



Physical Activity and Mental Health Declined during the Time of the COVID-19 Pandemic: A Narrative Literature Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Eligibility Criteria
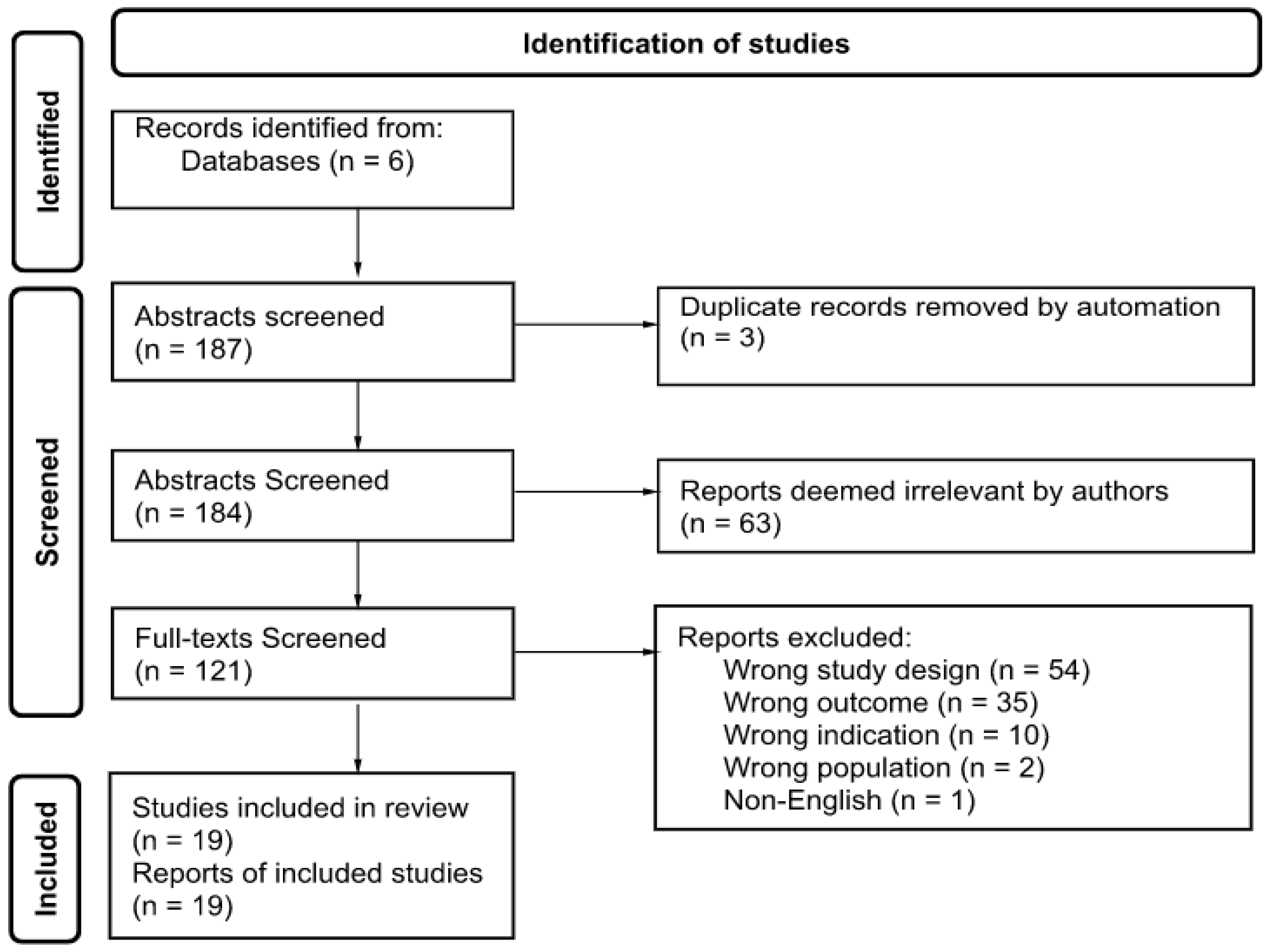
2.4. Study Selection
2.5. Data Extraction
2.6. Quality Assessment
2.7. Data Analysis
3. Results
3.1. Study Characteristics
3.2. Mental Health Assessment
3.3. Physical Activity Assessment
3.4. MH and PA Interaction
4. Discussion
4.1. Research Implications
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Characteristics of Included Studies

{kind=link}
| Study Description | Study Sample | Assessment Tools | Outcomes | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author, Year | Country of the Study | Study Design | Aim(s) of the Study | Sample Size | Age M or Range | Gender % | Education | Mental Health | Physical Activity | Key Observation(s) |
| Almandoz, 2020 [52] | USA | Cross-sectional online survey | The study examined the relationship between COVID-19 psychosocial health implications among clinical obese adult patients and health professionals’ attitudes regarding COVID-19. | 123 | M = 51.2 (SD ± 13.0) | Female 87% (n = 107) | Bachelors or higher 56.1% (n = 69) | Quick Inventory of Depressive Symptomatology | Has the time you dedicated to exercise changed? Has the intensity of your exercise changed? | PA substantially decreased in duration and intensity (47.9%, 55.8%, respectively) among obese patients and they showed an increase in anxiety (72.8%) and depression (83.6%). |
| Choi, 2020 [69] | South Korea | Cross-sectional | The study analyzed the health concerns caused by COVID-19 and the intention of people to continue to participate in sports. | 229 | 18–55+ years | Female 42.4% (n = 98) | N/A | Illness Attitude Scale | 4 items for sport participation | Findings indicated that the individuals participated in group sports but were anxious about their health and intended to discontinue group sports activities. It was understood that the participants were slightly anxious about the possibility of infection due to increased spread of COVID-19 and that they would no longer participate in group sports. |
| Coughenour, 2021 [53] | USA | Cross-sectional online survey | The study examined PA minutes among college students before and after “stay-at-home” orders and determined if the changes were due to depression. | 194 | M = 25.11 (SD ± 7.84) | Female 72.2% (n = 140) | Current college students n = 100% | Diagnostic & Statistical Manual of Mental Disorders, Version Four (DSM-IV). | Patient Health Questionnaire (PHQ-9) | College students reported higher depression scores (p < 0.01) and reduced PA (p = 0.01) after “stay-at-home” orders were issued. There was a small but significant (p = 0.04) correlation between changes in total minutes of PA and depression scores. Seniors (p = 0.05) and Hispanic students (p = 0.03) were less likely to report worsening depression scores than first year and non-Hispanic white students. Asian students were significantly more likely to report decreased PA than non-Hispanic white students. This study suggests that COVID-19 and its consequences may contribute to reduced PA and greater depressive symptoms in college students and that sub-groups of college students have been affected differently. |
| Czenczek-Lewandowska, 2021 [55] | Poland | Retrospective, pre-post survey study | The study assessed whether and to what extent the COVID-19 pandemic has affected the health behaviors of young adults and assessed the level of generalized anxiety and its impact on health-related behaviors. | 506 | M = 24.67 (SD ± 4.23) | Female 70.2% (n = 355) | Bachelors or higher 46.0% (n = 233) | Generalized Anxiety Disorder (GAD-7) scale | IPAQ-Short Form | During the COVID-19 lockdown, generalized anxiety negatively impacted sedentary behaviors and sleep quality. |
| Ding, 2021 [68] | Brazil Bulgaria China India Ireland Malaysia North Macedonia Singapore Spain Turkey USA | Cross-sectional | The study investigated the associations of country-level COVID-19 risk, mental health symptoms, demographic factors with PA engagement, level of PA, and change in PA during the COVID-19 lockdown. | 11,775 | 18–65+ years | Female 63.7% (n = 7498) | Bachelors or higher 62.9% (n = 7406) | Adult Patient Reported Outcomes Measurement Information System (PROMIS) Short Form v1.0-Anxiety 4a and PROMIS Short Form v1.0-Depression 4a | IPAQ-7 item | The study reported that higher depression symptom mean scores were associated with greater odds of being sufficiently inactive and decreased PA levels during the lockdown. Higher mean anxiety scores were associated with greater odds of decreased PA level during the lockdown. |
| Kaygısı, 2020 [63] | Northern Cyprus | Cross-sectional online survey | The study examined exercise habits before and during the pandemic among post-menopausal women’s PA levels and anxiety. The study examined the factors related to the PA levels among post-menopausal women who self-quarantined during the pandemic. | 104 | 50–70 years | Female 100% (n = 104) | N/A | Beck Anxiety Inventory | IPAQ-Short Form-Turkish version | The results showed that the post-menopausal women who exercised before the pandemic had higher PA levels during the pandemic. Post-menopausal women with more grandchildren engaged in less PA and reported higher anxiety levels. The levels of anxiety and PA were negatively associated with each other. |
| Kekäläinen, 2021 [56] | Finland | Longitudinal surveys | The study examined pre- to in-pandemic changes in health behaviors and depressive symptoms and investigated the role of personality in these changes among middle-aged Finnish females. | 358 | 51–59 years | Female 100% n = 358 | N/A | Center for Epidemiological Studies- Depression Scale (CES-D) | The frequency, intensity, and duration of leisure-time PA and recorded as MET hours per day were collected among participants. Perceived change in PA was asked about in the in-pandemic-I and -II questionnaires with the question: “Have you changed your PA or exercise behavior during the COVID-19 pandemic?” | Females reported more depressive symptoms and unhealthier eating habits at the end of the emergency conditions compared to the pre-pandemic time. An increase in depressive symptoms was associated with changing to unhealthier eating habits. Higher extraversion was associated with a perceived decrease in alcohol consumption and with changing to healthier eating habits. Females with higher neuroticism reported changing to either healthier or unhealthier eating habits. In general, some females reported healthier lifestyle changes while other females reported the opposite. Personality traits help understand these individual differences inadaptation to the pandemic situation. |
| Lara, 2021 [57] | Spain | Cross-sectional | The study examined which coping strategies and styles were associated with anxiety levels and determined whether PA during the COVID-19 pandemic differed in coping strategies and styles. | 200 | 18–74 years | Female 70% (n = 140) | Bachelors or higher 57.5% (n = 115) | Zung’s Self- Reported Anxiety Scale (SAS), Spanish version | PA levels were self-reported before and during the pandemic weekly. | The study found PA as a coping resource. The study found that the prevalence of a sedentary lifestyle was four times higher during the pandemic than in the pre-pandemic stage (21% pre-pandemic, 87% during the pandemic). The negative change in PA was due to the restrictions to prevent the spread of COVID-19. The factors for decreased PA were the lack of home-based programming. |
| Marashi, 2021 [67] | Canada | Cross-sectional online survey | The study aimed to examine the relationship between PA and sedentary behavior and how it impacts perceived barriers and motivators to PA during the COVID-19 pandemic. | 1669 | 18–65+ years | Female 82.4% (n = 1218) | Bachelors or higher 80.7% (n = 1026) | Generalized Anxiety Disorder 7-item Scale (GAD-7) Patient Health Questionnaire (PHQ-9) | PA and Sedentary Behavior Questionnaire (PASB-Q) was adapted to report PA and sedentary behavior 6 months before and during the COVID-19 pandemic | Participants reported higher psychological stress and moderate levels of anxiety and depression during the pandemic. Participants with the highest reported mental health deterioration were the least likely to be active. Most participants were unmotivated to exercise because they were anxious. The findings highlight the paradox between mental health and PA. People who wanted to be active to improve their mental health but found it challenging to be active due to their poor mental health. Likewise, participants who were more depressed were less motivated to engage in PA. |
| Martinez, 2020 [64] | Brazil | Cross-sectional | The study aimed to assess the changes in PA levels among Brazilians after social distancing measures were placed during the COVID-19 epidemic. The study also described the participants’ levels of anxiety and depression during the pandemic. | 1613 | 18–60+ years | Female 63.1% (n = 1017) | Bachelors or higher 74.3% (n = 1198) | Hospital Anxiety Depression Scale | PA frequency was asked before the “stay-at-home” mandate and their perceptions of the impact of COVID-19 on their PA and life routines. The participants were asked if they were professional athletes or if they had a home gym. | The study found that participants who are against the social distancing measures on PA and do not agree that COVID-19 is a significant public health concern tend to have a higher prevalence of depression symptoms. Anxiety symptoms were reported lower among the participants who reported a low impact of social distancing on PA and daily life. The findings highlight the profound impact of the COVID-19 pandemic on the population’s mental health and show a global demand for strategies to improve the coping and adaptation process in a situation of social isolation. |
| Moriarty, 2021 [54] | USA | Cross-sectional survey | The study examined the relationship between perceived stress and health behaviors among college students during the COVID-19 pandemic. | 868 | M = 21.3 (SD ± 3.8) | Female 74.2% (n = 408) | College students 100% (n = 550) | Perceived Stress Scale (PSS) | International Physical Activity Questionnaire – Short Form (IPAQ-SF) | The findings indicated that reduced sleep and exercise were associated with higher stress levels regardless of degree programs among college students. |
| Park, 2021 [61] | South Korea | Cross-sectional online survey | The study investigated the impact of the COVID-19 pandemic on lifestyle, mental health, and quality of life. | 104 | M = 32.07 (SD ± 7.64) | Female 72.12% (n = 75) | Bachelors or higher 92.31% (n = 96) | Center for Epidemiological Studies Depression Scale (CESD) | Yonsei Lifestyle Profile | The study found significant reductions in PA and activity participation and decreased frequency and time during the pandemic compared to earlier periods. |
| Perez, 2021 [58] | Spain | Cross-sectional phone interviews | The study examined the PA changes among community-dwelling, frail older adults enrolled in a running program who were not diagnosed with COVID-19. | 98 | M = 82.4 years (SD ± 6.1) | Female 66.3% (n = 65) | Bachelors or higher 14.4% (n = 14) | Yesavage Geriatric Depression Scale | Brief PA Assessment Tool (BPAAT) | Overall, depressive symptoms decreased the odds of maintaining sufficient PA. Moreover, pre-lockdown mental health, frailty, and social relationships were associated with PA levels during the lockdown. |
| Puccinelli, 2021 [65] | Brazil | Cross-sectional | The study examined the impact of social distancing on PA levels and the association between depression and anxiety levels by gender while controlling for objective PA levels, PA changes during the pandemic, adhesion to social distancing, family members, and age. | 1853 | M = 38.6 (SD ± 12.4) | Female 60% (n = 1110) | N/A | Patient Health Questionnaire-9 (PHQ-9) General Anxiety Disorder-7 (GAD-7) | IPAQ | The study found that PA levels during social distancing were significantly lower than before the “stay-at-home” mandate, with 30% of the participants reporting moderate or severe symptoms of depression and approximately 23.3% moderate or severe symptoms of anxiety. Depression and anxiety levels were significantly associated with lower levels of PA, low family monthly income, and age associated with higher levels of anxiety and depression. |
| Rossinot, 2020 [59] | France | Cross-sectional | The study aimed to understand people’s behavior and mental state changes during COVID-19 quarantine. | 1705 | 24–65 years | Female 63.5% (n = 924) | Bachelors or higher 84.3% (n = 1376) | Mental Stress Indicator | Self-reported PA change | The study found that negative mental state changes were strongly associated with nutrition, sleep, PA, and alcohol consumption. Confinement impacted every behavior studied except for nutrition. Almost 50.6% of the participants reported increased depression, stress, and irritability since COVID-19. |
| Shalash, 2020 [62] | Australia | Cross-sectional phone interviews | The study examined the impact of the COVID-19 pandemic on mental health, PA, and quality of life (QoL) among psychological distress patients. | 58 | Parkinson’s disease Patients M = 55.6 years (SD ± 9.956) Control M = 55.55 years (SD ± 5.708) | Parkinson’s disease Female 23.7% (n = 9) Control Females 30% (n = 6) | Bachelors or higher 0.0% (n = 58) | Depression, Anxiety, and Stress Scale-21 (DASS-21) Beck Depression Inventory (BDI) | International Physical Activity Questionnaire (IPAQ)–Short Form | Parkinson’s disease patients reported a negative impact on their mental health, PA, health care, and interest in virtual visits. Parkinson’s patients reported worsened stress, depression, and anxiety compared to the control group. Parkinson’s patients also reported decreased PA since the pandemic. |
| Stanton, 2020 [40] | Australia | Cross-sectional online survey | The study examined the association between psychological distress and changes in selected health behaviors since the onset of COVID-19 and related social isolation measures in Australia. | 1491 | M = 50.5 years (SD ± 14.9) | Females 67.4% (n = 999) | Years of education M = 16.3 (SD ± 5.1) | Depression, Anxiety and Stress Scale (DASS 21) | Active Australia Survey (AAS) | Depression, anxiety, and stress were associated with adverse changes in health behavior. Participants who reported a decrease in PA were likelier to report higher depression, anxiety, and stress symptoms. |
| van der Heide, 2020 [60] | Netherlands | Single-center, longitudinal observational study with an observation period of two years. | The study hypothesized that the COVID-19 pandemic increased psychological distress and decreased PA among patients diagnosed with Parkinson’s disease. | 498 | Responders M = 62.8 years (SD ± 9.0) Non-Responders M = 63.3 years (SD ± 9.1) | Responders Females 38.5% (n = 138) Non-Responders Female 44.3% (n = 62) | N/A | Perceived Stress Scale (PSS), Perceived Anxiety Scale (PAS), Ruminative Response Scale (RRS). | Self-reported changes in PA and minutes/hours of (moderate) intensive exercise per week | The findings found that the COVID-19 pandemic worsened Parkinson’s disease symptoms by evoking psychological distress and reduced PA. |
| Werneck, 2020 [66] | Brazil | Cross-sectional | The study examined the association between diagnosed lifetime depression, changes in physical activity, TV viewing, consumption of fruits and vegetables, and the frequency of ultra-processed food consumption during the COVID-19 pandemic. | 41, 923 | 18–60+ years | Without Depression Female 50.8% (n = 17,801) With Depression Female 68.2 (n = 4693) | Bachelors or higher 35.5% (n = 14,883) | Previous diagnosis of depression | The frequency and duration of leisure-time physical activities before and during the quarantine period and classified using the cut-off point of 150 min per week. | Pre-COVID, individuals diagnosed with depression were more likely to have a higher prevalence rate of physical inactivity. During COVID, the physical inactivity incidence rate did not differ among people diagnosed with depression compared with the general population. |
Appendix B. Quality Appraisal for Selected Studies
| Were the Criteria for Inclusion in the Sample Clearly Defined? | Were the Study Subjects and the Setting Described in Detail? | Was the Exposure Measured in a Valid and Reliable Way? | Were Objective, Standard Criteria Used for Measurement of the Condition? | Were Confounding Factors Identified? | Were Strategies to Deal with Confounding Factors Stated? | Were the Outcomes Measured in a Valid and Reliable Way? | Was Appropriate statistical Analysis Used? | |
|---|---|---|---|---|---|---|---|---|
| Almandoz, 2020 [52] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Choi, 2020 [69] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Coughenour, 2021 [53] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Czenczek-Lewandowska, 2021 [55] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Ding, 2021 [68] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Kaygısız, 2020 [63] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Kekäläinen, 2021 [56] | Yes | Yes | Yes | Yes | Unsure | Unsure | Yes | Yes |
| Lara, 2021 [57] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Marashi, 2021 [67] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Martinez, 2020 [64] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Moriarty, 2021 [54] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Park, 2021 [61] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Perez, 2021 [58] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Puccinelli, 2021 [65] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Rossinot, 2020 [59] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Shalash, 2020 [62] | Yes | Yes | Yes | Yes | Unsure | Unsure | Yes | Yes |
| Stanton, 2020 [40] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| van der Heide, 2020 [60] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Werneck, 2020 [66] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
References
- Booth, F.W.; Laye, M.J. The future: Genes, physical activity and health. Acta Physiol. 2010, 199, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Dunton, G.F. Sustaining Health-Protective Behaviors Such as Physical Activity and Healthy Eating. JAMA 2018, 320, 639–640. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Landolfo, C.; Niebauer, J.; Ozemek, C.; Arena, R.; Lavie, C.J. Promoting Physical Activity and Exercise. J. Am. Coll. Cardiol. 2018, 72, 1622–1639. [Google Scholar] [CrossRef] [PubMed]
- Teychenne, M.; White, R.L.; Richards, J.; Schuch, F.B.; Rosenbaum, S.; Bennie, J.A. Do we need physical activity guidelines for mental health: What does the evidence tell us? Ment. Health Phys. Act. 2019, 18, 100315. [Google Scholar] [CrossRef]
- DeFina, L.F.; Radford, N.B.; Barlow, C.E.; Willis, B.L.; Leonard, D.; Haskell, W.L.; Farrell, S.W.; Pavlovic, A.; Abel, K.; Berry, J.D.; et al. Association of All-Cause and Cardiovascular Mortality With High Levels of Physical Activity and Concurrent Coronary Artery Calcification. JAMA Cardiol. 2019, 4, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Kraus, W.E.; Powell, K.E.; Haskell, W.L.; Janz, K.F.; Campbell, W.W.; Jakicic, J.M.; Troiano, R.P.; Sprow, K.; Torres, A.; Piercy, K.L.; et al. Physical Activity, All-Cause and Cardiovascular Mortality, and Cardiovascular Disease. Med. Sci. Sports Exerc. 2019, 51, 1270–1281. [Google Scholar] [CrossRef]
- Ozemek, C.; Laddu, D.R.; Lavie, C.J.; Claeys, H.; Kaminsky, L.A.; Ross, R.; Wisloff, U.; Arena, R.; Blair, S.N. An Update on the Role of Cardiorespiratory Fitness, Structured Exercise and Lifestyle Physical Activity in Preventing Cardiovascular Disease and Health Risk. Prog. Cardiovasc. Dis. 2018, 61, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Pescatello, L.S.; Buchner, D.M.; Jakicic, J.M.; Powell, K.E.; Kraus, W.E.; Bloodgood, B.; Campbell, W.W.; Dietz, S.; Dipietro, L.; George, S.M.; et al. Physical Activity to Prevent and Treat Hypertension: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1314–1323. [Google Scholar] [CrossRef] [PubMed]
- Smart, C.; Vliet, E.A.-V.; Waldron, S. Nutritional management in children and adolescents with diabetes. Pediatr. Diabetes 2009, 10, 100–117. [Google Scholar] [CrossRef] [PubMed]
- Demark-Wahnefried, W.; Schmitz, K.H.; Alfano, C.M.; Bail, J.R.; Goodwin, P.J.; Thomson, C.A.; Bradley, D.W.; Courneya, K.S.; Befort, C.A.; Denlinger, C.S.; et al. Weight management and physical activity throughout the cancer care continuum. CA A Cancer J. Clin. 2018, 68, 64–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rock, C.L.; Thomson, C.; Gansler, T.; Gapstur, S.M.; McCullough, M.L.; Patel, A.V.; Bandrews, K.S.; Bandera, E.V.; Spees, C.K.; Robien, K.; et al. American Cancer Society guideline for diet and physical activity for cancer prevention. CA A Cancer J. Clin. 2020, 70, 245–271. [Google Scholar] [CrossRef]
- Oza, R.; Rundell, K.; Garcellano, M. Recurrent Ischemic Stroke: Strategies for Prevention. Am. Fam. Physic. 2017, 96, 436–440. [Google Scholar]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Sigal, R.J.; Armstrong, M.J.; Bacon, S.L.; Boulé, N.G.; Dasgupta, K.; Kenny, G.P.; Riddell, M.C. Physical Activity and Diabetes. Can. J. Diabetes 2018, 42, S54–S63. [Google Scholar] [CrossRef]
- Nyström, M.B.; Neely, G.; Hassmén, P.; Carlbring, P. Treating Major Depression with Physical Activity: A Systematic Overview with Recommendations. Cogn. Behav. Ther. 2015, 44, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, L.; Shamila, S.; Scott, B.P.; Demers, A. Self-management of mood and/or anxiety disorders through physical activi-ty/exercise. Health Promot. Chronic Dis. Prev. Can Res. Policy Pract. 2017, 37, 27–32. [Google Scholar]
- WHO-HEP-HPR-RUN-2021.2-eng.pdf. Available online: https://apps.who.int/iris/bitstream/handle/10665/346252/WHO-HEP-HPR-RUN-2021.2-eng.pdf?sequence=1&isAllowed=y (accessed on 19 June 2022).
- Development of the National Health Promotion and Disease Prevention Objectives for 2030. Healthy People 2020. Available online: https://www.healthypeople.gov/2020/About-Healthy-People/Development-Healthy-People-2030 (accessed on 19 June 2022).
- World Health Organization. Fact Sheets: Physical Activity. Available online: http://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 19 June 2022).
- Healy, G.N.; Clark, B.K.; Winkler, E.A.; Gardiner, P.A.; Brown, W.J.; Matthews, C.E. Measurement of Adults’ Sedentary Time in Population-Based Studies. Am. J. Prev. Med. 2011, 41, 216–227. [Google Scholar] [CrossRef]
- Charansonney, O.L. Physical activity and aging: A life-long story. Discov. Med. 2011, 12, 177–185. [Google Scholar] [PubMed]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Runacres, A.; Mackintosh, K.A.; Knight, R.L.; Sheeran, L.; Thatcher, R.; Shelley, J.; McNarry, M.A. Impact of the COVID-19 Pandemic on Sedentary Time and Behaviour in Children and Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11286. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, S.J.; Coyne, P.; St-Pierre, E. Stress, physical activity, and screen-related sedentary behaviour within the first month of the COVID-19 pandemic. Appl. Psychol. Health Well-Being 2021, 13, 454–468. [Google Scholar] [CrossRef]
- Greaney, M.L.; Kunicki, Z.J.; Drohan, M.M.; Ward-Ritacco, C.L.; Riebe, D.; Cohen, S.A. Self-reported changes in physical activity, sedentary behavior, and screen time among informal caregivers during the COVID-19 pandemic. BMC Public Health 2021, 21, 1292. [Google Scholar] [CrossRef] [PubMed]
- Timeline: World Health Organization’s COVID-19 Response. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/interactive-timeline (accessed on 19 June 2022).
- CDC. Healthcare Workers; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/long-term-care.html (accessed on 19 June 2022).
- Nyenhuis, S.M.; Greiwe, J.; Zeiger, J.S.; Nanda, A.; Cooke, A. Exercise and Fitness in the Age of Social Distancing During the COVID-19 Pandemic. J. Allergy Clin. Immunol. Pract. 2020, 8, 2152–2155. [Google Scholar] [CrossRef]
- Stay Safe, Have Fun during the COVID-19 Pandemic. Mayo Clinic. Available online: https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/safe-activities-during-covid19/art-20489385 (accessed on 19 June 2022).
- Staying Active While Social Distancing: Questions and Answers—News & Events. Available online: https://health.gov/news/202004/staying-active-while-social-distancing-questions-and-answers (accessed on 19 June 2022).
- García-Fernández, J.; Gálvez-Ruiz, P.; Grimaldi-Puyana, M.; Angosto, S.; Fernández-Gavira, J.; Bohórquez, M.R. The Promotion of Physical Activity from Digital Services: Influence of E-Lifestyles on Intention to Use Fitness Apps. Int. J. Environ. Res. Public Health 2020, 17, 6839. [Google Scholar] [CrossRef] [PubMed]
- News Detail. ACSM_CMS. Available online: https://www.acsm.org/news-detail (accessed on 19 June 2022).
- Robinson, K.R. Comparing the Spanish flu and COVID-19 pandemics: Lessons to carry forward. Nurs. Forum 2021, 56, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Javelle, E.; Raoult, D. COVID-19 pandemic more than a century after the Spanish flu. Lancet Infect. Dis. 2020, 21, e78. [Google Scholar] [CrossRef]
- Lee, S.M.; Kang, W.S.; Cho, A.-R.; Kim, T.; Park, J.K. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Sim, M. Psychological trauma of Middle East Respiratory Syndrome victims and bereaved families. Epidemiol. Health 2016, 38, e2016054. [Google Scholar] [CrossRef]
- Fiest, K.M.; Leigh, J.P.; Krewulak, K.D.; Plotnikoff, K.M.; Kemp, L.G.; Ng-Kamstra, J.; Stelfox, H.T. Experiences and management of physician psychological symptoms during infectious disease outbreaks: A rapid review. BMC Psychiatry 2021, 21, 91. [Google Scholar] [CrossRef]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Depression and anxiety during COVID-19. Lancet 2022, 399, 518. [Google Scholar] [CrossRef]
- Wilke, J.; Mohr, L.; Tenforde, A.; Edouard, P.; Fossati, C.; González-Gross, M.; Ramírez, C.S.; Laiño, F.; Tan, B.; Pillay, J.; et al. A Pandemic within the Pandemic? Physical Activity Levels Substantially Decreased in Countries Affected by COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 2235. [Google Scholar] [CrossRef]
- Pérez, L.M.; Castellano-Tejedor, C.; Cesari, M.; Soto-Bagaria, L.; Ars, J.; Zambom-Ferraresi, F.; Baró, S.; Díaz-Gallego, F.; Vilaró, J.; Enfedaque, M.B.; et al. Depressive Symptoms, Fatigue and Social Relationships Influenced Physical Activity in Frail Older Community-Dwellers during the Spanish Lock-down due to the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 808. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Lau, J.T.F.; Griffiths, S.; Choi, K.C.; Tsui, H.Y. Avoidance behaviors and negative psychological responses in the general population in the initial stage of the H1N1 pandemic in Hong Kong. BMC Infect. Dis. 2010, 10, 139. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [PubMed]
- Porcelli, P. Fear, anxiety and health-related consequences after the COVID-19 epidemic. Clin. Neuropsychiatry 2020, 17, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Scully, D.; Kremer, J.; Meade, M.M.; Graham, R.; Dudgeon, K. Physical exercise and psychological well being: A critical review. Br. J. Sports Med. 1998, 32, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moola, S. JBI Manual for Evidence Synthesis—JBI Global Wiki. Chapter 7: Systematic Reviews of Etiology and Risk. 2019. Available online: https://jbi-global-wiki.refined.site/space/MANUAL/4687372/Chapter+7%3A+Systematic+reviews+of+etiology+and+risk (accessed on 19 June 2022).
- Almandoz, J.; Xie, L.; Schellinger, J.N.; Mathew, M.S.; Gazda, C.; Ofori, A.; Kukreja, S.; Messiah, S.E. Impact of COVID-19 stay-at-home orders on weight-related behaviours among patients with obesity. Clin. Obes. 2020, 10, e12386. [Google Scholar] [CrossRef]
- Coughenour, C.; Gakh, M.; Pharr, J.R.; Bungum, T.; Jalene, S. Changes in Depression and Physical Activity among College Students on a Diverse Campus After a COVID-19 Stay-at-Home Order. J. Community Health 2021, 46, 758–766. [Google Scholar] [CrossRef]
- Moriarty, T.; Bourbeau, K.; Zuhl, M. Exercise and Neural Adaptations: Designing a Novel Treatment for Alcohol Addiction. Altern. Ther. Health Med. 2020, 26, 48–57. [Google Scholar]
- Lewandowska, E.C.; Wyszyńska, J.; Leszczak, J.; Baran, J.; Weres, A.; Mazur, A.; Lewandowski, B. Health behaviours of young adults during the outbreak of the COVID-19 pandemic—A longitudinal study. BMC Public Health 2021, 21, 1038. [Google Scholar] [CrossRef]
- Kekäläinen, T.; Hietavala, E.-M.; Hakamäki, M.; Sipilä, S.; Laakkonen, E.; Kokko, K. Personality Traits and Changes in Health Behaviors and Depressive Symptoms during the COVID-19 Pandemic: A Longitudinal Analysis from Pre-pandemic to Onset and End of the Initial Emergency Conditions in Finland. Int. J. Environ. Res. Public Health 2021, 18, 7732. [Google Scholar] [CrossRef] [PubMed]
- Lara, R.; Fernández-Daza, M.; Zabarain-Cogollo, S.; Olivencia-Carrión, M.; Jiménez-Torres, M.; Olivencia-Carrión, M.; Ogallar-Blanco, A.; Godoy-Izquierdo, D. Active Coping and Anxiety Symptoms during the COVID-19 Pandemic in Spanish Adults. Int. J. Environ. Res. Public Health 2021, 18, 8240. [Google Scholar] [CrossRef]
- Perez, P.; Dray, A.; Moore, D.; Dietze, P.; Bammer, G.; Jenkinson, R.; Siokou, C.; Green, R.; Hudson, S.L.; Maher, L. SimAmph: An agent-based simulation model for exploring the use of psychostimulants and related harm amongst young Australians. Int. J. Drug Policy 2012, 23, 62–71. [Google Scholar] [CrossRef]
- Rossinot, H.; Fantin, R.; Venne, J. Behavioral Changes during COVID-19 Confinement in France: A Web-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 8444. [Google Scholar] [CrossRef]
- van der Heide, A.; Meinders, M.J.; Bloem, B.R.; Helmich, R.C. The Impact of the COVID-19 Pandemic on Psychological Distress, Physical Activity, and Symptom Severity in Parkinson’s Disease. J. Parkinson’s Dis. 2020, 10, 1355–1364. [Google Scholar] [CrossRef]
- Park, K.-H.; Kim, A.-R.; Yang, M.-A.; Lim, S.-J.; Park, J.-H. Impact of the COVID-19 pandemic on the lifestyle, mental health, and quality of life of adults in South Korea. PLoS ONE 2021, 16, e0247970. [Google Scholar] [CrossRef]
- Shalash, A.; Roushdy, T.; Essam, M.; Fathy, M.; Dawood, N.L.; Abushady, E.M.; Elrassas, H.; Helmi, A.; Hamid, E. Mental Health, Physical Activity, and Quality of Life in Parkinson’s Disease During COVID-19 Pandemic. Mov. Disord. 2020, 35, 1097–1099. [Google Scholar] [CrossRef] [PubMed]
- Kaygısız, B.B.; Topcu, Z.G.; Meriç, A.; Gözgen, H.; Çoban, F. Determination of exercise habits, physical activity level and anxiety level of postmenopausal women during COVID-19 pandemic. Health Care Women Int. 2020, 41, 1240–1254. [Google Scholar] [CrossRef] [PubMed]
- Martinez, E.Z.; Silva, F.M.; Morigi, T.Z.; Zucoloto, M.L.; Silva, T.L.; Joaquim, A.G.; Dall’Agnol, G.; Galdino, G.; Martinez, M.O.Z.; Da Silva, W.R. Physical activity in periods of social distancing due to COVID-19: A cross-sectional survey. Ciênc. Saúde Coletiva 2020, 25, 4157–4168. [Google Scholar] [CrossRef]
- Puccinelli, P.J.; da Costa, T.S.; Seffrin, A.; de Lira, C.A.B.; Vancini, R.L.; Nikolaidis, P.T.; Knechtle, B.; Rosemann, T.; Hill, L.; Andrade, M.S. Reduced level of physical activity during COVID-19 pandemic is associated with depression and anxiety levels: An internet-based survey. BMC Public Health 2021, 21, 425. [Google Scholar] [CrossRef]
- Werneck, A.O.; Da Silva, D.R.; Malta, D.C.; De Souza-Júnior, P.R.B.; Azevedo, L.O.; Barros, M.B.D.A.; Szwarcwald, C.L. Lifestyle behaviors changes during the COVID-19 pandemic quarantine among 6,881 Brazilian adults with depression and 35,143 without depression. Ciênc. Saúde Coletiva 2020, 25, 4151–4156. [Google Scholar] [CrossRef]
- Marashi, M.Y.; Nicholson, E.; Ogrodnik, M.; Fenesi, B.; Heisz, J.J. A mental health paradox: Mental health was both a motivator and barrier to physical activity during the COVID-19 pandemic. PLoS ONE 2021, 16, e0239244. [Google Scholar] [CrossRef]
- Ding, K.; Yang, J.; Chin, M.-K.; Sullivan, L.; Durstine, J.L.; Violant-Holz, V.; Demirhan, G.; Oliveira, N.R.C.; Popeska, B.; Kuan, G.; et al. Physical Activity among Adults Residing in 11 Countries during the COVID-19 Pandemic Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 7056. [Google Scholar] [CrossRef] [PubMed]
- Choi, C.; Bum, C.-H. Changes in the Type of Sports Activity Due to COVID-19: Hypochondriasis and the Intention of Continuous Participation in Sports. Int. J. Environ. Res. Public Health 2020, 17, 4871. [Google Scholar] [CrossRef] [PubMed]
- Centre for Reviews and Dissemination, University of York. University of York. Available online: https://www.york.ac.uk/crd/ (accessed on 19 June 2022).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amo, C.; Almansour, N.; Harvey, I.S. Physical Activity and Mental Health Declined during the Time of the COVID-19 Pandemic: A Narrative Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 11230. https://doi.org/10.3390/ijerph191811230
Amo C, Almansour N, Harvey IS. Physical Activity and Mental Health Declined during the Time of the COVID-19 Pandemic: A Narrative Literature Review. International Journal of Environmental Research and Public Health. 2022; 19(18):11230. https://doi.org/10.3390/ijerph191811230
Chicago/Turabian StyleAmo, Christina, Najla Almansour, and Idethia S. Harvey. 2022. "Physical Activity and Mental Health Declined during the Time of the COVID-19 Pandemic: A Narrative Literature Review" International Journal of Environmental Research and Public Health 19, no. 18: 11230. https://doi.org/10.3390/ijerph191811230