
Factorial Model of Obese Adolescents: The Role of Body Image Concerns and Selective Depersonalization—A Pilot Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
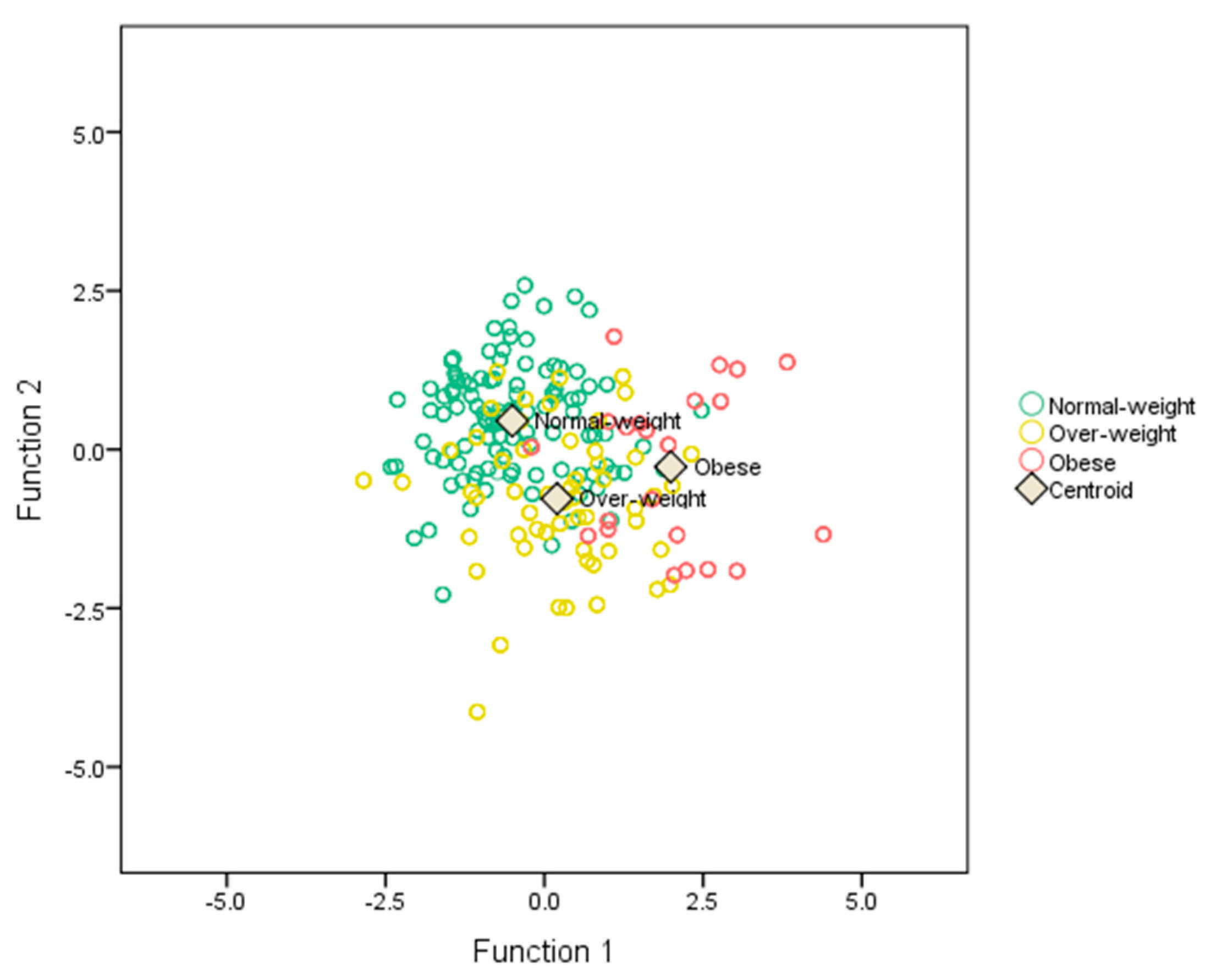
3.2. Stepwise Discriminant Analysis
3.3. Classification Results
3.4. Principal Components Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2018: Building Climate Resilience for Food Security and Nutrition; Food and Agriculture of the United Nations: Rome, Italy, 2018. [Google Scholar]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Ogden, C.L.; Fryar, C.D.; Carroll, M.D.; Flegal, K.M. Mean body weight, height, and body mass index, United States 1960–2002. Adv. Data 2004, 347, 1–17. [Google Scholar]
- Ogden, C.L.; Carroll, M.D.; Curtin, L.R.; McDowell, M.A.; Tabak, C.J.; Flegal, K. Prevalence of Overweight and Obesity in the United States, 1999–2004. JAMA 2006, 295, 1549–1555. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, R.C.; Wright, J.A.; Pepe, M.S.; Seidel, K.D.; Dietz, W.H. Predicting obesity in young adulthood from childhood and parental obesity. New Engl. J. Med. 1997, 337, 869–873. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.S.; Mulder, C.; Twisk, J.W.R.; Van Mechelen, W.; Chinapaw, M.J.M. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Crispino, M.; Trinchese, G.; Penna, E.; Cimmino, F.; Catapano, A.; Villano, I.; Perrone-Capano, C.; Mollica, M.P. Interplay between peripheral and central inflammation in obesity-promoted disorders: The impact on synaptic mitochondrial functions. Int. J. Mol. Sci. 2020, 21, 5964. [Google Scholar] [CrossRef]
- La Marra, M.; Caviglia, G.; Perrella, R. Using Smartphones When Eating Increases Caloric Intake in Young People: An Overview of the Literature. Front. Psychol. 2020, 11, 587886. [Google Scholar] [CrossRef]
- Monda, V.; la Marra, M.; Perrella, R.; Caviglia, G.; Iavarone, A.; Chieffi, S.; Messina, G.; Carotenuto, M.; Monda, M.; Messina, A. Obesity and brain illness: From cognitive and psychological evidences to obesity paradox. Diabetes Metab. Syndr. Obes. Targets Ther. 2017, 10, 473–479. [Google Scholar] [CrossRef]
- Sinha, A.; Kling, S. A Review of Adolescent Obesity: Prevalence, Etiology, and Treatment. Obes. Surg. 2008, 19, 113–120. [Google Scholar] [CrossRef]
- Signoriello, E.; Lus, G.; Polito, R.; Casertano, S.; Scudiero, O.; Coletta, M.; Monaco, M.L.; Rossi, F.; Nigro, E.; Daniele, A. Adiponectin profile at baseline is correlated to progression and severity of multiple sclerosis. Eur. J. Neurol. 2018, 26, 348–355. [Google Scholar] [CrossRef]
- Monda, M.; Messina, G.; Mangoni, C.; De Luca, B. Resting energy expenditure and fat-free mass do not decline during aging in severely obese women. Clin. Nutr. 2008, 27, 657–659. [Google Scholar] [CrossRef] [PubMed]
- De Fusco, C.; Messina, A.; Monda, V.; Viggiano, E.; Moscatelli, F.; Valenzano, A.; Esposito, T.; Sergio, C.; Cibelli, G.; Monda, M.; et al. Osteopontin: Relation between Adipose Tissue and Bone Homeostasis. Stem Cells Int. 2017, 2017, 4045238. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Brownell, K.D.; Foster, G.D. Obesity: Responding to the global epidemic. J. Consult. Clin. Psychol. 2002, 70, 510–525. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.E.; Cohen, P.; Naumova, E.N.; Jacques, P.F.; Must, A. Adolescent obesity and risk for subsequent major depressive disorder and anxiety disorder: Prospective evidence. Psychosom. Med. 2007, 69, 740–747. [Google Scholar] [CrossRef]
- Britz, B.; Siegfried, W.; Ziegler, A.; Lamertz, C.; Herpertz-Dahlmann, B.; Remschmidt, H.; Wittchen, H.-U.; Hebebrand, J. Rates of psychiatric disorders in a clinical study group of adolescents with extreme obesity and in obese adolescents ascertained via a population based study. Int. J. Obes. 2000, 24, 1707–1714. [Google Scholar] [CrossRef]
- Daniels, S.R.; Arnett, D.K.; Eckel, R.H.; Gidding, S.S.; Hayman, L.L.; Kumanyika, S.; Williams, C.L. Overweight in children and adolescents: Pathophysiology, consequences, prevention, and treatment. Circulation 2005, 111, 1999–2012. [Google Scholar] [CrossRef]
- Eisenberg, M.E.; Neumark-Sztainer, D.; Story, M. Associations of weight-based teasing and emotional well-being among adolescents. Arch. Pediatr. Adolesc. Med. 2003, 157, 733–738. [Google Scholar] [CrossRef]
- Fabricatore, A.N.; Wadden, T.A. Psychological aspects of obesity. Clin. Dermatol. 2004, 22, 332–337. [Google Scholar] [CrossRef]
- Franko, D.L.; Striegel-Moore, R.H.; Thompson, D.; Schreiber, G.B.; Daniels, S.R. Does adolescent depression predict obesity in black and white young adult women? Psychol. Med. 2005, 35, 1505–1513. [Google Scholar] [CrossRef]
- Goodman, E.; Whitaker, R.C. A Prospective study of the role of depression in the development and persistence of adolescent obesity. Pediatrics 2002, 110, 497–504. [Google Scholar] [CrossRef]
- Hasler, G.; Pine, D.S.; Kleinbaum, D.G.; Gamma, A.; Luckenbaugh, D.; Ajdacic, V.; Eich, D.; Rössler, W.; Angst, J. Depressive symptoms during childhood and adult obesity: The Zurich Cohort Study. Mol. Psychiatry 2005, 10, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Herva, A.; Laitinen, J.; Miettunen, J.; Veijola, J.; Karvonen, J.T.; Läksy, K.; Joukamaa, M. Obesity and depression: Results from the longitudinal Northern Finland 1966 Birth Cohort Study. Int. J. Obes. 2005, 30, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Kasen, S.; Cohen, P.; Chen, H.; Must, A. Obesity and psychopathology in women: A three decade prospective study. Int. J. Obes. 2007, 32, 558–566. [Google Scholar] [CrossRef]
- Lobstein, T.; Baur, L.; Uauy, R. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5, 4–85. [Google Scholar] [CrossRef] [PubMed]
- Marcus, M.D.; Wildes, J.E. Obesity: Is it a mental disorder? Int. J. Eat. Disord. 2009, 42, 739–753. [Google Scholar] [CrossRef]
- Merten, M.J.; Wickrama, K.A.S.; Williams, A.L. Adolescent obesity and young adult psychosocial outcomes: Gender and racial differences. J. Youth Adolesc. 2008, 37, 1111–1122. [Google Scholar] [CrossRef]
- Richardson, L.P.; Davis, R.; Poulton, R.; McCauley, E.; Moffitt, T.E.; Caspi, A.; Connell, F. A longitudinal evaluation of adolescent depression and adult obesity. Arch. Pediatr. Adolesc. Med. 2003, 157, 739–745. [Google Scholar] [CrossRef]
- Roberts, R.E.; Deleger, S.; Strawbridge, W.J.; Kaplan, G.A. Prospective association between obesity and depression: Evidence from the Alameda County Study. Int. J. Obes. 2003, 27, 514–521. [Google Scholar] [CrossRef]
- Wang, Y.; Lobstein, T. Worldwide trends in childhood overweight and obesity. Pediatr. Obes. 2006, 1, 11–25. [Google Scholar] [CrossRef]
- Wardle, J.; Williamson, S.; Johnson, F.; Edwards, C. Depression in adolescent obesity: Cultural moderators of the association between obesity and depressive symptoms. Int. J. Obes. 2005, 30, 634–643. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- French, S.A.; Story, M.; Perry, C.L. Self-esteem and obesity in children and adolescents: A literature review. Obes. Res. 1995, 3, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Schwimmer, J.B.; Burwinkle, T.M.; Varni, J.W. Health-related quality of life of severely obese children and adolescents. JAMA 2003, 289, 1813–1819. [Google Scholar] [CrossRef] [PubMed]
- Braet, C.; Mervielde, I.; Vandereycken, W. Psychological aspects of childhood obesity: A controlled study in a clinical and nonclinical sample. J. Pediatr. Psychol. 1997, 22, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Erermis, S.; Cetin, N.; Tamar, M.; Bukusoglu, N.; Akdeniz, F.; Goksen, D. Is obesity a risk factor for psychopathology among adolescents? Pediatr. Int. 2004, 46, 296–301. [Google Scholar] [CrossRef]
- Wardle, J.; Cooke, L. The impact of obesity on psychological well-being. Best Pract. Res. Clin. Endocrinol. Metab. 2005, 19, 421–440. [Google Scholar] [CrossRef]
- Hill, A.J. Psychological aspects of obesity. Psychiatry 2005, 4, 26–30. [Google Scholar] [CrossRef]
- Ackard, D.M.; Croll, J.K.; Kearney-Cooke, A. Dieting frequency among college females: Association with disordered eating, body image, and related psychological problems. J. Psychosom. Res. 2002, 52, 129–136. [Google Scholar] [CrossRef]
- Cooley, E.; Toray, T. Body image and personality predictors of eating disorder symptoms during the college years. Int. J. Eat. Disord. 2001, 30, 28–36. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Paxton, S.J.; Hannan, P.J.; Haines, J.; Story, M. Does body satisfaction matter? J. Adolesc. Health 2006, 39, 244–251. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Wall, M.M.; Guo, J.; Story, M.; Haines, J.; Eisenberg, M.E. Obesity, disordered eating, and eating disorders in a longitudinal study of adolescents: How do dieters fare 5 years later? J. Am. Diet. Assoc. 2006, 106, 559–568. [Google Scholar] [CrossRef]
- Rohde, P.; Stice, E.; Marti, C.N. Development and predictive effects of eating disorder risk factors during adolescence: Implications for prevention efforts. Int. J. Eat. Disord. 2014, 48, 187–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Berg, P.; Neumark-Sztainer, D. Fat ‘n happy 5 years later: Is it bad for overweight girls to like their bodies? J. Adolesc. Health 2007, 41, 415–417. [Google Scholar] [CrossRef] [PubMed]
- Cash, T.F.; Phillips, K.A.; Santos, M.T.; Hrabosky, J.I. Measuring “negative body image”: Validation of the body image disturbance questionnaire in a nonclinical population. Body Image 2004, 1, 363–372. [Google Scholar] [CrossRef]
- Grogan, S. Promoting Positive Body Image in Males and Females: Contemporary Issues and Future Directions. Sex Roles 2010, 63, 757–765. [Google Scholar] [CrossRef]
- Chieffi, S.; Iavarone, A.; La Marra, M.; Messina, G.; Villano, I.; Ranucci, S.; Monda, M. Memory for proprioceptive targets in bulimia nervosa. J. Psychiatry. 2015, 18, 297. [Google Scholar]
- Mölbert, S.C.; Sauer, H.; Dammann, D.; Zipfel, S.; Teufel, M.; Junne, F.; Enck, P.; Giel, K.E.; Mack, I. Multimodal Body Representation of Obese Children and Adolescents before and after Weight-Loss Treatment in Comparison to Normal-Weight Children. PLoS ONE 2016, 11, e0166826. [Google Scholar] [CrossRef]
- Bearman, S.K.; Presnell, K.; Martinez, E.; Stice, E. The Skinny on body dissatisfaction: A longitudinal study of adolescent girls and boys. J. Youth Adolesc. 2006, 35, 217–229. [Google Scholar] [CrossRef]
- Caccavale, L.J.; Farhat, T.; Iannotti, R.J. Social engagement in adolescence moderates the association between weight status and body image. Body Image 2012, 9, 221–226. [Google Scholar] [CrossRef]
- Calzo, J.P.; Sonneville, K.R.; Haines, J.; Blood, E.A.; Field, A.E.; Austin, S.B. The development of associations among body mass index, body dissatisfaction, and weight and shape concern in adolescent boys and girls. J. Adolesc. Health 2012, 51, 517–523. [Google Scholar] [CrossRef]
- Barker, E.T.; Galambos, N.L. Body dissatisfaction of adolescent girls and boys: Risk and resource factors. J. Early Adolesc. 2003, 23, 141–165. [Google Scholar] [CrossRef]
- Bucchianeri, M.M.; Arikian, A.J.; Hannan, P.J.; Eisenberg, M.E.; Neumark-Sztainer, D. Body dissatisfaction from adolescence to young adulthood: Findings from a 10-year longitudinal study. Body Image 2012, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Field, A.E.; Camargo, C.A.; Taylor, C.B.; Berkey, C.S.; Roberts, S.B.; Colditz, G.A. Peer, parent, and media influences on the development of weight concerns and frequent dieting among preadolescent and adolescent girls and boys. Pediatrics 2001, 107, 54–60. [Google Scholar] [CrossRef]
- Jones, D.C. Body Image Among Adolescent Girls and Boys: A Longitudinal Study. Dev. Psychol. 2004, 40, 823–835. [Google Scholar] [CrossRef] [PubMed]
- Lawler, M.; Nixon, E. Body dissatisfaction among adolescent boys and girls: The effects of body mass, peer appearance culture and internalization of appearance ideals. J. Youth Adolesc. 2010, 40, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Presnell, K.; Bearman, S.K.; Stice, E. Risk factors for body dissatisfaction in adolescent boys and girls: A prospective study. Int. J. Eat. Disord. 2004, 36, 389–401. [Google Scholar] [CrossRef]
- Quick, V.; Eisenberg, M.E.; Bucchianeri, M.M.; Neumark-Sztainer, D. Prospective predictors of body dissatisfaction in young adults: 10-year longitudinal findings. Emerg. Adulthood 2013, 4, 271–282. [Google Scholar] [CrossRef]
- Tiggemann, M. Body dissatisfaction and adolescent self-esteem: Prospective findings. Body Image 2005, 2, 129–135. [Google Scholar] [CrossRef]
- Elfhag, K. Personality correlates of obese eating behaviour: Swedish universities Scales of Personality and the Three Factor Eating Questionnaire. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2005, 10, 210–215. [Google Scholar] [CrossRef]
- Elfhag, K.; Linné, Y. Gender differences in associations of eating pathology between mothers and their adolescent offspring. Obes. Res. 2005, 13, 1070–1076. [Google Scholar] [CrossRef]
- Van Strien, T. Ice-cream consumption, tendency toward overeating, and personality. Int. J. Eat. Disord. 2000, 28, 460–464. [Google Scholar] [CrossRef]
- Kaplan, H.I.; Kaplan, H.S. The psychosomatic concept of obesity. J. Nerv. Ment. Dis. 1957, 125, 181–201. [Google Scholar] [CrossRef] [PubMed]
- Heatherton, T.F.; Herman, C.P.; Polivy, J. Effects of physical threat and ego threat on eating behaviour. J. Pers. Soc. Psychol. 1991, 60, 138–143. [Google Scholar] [CrossRef]
- van Strien, T.; Ouwens, M.A. Effects of distress, alexithymia and impulsivity on eating. Eat. Behav. 2007, 8, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Adam, T.C.; Epel, E.S. Stress, eating and the reward system. Physiol. Behav. 2007, 91, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Messina, A.; Monda, V. Role of the orexin system on arousal, attention, feeding behaviour and sleep disorders. Acta Med. Mediterr. 2017, 4, 645–649. [Google Scholar] [CrossRef]
- Cavaliere, G.; Viggiano, E.; Trinchese, G.; De Filippo, C.; Messina, A.; Monda, V.; Valenzano, A.; Cincione, R.I.; Zammit, C.; Cimmino, F.; et al. Long Feeding High-Fat Diet Induces Hypothalamic Oxidative Stress and Inflammation, and Prolonged Hypothalamic AMPK Activation in Rat Animal Model. Front. Physiol. 2018, 9, 818. [Google Scholar] [CrossRef]
- Gibson, E.L. The psychobiology of comfort eating: Implications for neuropharmacological interventions. Behav. Pharmacol. 2012, 23, 442–460. [Google Scholar] [CrossRef]
- Messina, A.; Monda, M.; Valenzano, A.; Messina, G.; Villano, I.; Moscatelli, F.; Cibelli, G.; Marsala, G.; Polito, R.; Ruberto, M.; et al. Functional Changes Induced by Orexin A and Adiponectin on the Sympathetic/Parasympathetic Balance. Front. Physiol. 2018, 9, 259. [Google Scholar] [CrossRef]
- Braet, C.; Claus, L.; Verbeken, S.; Van Vlierberghe, L. Impulsivity in overweight children. Eur. Child Adolesc. Psychiatry 2007, 16, 473–483. [Google Scholar] [CrossRef]
- dos Passos, D.R.; Gigante, D.P.; Maciel, F.V.; Matijasevich, A. Children’s eating behaviour: Comparison between normal and overweight children from a school in Pelotas, Rio Grande do Sul, Brazil. Rev. Paul. Pediatr. 2015, 33, 42–49. [Google Scholar]
- Steinsbekk, S.; Barker, E.D.; Llewellyn, C.; Fildes, A.; Wichstrøm, L. Emotional Feeding and Emotional Eating: Reciprocal Processes and the Influence of Negative Affectivity. Child Dev. 2018, 89, 1234–1246. [Google Scholar] [CrossRef] [PubMed]
- Viana, V.; Sinde, S.; Saxton, J.C. Children’s Eating Behaviour Questionnaire: Associations with BMI in Portuguese children. Br. J. Nutr. 2008, 100, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Webber, L.; Hill, C.; Saxton, J.; Van Jaarsveld, C.H.; Wardle, J. Eating behaviour and weight in children. Int. J. Obes. 2008, 33, 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braet, C.; Claus, L.; Goossens, L.; Moens, E.; Van Vlierberghe, L.; Soetens, B. Differences in Eating Style between Overweight and Normal-Weight Youngsters. J. Health Psychol. 2008, 13, 733–743. [Google Scholar] [CrossRef]
- Snoek, H.M.; Van Strien, T.; Janssens, J.M.A.M.; Engels, R. Emotional, external, restrained eating and overweight in Dutch adolescents. Scand. J. Psychol. 2007, 48, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Caccialanza, R.; Nicholls, D.; Cena, H.; Maccarini, L.; Rezzani, C.; Antonioli, L.; Dieli, S.; Roggi, C. Validation of the Dutch Eating Behaviour Questionnaire parent version (DEBQ-P) in the Italian population: A screening tool to detect differences in eating behaviour among obese, overweight and normal-weight preadolescents. Eur. J. Clin. Nutr. 2004, 58, 1217–1222. [Google Scholar] [CrossRef]
- Ebbeling, C.B.; Pawlak, D.B.; Ludwig, D.S. Childhood obesity: Public-health crisis, common sense cure. Lancet 2002, 360, 473–482. [Google Scholar] [CrossRef]
- van Strien, T.; Oosterveld, P. The children’s DEBQ for assessment of restrained, emotional, and external eating in 7- to 12-year-old children. Int. J. Eat. Disord. 2008, 41, 72–81. [Google Scholar] [CrossRef]
- Obese Humans and Ruts; Schachter, S.; Rodin, J. (Eds.) ErlbaumiWiley: Washington, DC, USA, 1974. [Google Scholar]
- Elfhag, K.; Morey, L.C. Personality traits and eating behavior in the obese: Poor self-control in emotional and external eating but personality assets in restrained eating. Eat. Behav. 2008, 9, 285–293. [Google Scholar] [CrossRef]
- Messina, A.; Monda, V. An allied health: The pasta. Acta Med. Mediterr. 2017, 4, 641–644. [Google Scholar] [CrossRef]
- Stice, E.; Spoor, S.; Bohon, C.; Veldhuizen, M.G.; Small, D.M. Relation of reward from food intake and anticipated food intake to obesity: A functional magnetic resonance imaging study. J. Abnorm. Psychol. 2008, 117, 924–935. [Google Scholar] [CrossRef] [PubMed]
- Monda, V.; Polito, R.; Lovino, A.; Finaldi, A.; Valenzano, A.; Nigro, E.; Corso, G.; Sessa, F.; Asmundo, A.; Di Nunno, N.; et al. Short-Term Physiological Effects of a Very Low-Calorie Ketogenic Diet: Effects on Adiponectin Levels and Inflammatory States. Int. J. Mol. Sci. 2020, 21, 3228. [Google Scholar] [CrossRef] [PubMed]
- Field, A.E.; Austin, S.B.; Taylor, C.B.; Malspeis, S.; Rosner, B.; Rockett, H.R.; Gillman, M.W.; Colditz, G.A. Relation between dieting and weight change among preadolescents and adolescents. Pediatrics 2003, 112, 900–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, F.; Wardle, J. Dietary restraint, body dissatisfaction, and psychological distress: A prospective analysis. J. Abnorm. Psychol. 2005, 114, 119–125. [Google Scholar] [CrossRef]
- Stice, E.; Shaw, H.A. Role of body dissatisfaction in the onset and maintenance of eating pathology: A synthesis of research findings. J. Psychosom. Res. 2002, 53, 985–993. [Google Scholar] [CrossRef]
- Claus, L.; Braet, C.; Decaluwé, V. Dieting history in obese youngsters with and without disordered eating. Int. J. Eat. Disord. 2006, 39, 721–728. [Google Scholar] [CrossRef]
- Tanofsky-Kraff, M.; Yanovski, S.Z.; Schvey, N.A.; Olsen, C.H.; Gustafson, J.; Yanovski, J.A. A prospective study of loss of control eating for body weight gain in children at high risk for adult obesity. Int. J. Eat. Disord. 2009, 42, 26–30. [Google Scholar] [CrossRef]
- Pulkki-Råback, L.; Elovainio, M.; Kivimäki, M.; Raitakari, O.T.; Keltikangas-Järvinen, L. Temperament in childhood predicts body mass in adulthood: The cardiovascular risk in young finns study. Health Psychol. 2005, 24, 307–315. [Google Scholar] [CrossRef]
- Hintsanen, M.; Jokela, M.; Cloninger, C.R.; Pulkki-Råback, L.; Hintsa, T.; Elovainio, M.; Josefsson, K.; Rosenström, T.; Mullola, S.; Raitakari, O.T.; et al. Temperament and character predict body-mass index: A population-based prospective cohort study. J. Psychosom. Res. 2012, 73, 391–397. [Google Scholar] [CrossRef]
- Yang, X.; Telama, R.; Hirvensalo, M.; Hintsa, T.; Pulkki-Råback, L.; Hintsanen, M.; Keltikangas-Järvinen, L.; Viikari, J.S.A.; Raitakari, O.T. Leadership component of type A behavior predicts physical activity in early midlife. Int. J. Behav. Med. 2010, 19, 48–55. [Google Scholar] [CrossRef]
- Bree, M.B.V.D.; Przybeck, T.R.; Cloninger, C.R. Diet and personality: Associations in a population-based sample. Appetite 2006, 46, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.A.; Caterson, I.; Seidell, J.C.; James, W.P.T. Diet, nutrition and the prevention of excess weight gain and obesity. Public Health Nutr. 2004, 7, 123–146. [Google Scholar] [PubMed]
- Moscatelli, F.; Messina, G.; Valenzano, A.; Petito, A.; Triggiani, A.I.; Ciliberti, M.A.P.; Monda, V.; Messina, A.; Tafuri, D.; Capranica, L.; et al. Relationship between RPE and Blood Lactate after Fatiguing Handgrip Exercise in Taekwondo and Sed-entary Subjects. Biol. Med. 2015, 1, S3008. [Google Scholar] [CrossRef]
- Villano, I.; La Marra, M.; Messina, A.; Di Maio, G.; Moscatelli, F.; Chieffi, S.; Monda, M.; Messina, G.; Monda, V. Effects of vegetarian and vegan nutrition on body composition in competitive futsal athletes. Prog. Nutr. 2021, 23, e2021126. [Google Scholar] [CrossRef]
- Krebs, H.; Weyers, P.; Janke, W. Validation of the German version of Cloninger’s TPQ: Replication and correlations with stress coping, mood measures and drug use. Pers. Individ. Differ. 1998, 24, 805–814. [Google Scholar] [CrossRef]
- Hwang, J.W.; Lyoo, I.K.; Kim, B.N.; Shin, M.S.; Kim, S.J.; Cho, S.C. The relationship Between temperament and character and psychopathology in community children with overweight. J. Dev. Behav. Pediatr. 2006, 27, 18–24. [Google Scholar] [CrossRef]
- Nederkoorn, C.; Braet, C.; Van Eijs, Y.; Tanghe, A.; Jansen, A. Why obese children cannot resist food: The role of impulsivity. Eat. Behav. 2006, 7, 315–322. [Google Scholar] [CrossRef]
- Villano, I.; Ilardi, C.R.; Arena, S.; Scuotto, C.; Gleijeses, M.G.; Messina, G.; Messina, A.; Monda, V.; Monda, M.; Iavarone, A.; et al. Obese Subjects without Eating Disorders Experience Binge Episodes Also Independently of Emotional Eating and Personality Traits among University Students of Southern Italy. Brain Sci. 2021, 11, 1145. [Google Scholar] [CrossRef]
- Friedman, M.A.; Brownell, K.D. Psychological correlates of obesity: Moving to the next research generation. Psychol. Bull. 1995, 117, 3–20. [Google Scholar] [CrossRef]
- Hassan, A.; De Luca, V.; Dai, N.; Asmundo, A.; Di Nunno, N.; Monda, M.; Villano, I. Effectiveness of Antipsychotics in Reducing Suicidal Ideation: Possible Physiologic Mechanisms. Healthcare 2021, 9, 389. [Google Scholar] [CrossRef]
- Ilardi, C.R.; Chieffi, S.; Scuotto, C.; Gamboz, N.; Galeone, F.; Sannino, M.; Garofalo, E.; La Marra, M.; Ronga, B.; Iavarone, A. The Frontal Assessment Battery 20 years later: Normative data for a shortened version (FAB15). Neurol. Sci. 2021, 43, 1709–1719. [Google Scholar] [CrossRef]
- Cacciari, E.; Milani, S.; Balsamo, A.; Spada, E.; Bona, G.; Cavallo, L.; Cerutti, F.; Gargantini, L.; Greggio, N.; Tonini, G.; et al. Italian cross-sectional growth charts for height, weight and BMI (2 to 20 yr). J. Endocrinol. Investig. 2006, 29, 581–593. [Google Scholar] [CrossRef]
- Garner, D.M. Eating Disorder Inventory-2 Professional Manual; Psychological Assessment Resources: Odessa, Ukraine, 1991. [Google Scholar]
- Rizzardi, M.; Trombini, E.; Trombini, G. EDI-2: Manuale; Organizzazioni Speciali: Firenze, Italy, 1995. [Google Scholar]
- Cuzzolaro, M.; Vetrone, G.; Marano, G.; Garfinkel, P. The Body Uneasiness Test (BUT): Development and validation of a new body image assessment scale. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2006, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Molinari, E. Factor Structure of the Italian Version of the Body Satisfaction Scale: A Multisample Analysis. Percept. Mot. Ski. 1998, 86, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Slade, P.D.; Dewey, M.E.; Newton, T.; Brodie, D.; Kiemle, G. Development and preliminary validation of the body satisfaction scale (BSS). Psychol. Health 1990, 4, 213–220. [Google Scholar] [CrossRef]
- Molinari, E.; Compare, A. Psicologia clinica dell’obesità in età pediatrica. In Salute & Equilibrio Nutrizionale; Giovannini, M., Ed.; Springer: Milano, Italy, 2006; pp. 59–90. [Google Scholar]
- Schlundt, D.G.; Zimering, R.T. The Dieter’s Inventory of Eating Temptations: A Measure of Weight Control Competence. Addict. Behav. 1988, 13, 151–164. [Google Scholar] [CrossRef]
- Baiocco, R.; Giannini, A.M.; Laghi, F.; SAR. Scala Alessitimica Romana. Valutazione delle Capacità di Riconoscere, Esprimere e Verbalizzare le Emozioni. Manuale e Protocolli [RAS. Roman Alexithymic Scale. Evaluation of the Ability to Recognize, Express and Verbalize Emotions. Manual and Protocols]; Erickson: Trento, Italy, 2005. [Google Scholar]
- Armstrong, J.G.; Putnam, F.W.; Carlson, E.; Libero, D.Z.; Smith, S.R. Development and Validation of a Measure of Adolescent Dissociation: The Adolescent Dissociative Experiences Scale. J. Nerv. Ment. Dis. 1997, 185, 491–497. [Google Scholar] [CrossRef]
- Schimmenti, A. Psychometric Properties of the Adolescent Dissociative Experiences Scale (A-DES) in a Sample of Italian Adolescents. J. Trauma Dissociation 2015, 17, 244–257. [Google Scholar] [CrossRef]
- Abbate-Daga, G.; Gramaglia, C.; Malfi, G.; Pierò, A.; Fassino, S. Eating problems and personality traits. An Italian pilot study among 992 high school students. Eur. Eat. Disord. Rev. 2006, 15, 471–478. [Google Scholar] [CrossRef]
- Cloninger, C.R.; Przybeck, T.R.; Svrakic, D.M.; Wetzel, R.D. The Temperament and Character Inventory (TCI): A Guide to Its Development and Use; Washington University: St-Louis, MO, USA, 1994. [Google Scholar]
- Ilardi, C.R.; Garofalo, E.; Chieffi, S.; Gamboz, N.; La Marra, M.; Iavarone, A. Daily exposure to digital displays may affect the clock-drawing test: From psychometrics to serendipity. Neurol. Sci. 2020, 41, 3683–3690. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Cooper, P.J.; Whelan, E.; Woolgar, M.; Morrell, J.; Murray, L. Association between childhood feeding problems and maternal eating disorder: Role of the family environment. Br. J. Psychiatry 2004, 184, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Cooper, M.J.; Rose, K.S.; Turner, H. The specific content of core beliefs and schema in adolescent girls high and low in eating disorder symptoms. Eat. Behav. 2006, 7, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Rushford, N.; Ostermeyer, A. Body image disturbances and their change with videofeedback in anorexia nervosa. Behav. Res. Ther. 1997, 35, 389–398. [Google Scholar] [CrossRef]
- Viken, R.J.; Treat, T.A.; Nosofsky, R.M.; McFall, R.M.; Palmeri, T.J. Modeling individual differences in perceptual and attentional processes related to bulimic symptoms. J. Abnorm. Psychol. 2002, 111, 598–609. [Google Scholar] [CrossRef]
- Groesz, L.M.; Levine, M.P.; Murnen, S.K. The effect of experimental presentation of thin media images on body satisfaction: A meta-analytic review. Int. J. Eat. Disord. 2001, 31, 10005. [Google Scholar] [CrossRef]
- Posavac, S.S.; Posavac, H.D. Predictors of Women’s Concern with Body Weight: The Roles of Perceived Self-Media Ideal Discrepancies and Self-Esteem. Eat. Disord. 2002, 10, 153–160. [Google Scholar] [CrossRef]
- Sands, E.R.; Wardle, J. Internalization of ideal body shapes in 9-12-year-old girls. Int. J. Eat. Disord. 2003, 33, 193–204. [Google Scholar] [CrossRef]
- Ahern, A.L.; Bennett, K.M.; Kelly, M.; Hetherington, M.M. A qualitative exploration of young women’s attitudes towards the thin ideal. J. Health Psychol. 2010, 16, 70–79. [Google Scholar] [CrossRef]
- Bojorquez-Chapela, I.; Unikel, C.; Mendoza, M.-E.; De Lachica, F. Another body project: The thin ideal, motherhood, and body dissatisfaction among Mexican women. J. Health Psychol. 2013, 19, 1120–1131. [Google Scholar] [CrossRef]
- Mask, L.; Blanchard, C.M. The protective role of general self-determination against “thin ideal” media exposure on women’s body image and eating–related concerns. J. Health Psychol. 2011, 16, 489–499. [Google Scholar] [CrossRef]
- Shroff, H.; Thompson, J.K. Peer influences, body-image dissatisfaction, eating dysfunction and self-esteem in adolescent girls. J. Health Psychol. 2006, 11, 533–551. [Google Scholar] [CrossRef] [PubMed]
- Th⊘Gersen-Ntoumani, C.; Ntoumanis, N.; Nikitaras, N. Unhealthy weight control behaviours in adolescent girls: A process model based on self-determination theory. Psychol. Health 2010, 25, 535–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hargreaves, D.; Tiggemann, M. The role of appearance schematicity in the development of adolescent body dissatisfaction. Cogn. Ther. Res. 2002, 26, 691–700. [Google Scholar] [CrossRef]
- Williamson, N.A. Body image disturbance in eating disorders: A form of cognitive bias? Eat. Disord. 1996, 4, 47–58. [Google Scholar] [CrossRef]
- Freeman, R.; Touyz, S.; Sara, G.; Rennie, C.; Gordon, E.; Beumont, P. In the eye of the beholder: Processing body shape information in anorexic and bulimic patients. Int. J. Eat. Disord. 1991, 10, 709–714. [Google Scholar] [CrossRef]
- Jansen, A.; Nederkoorn, C.; Mulkens, A. Selective visual attention for ugly and beautiful body parts in eating disorders. Behav. Res. Ther. 2005, 43, 183–196. [Google Scholar] [CrossRef]
- Jansen, A.; Voorwinde, V.; Hoebink, Y.; Rekkers, M.; Martijn, C.; Mulkens, S. Mirror exposure to increase body satisfaction: Should we guide the focus of attention towards positively or negatively evaluated body parts? J. Behav. Ther. Exp. Psychiatry 2016, 50, 90–96. [Google Scholar] [CrossRef]
- McGuigan, F.J.; Andreassi, J.L. Psychophysiology—Human Behavior and Physiological Response. Am. J. Psychol. 1981, 94, 359. [Google Scholar] [CrossRef]
- Siegle, G.J.; Granholm, E.; E Ingram, R.; Matt, G. Pupillary and reaction time measures of sustained processing of negative information in depression. Biol. Psychiatry 2001, 49, 624–636. [Google Scholar] [CrossRef]
- Gregory, R.L. Eye and brain: The Psychology of Seeing; Princeton University Press: Princeton, NJ, USA, 2015; Volume 80. [Google Scholar]
- Cruz-Sáez, S.; Pascual, A.; Salaberria, K.; Etxebarria, I.; Echeburúa, E. Risky eating behaviors and beliefs among adolescent girls. J. Health Psychol. 2015, 20, 154–163. [Google Scholar] [CrossRef]
- Cramer, P.; Steinwert, T. Thin is good, fat is bad: How early does it begin? J. Appl. Dev. Psychol. 1998, 19, 429–451. [Google Scholar] [CrossRef]
- Staffieri, J.R. A study of social stereotype of body image in children. J. Pers. Soc. Psychol. 1967, 7, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Vener, A.M.; Krupka, L.R.; Gerard, R.J. Overweight/obese patients: An overview. Practitioner 1982, 226, 1102–1109. [Google Scholar] [PubMed]
- Sapuppo, W.; Ruggiero, G.M.; Caselli, G.; Sassaroli, S. The Body of Cognitive and Metacognitive Variables in Eating Disorders: Need of Control, Negative Beliefs about Worry Uncontrollability and Danger, Perfectionism, Self-esteem and Worry. Isr. J. Psychiatry Relat. Sci. 2018, 55, 55–63. [Google Scholar]
- Martin, L.L.; Tesser, A. Some ruminative thoughts. Adv. Soc. Cogn. 1996, 9, 1–47. [Google Scholar]
- Sierra, M.; David, A.S. Depersonalization: A selective impairment of self-awareness. Conscious. Cogn. 2011, 20, 99–108. [Google Scholar] [CrossRef]
- Sierra, M.; Berrios, G. Depersonalization: Neurobiological perspectives. Biol. Psychiatry. 1998, 44, 898–908. [Google Scholar] [CrossRef]
- Reutens, S.; Nielsen, O.; Sachdev, P. Depersonalization disorder. Curr. Opin. Psychol. 2010, 23, 278–283. [Google Scholar] [CrossRef]
- Sierra, M.; David, A.S.; Hunter, E.C.M. The epidemiology of depersonalisation and derealisation. Soc. Psychiatry 2004, 39, 9–18. [Google Scholar] [CrossRef]
- Medford, N.; Sierra, M.; Baker, D.; David, A.S. Understanding and treating depersonalization disorder. Adv. Psychiatr. Treat. 2005, 11, 92–100. [Google Scholar] [CrossRef]
- Baker, D.; Hunter, E.; Lawrence, E.; Medford, N.; Patel, M.; Senior, C.; Sierra, M.; Lambert, M.V.; Phillips, M.L.; David, A.S. Depersonalisation disorder: Clinical features of 204 cases. Br. J. Psychiatry. 2003, 182, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Lemche, E.; Surguladze, S.; Giampietro, V.; Anilkumar, A.; Brammer, M.; Sierra, M.; Chitnis, X.; Williams, S.; Gasston, D.; Joraschky, P.; et al. Limbic and prefrontal response to facial emotion expressions in depersonalisation. Neuroreport 2007, 18, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Medford, N.; Brierley, B.; Brammer, M.; Bullmore, E.T.; David, A.S.; Phillips, M.L. Emotional memory in depersonalization disorder: A functional MRI study. Psychiatry Res. Neuroimaging 2006, 148, 93–102. [Google Scholar] [CrossRef] [PubMed]
- La Marra, M.; Ilardi, C.R.; Villano, I.; Carosella, M.; Staiano, M.; Iavarone, A.; Chieffi, S.; Messina, G.; Polito, R.; Scarinci, A.; et al. Functional Relationship between Inhibitory Control, Cognitive Flexibility, Psychomotor Speed and Obesity. Brain Sci. 2022, 12, 1080. [Google Scholar] [CrossRef] [PubMed]
- La Marra, M.; Villano, I.; Ilardi, C.R.; Carosella, M.; Staiano, M.; Iavarone, A.; Chieffi, S.; Messina, G.; Polito, R.; Porro, C.; et al. Executive Functions in Overweight and Obese Treatment-Seeking Patients: Cross-Sectional Data and Longitudinal Perspectives. Brain Sci. 2022, 12, 777. [Google Scholar] [CrossRef]
- Chieffi, S.; Ilardi, C.R.; Iavarone, A. Parietal lobe dysfunction in schizophrenia: A review. Curr. Psychiatry Rev. 2018, 14, 71–83. [Google Scholar] [CrossRef]
- Chieffi, S.; Castaldi, C.; Di Maio, G.; La Marra, M.; Messina, A.; Monda, V.; Villano, I. Attentional bias in the radial and vertical dimensions of space. Comptes Rendus. Biol. 2019, 342, 97–100. [Google Scholar] [CrossRef]
- Mantovani, A.; Simeon, D.; Urban, N.; Bulow, P.; Allart, A.; Lisanby, S.H. Temporo-parietal junction stimulation in the treatment of depersonalization disorder. Psychiatry Res. 2011, 186, 138–140. [Google Scholar] [CrossRef]
- Simeon, D.; Guralnik, O.; Hazlett, E.A.; Spiegel-Cohen, J.; Hollander, E.; Buchsbaum, M.S. Feeling unreal: A PET study of depersonalization disorder. Am. J. Psychiatry 2000, 157, 1782–1788. [Google Scholar] [CrossRef]
- Ilardi, C.R.; Iavarone, A.; La Marra, M.; Iachini, T.; Chieffi, S. Hand movements in mild cognitive impairment: Clinical implications and insights for future research. J. Integr. Neurosci. 2022, 21, 67. [Google Scholar] [CrossRef]
- Ilardi, C.R.; Chieffi, S.; Iachini, T.; Iavarone, A. Neuropsychology of posteromedial parietal cortex and conversion factors from Mild Cognitive Impairment to Alzheimer’s disease: Systematic search and state-of-the-art review. Aging 2021, 34, 289–307. [Google Scholar] [CrossRef] [PubMed]
- De Vignemont, F. Body schema and body image—Pros and cons. Neuropsychologia 2010, 48, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Dijkerman, H.C.; de Haan, E.H. Somatosensory processes subserving perception and action. Behav. Brain Sci. 2007, 30, 189–201. [Google Scholar] [CrossRef]
- Černelič-Bizjak, M.; Jenko-Pražnikar, Z. Impact of negative cognitions about body image on inflammatory status in relation to health. Psychol. Health 2013, 29, 264–278. [Google Scholar] [CrossRef] [PubMed]
- Chieffi, S.; Messina, A.; Villano, I.; Valenzano, A.A.; Nigro, E.; la Marra, M.; Cibelli, G.; Monda, V.; Salerno, M.; Tafuri, D.; et al. The Use of Velocity Information in Movement Reproduction. Front. Psychol. 2017, 8, 983. [Google Scholar] [CrossRef] [PubMed]
- Chieffi, S.; Messina, G.; Messina, A.; Villano, I.; Monda, V.; Ambra, F.I.; Garofalo, E.; Romano, F.; Mollica, M.P.; Monda, M.; et al. Memory for Spatial Locations in a Patient with Near Space Neglect and Optic Ataxia: Involvement of the Occipitotemporal Stream. Front. Neurol. 2017, 8, 231. [Google Scholar] [CrossRef] [PubMed]
- Chieffi, S.; Messina, G.; Villano, I.; Messina, A.; Ilardi, C.R.; Monda, M.; Salerno, M.; Sessa, F.; Mollica, M.P.; Cavaliere, G.; et al. Hemispheric Asymmetries in Radial Line Bisection: Role of Retinotopic and Spatiotopic Factors. Front. Psychol. 2018, 9, 2200. [Google Scholar] [CrossRef]
- Gallagher, S.; Cole, J. Body image and body schema in a deafferented subject. JMB 1995, 16, 369–389. [Google Scholar]
- Sedda, A.; Scarpina, F. Dorsal and ventral streams across sensory modalities. Neurosci. Bull. 2012, 28, 291–300. [Google Scholar] [CrossRef]
- Monda, V.; Valenzano, A.; Moscatelli, F.; Salerno, M.; Sessa, F.; Triggiani, A.I.; Viggiano, A.; Capranica, L.; Marsala, G.; De Luca, V.; et al. Primary Motor Cortex Excitability in Karate Athletes: A Transcranial Magnetic Stimulation Study. Front. Physiol. 2017, 8, 695. [Google Scholar] [CrossRef]
- Aldosky, H.Y. Impact of obesity and gender differences on electrodermal activities. Gen. Physiol. Biophys. 2019, 38, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Chieffi, S.; Villano, I.; Messina, A.; Monda, V.; La Marra, M.; Messina, G.; Monda, M. Involvement of orexin in sleep disorders and neurodegenerative diseases. Curr. Top. Pept. 2015, 16, 49–54. [Google Scholar]
- Craig, A.D. Significance of the insula for the evolution of human awareness of feelings from the body. Ann. N. Y. Acad. Sci. 2011, 1225, 72–82. [Google Scholar] [CrossRef]
- Critchley, H.D.; Wiens, S.; Rotshtein, P.; Öhman, A.; Dolan, R. Neural systems supporting interoceptive awareness. Nat. Neurosci. 2004, 7, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Villano, I.; La Marra, M.; Di Maio, G.; Monda, V.; Chieffi, S.; Guatteo, E.; Messina, G.; Moscatelli, F.; Monda, M.; Messina, A. Physiological Role of Orexinergic System for Health. Int. J. Environ. Res. Public Health 2022, 19, 8353. [Google Scholar] [CrossRef] [PubMed]
- Farrer, C.; Franck, N.; Georgieff, N.; Frith, C.; Decety, J.; Jeannerod, M. Modulating the experience of agency: A positron emission tomography study. NeuroImage 2003, 18, 324–333. [Google Scholar] [CrossRef]
- Giesbrecht, T.; Merckelbach, H.; Ter Burg, L.; Cima, M.; Simeon, D. Acute dissociation predicts rapid habituation of skin conductance responses to aversive auditory probes. J. Trauma. Stress 2008, 21, 247–250. [Google Scholar] [CrossRef]
- Scarpina, F.; Castelnuovo, G.; Molinari, E. Tactile mental body parts representation in obesity. Psychiatry Res. 2014, 220, 960–969. [Google Scholar] [CrossRef]
- Sierra, M.; Senior, C.; Phillips, M.L.; David, A.S. Autonomic response in the perception of disgust and happiness in depersonalization disorder. Psychiatry Res. 2006, 145, 225–231. [Google Scholar] [CrossRef]
- Simeon, D.; Knutelska, M.; Nelson, D.; Guralnik, O. Feeling unreal: A depersonalization disorder update of 117 cases. J. Clin. Psychiatry 2003, 64, 990–997. [Google Scholar] [CrossRef]
- Taylor-Clarke, M.; Jacobsen, P.; Haggard, P. Keeping the world a constant size: Object constancy in human touch. Nat. Neurosci. 2004, 7, 219–220. [Google Scholar] [CrossRef] [PubMed]
- Chieffi, S.; Messina, G.; La Marra, M.; Iavarone, A.; Viggiano, A.; De Luca, V.; Monda, M. Distractor interference in visual motor tasks. In Horizon in Neuroscience Research; Nova Science Publishers, Inc.: Hauppauge, NY, USA, 2014. [Google Scholar]
- Precenzano, F.; Ruberto, M. Sleep habits in children affected by autism spectrum disorders: A preliminary case-control study. Int. J. Obes. 2017, 3, 405–409. [Google Scholar] [CrossRef]
- Maximova, K.; McGrath, J.; Barnett, T.; O’Loughlin, J.; Paradis, G.; Lambert, M. Do you see what I see? Weight status misperception and exposure to obesity among children and adolescents. Int. J. Obes. 2008, 32, 1008–1015. [Google Scholar] [CrossRef]
- O’Connor, J.N.; Golley, R.K.; Perry, R.A.; Magarey, A.M.; Truby, H. A longitudinal investigation of overweight children’s body perception and satisfaction during a weight management program. Appetite 2015, 85, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Docteur, A.; Urdapilleta, I.; Defrance, C.; Raison, J. Body Perception and Satisfaction in Obese, Severely Obese, and Normal Weight Female Patients. Obesity 2010, 18, 1464–1465. [Google Scholar] [CrossRef]
- Gardner, R.M.; Gallegos, V.; Martinez, R.; Espinoza, T. Mirror feedback and judgments of body size. J. Psychosom. Res. 1989, 33, 603–607. [Google Scholar] [CrossRef]
- Braet, C.; Tanghe, A.; Decaluwé, V.; Moens, E.; Rosseel, Y. Inpatient Treatment for Children With Obesity: Weight Loss, Psychological Well-being, and Eating Behavior. J. Pediatr. Psychol. 2004, 29, 519–529. [Google Scholar] [CrossRef]
- Ratcliff, M.B.; Eshleman, K.E.; Reiter-Purtill, J.; Zeller, M.H. Prospective changes in body image dissatisfaction among adolescent bariatric patients: The importance of body size estimation. Surg. Obes. Relat. Dis. 2011, 8, 470–475. [Google Scholar] [CrossRef]
- Shaban, L.H.; Vaccaro, J.A.; Sukhram, S.D.; Huffman, F.G. Perceived body image, eating behavior, and sedentary activities and body mass index categories in Kuwaiti female adolescents. Int. J. Pediatr. 2016, 2016, 1092819. [Google Scholar] [CrossRef]
- Watson, P.M.; Dugdill, L.; Pickering, K.; Owen, S.; Hargreaves, J.; Staniford, L.J.; Murphy, R.C.; Knowles, Z.; Cable, N. Service evaluation of the GOALS family-based childhood obesity treatment intervention during the first 3 years of implementation. BMJ Open 2015, 5, e006519. [Google Scholar] [CrossRef]
- Griffen, T.C.; Naumann, E.; Hildebrandt, T. Mirror exposure therapy for body image disturbances and eating disorders: A review. Clin. Psychol. Rev. 2018, 65, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Kollei, I.; Horndasch, S.; Erim, Y.; Martin, A. Visual selective attention in body dysmorphic disorder, bulimia nervosa and healthy controls. J. Psychosom. Res. 2016, 92, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Beglin, S.J. Assessment of eating disorders: Interview or self-report questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar] [CrossRef]


{kind=link}
| Normal-Weight (n = 437) | Overweight (n = 224) | Obese (n = 88) | p-Value | |
|---|---|---|---|---|
| Eating Disorder Inventory 2 (EDI-2) | ||||
| Drive for Thinness—DT | 3.8 (5) | 8.1 (5.8) | 11.6 (5.5) | <0.001 * |
| Bulimia—BU | 2.4 (2.8) | 2.7 (3.7) | 3.1 (3) | 0.156 |
| Body Dissatisfaction—BD | 6.4 (5.8) | 12.8 (7.6) | 16 (6.1) | <0.001 * |
| Ineffectiveness—IN | 3.1 (3.4) | 4.7 (4.5) | 4.2 (3.9) | <0.001 * |
| Perfectionism—P | 4.7 (3.2) | 5 (3.7) | 5.4 (3) | 0.175 |
| Interpersonal Distrust—ID | 3.4 (2.8) | 3.5 (2.8) | 5 (3.6) | 0.006 * |
| Interoceptive Awareness—IA | 5.1 (5) | 6 (4.9) | 6.2 (6.6) | 0.113 |
| Maturity Fears—MF | 6.3 (3.7) | 6.9 (4.8) | 7 (3.7) | 0.425 |
| Asceticism—ASC | 3.3 (2.8) | 4.1 (3.1) | 4.6 (3.3) | 0.001 * |
| Impulse Regulation—IR | 4.3 (4.3) | 5.8 (4.8) | 5.9 (5.7) | <0.001 * |
| Social Insecurity—SI | 3.4 (2.4) | 4 (3.4) | 4.2 (3.9) | 0.048 |
| Body Uneasiness Test (BUT-Form A) | ||||
| Global Severity Index—GSI | 0.8 (0.7) | 1.4 (1) | 1.5 (0.8) | <0.001 * |
| Weight Phobia—WP | 1.2 (0.8) | 2 (1.2) | 2 (0.9) | <0.001 * |
| Body Image Concerns—BIC | 0.9 (0.8) | 1.9 (1.3) | 2.2 (1.1) | <0.001 * |
| Compulsive Self-Monitoring—CSM | 0.9 (0.8) | 1.2 (0.9) | 1.2 (0.8) | <0.001 * |
| Avoidance—A | 0.4 (0.7) | 0.7 (0.8) | 0.8 (0.9) | <0.001 * |
| Depersonalization—D | 0.5 (0.7) | 0.8 (0.9) | 1 (0.9) | <0.001 * |
| Body Satisfaction Scale (BSS) | ||||
| BSS-Total | 35.1 (12) | 38.8 (9.8) | 40.9 (11.6) | <0.001 * |
| BSS-Head | 13.8 (5.1) | 12.9 (4.6) | 13.6 (6) | 0.377 |
| BSS-Torso | 10.9 (4.3) | 12.7 (3.8) | 14.7 (4.2) | <0.001 * |
| BSS-Limbs | 10.4 (4.8) | 13.2 (4.8) | 12.6 (4.9) | <0.001 * |
| Dieter’s Inventory of Eating Temptations (DIET) | ||||
| DIET Total Score | 4.3 (1) | 4.1 (0.9) | 4.1 (0.9) | 0.042 |
| Overeating—OE | 3.7 (1.5) | 3.8 (1.5) | 3.6 (1.4) | 0.811 |
| Negative Emotions—NE | 4.8 (1.4) | 4.7 (1.3) | 4.4 (1.5) | 0.233 |
| Positive Social—PS | 4.6 (1.6) | 4.2 (1.3) | 4.1 (1.2) | 0.009 * |
| Food Choice—FC | 3.1 (1.5) | 3.0 (1.2) | 2.9 (1.4) | 0.810 |
| Resisting Temptation—RT | 5.1 (1.6) | 4.3 (1.5) | 4.6 (1.5) | <0.001 * |
| Exercise—EX | 3.9 (1.3) | 3.9 (1.2) | 4.2 (1.5) | 0.067 |
| Roman Alexithymia Scale (RAS) | ||||
| Somatic Expression of Emotions—SEE | 8.9 (2.5) | 9.3 (3.0) | 9.2 (3.4) | 0.753 |
| Difficulties to identify the emotions—DIE | 13.2 (3.4) | 14.4 (3.4) | 12.8 (3.3) | <0.001 * |
| Difficulties to communicate the emotion—DCE | 10.6 (2.9) | 9.3 (2.3) | 9.7 (2.3) | <0.001 * |
| Externally oriented thinking—EOT | 10.2 (1.9) | 10.3 (2.3) | 10.3 (2.6) | 0.841 |
| Difficulties to be empathetic—DE | 11.4 (2.3) | 11.1 (2.1) | 12.2 (2.7) | <0.001 * |
| Total score RAS | 53.4 (7.1) | 54.3 (8.3) | 55.1 (10) | 0.363 |
| Adolescent Dissociative Experiences Scale (A-DES) | 1.9 (1.4) | 1.9 (1.3) | 2.3 (1.8) | 0.862 |
| Temperament and Character Inventory (TCI) | ||||
| Novelty Seeking—NS | 20.9 (4.7) | 20.8 (5.7) | 20.2 (4.5) | 0.410 |
| Harm avoidance—HA | 46.5 (36.2) | 52.5 (40.8) | 45.4 (40.4) | 0.142 |
| Reward Dependence—RD | 15.6 (3.3) | 15.9 (2.9) | 15.4 (3) | 0.662 |
| Persistence—P | 4.5 (1.6) | 4.4 (1.5) | 4.7 (1.7) | 0.281 |
| Self-Directedness—SD | 26.2 (6) | 25.5 (7.7) | 28.3 (7.3) | 0.001 * |
| Cooperativeness—C | 30.2 (5.6) | 30.3 (5.2) | 30.1 (5.8) | 0.846 |
| Self-Transcendence—ST | 17.3 (5.3) | 16 (5.6) | 14.8 (5.6) | <0.001 * |
| Functions | ||
|---|---|---|
| 1 | 2 | |
| EDI-2—Drive for Thinness—DT | 0.476 | |
| EDI-2—Body Dissatisfaction—BD | 0.433 | |
| BSS-Torso | 0.317 | |
| EDI-2—Interpersonal Distrust—ID | 0.245 | |
| BUT—Depersonalization—D | 0.211 | |
| DIET—Resisting Temptation—RT | 0.446 | |
| EDI-2—Ineffectiveness—IN | −0.294 | |
| BUT—Compulsive Self-Monitoring—CSM | −0.237 | |
| RAS—Difficulties to communicate the emotion—DCE | 0.205 | |
| BMI | Predicted Group Membership (%) | Total | ||
|---|---|---|---|---|
| Normal-Weight | Overweight | Obese | ||
| Normal-weight | 87.1 | 10.1 | 2.8 | 100.0 |
| Overweight | 37.4 | 57.2 | 5.4 | 100.0 |
| Obese | 18.2 | 13.6 | 68.2 | 100.0 |
| Functions | ||
|---|---|---|
| 1 | 2 | |
| Normal-weight | −0.505 | 0.452 |
| Overweight | 0.199 | −0.775 |
| Obese | 0.992 | −0.274 |
| Component | ||
|---|---|---|
| 1 | 2 | |
| EDI-2—Drive for Thinness—DT | 0.899 | |
| EDI-2—Body Dissatisfaction—BD | 0.824 | |
| EDI-2—Interpersonal Distrust—ID | 0.474 | |
| BUT—Depersonalization—D | 0.904 | |
| BSS-Torso | 0.889 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Marra, M.; Messina, A.; Ilardi, C.R.; Staiano, M.; Di Maio, G.; Messina, G.; Polito, R.; Valenzano, A.; Cibelli, G.; Monda, V.; et al. Factorial Model of Obese Adolescents: The Role of Body Image Concerns and Selective Depersonalization—A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 11501. https://doi.org/10.3390/ijerph191811501
La Marra M, Messina A, Ilardi CR, Staiano M, Di Maio G, Messina G, Polito R, Valenzano A, Cibelli G, Monda V, et al. Factorial Model of Obese Adolescents: The Role of Body Image Concerns and Selective Depersonalization—A Pilot Study. International Journal of Environmental Research and Public Health. 2022; 19(18):11501. https://doi.org/10.3390/ijerph191811501
Chicago/Turabian StyleLa Marra, Marco, Antonietta Messina, Ciro Rosario Ilardi, Maria Staiano, Girolamo Di Maio, Giovanni Messina, Rita Polito, Anna Valenzano, Giuseppe Cibelli, Vincenzo Monda, and et al. 2022. "Factorial Model of Obese Adolescents: The Role of Body Image Concerns and Selective Depersonalization—A Pilot Study" International Journal of Environmental Research and Public Health 19, no. 18: 11501. https://doi.org/10.3390/ijerph191811501