
Physical Functions among Children before and during the COVID-19 Pandemic: A Prospective Longitudinal Observational Study (Stage 1)

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
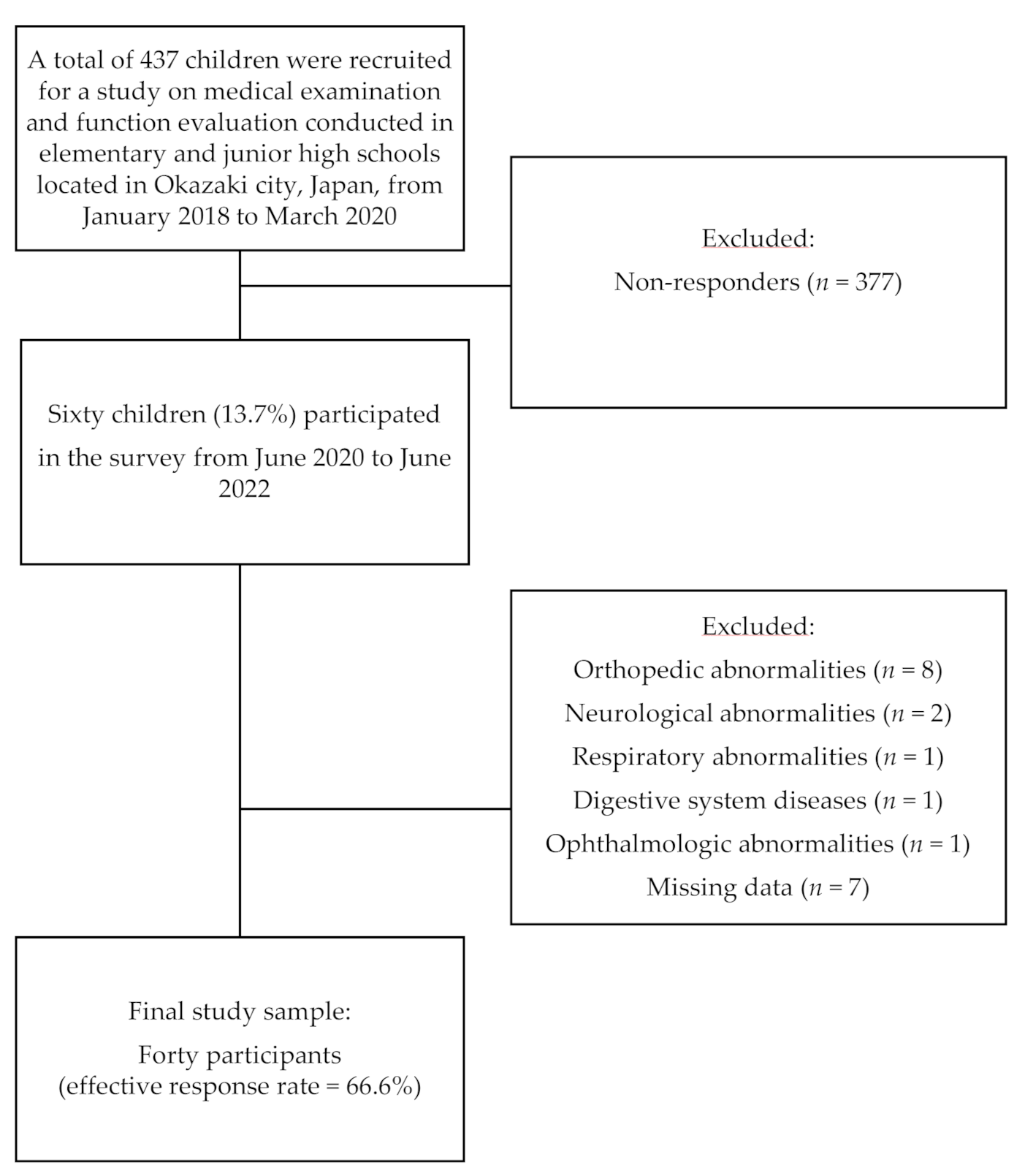
2.1. Study Design and Population
2.2. Data Collection
2.2.1. FTSST
2.2.2. Two-Step Test
2.2.3. One-Legged Stance Test
2.2.4. Gait Analysis
2.2.5. Body Fat Percentage
2.2.6. Questionnaires
2.2.7. Sample Size
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Okuyama, J.; Seto, S.; Fukuda, Y.; Funakoshi, S.; Amae, S.; Onobe, J.; Izumi, S.; Ito, K.; Imamura, F. Mental health and physical activity among children and adolescents during the COVID-19 pandemic. Tohoku J. Exp. Med. 2021, 253, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Ito, T.; Sugiura, H.; Ito, Y.; Noritake, K.; Ochi, N. Effect of the COVID-19 emergency on physical function among school-aged children. Int. J. Environ. Res. Public Health 2021, 18, 9620. [Google Scholar] [CrossRef] [PubMed]
- Riazi, N.A.; Wunderlich, K.; Gierc, M.; Brussoni, M.; Moore, S.A.; Tremblay, M.S.; Faulkner, G. ‘You can’t go to the park, you can’t go here, you can’t go there’: Exploring parental experiences of COVID-19 and its impact on their children’s movement behaviours. Children 2021, 8, 219. [Google Scholar] [CrossRef] [PubMed]
- Pombo, A.; Luz, C.; de Sá, C.; Rodrigues, L.P.; Cordovil, R. Effects of the COVID-19 lockdown on Portuguese children’s motor competence. Children 2021, 8, 199. [Google Scholar] [CrossRef]
- Ten Velde, G.; Lubrecht, J.; Arayess, L.; van Loo, C.; Hesselink, M.; Reijnders, D.; Vreugdenhil, A. Physical activity behaviour and screen time in Dutch children during the COVID-19 pandemic: Pre-, during- and post-school closures. Pediatr. Obes. 2021, 16, e12779. [Google Scholar] [CrossRef]
- Susilowati, I.H.; Nugraha, S.; Alimoeso, S.; Hasiholan, B.P. Screen time for preschool children: Learning from home during the COVID-19 pandemic. Glob. Pediatr. Health 2021, 8, 2333794X211017836. [Google Scholar] [CrossRef]
- Wunsch, K.; Nigg, C.; Niessner, C.; Schmidt, S.C.E.; Oriwol, D.; Hanssen-Doose, A.; Burchartz, A.; Eichsteller, A.; Kolb, S.; Worth, A.; et al. The impact of COVID-19 on the interrelation of physical activity, screen time and health-related quality of life in children and adolescents in Germany: Results of the Motorik-Modul study. Children 2021, 8, 98. [Google Scholar] [CrossRef]
- Neshteruk, C.D.; Zizzi, A.; Suarez, L.; Erickson, E.; Kraus, W.E.; Li, J.S.; Skinner, A.C.; Story, M.; Zucker, N.; Armstrong, S.C. Weight-Related Behaviors of Children with Obesity during the COVID-19 Pandemic. Child Obes. 2021, 17, 371–378. [Google Scholar] [CrossRef]
- Surekha, B.C.; Karanati, K.; Venkatesan, K.; Sreelekha, B.C.; Kumar, V.D. E-Learning During COVID-19 Pandemic: A Surge in Childhood Obesity. Indian J. Otolaryngol. Head Neck Surg. 2021, 14, 1–7. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Otto, C.; Devine, J.; Löffler, C.; Hurrelmann, K.; Bullinger, M.; Barkmann, C.; Siegel, N.A.; et al. Quality of life and mental health in children and adolescents during the first year of the COVID-19 pandemic: Results of a two-wave nationwide population-based study. Eur. Child Adolesc. Psychiatry 2021, 12, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Sugiura, H.; Ito, Y.; Noritake, K.; Ochi, N. Relationship between the skeletal muscle mass index and physical activity of Japanese children: A cross-sectional, observational study. PLoS ONE 2021, 16, e0251025. [Google Scholar] [CrossRef]
- Gu, Y.; Ito, T.; Ito, Y.; Noritake, K.; Ochi, N.; Matsunaga, N.; Takahashi, D.; Sugiura, H. Factors related to locomotive syndrome in school-aged children in Okazaki: A cross-sectional study. Healthcare 2021, 9, 1595. [Google Scholar] [CrossRef]
- Pujia, R.; Ferro, Y.; Maurotti, S.; Khoory, J.; Gazzaruso, C.; Pujia, A.; Montalcini, T.; Mazza, E. The Effects of COVID-19 on the Eating Habits of Children and Adolescents in Italy: A Pilot Survey Study. Nutrients 2021, 13, 2641. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Martínez, A.M.; Ramírez-Vélez, R.; García-Alonso, Y.; Izquierdo, M.; García-Hermoso, A. Physical Activity, Sedentary Behavior, Sleep and Self-Regulation in Spanish Preschoolers during the COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 693. [Google Scholar] [CrossRef] [PubMed]
- Chambonniere, C.; Lambert, C.; Fearnbach, N.; Tardieu, M.; Fillon, A.; Genin, P.; Larras, B.; Melsens, P.; Bois, J.; Pereira, B.; et al. Effect of the COVID-19 lockdown on physical activity and sedentary behaviors in French children and adolescents: New results from the ONAPS national survey. Eur. J. Integr. Med. 2021, 43, 101308. [Google Scholar] [CrossRef]
- Rúa-Alonso, M.; Rial-Vázquez, J.; Nine, I.; Lete-Lasa, J.R.; Clavel, I.; Giráldez-García, M.A.; Rodríguez-Corral, M.; Dopico-Calvo, X.; Iglesias-Soler, E. Comparison of physical fitness profiles obtained before and during COVID-19 pandemic in two independent large samples of children and adolescents: DAFIS project. Int. J. Environ. Res. Public Health 2022, 19, 3963. [Google Scholar] [CrossRef]
- Raven, J.; Raven, J.C.; Court, J.H. Manual for Raven’s Progressive Matrices and Vocabulary Scales; Oxford Psychologists Press: Oxford, UK, 1998. [Google Scholar]
- Ueno, K.; Nagoshi, N.; Konuki, S. Picture vocabulary test-revised. In Nihon Bunka Kagakusha; Tokyo, Japan, 2008. [Google Scholar]
- Abbruzzese, L.D.; Ruggeri, A.R.; Esquerre, J.C.; Patel, P.; Raske, L. Feasibility and reliability of functional mobility measures in children with cri du chat (5P-) Syndrome. Pediatr. Phys. Ther. 2020, 32, 161–167. [Google Scholar] [CrossRef]
- Stansfield, B.W.; Hillman, S.J.; Hazlewood, M.E.; Lawson, A.M.; Mann, A.M.; Loudon, I.R.; Robb, J.E. Normalisation of gait data in children. Gait Posture 2003, 17, 81–87. [Google Scholar] [CrossRef]
- Leboeuf, F.; Baker, R.; Barré, A.; Reay, J.; Jones, R.; Sangeux, M. The conventional gait model, an open-source implementation that reproduces the past but prepares for the future. Gait Posture 2019, 69, 235–241. [Google Scholar] [CrossRef]
- Ito, T.; Noritake, K.; Ito, Y.; Tomita, H.; Mizusawa, J.; Sugiura, H.; Matsunaga, N.; Ochi, N.; Sugiura, H. Three-dimensional gait analysis of lower extremity gait parameters in Japanese children aged 6 to 12 years. Sci. Rep. 2022, 12, 7822. [Google Scholar] [CrossRef]
- Deconinck, F.J.; De Clercq, D.; Savelsbergh, G.J.; Van Coster, R.; Oostra, A.; Dewitte, G.; Lenoir, M. Differences in gait between children with and without developmental coordination disorder. Motor Control 2006, 10, 125–142. [Google Scholar] [CrossRef]
- Müller, J.; Müller, S.; Baur, H.; Mayer, F. Intra-individual gait speed variability in healthy children aged 1–15 years. Gait Posture 2013, 38, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, T.; Nakayama, T.; Kuru, S. Muscle development in healthy children evaluated by bioelectrical impedance analysis. Brain Dev. 2017, 39, 122–129. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010; Available online: https://www.who.int/publications/i/item/9789241599979 (accessed on 8 January 2020).
- Kobayashi, K.; Kamibeppu, K. Measuring quality of life in Japanese children: Development of the Japanese version of PedsQL. Pediatr Int. 2010, 52, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.K.; Hairi, N.N.; Jalaludin, M.Y.; Majid, H.A. Dietary intake, physical activity and muscle strength among adolescents: The Malaysian Health and Adolescents Longitudinal Research Team (MyHeART) study. BMJ Open 2019, 9, e026275. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A.G. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Yanovich, E.; Bar-Shalom, S. Static and Dynamic Balance Indices among Kindergarten Children: A Short-Term Intervention Program during COVID-19 Lockdowns. Children 2022, 9, 939. [Google Scholar] [CrossRef]
- Martínez-Córcoles, V.; Nieto-Gil, P.; Ramos-Petersen, L.; Ferrer-Torregrosa, J. Balance performance analysis after the COVID-19 quarantine in children aged between 8 and 12 years old: Longitudinal study. Gait Posture 2022, 94, 203–209. [Google Scholar] [CrossRef]
- Wojciechowska-Maszkowska, B.; Borzucka, D.; Rogowska, A.M.; Kuczyński, M. The relationship between postural control and self-reported engagement in physical activity in young and older age. J. Aging Phys. Act. 2016, 24, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Eid, M.A.; Aly, S.M.; Huneif, M.A.; Ismail, D.K. Effect of isokinetic training on muscle strength and postural balance in children with Down’s syndrome. Int. J. Rehabil. Res. 2017, 40, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Condon, C.; Cremin, K. Static balance norms in children. Physiother. Res. Int. 2014, 19, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Jarnig, G.; Kerbl, R.; van Poppel, M.N.M. The impact of COVID-19-related mitigation measures on the health and fitness status of primary school children in Austria: A longitudinal study with data from 708 children measured before and during the ongoing COVID-19 pandemic. Sports 2022, 10, 43. [Google Scholar] [CrossRef] [PubMed]
- Dunton, G.F.; Do, B.; Wang, S.D. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Before the Pandemic | During the Pandemic | p | Effect Size (r) |
|---|---|---|---|---|
| Age (years), median (range) | 9.0 (6–12) | 12 (9–15) | 0.0001 | −0.9 |
| Height (cm), mean (SD) | 133.9 (9.7) | 149.3 (8.8) | 0.0001 | 1.0 |
| Weight (kg), mean (SD) | 28.8 (6.1) | 39.3 (7.9) | 0.0001 | 1.0 |
| Body mass index z-score, mean (SD) | −0.6 (0.8) | −0.5 (0.8) | 0.504 | 0.1 |
| Variable | Before the Pandemic | During the Pandemic | p | Effect Size (r) |
|---|---|---|---|---|
| Five Times Sit-To-Stand test | 21.1 (13.11–34.97) | 20.1 (14.8–34.71) | 0.064 | −0.3 |
| Two-step test | 1.60 (0.14) | 1.55 (0.1) | 0.039 | 0.3 |
| Single leg stance test | 445.4 (39.4−502.3) | 431.1 (136.1−473.5) | 0.861 | −0.03 |
| Gait speed | 0.46 (0.07) | 0.45 (0.05) | 0.415 | 0.1 |
| Body fat percentage (%) | 13.2 (4.5−32) | 16.2 (4.0−37.6) | 0.0001 | −0.7 |
| Variable | Before the Pandemic | During the Pandemic | p | Effect Size (r) |
|---|---|---|---|---|
| Physical activity (hour), median (range) | 3.0 (0–20) | 5.5 (0–20.5) | 0.068 | −0.3 |
| Pediatric Quality of Life Inventory (version 4.0) (points), median (range) | 95.7 (48.9–100) | 95.7 (58.7–100) | 0.371 | −0.1 |
| Number of meals (time), median (range) | 21 (21–21) | 21 (19−21) | 0.102 | −0.3 |
| Screen time (hour), median (range) | 1.5 (0.5–7) | 2.0 (0.3–8.0) | 0.002 | −0.5 |
| Sleep time per day (hour), median (range) | 9 (8−10) | 8 (6−9) | 0.0001 | −0.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, T.; Sugiura, H.; Ito, Y.; Narahara, S.; Noritake, K.; Takahashi, D.; Natsume, K.; Ochi, N. Physical Functions among Children before and during the COVID-19 Pandemic: A Prospective Longitudinal Observational Study (Stage 1). Int. J. Environ. Res. Public Health 2022, 19, 11513. https://doi.org/10.3390/ijerph191811513
Ito T, Sugiura H, Ito Y, Narahara S, Noritake K, Takahashi D, Natsume K, Ochi N. Physical Functions among Children before and during the COVID-19 Pandemic: A Prospective Longitudinal Observational Study (Stage 1). International Journal of Environmental Research and Public Health. 2022; 19(18):11513. https://doi.org/10.3390/ijerph191811513
Chicago/Turabian StyleIto, Tadashi, Hideshi Sugiura, Yuji Ito, Sho Narahara, Koji Noritake, Daiki Takahashi, Kentaro Natsume, and Nobuhiko Ochi. 2022. "Physical Functions among Children before and during the COVID-19 Pandemic: A Prospective Longitudinal Observational Study (Stage 1)" International Journal of Environmental Research and Public Health 19, no. 18: 11513. https://doi.org/10.3390/ijerph191811513