

Health and Care Dependency of Older Adults in Dresden, Germany: Results from the LAB60+ Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.2.1. Physical Health and Chronic Illnesses
2.2.2. Care Dependency
2.2.3. Health-Related Quality of Life (HRQoL), Well-Being, and Depressivity
2.2.4. Sociodemographic Factors
2.3. Statistical Analysis
3. Results
3.1. Participants’ Response and Characteristics
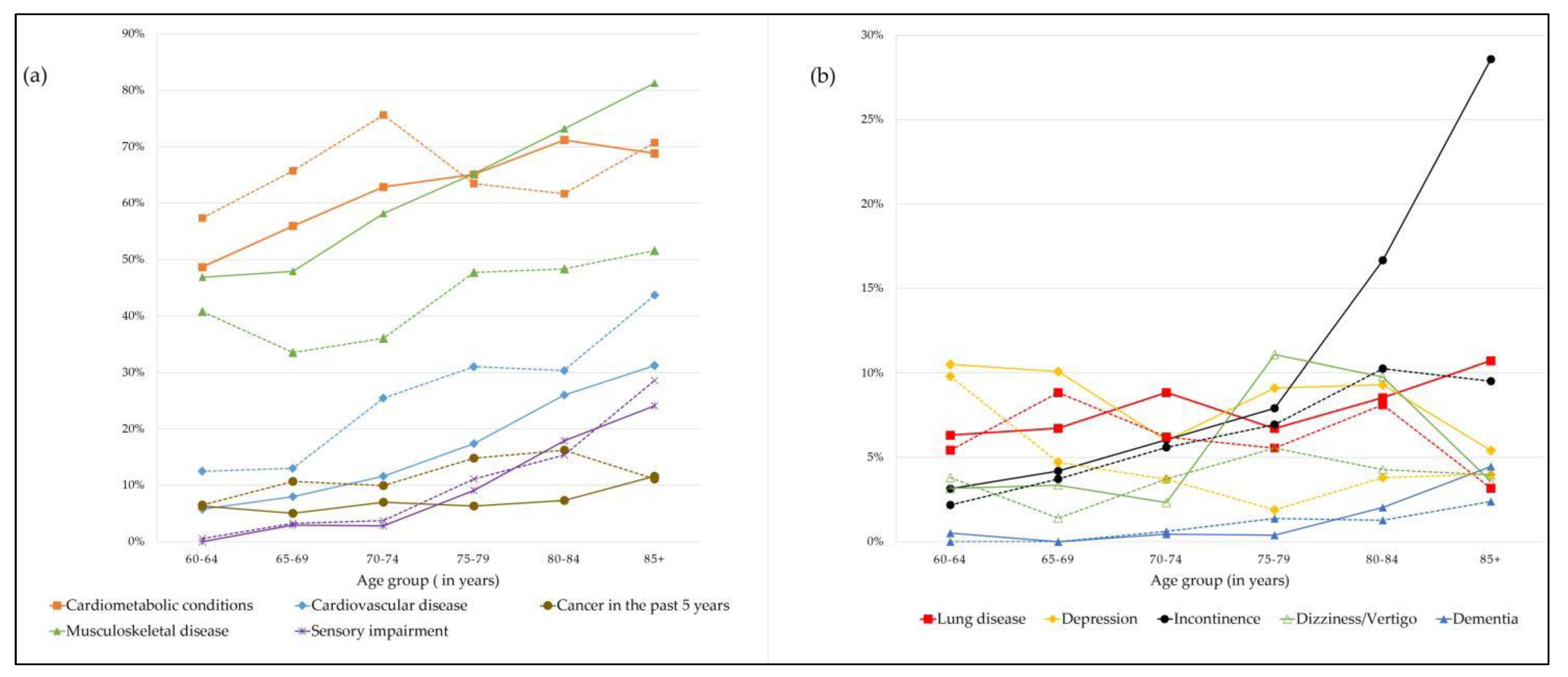
3.2. Chronic Conditions
3.3. Care Dependency
3.4. Health-Related Quality of Life and Well-Being
4. Discussion
4.1. Chronic Conditions and Multimorbidity
4.2. Care Dependency
4.3. Health-Related Quality of Life (HRQoL) and Well-Being
4.4. Strengths and Weaknesses
4.5. Public Health Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statistisches Bundesamt (Destasis). Number of People Aged 67 or Over Will Grow 22% by 2035. Available online: https://www.destatis.de/EN/Press/2021/09/PE21_459_12411.html (accessed on 1 May 2022).
- Statista. Median Age of the Population in Germany 1950–2050. Available online: https://www.statista.com/statistics/624303/average-age-of-the-population-in-germany/#statisticContainer (accessed on 29 April 2022).
- Kommunale Statistikstelle Dresden. Kommunale Bürgerumfrage 2020: Hauptaussagen. Available online: https://www.dresden.de/media/pdf/onlineshop/statistikstelle/KBU_2020-Hauptaussagen.pdf (accessed on 29 April 2022).
- Landeshauptstadt Dresden. Bevölkerungsprognose 2020. Available online: https://www.dresden.de/de/leben/stadtportrait/statistik/bevoelkerung-gebiet/bevoelkerungsprognose.php (accessed on 9 November 2021).
- Scharf, T.; Phillipson, C.; Smith, A.E.; Kingston, P. Growing Older in Socially Deprived Areas: Social Exclusion in Later Life. 2002. Available online: https://eprints.ncl.ac.uk/file_store/production/224272/155BAEA3-29AA-4132-BC8A-914E1D59C144.pdf (accessed on 29 April 2022).
- Antón, J.-I.; Braña, F.-J.; Muñoz de Bustillo, R. An analysis of the cost of disability across Europe using the standard of living approach. SERIEs 2016, 7, 281–306. [Google Scholar] [CrossRef]
- Pani-Harreman, K.E.; Bours, G.J.J.W.; Zander, I.; Kempen, G.I.J.M.; van Duren, J.M.A. Definitions, key themes and aspects of ‘ageing in place’: A scoping review. Ageing Soc. 2021, 41, 2026–2059. [Google Scholar] [CrossRef]
- Hasselhorn, H.M.; Peter, R.; Rauch, A.; Schröder, H.; Swart, E.; Bender, S.; du Prel, J.-B.; Ebener, M.; March, S.; Trappmann, M.; et al. Cohort profile: The lidA Cohort Study—a German Cohort Study on Work, Age, Health and Work Participation. Int. J. Epidemiol. 2014, 43, 1736–1749. [Google Scholar] [CrossRef]
- Börsch-Supan, A.; Hank, K.; Jürges, H. A new comprehensive and international view on ageing: Introducing the ‘Survey of Health, Ageing and Retirement in Europe’. Eur. J. Ageing 2005, 2, 245–253. [Google Scholar] [CrossRef]
- Menec, V.; Nowicki, S. Examining the relationship between communities’’ age-friendliness’ and life satisfaction and self-perceived health in rural Manitoba, Canada. Rural. Remote Health 2014, 14, 159–172. [Google Scholar] [CrossRef]
- Nieboer, A.P.; Cramm, J.M. Age-Friendly Communities Matter for Older People’s Well-Being. J. Happiness Stud. 2018, 19, 2405–2420. [Google Scholar] [CrossRef]
- Ng, S.-I.; Lim, X.-J.; Hsu, H.-C. The Importance of Age-Friendly City on Older People’s Continuity and Life Satisfaction. Int. J. Environ. Res. Public Health 2021, 18, 7252. [Google Scholar] [CrossRef]
- Nolte, E.; Shkolnikov, V.; McKee, M. Changing mortality patterns in East and West Germany and Poland. I: Long term trends (1960-1997). J. Epidemiol. Community Health 2000, 54, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Vogel, N.; Gerstorf, D.; Ram, N.; Goebel, J.; Wagner, G.G. Terminal decline in well-being differs between residents in East Germany and West Germany. Int. J. Behav. Dev. 2017, 41, 115–126. [Google Scholar] [CrossRef]
- Frijters, P.; Haisken-DeNew, J.P.; Shields, M.A. Investigating the patterns and determinants of life satisfaction in Germany following reunification. J. Hum. Resour. 2004, 39, 649–674. [Google Scholar] [CrossRef]
- Fortin, M.; Hudon, C.; Haggerty, J.; van den Akker, M.; Almirall, J. Prevalence estimates of multimorbidity: A comparative study of two sources. BMC Health Serv. Res. 2010, 10, 111. [Google Scholar] [CrossRef]
- Schram, M.T.; Frijters, D.; van de Lisdonk, E.H.; Ploemacher, J.; de Craen, A.J.M.; de Waal, M.W.M.; van Rooij, F.J.; Heeringa, J.; Hofman, A.; Deeg, D.J.H.; et al. Setting and registry characteristics affect the prevalence and nature of multimorbidity in the elderly. J. Clin. Epidemiol. 2008, 61, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Bundesministerium für Gesundheit. Online-Ratgeber Pflege: Pflegegrade. Available online: https://www.bundesgesundheitsministerium.de/pflegegrade.html (accessed on 12 October 2021).
- Ellert, U.; Lampert, T.; Ravens-Sieberer, U. Measuring health-related quality of life with the SF-8. Normal sample of the German population. Bundesgesundheitsblatt Gesundh. Gesundh 2005, 48, 1330–1337. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.J.; Kosinski, M.; Dewey, J.E.; Gandek, B.; Kisinski, M.; Ware, J.E.; Dewey, J.E. How to score and interpret single-item health status measures: A manual for users of the SF-8™ Health Survey. Semant. Sch. 2001. [Google Scholar]
- Beierlein, V.; Morfeld, M.; Bergelt, C.; Bullinger, M.; Brähler, E. Messung der gesundheitsbezogenen Lebensqualität mit dem SF-8. Diagnostica 2012, 58, 145–153. [Google Scholar] [CrossRef]
- Brähler, E.; Mühlan, H.; Albani, C.; Schmidt, S. Teststatistische Prüfung und Normierung der deutschen Versionen des EUROHIS-QOL Lebensqualität-Index und des WHO-5 Wohlbefindens-Index. Diagnostica 2007, 53, 83–96. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Winkler, J.; Stolzenberg, H. Adjustierung des Sozialen-Schicht-Index für die Anwendung im Kinder- und Jugendgesundheitssurvey (KiGGS); Hochsch. Fachbereich Wirtschaft: Wismar, Germany, 2009; p. 26. [Google Scholar]
- Royal, K.D. Survey research methods: A guide for creating post-stratification weights to correct for sample bias. Educ. Health Prof. 2019, 2, 48. [Google Scholar] [CrossRef]
- Barros, A.J.; Hirakata, V.N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 3, 1–13. [Google Scholar] [CrossRef]
- Lange, C.; Jentsch, F.; Allen, J.; Hoebel, J.; Kratz, A.L.; von der Lippe, E.; Müters, S.; Schmich, P.; Thelen, J.; Wetzstein, M.; et al. Data Resource Profile: German Health Update (GEDA)—the health interview survey for adults in Germany. Int. J. Epidemiol. 2015, 44, 442–450. [Google Scholar] [CrossRef]
- Klaus, D.; Engstler, H.; Mahne, K.; Wolff, J.K.; Simonson, J.; Wurm, S.; Tesch-Römer, C. Cohort profile: The German ageing survey (DEAS). Int. J. Epidemiol. 2017, 46, 1105g. [Google Scholar] [CrossRef]
- Fuchs, J.; Busch, M.; Lange, C.; Scheidt-Nave, C. Prevalence and patterns of morbidity among adults in Germany. Bundesgesundheitsbl. Pub. Med. 2012, 55, 576–586. [Google Scholar]
- Neuhauser, H.; Kuhnert, R.; Born, S. 12-Monatsprävalenz von Bluthochdruck in Deutschland. J. Health Monit. 2017, 2, 57–63. [Google Scholar] [CrossRef]
- Hajek, A.; König, H.-H. The association between obesity and social exclusion in middle-aged and older adults: Findings from a nationally representative study in Germany. BMC Geriatr. 2018, 18, 258. [Google Scholar] [CrossRef]
- Du, Y.; Heidemann, C.; Gößwald, A.; Schmich, P.; Scheidt-Nave, C. Prevalence and comorbidity of diabetes mellitus among non-institutionalized older adults in Germany-results of the national telephone health interview survey ‘German Health Update (GEDA)’ 2009. BMC Public Health 2013, 13, 1–13. [Google Scholar] [CrossRef]
- Kristensen, K.; König, H.-H.; Hajek, A. The association of multimorbidity, loneliness, social exclusion and network size: Findings from the population-based German Ageing Survey. BMC Public Health 2019, 19, 1383. [Google Scholar] [CrossRef]
- Puth, M.-T.; Weckbecker, K.; Schmid, M.; Münster, E. Prevalence of multimorbidity in Germany: Impact of age and educational level in a cross-sectional study on 19,294 adults. BMC Public Health 2017, 17, 826. [Google Scholar] [CrossRef]
- Johnston, M.C.; Crilly, M.; Black, C.; Prescott, G.J.; Mercer, S.W. Defining and measuring multimorbidity: A systematic review of systematic reviews. Eur. J. Public Health 2019, 29, 182–189. [Google Scholar] [CrossRef]
- Le Reste, J.Y.; Nabbe, P.; Manceau, B.; Lygidakis, C.; Doerr, C.; Lingner, H.; Czachowski, S.; Munoz, M.; Argyriadou, S.; Claveria, A. The European General Practice Research Network presents a comprehensive definition of multimorbidity in family medicine and long term care, following a systematic review of relevant literature. J. Am. Med. Dir. Assoc. 2013, 14, 319–325. [Google Scholar] [CrossRef]
- Willadsen, T.G.; Bebe, A.; Køster-Rasmussen, R.; Jarbøl, D.E.; Guassora, A.D.; Waldorff, F.B.; Reventlow, S.; Olivarius, N.d.F. The role of diseases, risk factors and symptoms in the definition of multimorbidity–A systematic review. Scand. J. Prim. Health Care 2016, 34, 112–121. [Google Scholar] [CrossRef]
- Pflegestatistik, D. Pflege im Rahmen der Pflegeversicherung, Deutschlandergebnisse. Stat. Bundesamt (Destatis) 2020. [Google Scholar]
- Statistisches Bundesamt. Mehr Pflegebedürftige. Available online: https://www.presseportal.de/pm/32102/2581109 (accessed on 28 November 2021).
- Bund-Länder Demografie Portal. Altersspezifisce Pflegequoten. Available online: https://www.demografie-portal.de/DE/Fakten/pflegequote-alter.html (accessed on 29 November 2021).
- Backes, G.; Amrhein, L.; Wolfinger, M. Gender in der Pflege: Herausforderungen für Die Politik; Friedrich-Ebert-Stiftung: Bonn, Germany, 2008. [Google Scholar]
- Melzer, D.; McWilliams, B.; Brayne, C.; Johnson, T.; Bond, J. Socioeconomic status and the expectation of disability in old age: Estimates for England. J. Epidemiol. Community Health 2000, 54, 286–292. [Google Scholar] [CrossRef]
- Majer, I.M.; Nusselder, W.J.; Mackenbach, J.P.; Kunst, A.E. Socioeconomic inequalities in life and health expectancies around official retirement age in 10 Western-European countries. J. Epidemiol. Community Health 2011, 65, 972–979. [Google Scholar] [CrossRef]
- Kroll, L.E.; Lampert, T.; Lange, C.; Ziese, T. Entwicklung und Einflussgrößen der gesunden Lebenserwartung. (Discussion Papers / Wissenschaftszentrum Berlin für Sozialforschung, Forschungsschwerpunkt Bildung, Arbeit und Lebenschancen, Forschungsgruppe Public Health, 2008-306). Berlin: Wissenschaftszentrum Berlin für Sozialforschung gGmbH. Available online: https://nbn-resolving.org/urn:nbn:de:0168-ssoar-25929 (accessed on 29 April 2022).
- Wahrendorf, M.; Reinhardt, J.D.; Siegrist, J. Relationships of disability with age among adults aged 50 to 85: Evidence from the United States, England and continental europe. PLoS ONE 2013, 8, e71893. [Google Scholar] [CrossRef]
- Zaninotto, P.; Batty, G.D.; Stenholm, S.; Kawachi, I.; Hyde, M.; Goldberg, M.; Westerlund, H.; Vahtera, J.; Head, J. Socioeconomic Inequalities in Disability-free Life Expectancy in Older People from England and the United States: A Cross-national Population-Based Study. J. Gerontol. Ser. A 2020, 75, 906–913. [Google Scholar] [CrossRef]
- Richter, D.; Riedel-Heller, S.; Zürcher, S.J. Mental health problems in the general population during and after the first lockdown phase due to the SARS-Cov-2 pandemic: Rapid review of multi-wave studies. Epidemiol. Psychiatr. Sci. 2021, 30, e27. [Google Scholar] [CrossRef] [PubMed]
- Wettstein, M.; Nowossadeck, S.; Vogel, C. Well-being trajectories of middle-aged and older adults and the corona pandemic: No “COVID-19 effect” on life satisfaction, but increase in depressive symptoms. Psychol. Aging 2022, 37, 175–189. [Google Scholar] [CrossRef]
- Tsai, F.-Y.; Schillok, H.; Coenen, M.; Merkel, C.; Jung-Sievers, C.; COSMO Study Group. The Well-Being of the German Adult Population Measured with the WHO-5 over Different Phases of the COVID-19 Pandemic: An Analysis within the COVID-19 Snapshot Monitoring Study (COSMO). Int. J. Environ. Res. Public Health 2022, 19, 3236. [Google Scholar] [CrossRef]
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective wellbeing, health, and ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef]
- Bittmann, F. Beyond the U-Shape: Mapping the Functional Form Between Age and Life Satisfaction for 81 Countries Utilizing a Cluster Procedure. J. Happiness Stud. 2021, 22, 2343–2359. [Google Scholar] [CrossRef]
- Leckcivilize, A.; McNamee, P. The Effects of Retirement on Health and Health Behaviour among Retirees and their Partners: Evidence from the English Longitudinal Study of Ageing. J. Popul. Ageing 2021, 15, 381–412. [Google Scholar] [CrossRef]
- Åhlin, J.K.; Peristera, P.; Westerlund, H.; Magnusson Hanson, L.L. Psychosocial working characteristics before retirement and depressive symptoms across the retirement transition: A longitudinal latent class analysis. Scand. J. Work. Environ. Health 2020, 46, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Gerstorf, D.; Ram, N.; Goebel, J.; Schupp, J.; Lindenberger, U.; Wagner, G.G. Where people live and die makes a difference: Individual and geographic disparities in well-being progression at the end of life. Psychol. Aging 2010, 25, 661–676. [Google Scholar] [CrossRef] [Green Version]
- Pinquart, M.; Sörensen, S. Gender Differences in Self-Concept and Psychological Well-Being in Old Age: A Meta-Analysis. J. Gerontol. Ser. B 2001, 56, P195–P213. [Google Scholar] [CrossRef]
- Marmot, M.; Wilkinson, R. Social Determinants of Health; Oup Oxford: Oxford, UK, 2005. [Google Scholar]


{kind=link}
| Chronic Condition | Disease Category |
|---|---|
| Hypertension, diabetes, obesity (BMI ≥ 30) | Cardiometabolic conditions |
| Myocardial infarction, chronic heart failure, stroke, coronary heart disease | Cardiovascular disease |
| Osteoarthrosis, rheuma, osteoporosis, chronic pain (e.g., back pain) | Musculoskeletal disease |
| Depression | Depression |
| Dementia (e.g., Alzheimer’s) | Dementia |
| Lung disease (e.g., COPD) | Lung disease |
| Eye disease (e.g., cataract), hearing impairment | Sensory limitations |
| Cancer (in the past 5 years) | Cancer |
| Incontinence | Incontinence |
| Dizziness/Vertigo | Dizziness |
| Characteristics | All | By Age Group | By Gender | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 60+ Years | 60–64 Years | 65–69 Years | 70–74 Years | 75–79 Years | 80–84 Years | 85+ Yars | Women | Men | |
| (N = 2399) | (N = 376) | (N = 455) | (N = 379) | (N = 470) | (N = 480) | (N = 239) | (N = 1254) | (N = 1136) | |
| 100% | 19.6% | 19.9% | 15.0% | 20.3% | 15.7% | 9.5% | 52.5% | 47.6% | |
| Wtd. % | Wtd. % | Wtd. % | Wtd. % | Wtd. % | Wtd. % | Wtd. % | Wtd. % | Wtd. % | |
| Gender | |||||||||
| Women | 52.5 | 50.8 | 52.5 | 57.2 | 53.9 | 51.3 | 47.1 | n/a | n/a |
| Men | 47.6 | 49.2 | 47.5 | 42.8 | 46.1 | 48.8 | 52.9 | n/a | n/a |
| Age Group | |||||||||
| 60–64 years | n/a | n/a | n/a | n/a | n/a | n/a | n/a | 19.0 | 20.3 |
| 65–69 years | n/a | n/a | n/a | n/a | n/a | n/a | n/a | 19.9 | 19.9 |
| 70–74 years | n/a | n/a | n/a | n/a | n/a | n/a | n/a | 16.3 | 13.4 |
| 75–79 years | n/a | n/a | n/a | n/a | n/a | n/a | n/a | 20.9 | 19.7 |
| 80–84 years | n/a | n/a | n/a | n/a | n/a | n/a | n/a | 15.4 | 16.2 |
| 85+ years | n/a | n/a | n/a | n/a | n/a | n/a | n/a | 8.5 | 10.6 |
| Family status | |||||||||
| Single | 4.7 | 7.8 | 6.0 | 4.6 | 3.2 | 1.9 | 3.8 | 4.3 | 5.1 |
| Married | 69.1 | 72.1 | 72.3 | 73.7 | 73.4 | 63.4 | 49.6 | 60.4 | 78.9 |
| Divorced | 10.7 | 16.1 | 14.0 | 9.1 | 7.6 | 7.5 | 6.7 | 12.7 | 8.2 |
| Widowed | 15.5 | 4.0 | 7.8 | 12.6 | 15.8 | 27.2 | 39.9 | 22.5 | 7.8 |
| Country of birth | |||||||||
| Germany | 94.9 | 96.0 | 97.1 | 97.6 | 91.4 | 93.5 | 93.7 | 95.1 | 94.7 |
| Other | 5.1 | 4.0 | 2.9 | 2.4 | 8.6 | 6.5 | 6.3 | 4.9 | 5.3 |
| SES | |||||||||
| Low | 15.5 | 10.6 | 8.5 | 13.5 | 15.5 | 23.8 | 33.7 | 19.8 | 11.1 |
| Middle | 45.4 | 43.5 | 49.5 | 54.1 | 50.7 | 35.6 | 29.3 | 49.9 | 40.3 |
| High | 39.2 | 45.9 | 42.1 | 32.4 | 33.8 | 40.6 | 37.0 | 30.3 | 48.6 |
| Chronic Condition | All | Women | Men |
|---|---|---|---|
| (N = 2219) | (N = 1166) | (N = 1053) | |
| Wtd. % (95% CI) | Wtd. % (95% CI) | Wtd. % (95% CI) | |
| No chronic conditions | 8.4 (7.4–9.6) | 8.7 (7.2–10.4) | 8.2 (6.8–10.0) |
| Cardiometabolic conditions | 62.9 (60.9–64.8) | 61.0 (58.3–63.7) | 64.8 (61.9–67.5) |
| Diabetes | 18.2 (16.7–19.8) | 16.3 (14.4–18.4) | 20.2 (18.0–22.7) |
| Hypertension | 52.3 (50.4–54.3) | 50.9 (48.2–53.7) | 54.0 (51.5–56.9) |
| Obesity | 20.4 (18.9–22.1) | 21.6 (19.3–24.0) | 19.0 (16.8–21.4) |
| Cardiovascular disease | 19.2 (17.7–20.8) | 14.9 (13.0–17.0) * | 24.2 (21.8–26.7) * |
| Heart failure | 7.5 (6.5–8.7) | 6.7 (5.5–8.2) | 8.5 (7.0–10.3) |
| Coronary heart disease | 8.9 (8.8–9.1) | 7.5 (6.2–9.1) * | 13.9 (12.0–16.0) * |
| Cardiac infarction | 4.1 (3.4–5.0) | 2.2 (1.5–3.2) * | 6.2 (5.0–7.8) * |
| Stroke | 3.8 (3.2–4.6) | 2.8 (2.0–3.9) | 4.9 (3.8–6.3) |
| Lung disease | 7.0 (6.1–8.1) | 7.6 (6.3–9.2) | 6.4 (5.1–8.0) |
| Cancer (in the past 5 years) | 9.0 (7.9–10.2) | 6.8 (5.5–8.3) * | 11.5 (9.8–13.5) * |
| Musculoskeletal disease | 51.6 (49.6–53.6) | 59.7 (57.0–62.4) | 42.4 (39.6–45.3) |
| Arthrosis | 31.2 (29.4–33.1) | 37.3 (34.7–40.0) * | 24.3 (21.9–26.9) * |
| Rheumatism | 4.8 (4.0–5.7) | 5.8 (4.6–7.2) | 3.8 (2.8–5.0) |
| Osteoporosis | 12.6 (11.3–13.9) | 19.2 (17.2–21.5) * | 5.1 (4.0–6.6) * |
| Chronic pain (e.g., back pain) | 30.8 (28.9–32.6) | 37.2 (34.5–39.9) * | 23.6 (21.1–26.1) * |
| Depression | 7.0 (6.0–8.0) | 8.8 (7.3–10.5) * | 4.8 (3.7–6.2) * |
| Sensory impairment | 35.0 (33.1–37.0) | 34.6 (32.0–37.3) | 35.5 (32.8–38.3) |
| Eye disease | 22.8 (21.1–24.5) | 24.5 (22.2–26.9) | 20.9 (18.6–23.3) |
| Hearing impairment | 20.6 (19.0–22.2) | 17.9 (15.9–20.1) * | 23.6 (21.2–26.1) * |
| Incontinence | 7.6 (6.6–8.7) | 9.1 (7.6–10.8) * | 6.0 (4.7–7.5) * |
| Dizziness/vertigo | 11.4 (10.2–12.7) | 13.4 (11.6–15.4) * | 9.3 (7.7–11.1) * |
| Dementia | 0.9 (0.6–1.3) | 1.0 (0.5–1.7) | 0.8 (0.4–1.5) |
| Gender | Age Group | SES | ||||||
|---|---|---|---|---|---|---|---|---|
| Chronic Condition | Men vs. Women (Ref.) | 65–69 yrs. vs. 60–64 yrs. (Ref.) | 70–74 yrs. vs. 60–64 yrs. (Ref.) | 75–79 yrs. vs. 60–64 yrs. (Ref.) | 80–84 yrs. vs. 60–64 yrs. (Ref.) | 85+ yrs vs. 60–64 yrs. (Ref.) | Middle vs.High SES (Ref.) | Low vs. High SES (Ref.) |
| RR (95% CI) | RR (95% CI) | RR (95% CI) | RR (95% CI) | RR (95% CI) | RR (95% CI) | RR (95% CI) | RR (95% CI) | |
| Cardiometabolic conditions | 1.20 (1.02–1.18) | 1.19 (1.04–1.36) | 1.33 (1.17–1.52) | 1.24 (1.09–1.42) | 1.27 (1.12–1.45) | 1.36 (1.18–1.57) | 1.11 (1.03–1.21) | 1.16 (1.04–1.28) |
| Diabetes | 1.38 (1.13–1.69) | 1.66 (1.09–2.53) | 2.62 (1.76–3.92) | 1.94 (1.29–2.92) | 2.26 (1.51–3.38) | 2.39 (1.53–3.72) | 1.45 (1.16–1.83) | 1.58 (1.18–2.11) |
| Hypertension | 1.11 (1.02–1.22) | 1.18 (1.00–1.39) | 1.36 (1.15–1.60) | 1.37 (1.17–1.60) | 1.42 (1.21–1.66) | 1.47 (1.23–1.75) | 1.14 (1.04–1.26) | 1.09 (0.95–1.23) |
| Obesity | 0.97 (0.80–1.17) | 0.88 (0.67–1.16) | 1.03 (0.78–1.36) | 0.69 (0.51–0.93) | 0.50 (0.35–0.70) | 0.53 (0.35–0.80) | 1.17 (0.94–1.45) | 1.77 (1.37–2.29) |
| Cardiovascular disease | 1.70 (1.40–2.07) | 1.12 (0.71–1.77) | 1.96 (1.28–3.00) | 2.64 (1.78–3.90) | 2.98 (2.02–4.39) | 2.98 (2.02–4.39) | 1.06 (0.86–1.31) | 1.23 (0.95–1.59) |
| Heart failure | 1.25 (0.89–1.76) | 1.70 (0.77–3.74) | 2.00 (0.89–4.46) | 3.28 (1.60–6.76) | 4.24 (2.10–10.93) | 5.26 (2.53–10.92) | 1.08 (0.75–1.55) | 1.11 (0.70–1.77) |
| Coronary heart disease | 2.01 (1.50–2.67) | 1.38 (0.70–2.71) | 2.32 (1.22–4.42) | 2.92 (1.60–5.32) | 3.59 (1.99–6.46) | 4.64 (2.53–8.48) | 1.30 (0.95–1.78) | 1.62 (1.11–2.34) |
| Cardiac infarction | 2.90 (1.75–4.79) | 0.58 (0.21–1.60) | 1.98 (0.88–4.46) | 1.96 (0.91–4.24) | 1.92 (0.88–4.15) | 2.20 (0.94–5.12) | 0.88 (0.54–1.43) | 1.03 (0.55–1.94) |
| Stroke | 1.72 (1.05–2.81) | 0.65 (0.23–1.84) | 1.72 (0.72–4.14) | 1.35 (0.56–3.25) | 1.90 (0.82–4.43) | 3.38 (1.44–7.93) | 0.91 (0.55–1.53) | 1.43 (0.76–2.71) |
| Lung disease | 0.82 (0.58–1.18) | 1.32 (0.77–2.27) | 1.19 (0.67–2.13) | 0.78 (0.42–1.46) | 1.29 (0.74–2.26) | 0.99 (0.48–2.05) | 1.11 (0.75–1.65) | 1.56 (0.94–2.57) |
| Cancer (in the past 5 years) | 1.66 (1.23–2.23) | 1.04 (0.61–1.79) | 1.34 (0.78–2.31) | 1.49 (0.91–2.46) | 1.77 (1.09–2.88) | 1.75 (1.00–3.06) | 0.98 (0.72–1.34) | 1.19 (0.79–1.79) |
| Musculoskeletal disease | 0.72 (0.65–0.79) | 0.94 (0.79–1.11) | 1.02 (0.86–1.21) | 1.27 (1.09–1.63) | 1.40 (1.21–1.63) | 1.49 (1.27–1.75) | 1.17 (1.06–1.30) | 1.20 (1.06–1.36) |
| Arthrosis | 0.65 (0.56–0.75) | 0.94 (0.73–1.19) | 1.03 (0.80–1.32) | 1.19 (0.94–1.49) | 1.52 (1.21–1.90) | 1.56 (1.21–2.01) | 1.08 (0.88–1.32) | 1.20 (1.03–1.39) |
| Rheumatism | 0.83 (0.54–1.28) | 0.71 (0.31–1.62) | 0.45 (0.16–1.25) | 2.21 (1.15–4.29) | 1.74 (0.87–3.47) | 1.07 (0.45–2.58) | 1.23 (0.75–2.01) | 1.77 (0.99–3.15) |
| Osteoporosis | 0.25 (0.18–0.35) | 1.26 (0.71–2.21) | 1.47 (0.83–2.61) | 2.35 (1.42–3.90) | 2.51 (1.50–4.20) | 4.46 (2.67–7.46) | 1.18 (0.62–1.14) | 1.18 (0.84–1.66) |
| Chronic pain (e.g., chronic back pain) | 0.66 (0.57–0.77) | 0.87 (0.67–1.13) | 0.84 (0.64–1.11) | 1.37 (1.09–1.72) | 1.39 (1.10–1.76 | 1.57 (1.21–2.02) | 1.32 (1.12–1.56) | 1.43 (1.17–1.76) |
| Depression | 0.51 (0.35–75) | 0.86 (0.54–1.36) | 0.45 (0.25–0.83) | 0.47 (0.27–0.82) | 0.72 (0.43–1.20) | 0.39 (0.17–0.90) | 1.17 (0.79–1.71) | 1.18 (0.68–2.04) |
| Sensory impairment | 1.15 (0.85–1.55) | 11.01 (1.45–83.91) | 7.76 (0.96–62.82) | - * | - * | - * | 1.14 (0.81–1.59) | 1.21 (0.82–1.77) |
| Eye disease | 0.88 (0.74–1.05) | 1.74 (1.06–2.88) | 2.69 (1.65–4.38) | 4.78 (3.06–7.46) | 5.69 (3.66–8.85) | 7.36 (4.70–11.55) | 0.90 (0.75–1.09) | 0.99 (0.78–1.25) |
| Hearing impairment | 1.33 (1.11–1.60) | 1.21 (0.76–1.91) | 1.83 (1.18–2.85) | 2.51 (1.68–3.77) | 4.01 (2.74–5.88) | 5.71 (3.90–8.35) | 1.21 (0.99–1.47) | 1.11 (0.87–1.42) |
| Incontinence | 0.58 (0.42–0.82) | 1.17 (0.48–2.87) | 2.49 (1.10–5.63) | 3.45 (1.61–7.41) | 5.37 (2.56–11.28) | 7.86 (3.71–16.65) | 0.90 (0.62–1.29) | 1.09 (0.72–1.65) |
| Dizziness | 0.73 (0.56–0.96) | 1.21 (0.65–2.27) | 1.61 (0.87–2.99) | 2.16 (1.23–3.80) | 3.75 (2.20–6.38) | 5.08 (2.95–8.77) | 1.15 (0.85–1.57) | 1.46 (1.03–2.07) |
| Dementia | 1.11 (0.39–3.11) | - | 1.05 (0.06–17.3) | 2.46 (0.24–24.8) | 5.68 (0.74–43.78) | 6.72 (0.83–56.61) | 1.37 (0.36–5.28) | 3.33 (0.94–11.76) |
| Variables | Presence of Multimorbidity Wtd. % (95% CI) | Risk of Multimorbidity RR * (95% CI) |
|---|---|---|
| Gender | ||
| Women | 72.7 (70.1–75.1) | 1.00 (Ref.) |
| Men | 73.6 (70.9–76.2) | 1.05 (0.98–1.11) |
| Age Group | ||
| 60–64 years | 57.7 (52.7–62.6) | 1.00 (Ref.) |
| 65–69 years | 62.4 (57.9–66.8) | 1.10 (0.97–1.24) |
| 70–74 years | 74.1 (69.5–78.3) | 1.27 (1.14–1.43) |
| 75–79 years | 78.9 (75.0–82.4) | 1.37 (1.24–1.53) |
| 80–84 years | 86.9 (83.5–88.6) | 1.51 (1.37–1.67) |
| 85+ years | 90.8 (86.4–93.9) | 1.55 (1.39–1.72) |
| SES | ||
| High | 67.1 (63.6–70.5) | 1.00 (Ref.) |
| Middle | 73.2 (70.1–76.1) | 1.10 (1.03–1.17) |
| Low | 82.2 (77.5–86.3) | 1.15 (1.07–1.24) |
| Characteristics | Care Dependency | RR ‡ (95% CI) | |
|---|---|---|---|
| No | Yes | ||
| (N = 2063) | (N = 293) | ||
| Wtd. % (95% CI) | Wtd. % (95% CI) | ||
| Sex | |||
| Women | 86.3 (84.2–88.1) | 13.7 (11.9–15.7) | 1.00 (Ref.) |
| Men | 91.3 (89.5–92.8) | 8.7 (7.2–10.5) | 0.97 (0.95, 0.99) * |
| Age Group | |||
| 60–64 years | 98.9 (97.4, 99.5) | 1.1 (0.5, 2.6) | 1.00 (Ref.) |
| 65–69 years | 97.8 (96.0, 98.8) | 2.2 (1.2, 4.0) | 1.01 (1.00, 1.03) |
| 70–74 years | 95.2 (92.4, 97.0) | 4.8 (3.0, 7.6) | 1.03 (1.01, 1.06) * |
| 75–79 years | 89.9 (86.9, 92.3) | 10.1 (7.7, 13.1) | 1.08 (1.05, 1.11) * |
| 80–84 years | 77.3 (72.7, 81.3) | 22.7 (18.7, 27.3) | 1.18 (1.13, 1.22) * |
| 85+ years | 53.8 (47.3, 60.3) | 46.2 (39.7, 52.7) | 1.38 (1.32, 1.46) * |
| Socioeconomic Status | |||
| High | 95.1 (93.3, 96.4) | 4.9 (3.6, 6.7) | 1.00 (Ref.) |
| Middle | 91.3 (89.3, 93.1) | 8.7 (7.0, 10.7) | 1.04 (1.02, 1.06) * |
| Low | 75.5 (70.3, 80.1) | 24.5 (19.9, 29.7) | 1.12 (1.08, 1.16) * |
| Characteristics | All | Women | Men |
|---|---|---|---|
| (N = 2399) | (N = 1254) | (N = 1136) | |
| Wtd. % (95% CI) | Wtd. % (95% CI) | Wtd. % (95% CI) | |
| SF-8 | |||
| GH Mean (95% CI) | 44.5 (44.3, 44.8) | 44.2 (43.8, 44.6) | 44.9 (44.6, 45.3) |
| PF Mean (95% CI) | 43.8 (43.5, 44.2) | 43.3 (42.8, 43.9) | 44.4 (43.9, 44.9) |
| RP Mean (95% CI) | 44.7 (44.3, 45.0) | 44.1 (43.6, 44.6) | 45.2 (44.7, 45.8) |
| BP Mean (95% CI) | 48.3 (47.9, 48.7) | 47.3 (46.8, 47.9) | 49.4 (48.9, 50.0) |
| VT Mean (95% CI) | 47.6 (47.3, 47.9) | 46.9 (46.5, 47.4) | 48.3 (47.9, 48.7) |
| SF Mean (95% CI) | 46.1 (45.7, 46.5) | 45.2 (44.7, 45.8) | 47.0 (46.4, 47.6) |
| MH Mean (95% CI) | 48.0 (47.6, 48.4) | 46.7 (46.2, 47.3) | 49.4 (48.9, 49.9) |
| RE Mean (95% CI) | 45.7 (45.4, 46.0) | 45.0 (44.5, 45.5) | 46.5 (46.0, 46.9) |
| PCS-8 Mean (95% CI) | 44.5 (44.0, 44.9) | 43.9 (43.3, 44.5) | 45.1 (44.5, 45.6) |
| MCS-8 Mean (95% CI) | 48.2 (47.7, 48.6) | 46.8 (46.2, 47.4) | 49.6 (49.1, 50.2) |
| WHO-5 | |||
| Mean (95% CI) | 58.3 (57.3, 59.2) | 55.3 (54.0, 56.7) | 61.4 (60.1, 62.7) |
| Depressivity | |||
| No | 66.3 (64.4, 68.2) | 61.9 (59.0, 64.6) | 71.1 (68.3, 73.8) |
| Yes | 33.7 (31.8, 35.6) | 38.1 (35.4, 41.0) | 28.9 (26.2, 31.7) |
| Variables | PCS-8 β † (95% CI) | MCS-8 β † (95% CI) | Well-Being β † (95% CI) | Depressivity RR ‡ (95% CI) |
|---|---|---|---|---|
| Sex | ||||
| Women | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| Men | 0.36 (−0.51, 1.22) | 2.43 (1.50, 3.36) * | 5.16 (3.06–7.26) * | 0.78 (0.68–0.89) * |
| Age Group | ||||
| 60–64 years | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 65–69 years | 0.18 (−1.11, 1.47) | 1.82 (0.44, 3.20) * | 4.14 (1.00, 7.28) * | 0.78 (0.62–0.98) * |
| 70–74 years | −2.74 (−4.18, −1.30)* | 1.82 (0.29, 3.36) * | 3.63 (0.13, 7.14) * | 0.89 (0.70–1.13) |
| 75–79 years | −4.84 (−6.16, −3.52) * | 0.15 (−1.26, 1.57) | −1.06 (−4.26, 2.15) | 1.12 (0.91–1.39) |
| 80–84 years | −7.29 (−8.77, −5.82) * | −0.13 (−1.71, 1.44) | −3.74 (−7.31, −0.17) * | 1.14 (0.92–1.42) |
| 85+ years | −9.98 (−11.7, −8.25) * | 0.05 (−1.79, 1.90) | −5.72 (−9.86, −1.59) * | 1.28 (1.01–1.63) * |
| SES | ||||
| High | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| Middle | −2.59 (−3.53, −1.64) * | −2.00 (−3.00, −0.99) * | −4.40 (−6.67, −2.12) * | 1.24 (1.06–1.45) * |
| Low | −5.11 (−6.44, −3.78) * | −3.17 (−4.59, −1.75) * | −7.60 (−10,79, −4.41) * | 1.43 (1.18–1.73) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero Starke, K.; Hegewald, J.; Schmauder, S.; Kaboth, P.; Uhlmann, L.M.; Reissig, D.; Kaufmann, K.K.; Wegge, J.; Marquardt, G.; Seidler, A. Health and Care Dependency of Older Adults in Dresden, Germany: Results from the LAB60+ Study. Int. J. Environ. Res. Public Health 2022, 19, 11777. https://doi.org/10.3390/ijerph191811777
Romero Starke K, Hegewald J, Schmauder S, Kaboth P, Uhlmann LM, Reissig D, Kaufmann KK, Wegge J, Marquardt G, Seidler A. Health and Care Dependency of Older Adults in Dresden, Germany: Results from the LAB60+ Study. International Journal of Environmental Research and Public Health. 2022; 19(18):11777. https://doi.org/10.3390/ijerph191811777
Chicago/Turabian StyleRomero Starke, Karla, Janice Hegewald, Stefanie Schmauder, Pauline Kaboth, Lena Marie Uhlmann, David Reissig, Kristin Klaudia Kaufmann, Jürgen Wegge, Gesine Marquardt, and Andreas Seidler. 2022. "Health and Care Dependency of Older Adults in Dresden, Germany: Results from the LAB60+ Study" International Journal of Environmental Research and Public Health 19, no. 18: 11777. https://doi.org/10.3390/ijerph191811777