0) | 515 (10.9) |
| Variables | 2016 | 2019 | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Male | Female | All | Male | Female | All | Male | Female | |
| n (%) | |||||||||
| Self-rated health | |||||||||
| -very good/good | 4252 (73.1) | 2030 (75.4) | 2144 (71.2) | 3431 (72.3) | 1631 (75.1) | 1800 (70.0) | 7683 (72.7) | 3661 (75.2) | 3944 (70.5) |
| -fair/poor/very poor | 1566 (26.9) | 662 (24.6) | 867 (28.7) | 1315 (27.7) | 542 (24.9) | 773 (30.0) | 2880 (27.3) | 1204 (24.7) | 1640 (29.3) |
| Felt stress | |||||||||
| -not at all | 647 (13.5) | 353 (16.0) | 274 (11.0) | 811 (17.2) | 455 (21.0) | 356 (13.9) | 1458 (15.3) | 808 (16.6) | 630 (11.3) |
| -yes, some/yes, pretty much/yes, a lot | 4156 (86.5) | 1851 (68.7) | 2228 (73.8) | 3913 (82.8) | 1708 (78.6) | 2205 (85.7) | 8069 (84.7) | 3559 (73.1) | 4433 (79.3) |
| Sedentary behaviour | |||||||||
| -≤7 h per day | 4096 (70.7) | 1801 (66.8) | 2212 (73.2) | 3590 (75.8) | 1600 (73.6) | 1990 (77.3) | 7686 (73.0) | 3401 (69.9) | 4202 (75.1) |
| ->7 h per day | 1694 (29.3) | 876 (32.5) | 782 (25.9) | 1149 (24.2) | 570 (26.2) | 579 (22.5) | 2844 (23.0) | 1446 (29.7) | 1361 (24.3) |
| Daily physical activity | |||||||||
| -<150 min per week | 3615 (62.2) | 1717 (63.7) | 1821 (60.3) | 2897 (61.2) | 1397 (64.3) | 1500 (58.3) | 6512 (61.8) | 3114 (64.0) | 3321 (59.4) |
| -≥150 min per week | 2193 (37.8) | 970 (36.0) | 1182 (39.1) | 1838 (38.8) | 771 (35.5) | 1067 (41.5) | 4031 (38.2) | 1741 (35.8) | 2249 (40.2) |
| Physical exercise | |||||||||
| -<1 h per week | 3636 (62.7) | 1692 (62.8) | 1869 (61.9) | 2822 (59.6) | 1275 (58.7) | 1547 (60.1) | 6458 (61.3) | 2967 (60.9) | 3416 (61.1) |
| -≥1 h per week | 2166 (37.3) | 997 (37.0) | 1124 (37.2) | 1911 (40.4) | 895 (41.2) | 1016 (39.5) | 4077 (38.7) | 1892 (38.9) | 2140 (38.3) |
| Dietary habits | |||||||||
| -very healthy/healthy | 1722 (30.5) | 580 (21.5) | 1103 (36.5) | 1300 (27.7) | 419 (19.3) | 881 (34.2) | 3022 (29.2) | 999 (20.5) | 1984 (35.5) |
| -somewhat unhealthy/unhealthy | 3921 (69.5) | 2032 (75.4) | 1816 (60.1) | 3390 (72.3) | 1727 (79.5) | 1663 (64.6) | 7311 (70.8) | 3759 (77.2) | 3479 (62.2) |
| Diagnosis | |||||||||
| -hypertension | 1703 (29.2) | 822 (30.5) | 844 (27.9) | 1449 (30.5) | 714 (32.9) | 735 (28.6) | 3152 (29.8) | 1536 (31.6) | 1579 (28.2) |
| -diabetes | 218 (3.7) | 132 (4.9) | 84 (2.8) | 192 (4.0) | 107 (4.9) | 85 (3.3) | 410 (3.9) | 239 (4.9) | 169 (3.0) |
| -myocardial infarction | 142 (2.4) | 90 (3.3) | 45 (1.5) | 76 (1.6) | 54 (2.5) | 22 (0.9) | 218 (2.1) | 144 (3.0) | 67 (1.2) |
| -stroke | 98 (1.7) | 52 (1.9) | 44 (1.5) | 91 (1.9) | 50 (2.3) | 41 (1.6) | 189 (1.8) | 102 (2.1) | 85 (1.5) |
| Number of diagnoses | |||||||||
| -no diagnosis | 3958 (67.8) | 1775 (65.9) | 2101 (69.6) | 3170 (66.8) | 1400 (64.4) | 1770 (68.8) | 7128 (67.4) | 3175 (65.2) | 3871 (69.2) |
| -one diagnosis | 1625 (27.8) | 765 (28.4) | 827 (27.4) | 1366 (28.8) | 637 (29.3) | 729 (28.3) | 2991 (28.3) | 1402 (28.8) | 1556 (27.8) |
| -two diagnoses | 227 (3.9) | 135 (5.0) | 86 (2.8) | 192 (4.0) | 122 (5.6) | 70 (2.7) | 419 (4.0) | 257 (5.3) | 156 (2.8) |
| -three diagnoses | 26 (0.4) | 19 (0.7) | 6 (0.2) | 14 (0.3) | 12 (0.6) | 2 (0.1) | 40 (0.4) | 31 (0.6) | 8 (0.1) |
| -four diagnoses | 1 (0.02) | 1 (0.04) | - | 4 (0.1) | 2 (0.1) | 2 (0.1) | 5 (0.05) | 3 (0.1) | 2 (0.04) |
| Variables | Adj R2 | F-Value | p-Value | df 1, df 2 | β | p (for β) |
|---|---|---|---|---|---|---|
| Step 1 | ||||||
| Stress—self-rated health | 0.09 | 642.5 | <0.001 | 1, 6394 | 0.30 | <0.001 |
| Step 2 | ||||||
| Stress—sedentary behaviour | 0.01 | 30.5 | <0.001 | 1, 6379 | 0.07 | <0.001 |
| Stress—daily physical activity | 0.01 | 46.2 | <0.001 | 1, 6386 | −0.08 | <0.001 |
| Stress—physical exercise | 0.01 | 46.5 | <0.001 | 1, 6379 | −0.08 | <0.001 |
| Stress—dietary habits | 0.001 | 6.1 | 0.013 | 1, 6283 | 0.03 | 0.013 |
| Effect | No Diagnosis (n = 7128) | One Diagnosis (n = 2991) | Two Diagnoses (n = 419) |
|---|---|---|---|
| Direct effect (perceived stress) | 0.24 | 0.28 | 0.17 |
| Indirect effect | 0.02 * | 0.03 ** | 0.06 *** |
| Total effect (direct + indirect) | 0.26 | 0.31 | 0.23 |
| Variables | Adj R2 | F-Value | p-Value | df 1, df 2 | β | p (for β) |
|---|---|---|---|---|---|---|
| Step 1 | ||||||
| Stress—self-rated health | 0.10 | 295.5 | <0.001 | 1, 2695 | 0.31 | <0.001 |
| Step 2 | ||||||
| Stress—sedentary behaviour | 0.01 | 16.4 | <0.001 | 1, 2692 | 0.08 | <0.001 |
| Stress—daily physical activity | 0.01 | 22.2 | <0.001 | 1, 2695 | −0.09 | <0.001 |
| Stress—physical exercise | 0.01 | 16.1 | <0.001 | 1, 2695 | −0.08 | <0.001 |
| Stress—dietary habits | 0.0002 | 0.4 | 0.517 | 1, 2648 | 0.01 | 0.517 |
| Variables | Adj R2 | F-Value | p-Value | df 1, df 2 | β | p (for β) |
|---|---|---|---|---|---|---|
| Step 1 | ||||||
| Stress—self-rated health | 0.51 | 21.38 | <0.001 | 1, 375 | 0.23 | <0.001 |
| Step 2 | ||||||
| Stress—sedentary behaviour | 0.01 | 1.78 | 0.182 | 1, 372 | 0.07 | 0.182 |
| Stress—daily physical activity | 0.01 | 0.96 | 0.328 | 1, 375 | −0.05 | 0.328 |
| Stress—physical exercise | 0.05 | 19.74 | <0.001 | 1, 375 | −0.22 | <0.001 |
| Stress—dietary habits | −0.003 | 0.01 | 0.919 | 1, 363 | −0.005 | 0.919 |
| Variables | Adj R2 | F-Value | p Value | df 1, df 2 | β | P (for β) |
|---|---|---|---|---|---|---|
| Step 1 | ||||||
| Stress—self-rated health | 0.13 | 6.72 | 0.013 | 1, 38 | 0.39 | 0.013 |
| Step 2 | ||||||
| Stress—sedentary behaviour | 0.04 | 2.39 | 0.131 | 1, 37 | −0.25 | 0.131 |
| Stress—daily physical activity | −0.03 | 0.0005 | 0.983 | 1, 37 | −0.01 | 0.983 |
| Stress—physical exercise | −0.01 | 0.50 | 0.483 | 1, 37 | −0.12 | 0.483 |
| Stress—dietary habits | −0.02 | 0.27 | 0.609 | 1, 37 | 0.08 | 0.609 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nordgren, L.; von Heideken Wågert, P.; Söderlund, A.; Elvén, M. The Mediating Role of Healthy Lifestyle Behaviours on the Association between Perceived Stress and Self-Rated Health in People with Non-Communicable Disease. Int. J. Environ. Res. Public Health 2022, 19, 12071. https://doi.org/10.3390/ijerph191912071
Nordgren L, von Heideken Wågert P, Söderlund A, Elvén M. The Mediating Role of Healthy Lifestyle Behaviours on the Association between Perceived Stress and Self-Rated Health in People with Non-Communicable Disease. International Journal of Environmental Research and Public Health. 2022; 19(19):12071. https://doi.org/10.3390/ijerph191912071
Chicago/Turabian StyleNordgren, Lena, Petra von Heideken Wågert, Anne Söderlund, and Maria Elvén. 2022. "The Mediating Role of Healthy Lifestyle Behaviours on the Association between Perceived Stress and Self-Rated Health in People with Non-Communicable Disease" International Journal of Environmental Research and Public Health 19, no. 19: 12071. https://doi.org/10.3390/ijerph191912071